Introduction
Colorectal cancer (CRC), a prevalent
gastrointestinal malignant neoplasm, remains the second leading
cause of cancer-related mortality worldwide, with an estimated 1.93
million new cases and approximately 904,000 deaths reported
globally in 2022, accounting for 9.6% of all cancer incidence and
9.3% of cancer-related deaths (1).
The integration of curative resection and adjuvant cancer
chemotherapy has emerged as a paradigmatic treatment modality,
yielding notable overall improvement in the prognosis of patients
with CRC (2). However, a cascade of
alterations in epigenetic and metabolic processes can lead to a
strong transfer and invasive capacity in CRC cells, ultimately
resulting in a poor 5-year overall survival (OS) rate of ~12% in
patients with metastatic CRC (3).
Over decades, the American Joint Commission on Cancer/International
Union against Cancer tumor (T)-lymph node (N)-metastasis (M)
staging system has stood as the benchmark for predicting CRC
outcomes (4). Nonetheless, the
considerable variability in clinical prognoses among patients
classified under the same stage implies inherent limitations in the
predictive efficacy of the TNM staging system for CRC prognosis
(5). Accordingly, an integrated
approach that amalgamates the TNM staging system with other salient
prognostic parameters needs to be urgently adopted to direct the
clinical decision-making process and uncover individualized
therapeutic strategies.
Cancer-associated inflammation can occur throughout
the course of the disease and inflammatory cells serve a major role
in the tumor microenvironment. Inflammatory cells are mediators of
tumorigenesis and progression, provide cytokines to cancer cells,
and enhance cell survival and proliferation (6). The neutrophil-lymphocyte ratio (NLR),
a measure of the number of neutrophils per gram of body weight, is
increased in patients with higher disease stage and more aggressive
disease, indicated by an increased number of metastatic sites,
constituting a particularly high risk patient population (7). Consequently, a blood-value assay may
be useful to estimate prognosis in patients with cancer.
A nomogram is a statistical prediction model
presented as a simple graphical display, which integrates
prognostic factors to produce an individualized numeric probability
of a clinical event (8). Compared
with conventional TNM staging, a nomogram has more advantages for
treating numerous types of cancer, thus it has been presented as a
replacement or even a new standard (9,10).
Prognostic biomarkers, which can predict clinicopathological
features and survival in patients with CRC, are useful in the
screening, diagnosis, classification and treatment of CRC (11).
In the present study, a prognostic model was
formulated that was rooted in clinical parameters intricately
associated with clinical prognosis in CRC. The primary objective
was to predict the prognosis of individuals diagnosed with CRC,
thereby providing valuable insights to guide clinicians in
therapeutic strategies for patients with CRC.
Materials and methods
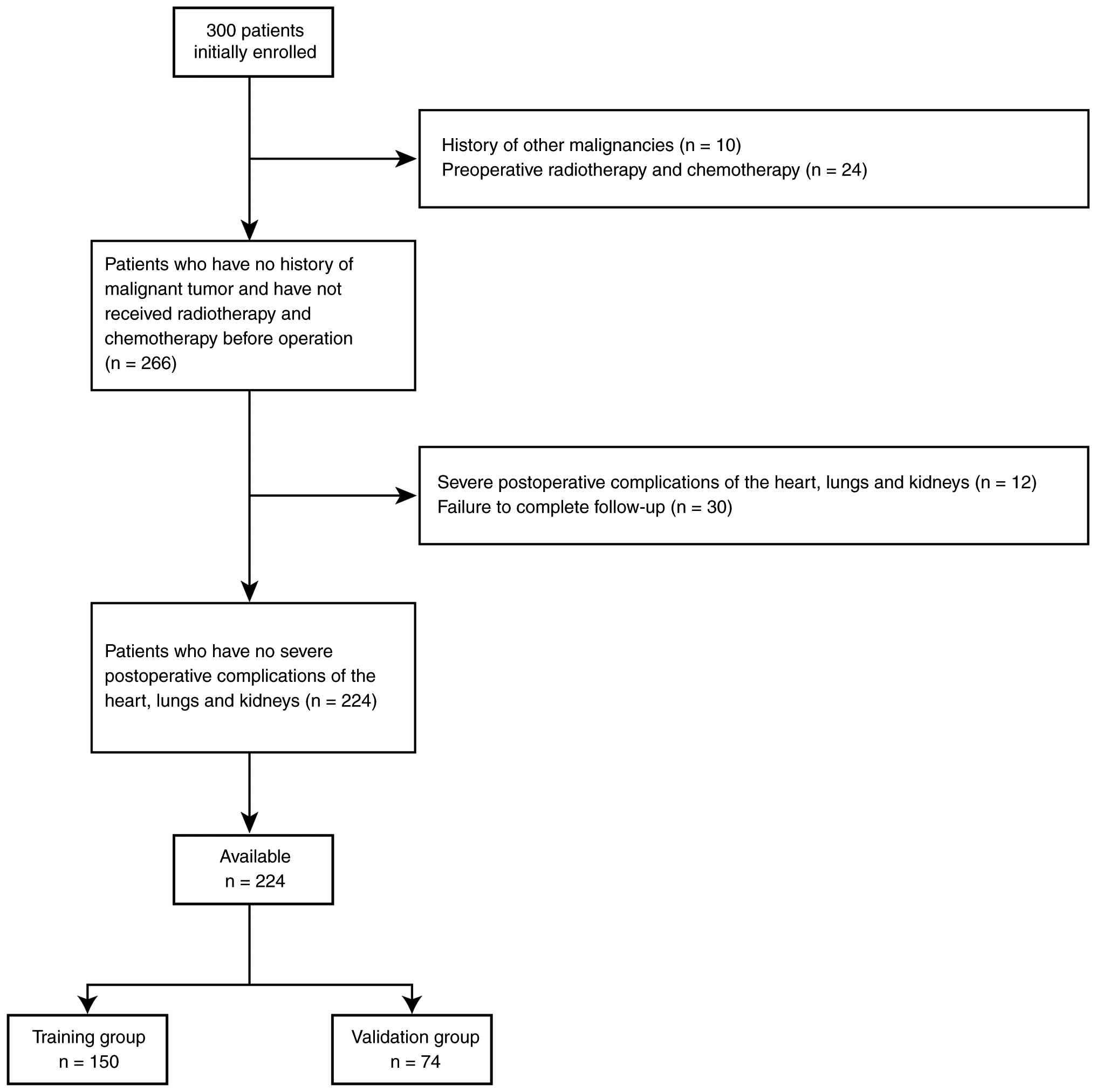
Study population
A total of 224 cases of surgically resected CRC
treated between June 2012 and June 2018 at The First Affiliated
Hospital of Soochow University (Suzhou, China) were included in the
retrospective cohort (Fig. 1). The
inclusion criteria for the selection of these patients were as
follows: i) Pathologically confirmed primary CRC; ii) underwent
primary surgical resection at The First Affiliated Hospital of
Soochow University within the specified timeframe; and iii)
complete preoperative laboratory data, clinicopathological
parameters and follow-up data were available. Among the 224
eligible patients, there were 119 men and 105 women. The median age
of the cohort was 63 years (age range, 49–90 years). All patients
underwent surgical resection and followed the standard treatment
guidelines outlined during this period. The exclusion were as
follows: i) Patients with a prior medical history of other
malignancies, including those related to the cervix, uterus or
bladder; ii) recent chemotherapy or radiotherapy; iii)
postoperative severe complications of the heart, lungs and kidneys;
iv) addiction or mental disorder; and v) patients who did not
attend follow up.
Prior to data collection, written informed consent
was obtained from all participants. The present study received
approval from the Committee for the Ethical Review of Research at
