Introduction
Secretory carcinoma (SC) of the salivary gland is a
rare malignant neoplasm first described by Skálová et al
(1) in 2010. This entity shares
histomorphologic and immunohistochemical features with SC of the
breast, which led to its initial designation as mammary analogue
secretory carcinoma (MASC). In the fourth edition of the World
Health Organization (WHO) Classification of Head and Neck Tumors
published in 2017, MASC was recognized as a distinct salivary gland
tumor and formally renamed SC (2).
The typical morphology of SC is defined by uniform, eosinophilic,
variably vacuolated cells with distinct nucleoli and abundant
periodic acid-positive luminal secretory material. The
immunohistochemical profile of SC includes positive staining for
S100 protein, mammaglobin and cytokeratin 7 (CK7), while DOG1 and
p63 are usually negative (2). Most
cases of salivary gland SC are characterized by the presence of the
ETV6::NTRK3 gene fusion, which represents a defining molecular
alteration. Given its rarity, the etiology and clinical features of
parotid gland SC have not been fully elucidated. Here, we report
two cases of parotid gland SC harboring the ETV6::NTRK3 gene
fusion, both of which were treated with surgical resection followed
by radiotherapy. These cases provide useful insights into imaging
variability, management implications, and the importance of
long-term follow-up.
Case report
Case 1. Case 1 involved a 21-year-old
Japanese man who presented with a 1-year history of a slowly
enlarging, painless mass in the right parotid gland (Table I). Ultrasonography revealed a
well-circumscribed, homogeneous, isoechoic mass adjacent to a tiny
cyst with posterior acoustic enhancement, measuring 16x12x10 mm
(Fig. 1A). Magnetic resonance
imaging (MRI) revealed a solid mass in the right parotid gland,
showing low signal intensity on T1-weighted imaging (T1WI)
(Fig. 1B) and high signal
intensity on T2-weighted imaging (T2WI) (Fig. 1C). Fine-needle aspiration cytology
(FNAC) demonstrated clusters with epithelial and spindle-shaped
cells with interstitial mucin, which was interpreted as
intermediate, with features suggestive of pleomorphic adenoma
corresponding to category IVA of the Milan System for Reporting
Salivary Gland Cytopathology (MSRSGC).
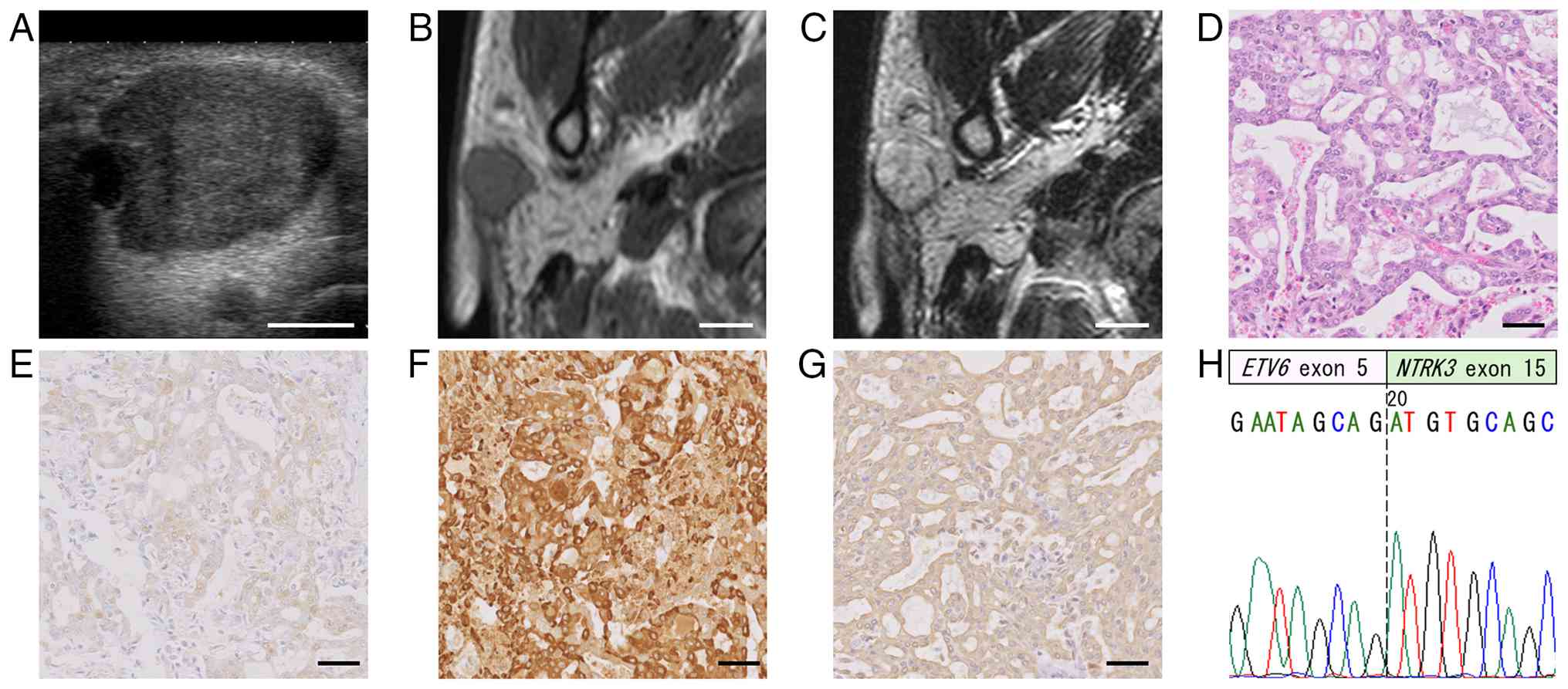 | Figure 1Imaging and histological findings of
case 1. (A) Ultrasonography revealed a well-circumscribed,
homogeneous, isoechoic mass adjacent to a tiny cyst with posterior
acoustic enhancement, measuring 16x12x10 mm. MRI revealed a solid
mass in the right parotid gland, showing (B) low signal intensity
on T1-weighted imaging and (C) high signal intensity on T2-weighted
imaging. (D) After superficial parotidectomy, histological
examination revealed predominantly irregularly shaped microcysts of