the First Affiliated Hospital of Soochow University (approval no.
125) and was conducted with adherence to institutional guidelines
and the principles outlined in the Declaration of Helsinki. Prior
to formal ethics approval, only a preliminary feasibility
assessment was conducted using limited registry data to evaluate
the available case pool. Patient hospital records were first
formally accessed for research purposes in April 2023, after ethics
approval had been obtained. Full data extraction, confirmation of
eligibility, cohort assignment and statistical analyses were
performed only after ethics approval.
Data collection
The collected clinical data were randomly divided
into the validation (n=74) and training (n=150) sets. The following
clinical data were collected and grouped separately: Sex, blood
type, age, hypertension status, diabetes, prognostic nutritional
index (PNI), lymphocyte-to-monocyte ratio (LMR),
platelet-to-lymphocyte ratio (PLR), body mass index (BMI), levels
of carbohydrate antigen (CA)19-9, CA72-4, CA125, carcinoembryonic
antigen (CEA), lymphocytes, thrombocytes, hemoglobin, neutrophils,
monocytes, alanine aminotransferase (ALT), aspartate
aminotransferase (AST), C-reactive protein (CRP), albumin and
fibrinogen, tumor site, tumor size, T stage, N stage, M stage,
survival time, survival status, systemic immune-inflammation index
(SII), postoperative adjuvant therapy, NLR and pathological type.
The PNI score was derived from the serum albumin level and
lymphocyte count, with the following formula: PNI=[albumin (g/l) +
5]x lymphocytes (109/l).
Treatment
In the Department of General Surgery of the First
Affiliated Hospital of Soochow University, patients with CRC
underwent surgical resection and the resected tissues were examined
pathologically in frozen sections to confirm the diagnosis and
negative surgical margin. According to the postoperative
pathological results, adjuvant chemotherapy was initiated within 3
months after the surgery, which included oxaliplatin plus
capecitabine or oxaliplatin plus capecitabine plus bevacizumab.
Specifically, patients received 130 mg/m2 oxaliplatin
intravenously on day 1 and 1,000 mg/m2 oral capecitabine
twice daily on days 1–14, repeated every 3 weeks. For patients
receiving the bevacizumab-containing regimen, 7.5 mg/kg bevacizumab
was administered intravenously on day 1 of each cycle. A maximum of
8 cycles was planned per patient.
Follow-up
OS was defined as the time from surgery to death in
any case. Follow-up evaluation was performed every 3 months for 5
years and OS data were collected until December 2022. Survival was
determined by reviewing the medical records, which included
laboratory data, computed tomography scans, colonoscopy results and
telephone follow-up results.
Feature selection and survival
analysis
Before starting the analysis, non-hierarchical
categorical variables were converted into dummy variables and
ordinal factor variables were transformed into numerical variables.
In addition, CA19-9 and CEA were dichotomized at the upper limits
of their clinically established reference ranges (CA19-9, 37 U/ml;
CEA, 5 ng/ml) for the analyses presented in Fig. 2C and D. NLR was analyzed as a
continuous variable in the Cox regression analyses, and no cut-off
value was applied. Least Absolute Shrinkage and Selection Operator
(LASSO) analysis was employed to identify prognostic factors using
the glmnet package (version 4.1–1; http://CRAN.R-project.org/package=glmnet) in R. The
estimation of the optimal penalty parameter was accomplished
through a 10-fold cross-validation procedure performed on the
training dataset. To ascertain the statistical significance of the
aforementioned prognostic factors, univariate Cox proportional
hazards regression analysis was conducted. This approach allowed
for the assessment of the impact of each factor on survival time
and the calculation of the corresponding hazard ratio (HR), 95%
confidence interval (CI) and two-sided P-value. Factors with
P<0.05 were included in the construction of the prognostic
clinical signature using the multivariate Cox proportional hazards
model. Subsequently, individual risk scores were computed for each
patient using the following formula: Risk score=[β1
(variable1) × value of variable1] + [β2 (variable2) ×
value of variable2] + ... + [βn (variablen) × value of
variablen], where β represents the regression coefficient obtained
from the multivariate Cox proportional hazards regression model.
The univariate and multivariate Cox proportional hazards regression
analyses were conducted using the ‘survival’ (version 3.2–7;
http://CRAN.R-project.org/package=survival) and
‘survminer’ (version 0.4.8; http://CRAN.R-project.org/package=survminer) R
packages, respectively. The median risk score was used as the
cut-off to stratify patients into high- and low-risk subgroups. For
the Kaplan-Meier analyses, the optimal cut-off value was determined
by the minimum P-value approach.
 | Figure 2.Prognostic factors and nomogram
development for CRC. (A) LASSO coefficient profiles of 34
preoperative indicators and clinicopathological factors associated
with CRC. (B) 10-fold cross-validation used for tuning parameter
selection in the LASSO model. (C) Forest plot displaying the HRs of
prognostic factors identified through univariate Cox analysis of
the training group. (D) Forest plot illustrating the HRs of
prognostic factors identified through multivariate Cox analysis of
the training group. (E) Nomogram designed for predicting 3- and
5-year survival rates for patients in the training group. The
nomogram was constructed based on the training group data and
integrated NLR, CA19-9, CEA and TNM staging information. HR, hazard
ratio; NLR, neutrophil-lymphocyte ratio; CA19-9, carbohydrate
antigen 19-9; CEA, carcinoembryonic antigen; TNM, tumor-lymph
node-metastasis; CRC, colorectal cancer; CI, confidence interval;
LASSO, Least Absolute Shrinkage and Selection Operator; vars,
variables. |
Nomogram construction and
evaluation
The discerned factors from the training group were
utilized to construct a nomogram employing the ‘rms’ (version
6.1–1; http://CRAN.R-project.org/package=rms) R package. To
evaluate its discriminatory capability, the nomogram underwent
bootstrapping validation (1,000 bootstrap resamples) to compute a
relatively corrected concordance index (C-index). Kaplan-Meier (KM)
survival curves with the log-rank test were employed to assess
differences in OS between the high- or low-risk groups.
Additionally, time-dependent receiver operating characteristic
(ROC) (timeROC package; version 0.4; http://CRAN.R-project.org/package=timeROC) and
calibration curves were utilized to evaluate the predictive
performance of the nomogram within the training group. Furthermore,
ROC analysis and decision curve analysis (DCA) (rmda package;
version 1.6; http://CRAN.R-project.org/package=rmda) were employed
to quantitatively assess and compare the clinical utility of the
nomogram, PNI score and standard TNM staging system. These
comparative analyses were replicated in the validation group.
Statistical analysis
Continuous variables are presented as the median
[interquartile range], while categorical variables are presented as
the count (proportion). Continuous variables were compared between
the two groups using the Mann-Whitney U test, and categorical
variables were compared using Fisher's exact test. All statistical
analyses were performed using R software (version 4.0.0; R
Foundation for Statistical Computing). P<0.05 was considered to
indicate a statistically significant difference.
Results
Clinical characteristics
The demographic and clinical profiles of 224
suitable participants who underwent radical resection for CRC are
presented in Table I. This includes
a cohort of 150 patients in the training group and 74 patients in
the validation group. Patients in both groups exhibited no
statistically significant differences in terms of sex, blood type,
age, hypertension status, diabetes, PNI, LMR, PLR, BMI, levels of
CA19-9, CA72-4, CA125, CEA, lymphocytes, thrombocytes, hemoglobin,
neutrophils, monocytes, ALT, AST, CRP, albumin and fibrinogen,
tumor site, tumor size, T stage, N stage, M stage, survival time,
survival status, SII or postoperative adjuvant therapy. However,
there were differences in NLR and pathological type between the two
groups. The median NLR in the training group was 2.54, while it was
2.24 in the validation group. In the training group, the proportion
of patients with moderate differentiation was slightly lower
(86.0%) compared with that in the validation group (89.2%). The
existence of significant differences in the pathological type may
be due to an unbalanced distribution of very few samples of
high/low differentiation.
 | Table I.Demographic and clinical
characteristics of patients in the validation (n=74) and training
(n=150) groups. |
Table I.
Demographic and clinical
characteristics of patients in the validation (n=74) and training
(n=150) groups.