varying sizes, lined by round to oval tumor cells and containing
light basophilic secretions within the lumina (hematoxylin and
eosin staining). (E) Immunohistochemical examination revealed that
S-100 protein was weakly and diffusely expressed in the nucleus and
cytoplasm of tumor cells. (F) Mammaglobin was strongly expressed in
the cytoplasm, whereas (G) cytokeratin 7 was expressed in both the
membrane and cytoplasm. (H) Sanger sequencing revealed an
ETV6::NTRK3 gene fusion point between exon 5 of the ETV6
gene (NM_001987.5) and exon 15 of the NTRK3 gene
(NM_002530.4). Based on the histological features,
immunohistochemical profile and molecular findings, the tumor was
diagnosed as secretory carcinoma and staged as pT1N1M0 (pStage
III). White scale bars, 1 cm; black scale bars, 50 µm. |
 | Table ISummary of the 2 cases. |
Table I
Summary of the 2 cases.
| Case | Age, years | Sex | Tumor size, mm | MRI T1WI | MRI T2WI | FNAC | Surgery | RT, Gy | Histology | pTNM | pStage | Outcome |
|---|
| 1 | 21 | Male | 16x12x10 | Low | Low | Pleomorphic
adenoma | Superficial
parotidectomy | 60 | Grade I | T1N1M0 | III | 7 years ANED |
| 2 | 79 | Male | 21x16x15 | High | Intermediate,
high | Suspicious for
malignancy | Total parotidectomy,
I-III neck dissection | 60 | Grade II | T4aN0M0 | IVA | 3 years ANED |
The patient subsequently underwent a right
superficial parotidectomy. Histologic examination revealed a
lobulated tumor composed of microcystic and reticular growth
patterns, with light basophilic secretions within the cystic lumina
(Fig. 1D). The tumor cells
exhibited mildly atypical, round to oval nuclei with vesicular
chromatin and small nucleoli. Few mitotic figures were identified
(1-2 mitoses per 10 high-power fields). These histologic findings
corresponded to Grade 1 according to the histologic grading system
for salivary gland SC proposed by Baněčková et al (3). One intraparotid lymph node was
metastasized. Immunoperoxidase staining of formalin-fixed,
paraffin-embedded (FFPE) tissue sections with anti-S-100 protein
polyclonal antibody (Nichirei; Tokyo, Japan), anti-mammaglobin
monoclonal antibody (31A5; Roche Diagnostics, Basel, Switzerland),
anti-cytokeratin (CK)7 monoclonal antibody (OV-TL 12/30; Nichirei),
anti-cytokeratin antibody (AE1/AE3; Nichirei), anti-p63 antibody
(4A4; Nichirei), and anti-DOG1 antibody (DOG1.1; Thermo Fisher
Scientific, Waltham, MA, USA) were performed using a Ventana
OptiView DAB IHC detection kit (Roche Diagnostics). S-100 protein
was weakly and diffusely expressed in the nucleus and cytoplasm of
tumor cells (Fig. 1E). Mammaglobin
was strongly expressed in the cytoplasm (Fig. 1F), whereas CK7 was expressed in
both the membrane and cytoplasm (Fig.
1G). AE1/AE3 staining was positive but staining for p63 and
DOG1was negative (data not shown).