| Variable | Validation
group | Training group | P-value |
|---|
| Sex, n (%) |
|
| 0.570 |
|
Female | 37 (50.00) | 68 (45.33) |
|
|
Male | 37 (50.00) | 82 (54.67) |
|
| Age, n (%) |
|
| 0.203 |
| ≥60
years | 34 (45.95) | 83 (55.33) |
|
| <60
years | 40 (54.05) | 67 (44.67) |
|
| Hypertension, n
(%) |
|
| 0.881 |
| No | 50 (67.57) | 99 (66.00) |
|
|
Yes | 24 (32.43) | 51 (34.00) |
|
| Diabetes, n
(%) |
|
| 0.200 |
| No | 68 (91.89) | 128 (85.33) |
|
|
Yes | 6 (8.11) | 22 (14.67) |
|
| Blood type, n
(%) |
|
| 0.157 |
| A | 15 (20.27) | 50 (33.33) |
|
| AB | 8 (10.81) | 12 (8.00) |
|
| B | 22 (29.73) | 45 (30.00) |
|
| O | 29 (39.19) | 43 (28.67) |
|
| Median CA19-9
[IQR], U/ml | 9.77
[3.78,16.48] | 9.89 [4.32,
29.00] | 0.276 |
| Median CA125 [IQR],
U/ml | 11.40 [7.40,
15.90] | 11.55 [8.10,
15.35] | 0.885 |
| Median CA72-4
[IQR], U/ml | 2.26 [1.16,
3.72] | 1.75 [0.97,
3.72] | 0.350 |
| Median CEA [IQR],
ng/ml | 3.45 [1.52,
7.39] | 3.46 [1.80,
7.45] | 0.652 |
| Median lymphocytes
[IQR], ×109/l | 1.48 [1.20,
1.92] | 1.38 [1.11,
1.78] | 0.098 |
| Median thrombocytes
[IQR], ×109/l | 211.50
[176.25,270.50] | 215.50 [177.50,
275.50] | 0.988 |
| Median hemoglobin
[IQR], g/l | 124.00
[107.50,136.25] | 128.00 [107.00,
140.00] | 0.394 |
| Median neutrophils
[IQR], ×109/l | 3.62 [2.89,
4.54] | 3.78 [2.85,
5.00] | 0.217 |
| Median monocytes
[IQR], ×109/l | 0.39 [0.32,
0.51] | 0.38 [0.29,
0.51] | 0.283 |
| Median ALT [IQR],
U/l | 13.85 [11.10,
18.00] | 15.00 [11.00,
21.00] | 0.324 |
| Median AST [IQR],
U/l | 18.45 [15.43,
22.00] | 18.65 [16.00,
22.00] | 0.676 |
| Median CRP [IQR],
mg/l | 2.71 [1.07,
6.42] | 2.57 [0.98,
9.41] | 0.745 |
| Median albumin
[IQR], g/l | 40.20 [37.60,
42.88] | 40.00 [37.60,
43.68] | 0.812 |
| Median fibrinogen
[IQR], g/l | 3.12 [2.62,
3.60] | 3.21 [2.82,
3.66] | 0.309 |
| Tumor site, n
(%) |
|
| 0.088 |
| Left
colon | 31 (41.89) | 42 (28.00) |
|
|
Rectal | 26 (35.14) | 73 (48.67) |
|
| Right
colon | 17 (22.97) | 35 (23.33) |
|
| Median Size [IQR],
cm | 4.00 [3.00,
5.00] | 4.00 [3.00,
5.00] | 0.793 |
| Pathological type,
n (%) |
|
| 0.040 |
| High
differentiation | 1 (1.35) | 0 (0.00) |
|
| Low
differentiation | 6 (8.11) | 8 (5.33) |
|
|
Moderate differentiation | 66 (89.19) | 129 (86.00) |
|
| Mucous
gland | 1 (1.35) | 13 (8.67) |
|
| T, n (%) |
|
| 0.307 |
| 1 | 5 (6.76) | 9 (6.00) |
|
| 2 | 7 (9.46) | 18 (12.00) |
|
| 3 | 56 (75.68) | 119 (79.33) |
|
| 4 | 6 (8.11) | 4 (2.67) |
|
| N, n (%) |
|
| 0.538 |
| 0 | 37 (50.00) | 85 (56.67) |
|
| 1 | 24 (32.43) | 38 (25.33) |
|
| 2 | 13 (17.57) | 27 (18.00) |
|
| M |
|
| 0.679 |
| 0 | 63 (85.14) | 131 (87.33) |
|
| 1 | 11 (14.86) | 19 (12.67) |
|
| Postoperative
adjuvant therapy, n (%) |
|
| 0.458 |
| No | 23 (31.08) | 55 (36.67) |
|
|
Yes | 51 (68.92) | 95 (63.33) |
|
| Median PNI
[IQR] | 48.20 [45.23,
52.86] | 48.15 [43.99,
51.88] | 0.613 |
| Median LMR
[IQR] | 3.85 [2.46,
5.21] | 3.65 [2.58,
5.15] | 0.713 |
| Median PLR
[IQR] | 145.22 [93.74,
206.87] | 153.14
[111.41,211.62] | 0.197 |
| Median BMI [IQR],
kg/m2 | 23.01 [20.81,
24.94] | 23.02 [20.70,
25.22] | 0.651 |
| Median NLR
[IQR] | 2.24 [1.62,
3.49] | 2.54 [2.01,
3.74] | 0.029 |
| Median SII
[IQR] | 495.55
[295.91,819.47] | 567.07 [381.88,
946.02] | 0.088 |
| Status |
|
| 0.569 |
|
Alive | 42 (56.76) | 78 (52.00) |
|
|
Dead | 32 (43.24) | 72 (48.00) |
|
| Median Time [IQR],
months | 65.67 [50.67,
70.57] | 64.28 [41.59,
71.07] | 0.398 |
Identification of prognostic factors
and development of the nomogram
LASSO was first performed to identify significant
factors related to prognosis. Sex, age, BMI, tumor diameter, tumor
stage, degree of differentiation, surgical procedure, chemotherapy,
and levels of lymphocytes, albumin, CA19-9, hemoglobin, platelets,
AST, ALT, prealbumin and CRP in the training group were included in
the LASSO regression analysis. With a λ value of 0.084, six pivotal
factors were discerned to hold significance in determining the
prognosis of patients with CRC, namely, NLR, CA19-9 and CEA, and
the T, M and N stages (Fig. 2A and
B). The univariate Cox regression analysis further unveiled the
prognostic relevance of all these six factors in relation to
patient outcomes (Fig. 2C). In the
multivariate Cox regression analysis encompassing all variables, a
multitude of independent prognostic factors surfaced, prominently
featuring NLR (HR=1.09; P=0.0044), CA19-9 (HR=1.85; P=0.042), M
stage (HR=1.88; P=0.031) and N stage (HR=3.03; P=0.0007) (Fig. 2D).