Reverse transcription-polymerase chain reaction
(RT-PCR) analysis was performed according to previously reported
method (4) with minor
modifications. Total RNA was extracted from formalin-fixed,
paraffin-embedded surgical specimens using a NucleoSpin®
totalRNA FFPE XS kit (Takara, Tokyo, Japan). A 110-bp fragment
corresponding to the ETV6::NTRK3 fusion transcript was amplified
using a OneStep RT-PCR kit (QIAGEN, Hilden, Germany) with a reverse
primer specific for NTRK3 (5'-CAGTTCTCGCTTCAGCACGATG-3') and
forward primer specific for ETV6 (5'-ACCACATCATGGTCTCTGTCTCCC-3').
A synthetic DNA fragment containing the ETV6::NTRK3 fusion junction
was used as a positive control. The negative control consisted of
RNA from tissue sections without carcinoma and no template. The
amplified products were purified and bidirectionally sequenced at
AZENTA Life Sciences (Tokyo, Japan). Sanger sequencing identified
an ETV6::NTRK3 fusion involving exon 5 of ETV6 and exon 15 of NTRK3
(Fig. 1H). Based on the histologic
features, immunohistochemical profile, and molecular findings, the
tumor was diagnosed as SC and staged as pT1N1M0 (pathologic Stage
III) according to the AJCC/TNM staging system, 8th edition
(5). Postoperatively, the patient
received radiotherapy to the parotid region with a total dose of 60
Gy. At 7 years of follow-up, the patient remains free of the
disease.
Case 2. Case 2 involved a 79-year-old
Japanese man who noticed a mass in the right parotid region 3 weeks
prior to presentation (Table I).
Ultrasonography revealed an irregularly marginated, heterogeneous,
hypoechoic mass measuring 21x16x15 mm (Fig. 2A). MRI revealed a solid tumor
located in the anterior part of the right parotid gland, showing
low signal intensity on T1WI (Fig.
2B) and a mixture of intermediate and high signal intensity
with extension to the masseter muscle on T2WI (Fig. 2C). Fluorodeoxyglucose-positron
emission tomography/computed tomography demonstrated increased
uptake in the parotid tumor, with no evidence of neck lymph node or
distant metastasis (Fig. 2D). FNAC
revealed irregular clusters of atypical epithelial cells with
nuclear overlapping, vesicular chromatin, and prominent nucleoli,
which was interpreted as suspicious for malignancy (Milan category
V) (Fig. 2E).
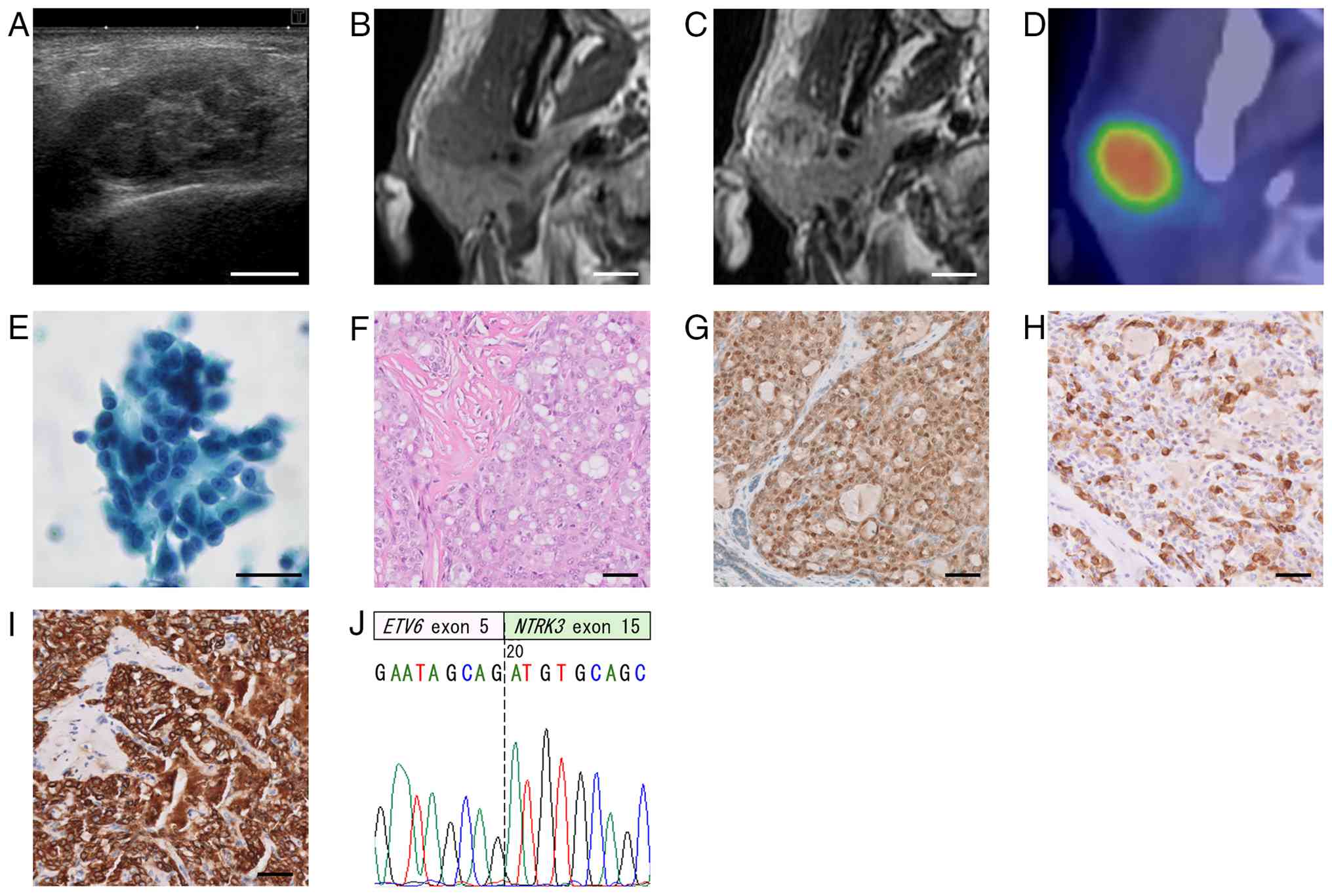 | Figure 2Imaging and histological findings of
case 2. (A) Ultrasonography revealed an irregular, marginated,
heterogeneous, hypoechoic mass measuring 21x16x15 mm. MRI revealed
a solid tumor located in the anterior part of the right parotid
gland, showing (B) low signal intensity on T1-weighted imaging and
(C) a mixture of intermediate and high signal intensity with
extension to the masseter muscle on T2-weighted imaging. (D)