With the aim of screening preoperative inflammatory
indicators and enhancing the predictive capacity beyond the
standard TNM staging system, three accessible preoperative factors
(NLR, CEA and CA19-9) were selected and integrated into a nomogram
along with the TNM stage. The primary aim was to establish a
user-friendly model for predicting the OS of patients who undergo
resection for CRC (Fig. 2E).
Assessing performance of the
nomogram
To assess the quantitative predictive performance of
the nomogram, time-dependent ROC analysis was conducted. For the
training group, the areas under the curve (AUCs) were 0.748 at 3
years and 0.749 at 5 years (Fig.
3A). For the validation group, the AUCs were 0.776 at 3 years
and 0.731 at 5 years (Fig. 3B). The
Harrell's C-index of the nomogram was 0.716 (95% CI, 0.58–0.82) in
the training group and 0.700 (95% CI, 0.50–0.84) in the validation
group. Moreover, the calibration curve exhibited good concordance
between the prognostic predictive model and the ideal reference
model (Fig. 3C and D).
To evaluate the effect of this prognostic model,
prognostic scores were calculated in both the training and
validation groups using the aforementioned risk score formula
(Fig. 4A and B). Patients in both
the training and validation groups were stratified according to the
optimal cut-off value determined by the minimum P-value approach,
and Kaplan-Meier curves were then constructed for each group. The
findings revealed that the high-risk subgroup exhibited
significantly shorter median OS times compared with the low-risk
subgroup in both the training (Fig.
4C) and validation (Fig. 4D)
groups.
In summary, the nomogram model may be an effective
and efficient tool for predicting the OS prognosis of patients with
CRC.
Clinical utility
ROC analysis showed that the nomogram could also
markedly predict the 5-year OS of patients with CRC (training
group: AUC=0.749; validation group: AUC=0.731) and was notably
superior to PNI scores (training group: AUC=0.466; validation
group: AUC=0.360) and TNM stage (training group: AUC=0.680;
validation group: AUC=0.697) (Fig. 5A
and B). Subsequently, a DCA was conducted for the nomogram, PNI
scores and TNM stage. The DCA of both the training and test groups
demonstrated that, when the threshold probability exceeded 0.25,
utilizing the developed nomogram for prognostic prediction resulted
in greater net benefits compared with PNI scores and the standard
TNM staging system. This finding indicates the clinical usefulness
of the nomogram (Fig. 5C and
D).
 | Figure 5.ROC curves of the TNM, PNI and
nomogram for predicting the 5-year OS rate of patients with
resected CRC in the training and validation groups. (A) ROC curves
comparing the nomogram, TNM stage and PNI in the training group.
(B) ROC curves comparing the nomogram, TNM stage and PNI in the
validation group. (C) DCA comparing the nomogram, TNM stage and PNI
in the training group. (D) DCA comparing the nomogram, TNM stage
and PNI in the validation group. ROC, receiver operating
characteristic; TNM, tumor-lymph node-metastasis; CRC, colorectal
cancer; OS, overall survival; DCA, decision curve analysis; PNI,
prognostic nutritional index; AUC, area under the receiver
operating characteristic curve. |
In summary, the nomogram model demonstrated improved
predictive accuracy and discriminative performance compared with
the standard TNM staging system.
Discussion
At present, CRC is the third most common malignancy
worldwide (1). The TNM staging
system is typically used to assess the prognosis of patients with
cancer in clinical practice, and although the TNM staging system is
considered the gold standard for assessing the clinical outcome of
patients, there are notable differences in prognosis even among
patients with the same TNM stage (12). The differences in genetic and
biological characteristics of patients at the same stage of disease
lead to limited predictive accuracy of the TNM staging system
(13). In view of this, a more
accurate and convenient method for predicting outcome is needed to
guide clinicians in the treatment of patients with CRC.
Cancer-associated inflammation is considered to be one of the key
features in the development of cancer (14). In the present study, preoperative
inflammatory indicators and tumor markers were investigated in
patients with CRC and combined with TNM staging to create a more
accurate and convenient nomogram for predicting OS. The nomogram
showed strong calibration and discrimination in both the training
and validation groups, and the discrimination, calibration and
clinical validity of the nomogram were superior to the TNM staging
system prognostic model.
A total of 224 eligible patients with CRC were
included in the present study. Patients were divided into training
(n=150) and validation (n=74) groups. LASSO regression and Cox
regression analyses were performed on the training group to
identify meaningful prognostic factors and construct a nomogram to
predict OS, which showed NLR, CA19-9 and CEA as valid risk factors.
The C-indices of the nomogram were 0.716 and 0.700 in the training
and validation groups, respectively. AUCs of the nomogram were
0.748 (training group) and 0.776 (validation group) at 3 years, and
0.749 (training group) and 0.731 (validation group) at 5 years.
Numerous studies have demonstrated the notable
involvement of inflammation in tumor initiation and progression.
Several recent studies have shown that systemic inflammatory
response markers, including CRP, Glasgow prognostic score, PLR and
LMR, are associated with CRC and with poor survival in a range of
other malignancies, including hepatocellular carcinoma and gastric
cancer (15–19). In particular, NLR, which is
considered a marker of systemic inflammatory response, is closely
related to the prognosis of patients with various types of cancer,
including prostate cancer (20) and
renal cell carcinoma (21).