Fluorodeoxyglucose-positron emission tomography/computed tomography
revealed increased uptake by the tumor. (E) Fine-needle aspiration
cytology with Papanicolaou staining demonstrated an irregular
cluster of atypical cells with nuclear overlap, vesicular chromatin
and prominent nucleoli, which was interpreted as suspicious for
malignancy. (F) After total parotidectomy with selective neck
dissection, histologic examination demonstrated infiltrative,
irregular sheets of atypical epithelial cells with vesicular
chromatin. The tumor cells exhibited prominent nucleoli, admixed
with microcysts containing light basophilic secretions within the
lumina, set in a hyalinized stroma (hematoxylin and eosin
staining). (G) Immunohistochemical examination revealed that S-100
protein was diffusely expressed in the nucleus and cytoplasm of
tumor cells. (H) Mammaglobin was focally expressed in the
cytoplasm, whereas (I) cytokeratin 7 was strongly expressed in both
the membrane and cytoplasm. (J) Sanger sequencing analysis revealed
the ETV6::NTRK3 gene fusion point. Based on these findings, the
tumor was diagnosed as secretory carcinoma and staged as pT4aN0M0
(pStage IVA). White scale bars, 1 cm; black scale bars, 50 µm. |
The patient underwent right total parotidectomy with
selective neck dissection of levels I, II, and III. Due to tumor
invasion, the buccal branch of the facial nerve and a portion of
the masseter muscle were resected. Histologic examination
demonstrated infiltrative, irregular sheets of atypical epithelial
cells with vesicular chromatin. The tumor cells exhibited prominent
nucleoli, admixed with microcysts containing light basophilic
secretions within the lumina, set in a hyalinized stroma (Fig. 2F). Few mitotic figures were
identified (4-5 mitoses per 10 high-power fields). These histologic
findings corresponded to Grade 2. No histologic evidence of lymph
node metastasis was found; however, the surgical margin was
positive. Tumor involvement of the resected masseter muscle was
also noted. Immunohistochemically, S-100 protein was diffusely
expressed in the nucleus and cytoplasm of tumor cells (Fig. 2G). Mammaglobin was focally
expressed in the cytoplasm (Fig.
2H), whereas CK7 was strongly expressed in both the membrane
and cytoplasm (Fig. 2I). AE1/AE3
staining was positive but staining p63 and DOG1was negative (data
not shown). Sanger sequencing analysis confirmed the presence of an
ETV6::NTRK3 gene fusion (Fig. 2J).
Based on these findings, the tumor was diagnosed as SC and staged
as pT4aN0M0 (pathologic Stage IVA). Postoperatively, the patient
received radiotherapy to the parotid gland and neck with a total
dose of 60 Gy. As of the 3-year follow-up, the patient remains free
of the disease.