Initially, neutrophils were considered to have a protective
function against tumors, but previous studies have shown that
neutrophils in the tumor microenvironment serve a role in promoting
the growth, invasion, angiogenesis and metastasis of various cancer
types, including colorectal, lung and breast cancers (22–24).
Circulating neutrophils migrate to tumor tissues via CXC motif
chemokine ligand 2-CXC motif chemokine receptor chemotaxis
(25,26) and are termed ‘tumor-associated
neutrophils’ (27). Lymphocytes
serve a notable role in cancer-specific immune responses, among
which tumor-infiltrating lymphocytes are one of the major cells
mediating the local immune response to tumors and are
phenotypically characterized by CD8+ and CD4+
status (28). Thus,
tumor-associated lymphocytes receive different stimuli in different
tumor microenvironments, leading to a shift in lymphocyte subtypes
that can serve both a tumor growth-promoting and tumor
growth-suppressing role. The presence of a severe inflammatory
response in the body is indicated by elevated NLR values.
The results of the present study suggest that NLR
may be an independent prognostic factor for poor survival in
patients with CRC. This finding is consistent with much of the
previous literature. For example, a study by Shin et al
(29) showed that preoperative NLR
predicted survival in patients with resectable stage T1-2 N0 CRC.
Kubo et al (30) also showed
that preoperative and postoperative NLR was a good predictor of
long-term survival in patients with CRC. These studies and the
present study suggest that high NLR values are important for the
prognosis of patients with CRC. Therefore, NLR was included in the
present prognostic model.
The survival of patients with cancer depends not
only on the host systemic inflammatory response but also on the
tumor characteristics (31,32). CEA and CA19-9 are tumor-related
markers widely used for prognosis prediction in patients with CRC
(19,33). Toiyama et al (34) proposed that elevated CEA is a
predictor of decreased OS after preoperative radiotherapy and
chemotherapy in patients with rectal cancer. Thirunavukarasu et
al (35) demonstrated that
serum CEA is an independent prognostic indicator in patients with
CRC, with a mean follow-up period of 27 months. Due to the
prognostic role of CEA, the American Society of Medical Oncology
recommends CEA levels as the gold follow-up standard after CRC
treatment (36,37). Therefore, we hypothesized that the
inclusion of both tumor markers that reflect tumor characteristics
(such as CEA and CA19-9) and NLR might be an improved way to
predict patient survival.
In the training group of the present study,
univariate and multivariate Cox analyses were performed to identify
prognostic variables, including T stage, N stage, M stage, CEA,
CA19-9 and NLR, in patients with CRC. Scores were assigned to the
patients based on the newly developed model and the patients were
subsequently categorized into the low-risk and high-risk subgroups.
The results indicated that the high-risk subgroup exhibited a
notably shorter survival time compared with the low-risk subgroup,
providing valuable suggestions for clinicians to make precise and
personalized decisions. While the individual prognostic values of
preoperative NLR, CEA and CA19-9 are well-established, the primary
clinical utility of the present study lies in integrating these
readily available biomarkers with the standard TNM staging system
into a unified, quantifiable nomogram. In clinical practice,
patients with the identical TNM stage often exhibit highly
heterogeneous survival outcomes. The present nomogram translates
complex statistical risks into an applicable tool for clinical
evaluation. Clinicians can calculate a personalized risk score for
each postoperative patient with CRC. If a patient is classified
into the high-risk subgroup by the nomogram (even if they present
with early-stage disease) clinicians might consider tailoring a
more intensive postoperative surveillance strategy and
incorporating personalized treatment plans. Furthermore, this
integrated model could provide valuable references during
multidisciplinary team discussions regarding the administration of
adjuvant chemotherapy, particularly for patients with CRC where the
benefit of chemotherapy often remains controversial (38).
In the present study, AUC and DCA were evaluated by
comparing TNM staging with PNI using column line plots. The results
showed that the nomograms had a higher C-index and a clearer
calibration curve in predicting OS compared with TNM or PNI.
The present study possesses several limitations.
Firstly, the study is retrospective and cannot avoid bias caused by
retrospective bias and follow-up compliance. Secondly, only
internal validation was used in the present study, which may lead
to overfitting of the model. Further external validation is needed
to more accurately assess the validity of the model. Thirdly, while
the model aims to serve as an intrinsic baseline prognostic tool
and includes general adjuvant therapy as a covariate, patients were
not further stratified by specific chemotherapy regimens. This
decision was made to avoid potential confounding by indication, as
the choice and intensity of subsequent treatments in the present
retrospective cohort were largely driven by the initial
pathological severity of the tumor.
In conclusion, the present study screened various
valuable blood biomarkers and clinicopathological characteristics
of patients and constructed and validated a nomogram utilizing
these factors to evaluate the inflammatory status and predict OS in
patients with CRC. The nomogram demonstrates potential enhancements
in predictive power, sensitivity and accuracy compared with the
conventional TNM staging system. As a more convenient and efficient
tool, the nomogram holds promise in assisting clinical
practitioners with informed decision-making.
Acknowledgements
Not applicable.
Funding
This work was supported by the Provincial-Level Talent Program
for National Center of Technology Innovation for Bio
Pharmaceuticals (grant no. NCTIB2024JS0101), the Suzhou Basic
Research Pilot Project (grant no. SSD2024047), the Suzhou Medical
College-QiLu Medical Research Program of Soochow University (grant
no. 24QL200103), Boxi Clinical Research The First Affiliated
Hospital of Soochow University (grant no. BXLC2024022), Prof.
Changgeng Ruan's Research and Innovation Fund for Graduate Students
of the First Affiliated Hospital of Soochow University (grant no.