Discussion
SC, previously described as MASC and classified as a
low-grade malignancy, accounts for approximately 1.5% of all
parotid gland carcinomas (6). The
mean age at presentation is reportedly 47.5 years, with a
male-to-female ratio of approximately 1.4:1(3). Regarding anatomic distribution within
the salivary glands, SC most commonly arises in the parotid gland
(77.1%), followed by the submandibular gland (6.3%), with the
remaining 16.6% of casas occurring in other salivary sites
(7). Clinically, parotid gland SC
typically presents as a painless, slowly enlarging mass (8).
On ultrasonography, SC typically presents as a
predominantly cystic tumor with a solid part of the papillary
projection (9). However, in both
Case 1 and Case 2 of the present report, no cystic lesions with
papillary projections were observed. On MRI of SC, the signal
intensities of the solid components varied from low to intermediate
on T1WI and from low to high on T2WI (9,10).
This variation in signal intensity reflected varying degrees of
histological formation of microcysts, a desmoplastic stromal
reaction, and cellularity in the tumor. Wang et al (8) described two patterns of MRI of SC:
one presenting as a partially cystic, lobulated mass that may mimic
a benign tumor, and the other presenting as an irregular mass with
a less cystic composition, which was associated with malignant
features in their series. In Case 1 of the present report,
ultrasonographic and MRI findings of a well-circumscribed,
homogeneous tumor were consistent with a benign tumor. In Case 2,
by contrast, ultrasonographic findings demonstrated an irregularly
marginated, heterogeneous mass, and MRI showed high signal
intensity on T2WI with extension into the masseter muscle,
suggesting a malignant tumor.
FNAC of SC typically shows moderately cellular
smears composed of loosely cohesive sheets, papillary or cribriform
tissue fragments, and dispersed tumor cells in a predominantly
mucinous background, although hemosiderophages and blood may be
present in some cases (11). The
tumor cells generally exhibit a low to moderate
nuclear-to-cytoplasmic ratio, abundant finely granular or
vacuolated cytoplasm, and uniform round to oval nuclei with fine
chromatin, distinct single nucleoli, and only mild cytologic
atypia. According to the MSRSGC, FNAC specimens of SC are most
frequently categorized as malignant (Category VI) (50%), followed
by suspicious for malignancy (Category V) (26%), salivary gland
neoplasm of uncertain malignant potential (Category IVB) (18%), and
atypia of undetermined significance (Category III) (6%) (12). The reported sensitivity of FNAC for
diagnosing malignancy in major salivary gland tumors ranges from 38
to 97% (11,13). However, a review by Kala et
al (11) reported a
sensitivity of FNAC specifically for diagnosing salivary gland SC
of only 27.7%, indicating a considerable diagnostic limitation. In
many cases, the characteristic cytologic features of SC are
recognized retrospectively after a definitive histologic diagnosis,
with or without confirmatory molecular analysis. In the present
study, FNAC findings in Case 1 were interpreted as intermediate,
with pleomorphic adenoma included in the differential diagnosis,
whereas in Case 2, FNAC results were suspicious for malignancy but
did not allow a specific diagnosis of SC.
Histologically, SC typically exhibits a lobulated
growth pattern, with lobules separated by fibrous septa and with
composition of variable architectural patterns, including
microcystic or solid, tubular, follicular, and papillary-cystic
structures with distinctive luminal secretions. The tumor often
demonstrates an infiltrative growth pattern with occasional
perineural invasion and is associated with abundant fibrosclerotic
stroma and prominent, thick, hyalinized septa (14). In 2023, Baněčková et al
(3) proposed a 3-tiered grading
system for SC featuring 4 histologic parameters: (i) architecture
and fibrous septae/fibrosis; (ii) nuclear pleomorphism; (iii)
perineural invasion, lymphovascular invasion, and tumor necrosis;
and (iv) mitotic activity/Ki-67 index. Each parameter was scored on
a scale of 1 to 3 and aggregated to yield a final grade: Grade
1=score 4-6, Grade 2=score 7-9, and Grade 3=score 10-12.
Higher-grade tumors were significantly associated with poor
prognosis (3). The histologic
grade corresponded to Grade 1 with a score of 4 in Case 1 and Grade
2 with a score of 7 in Case 2.
Immunohistochemically, SC reportedly shows CK7
expression in 97-100% of cases (7). In both Case 1 and Case 2, the tumor
cells were positive for S-100 protein, mammaglobin, and CK7 but
negative for DOG1. This immunophenotypic combination is
particularly useful for distinguishing SC from acinic cell
carcinoma, which mimics SC and is typically negative for S-100
protein and mammaglobin but strongly positive for DOG1(15).
SC of the salivary glands is typically characterized
by a recurrent t(12;15)(p13;q25) chromosomal translocation,
resulting in the ETV6::NTRK3 gene fusion, which is considered a
defining molecular alteration unique among salivary gland tumors
(1). The ETV6::NTRK3 fusion gene
encodes a chimeric tyrosine kinase that activates downstream
signaling pathways, including the Ras-mitogen-activated protein
kinase and phosphatidylinositol 3-kinase-Akt pathways, thereby
promoting tumorigenesis (16). The
ETV6::NTRK3 gene fusion has been reported in approximately 94% of
salivary gland SC cases (7).
Several methods are available for detecting this fusion, including
immunohistochemistry using antibodies against pan-tropomyosin
receptor kinase (pan-Trk) (17),
RT-PCR, fluorescence in situ hybridization (FISH), and DNA-
or RNA-based next-generation sequencing (NGS) (18). Nuclear and cytoplasmic staining
with anti-pan-Trk antibody showed an excellent sensitivity of 91%
and specificity of 100% for the presence of ETV6::NTRK3 gene fusion
positive salivary gland SC (17).
However, we did not have the opportunity to perform staining with
this antibody. RT-PCR is technically feasible, inexpensive and
relatively widely accessible, and it can be effectively applied to
FFPE tissue samples for the detection of ETV6::NTRK3 fusion
transcripts (16). The main
limitation of RT-PCR compared with FISH or NGS is the inability to
determine novel fusion partners because ETV6 can
occasionally fuse with alternative non-NTRK gene partners,
including RET (19),
MET (20), and MAML3
(21). In the present study,
classical ETV6::NTRK3 fusion transcripts with a junction between
exon 5 of ETV6 and exon 15 of NTRK3 were identified
in both Case 1 and Case 2. This canonical fusion type is reportedly
the most frequent in salivary gland SC and associated with less
infiltrative histologic features, such as prominent thick fibrous
septa, as well as more favorable clinical outcomes compared with
other ETV6::NTRK3 exon junction variants (16).
With regard to treatment, the National Comprehensive
Cancer Network Guidelines (version 1, 2026) recommend complete
surgical excision with preservation of the facial nerve for
clinically benign lesions and for T1 or T2 salivary gland
carcinomas (22). For patients
with T3 or T4a tumors, the guidelines recommend total parotidectomy
combined with selective neck dissection for clinically N0 disease,
and total neck dissection for patients with clinically evident
lymph node metastasis (22).
Postoperative radiotherapy is generally recommended for patients
with incomplete resection, close surgical margins (<5 mm),
perineural invasion, tumors classified as T3 or T4a, or regional
lymph node metastasis (23).
Previous reports have demonstrated that parotidectomy followed by
radiotherapy with a total dose exceeding 60 Gy yields excellent
local control with minimal treatment-related toxicity in patients
with parotid carcinoma (24). In
Case 1 of the present study, we performed superficial parotidectomy
under a presumed benign diagnosis based on preoperative FNAC. After
confirmation of SC, we did not consider reoperation, such as
completion parotidectomy or neck dissection, because we were
concerned about damage to the preserved facial nerve, and no lymph
node swelling was observed in the neck on imaging studies.
Postoperative radiotherapy with a total dose of 60 Gy was
administered due to close surgical margins. In Case 2, by contrast,
a malignant tumor was suspected based on FNAC and imaging findings,
and although no cervical lymph node metastasis was observed, total
parotidectomy with prophylactic, elective neck dissection of levels
I, II, and III was carried out. Radiotherapy was indicated due to
positive surgical margins and the presence of perineural and muscle
invasion.
More than 75% of patients with salivary gland SC
present with early-stage disease (stage I or II), whereas
approximately 14 and 8% exhibit regional and distant metastases,
respectively, at the first visit (7). The prognosis of patients with SC of
the salivary glands is generally favorable. Following complete
surgical excision, disease-specific survival rates of approximately
95-98% and disease-free survival rates of 87-89% have been reported
(3,25). By contrast, SC with high-grade
transformation is associated with a significantly poorer prognosis,
with reported postoperative survival typically ranging from 2 to 6
years (26).
Recently, the efficacy and safety of Trk inhibitors
have been established for the treatment of NTRK gene
fusion-positive tumors, including salivary gland SC. Doebele et
al (27) described the results
of two phase I trials and one phase II trial of entrectinib
involving a total of 54 patients with metastatic or locally
advanced NTRK gene fusion-positive tumors, including 7 patients
(13%) with salivary gland SC. Although 31 (57%) of the 54 patients
showed an overall response rate, 6 (86%) of the 7 patients with
salivary gland SC demonstrated an overall response rate to the
treatment. A study involving 55 patients with NTRK gene
fusion-positive metastatic or locally advanced tumors, including 12
patients (22%) with salivary gland SC, treated with larotrectinib
demonstrated an overall response rate of 75%, and no severe side
effects necessitating treatment discontinuation were observed
(28). If either patient we
treated develops unresectable lesions or distant metastasis in the
future, these agents would represent promising therapeutic
options.