RKYCX202405), Prof. Changgeng Ruan's Research and Innovation Fund
for Graduate Students of the First Affiliated Hospital of Soochow
University (grant no. RSJCX202510), the Jiangsu Province Chinese
Traditional Medicine Science and Technology Development Plan
Project (grant no. MS2025123) and the Graduate Cross-Innovation
Program Suzhou Medical College of Soochow University (grant no.
20244232055).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SH, BS, HG and JC conceived and designed the
project. ZP, QT, SW and XS collected the data. GC, BS and SH
analyzed and interpreted the data. BS and JC drafted the
manuscript. All authors read and approved the final version of the
manuscript. BS and SH confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
The study protocol was approved by the Ethics
Committee of The First Affiliated Hospital of Soochow University
(Suzhou, China; approval no. 125). Written informed consent was
obtained from all patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Riesco-Martinez MC, Modrego A,
Espinosa-Olarte P, La Salvia A and Garcia-Carbonero R:
Perioperative chemotherapy for liver metastasis of colorectal
cancer: Lessons learned and future perspectives. Curr Treat Options
Oncol. 23:1320–1337. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Panahi MH, Panahi H, Mahdavi Hezaveh A,
Mansournia MA and Bidhendi Yarandi R: Survival rate of colon and
rectum cancer in Iran: A systematic review and meta-analysis.
Neoplasma. 66:988–994. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Amin MB, Edge SB, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, et al: AJCC Cancer Staging Manual. 8th edition.
Springer; New York, NY: 2017
|
|
5
|
Liu X, Qin J, Nie J, Sun H, Pan Y and Wang
S: Reclassifying TNM stage I/II colorectal cancer into two
subgroups with different overall survival, tumor microenvironment,
and response to immune checkpoint blockade treatment. Front Genet.
13:9489202022. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Geng Y, Zhu D and Wu C, Wu J, Wang Q, Li
R, Jiang J and Wu C: A novel systemic inflammation response index
(SIRI) for predicting postoperative survival of patients with
esophageal squamous cell carcinoma. Int Immunopharmacol.
65:503–510. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kang Y, Zhu X, Lin Z, Zeng M, Shi P, Cao Y
and Chen F: Compare the diagnostic and prognostic value of MLR, NLR
and PLR in CRC patients. Clin Lab. Sep 1–2021.(Epub ahead of
print). doi: 10.7754/Clin.Lab.2021.201130. View Article : Google Scholar
|
|
8
|
Chen Y, Jiang W, Xi D, Chen J, Xu G, Yin
W, Chen J and Gu W: Development and validation of nomogram based on
SIRI for predicting the clinical outcome in patients with
nasopharyngeal carcinomas. J Investig Med. 67:691–698. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liu H, Li Z, Zhang Q, Li Q, Zhong H, Wang
Y, Yang H, Li H, Wang X, Li K, et al: Multi-institutional
development and validation of a nomogram to predict prognosis of
early-onset gastric cancer patients. Front Immunol. 13:10071762022.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li Y, Chen D, Xuan H, Dragomir MP, Calin
GA, Meng X, Chen M and Jin H: Construction and validation of
prognostic nomogram for metaplastic breast cancer. Bosn J Basic Med
Sci. 22:131–139. 2022.PubMed/NCBI
|
|
11
|
Ogunwobi OO, Mahmood F and Akingboye A:
Biomarkers in colorectal cancer: Current research and future
prospects. Int J Mol Sci. 21:53112020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sugimoto A, Fukuoka T, Shibutani M,
Kasashima H, Kitayama K, Ohira M and Maeda K: Prognostic
significance of the Naples prognostic score in colorectal cancer
patients undergoing curative resection: A propensity score matching
analysis. BMC Gastroenterol. 23:882023. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xie T, Wang X, Li M, Tong T, Yu X and Zhou
Z: Pancreatic ductal adenocarcinoma: A radiomics nomogram
outperforms clinical model and TNM staging for survival estimation
after curative resection. Eur Radiol. 30:2513–2524. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hanahan D: Hallmarks of cancer: New
dimensions. Cancer Discov. 12:31–46. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kubo H, Murayama Y, Arita T, Kuriu Y,
Nakanishi M and Otsuji E: The prognostic value of preoperative
Neutrophil-to-Lymphocyte ratio in colorectal cancer. World J Surg.
40:2796–2802. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang Y, Zhou GQ, Liu X, Chen L, Li WF,
Tang LL, Liu Q, Sun Y and Ma J: Exploration and validation of
C-Reactive Protein/Albumin ratio as a novel Inflammation-based
prognostic marker in nasopharyngeal carcinoma. J Cancer.
7:1406–1412. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Misiewicz A and Dymicka-Piekarska V:
Fashionable, but What is their real clinical usefulness? NLR, LMR,
and PLR as a promising indicator in colorectal cancer prognosis: A
systematic review. J Inflamm Res. 16:69–81. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gawiński C, Michalski W, Mróz A and
Wyrwicz L: Correlation between Lymphocyte-to-monocyte ratio (LMR),
Neutrophil-to-Lymphocyte ratio (NLR), Platelet-to-Lymphocyte ratio
(PLR) and Tumor-Infiltrating lymphocytes (TILs) in Left-sided
colorectal cancer patients. Biology (Basel). 11:3852022.PubMed/NCBI
|
|
19
|
Mahsuni Sevinc M, Riza Gunduz U, Kinaci E,
Armagan Aydin A, Bayrak S, Umar Gursu R and Gunduz S: Preoperative
neutrophil-to-lymphocyte ratio and plateletto-lymphocyte ratio as
new prognostic factors for patients with colorectal cancer. J BUON.