In conclusion, accurate diagnosis of parotid gland
SC requires a combined assessment of histologic and
immunohistochemical features, with confirmation by detection of the
ETV6::NTRK3 gene fusion. Recognition of this entity is important
because of its potential diagnostic overlap with other salivary
gland neoplasms and its prognostic and therapeutic implications. In
our cases, surgical resection followed by radiotherapy resulted in
favorable clinical outcomes, with no evidence of recurrence or
metastasis observed in either patient during follow-up.
Acknowledgements
The authors would like to thank Dr Ken-Ichi
Matsumoto and Dr Akihiko Miyamoto (Department of Radiation
Oncology, Hokuto Hospital, Obihiro, Hokkaido, Japan) for treating
patients with radiotherapy.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are not
publicly available due to privacy reasons but may be requested from
the corresponding author.
Authors' contributions
MH, NB, TG, SH, RA, KN and MT contributed to
clinical data acquisition and interpretation. MH, NB and HT drafted
the manuscript. TIY and HT performed cytologic diagnosis. SB and YK
performed mutational analyses. HT performed pathologic
investigations. MH and NB confirmed the authenticity of all the raw
data. All authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
All procedures performed on patient tumor samples in
the present study were conducted in accordance with the ethical
standards of the 1964 Declaration of Helsinki and its later
amendments or comparable ethical standards. The present study was
approved by the Ethics Committee of Hokuto Hospital (approval no.
1078; Obihiro, Japan).
Patient consent for publication
Written informed consent for publication of clinical
details and images was obtained from the patients and their
families.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Skálová A, Vanecek T, Sima R, Laco J,
Weinreb I, Perez-Ordonez B, Starek I, Geierova M, Simpson RH,
Passador-Santos F, et al: Mammary analogue secretory carcinoma of
salivary glands, containing the ETV6-NTRK3 fusion gene: A hitherto
undescribed salivary gland tumor entity. Am J Surg Pathol.
34:599–608. 2010.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Seethala RR and Stenman G: Update from the
4th edition of the world health organization classification of head
and neck tumours: Tumors of the salivary gland. Head Neck Pathol.
11:55–67. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Baněčková M, Thompson LDR, Hyrcza MD,
Vaněček T, Agaimy A, Laco J, Simpson RHW, Di Palma S, Stevens TM,
Brcic L, et al: Salivary gland secretory carcinoma:
clinicopathologic and genetic characteristics of 215 cases and
proposal for a grading system. Am J Surg Pathol. 47:661–677.
2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Majewska H, Skálová A, Stodulski D,
Klimková A, Steiner P, Stankiewicz C and Biernat W: Mammary
analogue secretory carcinoma of salivary glands: A new entity
associated with ETV6 gene rearrangement. Virchows Arch.
466:245–254. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
American Joint Committee on Cancer: Major
Salivary Glands. In: AJCC Cancer Staging Manual. 8th edition.
Springer, New York, NY, 2017.
|
|
6
|
Parikh AS, Khawaja A, Puram SV, Srikanth
P, Tjoa T, Lee H, Sethi RKV, Bulbul M, Varvares MA, Rocco JW, et
al: Outcomes and prognostic factors in parotid gland malignancies:
A 10-year single center experience. Laryngoscope Investig
Otolaryngol. 4:632–639. 2019.PubMed/NCBI View
Article : Google Scholar
|
|
7
|
Yosefof E, Boldes T, Dan D, Robenshtok E,
Strenov Y, Bachar G, Shpitzer T and Mizrachi A: Salivary gland
secretory carcinoma; Review of 13 years world-wide experience and
meta-analysis. Laryngoscope. 134:1716–1724. 2024.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wang S, Peng Y, Jiang C, Lin Z,
Infante-Cossio P and Li J: Case series of secretory carcinoma in
the parotid glands. Gland Surg. 13:2198–2205. 2024.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kashiwagi N, Nakatsuka SI, Murakami T,
Enoki E, Yamamoto K, Nakanishi K, Chikugo T, Kurisu Y, Kimura M,
Hyodo T, et al: MR imaging features of mammary analogue secretory
carcinoma and acinic cell carcinoma of the salivary gland: A
preliminary report. Dentomaxillofac Radiol.
47(20170218)2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Han F, Liu F, Wang H, Qin Y, Lu Q, Wu X,
Guo Z and Nan X: Clinicopathologic characterization of secretory
carcinoma of salivary gland. World J Surg Oncol.
22(282)2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Kala PS, Gupta M and Thapliyal N: Efficacy
of fine-needle aspiration cytology in diagnosing secretory
carcinoma of salivary gland: A systematic review and meta-analysis.
Acta Cytol. 68:83–106. 2024.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Wiles AB, Gabrielson M, Baloch ZW, Faquin
WC, Jo VY, Callegari F, Kholova I, Song S, Centeno BA, Ali SZ, et
al: Secretory carcinoma of the salivary gland, a rare entity: An
international multi-institutional study. Cancer Cytopathol.
130:684–694. 2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Stow N, Veivers D and Poole A: Fine-needle
aspiration cytology in the management of salivary gland tumors: An
Australian experience. Ear Nose Throat J. 83:128–131.
2004.PubMed/NCBI
|
|
14
|
Skálová A, Gnepp DR, Lewis JS Jr, Hunt JL,
Bishop JA, Hellquist H, Rinaldo A, Vander Poorten V and Ferlito A:
Newly described entities in salivary gland pathology. Am J Surg
Pathol. 41:e33–e47. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Khurram SA and Speight PM:
Characterisation of DOG-1 expression in salivary gland tumours and
comparison with myoepithelial markers. Head Neck Pathol.
13:140–148. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Skálová A, Vanecek T, Simpson RH, Laco J,
Majewska H, Baneckova M, Steiner P and Michal M: Mammary analogue
secretory carcinoma of salivary glands: Molecular analysis of 25
ETV6 gene rearranged tumors with lack of detection of classical
ETV6-NTRK3 fusion transcript by standard RT-PCR: Report of 4 cases
harboring ETV6-X gene fusion. Am J Surg Pathol. 40:3–13.
2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Yamamoto H, Nozaki Y, Sugii A, Taguchi K,
Hongo T, Jiromaru R, Sato M, Nakano T, Hashimoto K, Fujiwara M and
Oda Y: Pan-tropomyosin receptor kinase immunoreactivity, ETV6-NTRK3
fusion subtypes, and RET rearrangement in salivary secretory
carcinoma. Hum Pathol. 109:37–44. 2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Solomon JP, Benayed R, Hechtman JF and
Ladanyi M: Identifying patients with NTRK fusion cancer. Ann Oncol.
30 (Suppl 8):viii16–viii22. 2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Ishihara A, Kuwabara H, Yasuda E, Jinnin
T, Higashino M, Nagao T, Haginomori SI and Hirose Y: Salivary gland
secretory carcinoma with an ETV6::RET fusion: A case report. Biomed
Rep. 22(73)2025.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Rooper LM, Karantanos T, Ning Y, Bishop
JA, Gordon SW and Kang H: Salivary secretory carcinoma with a novel
ETV6-MET fusion: Expanding the molecular spectrum of a recently
described entity. Am J Surg Pathol. 42:1121–1126. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Guilmette J, Dias-Santagata D, Nosé V,
Lennerz JK and Sadow PM: Novel gene fusions in secretory carcinoma
of the salivary glands: enlarging the ETV6 family. Hum Pathol.
83:50–58. 2019.PubMed/NCBI View Article : Google Scholar
|
|
22
|
NCCN Clinical Practice Guidelines in
Oncology: Head and Neck Cancers (Version 1.2026). Available from:
https://www.nccn.org/guidelines/.
|
|
23
|
Yassin-Kassab A, Gainor D and Sufyan AS:
Atypical presentation of mammary analogue secretory carcinoma of
the lip. Ear Nose Throat J. 101:NP212–NP217. 2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Al-Mamgani A, van Rooij P, Verduijn GM,
Meeuwis CA and Levendag PC: Long-term outcomes and quality of life
of 186 patients with primary parotid carcinoma treated with surgery
and radiotherapy at the Daniel den Hoed Cancer Center. Int J Radiat
Oncol Biol Phys. 84:189–195. 2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Cipriani NA, Blair EA, Finkle J, Kraninger
JL, Straus CM, Villaflor VM and Ginat DT: Salivary gland secretory
carcinoma with high-grade transformation, CDKN2A/B loss, distant
metastasis, and lack of sustained response to crizotinib. Int J
Surg Pathol. 25:613–618. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Xu B, Viswanathan K, Umrau K, Al-Ameri
TAD, Dogan S, Magliocca K, Ghossein RA, Cipriani NA and Katabi N:
Secretory carcinoma of the salivary gland: A multi-institutional
clinicopathologic study of 90 cases with emphasis on grading and
prognostic factors. Histopathology. 81:670–679. 2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Doebele RC, Drilon A, Paz-Ares L, Siena S,
Shaw AT, Farago AF, Blakely CM, Seto T, Cho BC, Tosi D, et al:
Entrectinib in patients with advanced or metastatic NTRK
fusion-positive solid tumours: Integrated analysis of three phase
1-2 trials. Lancet Oncol. 21:271–282. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Drilon A, Laetsch TW, Kummar S, DuBois SG,
Lassen UN, Demetri GD, Nathenson M, Doebele RC, Farago AF, Pappo
AS, et al: Efficacy of larotrectinib in TRK fusion-positive cancers
in adults and children. N Engl J Med. 378:731–739. 2018.PubMed/NCBI View Article : Google Scholar
|