21:1153–1157. 2016.PubMed/NCBI
|
|
20
|
Maeda Y, Kawahara T, Koizumi M, Ito H,
Kumano Y, Ohtaka M, Kondo T, Mochizuki T, Hattori Y, Teranishi J,
et al: Lack of an association between Neutrophil-to-Lymphocyte
ratio and PSA failure of prostate cancer patients who underwent
radical prostatectomy. Biomed Res Int. 2016:61973532016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Byun SS, Hwang EC, Kang SH, Hong SH, Chung
J, Kwon TG, Kim HH, Kwak C, Kim YJ and Lee WK: Prognostic
significance of preoperative Neutrophil-to-Lymphocyte ratio in
nonmetastatic renal cell carcinoma: A large, multicenter cohort
analysis. Biomed Res Int. 2016:56341482016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Coffelt SB, Wellenstein MD and de Visser
KE: Neutrophils in cancer: Neutral no more. Nat Rev Cancer.
16:431–446. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zheng Z, Xu Y, Shi Y and Shao CL:
Neutrophils in the tumor microenvironment and their functional
modulation by mesenchymal stromal cells. Cell Immunol.
379:1045762022. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chandra R, Karalis JD, Liu C, Murimwa GZ,
Voth Park J, Heid CA, Reznik SI, Huang E, Minna JD and Brekken RA:
The colorectal cancer tumor microenvironment and its impact on
liver and lung metastasis. Cancers (Basel). 13:62062021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gijsbers K, Gouwy M, Struyf S, Wuyts A,
Proost P, Opdenakker G, Penninckx F, Ectors N, Geboes K and Van
Damme J: GCP-2/CXCL6 synergizes with other endothelial cell-derived
chemokines in neutrophil mobilization and is associated with
angiogenesis in gastrointestinal tumors. Exp Cell Res. 303:331–342.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Eck M, Schmausser B, Scheller K, Brändlein
S and Müller-Hermelink HK: Pleiotropic effects of CXC chemokines in
gastric carcinoma: Differences in CXCL8 and CXCL1 expression
between diffuse and intestinal types of gastric carcinoma. Clin Exp
Immunol. 134:508–515. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Que H, Fu Q, Lan T, Tian X and Wei X:
Tumor-associated neutrophils and neutrophil-targeted cancer
therapies. Biochim Biophys Acta Rev Cancer. 877:1887622022.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bai Z, Zhou Y, Ye Z, Xiong J, Lan H and
Wang F: Tumor-infiltrating lymphocytes in colorectal cancer: The
fundamental indication and application on immunotherapy. Front
Immunol. 12:8089642021. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Shin JS, Suh KW and Oh SY: Preoperative
neutrophil to lymphocyte ratio predicts survival in patients with
T1-2N0 colorectal cancer. J Surg Oncol. 112:654–657. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kubo T, Ono S, Ueno H, Shinto E, Yamamoto
J and Hase K: Impact of the perioperative neutrophil-to-lymphocyte
ratio on the long-term survival following an elective resection of
colorectal carcinoma. Int J Colorectal Dis. 29:1091–1099. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Friman TK, Jäämaa-Holmberg S, Åberg F,
Helanterä I, Halme M, Pentikäinen MO, Nordin A, Lemström KB,
Jahnukainen T, Räty R and Salmela B: Cancer risk and mortality
after solid organ transplantation: A population-based 30-year
cohort study in Finland. Int J Cancer. 150:1779–1791. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Slagter AE, Vollebergh MA, Caspers IA, van
Sandick JW, Sikorska K, Lind P, Nordsmark M, Putter H, Braak J,
Meershoek-Klein Kranenbarg E, et al: Prognostic value of tumor
markers and ctDNA in patients with resectable gastric cancer
receiving perioperative treatment: Results from the CRITICS trial.
Gastric Cancer. 25:401–410. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tsai PL, Su WJ, Leung WH, Lai CT and Liu
CK: Neutrophil-lymphocyte ratio, level as prognostic, predictive
factors in colorectal cancer: A systematic review and
meta-analysis. J Cancer Res Ther. 12:582–589. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Toiyama Y, Inoue Y, Saigusa S, Kawamura M,
Kawamoto A, Okugawa Y, Hiro J, Tanaka K, Mohri Y and Kusunoki M:
C-reactive protein as predictor of recurrence in patients with
rectal cancer undergoing chemoradiotherapy followed by surgery.
Anticancer Res. 33:5065–5074. 2013.PubMed/NCBI
|
|
35
|
Thirunavukarasu P, Sukumar S, Sathaiah M,
Mahan M, Pragatheeshwar KD, Pingpank JF, Zeh H III, Bartels CJ, Lee
KK and Bartlett DL: C-stage in colon cancer: Implications of
carcinoembryonic antigen biomarker in staging, prognosis, and
management. J Natl Cancer Inst. 103:689–697. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lakemeyer L, Sander S, Wittau M,
Henne-Bruns D, Kornmann M and Lemke J: Diagnostic and prognostic
value of CEA and CA19-9 in colorectal cancer. Diseases. 9:212021.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Rao H, Wu H, Huang Q, Yu Z and Zhong Z:
Clinical value of serum CEA, CA24-2 and CA19-9 in patients with
colorectal cancer. Clin Lab. Apr 1–2021.(Epub ahead of print).
View Article : Google Scholar
|
|
38
|
Baxter NN, Kennedy EB, Bergsland E, Berlin
J, George TJ, Gill S, Gold PJ, Hantel A, Jones L, Lieu C, et al:
Adjuvant therapy for stage II colon cancer: ASCO guideline update.
J Clin Oncol. 40:892–910. 2022. View Article : Google Scholar : PubMed/NCBI
|