Introduction
Juvenile localised scleroderma (JLS), known as
‘morphea’ in the dermatological literature, refers to a variety of
conditions characterised by skin thickening with increased collagen
deposition (1). The connective
tissue diseases that constiTtute JLS are rare, complex and have an
unknown etiology. Localised plaques are typically benign or
self-limiting; however, the condition may be cosmetically
disfiguring and result in permanent alopecia. JLS includes five
subtypes: Circumscribed morphoea, linear scleroderma, generalized
morphoea, pansclerotic morphoea and the mixed subtype if a
combination of two or more of the previous subtypes is present
(2). Linear lesions may progress to
invade the subcutaneous tissue, muscle and bone, leading to limb
atrophy, contracture and limb length discrepancies, thus resulting
in functional disabilities or severe cosmetic disfigurement. Early
diagnosis is critical, as early therapeutic protocols can improve
the patient's quality of life, slow disease progression and assist
with improved disease management. To date, few reports describing
cases of JLS are available in the literature, which reflects the
rarity of the condition.
Case report
A 10-year-old girl presented with an 8-month history
of white plaque at the skin of the left ala of the nose, with
subsequent painless scarring extending onto the centre of the upper
lip. A painless, pink, pitting plaque had initially appeared at the
skin of the left ala of the nose 8 months previously. The plaque
gradually expanded down through the columella nasi to the lip bead
on the centre of the labrum. The skin of the plaque also gradually
hardened and whitened. In the past 2 months, the maxillary anterior
teeth had exhibited a gradual loosening. The patient was examined
by doctors at local hospitals, but a firm diagnosis was not able to
be provided. The patient apparently looked physically healthy, and
no documented family history was available.
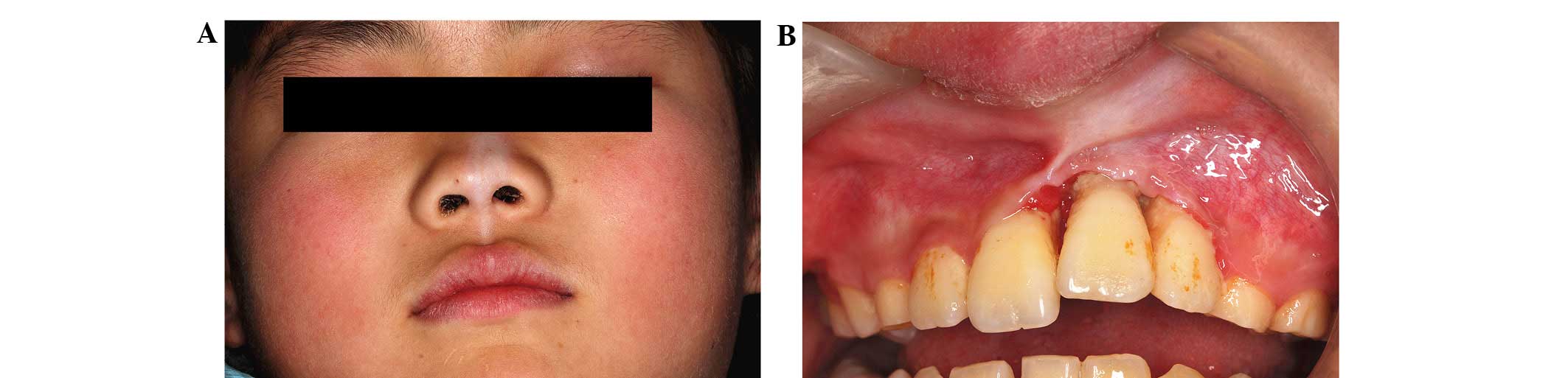
A facial examination revealed an ivory plaque
extending from the skin of the left ala of nose to the lip bead on
the centre of the upper lip. The lesion varied in width between 5
and 15 mm. The left ala of the nose was slightly concave (Fig. 1A). An intra-oral examination revealed
a white plaque extending from the centre of the upper lip mucosa to
the groove of the oral vestibule, eventually extending to the
labial gingivae attached to the left maxillary anterior tooth. The
periodontal pocket depth of the round structure of the maxillary
left central incisor and the mesial of the maxillary left lateral
incisor was 13 and 12 mm, respectively, which was deeper than that
of the opposite tooth, which had normal bone structures. The labial
gingiva of the maxillary left central incisor was eroded and shaped
like a ‘V’. The tooth mobility of the maxillary left central
incisor was degree II (Fig. 1B)
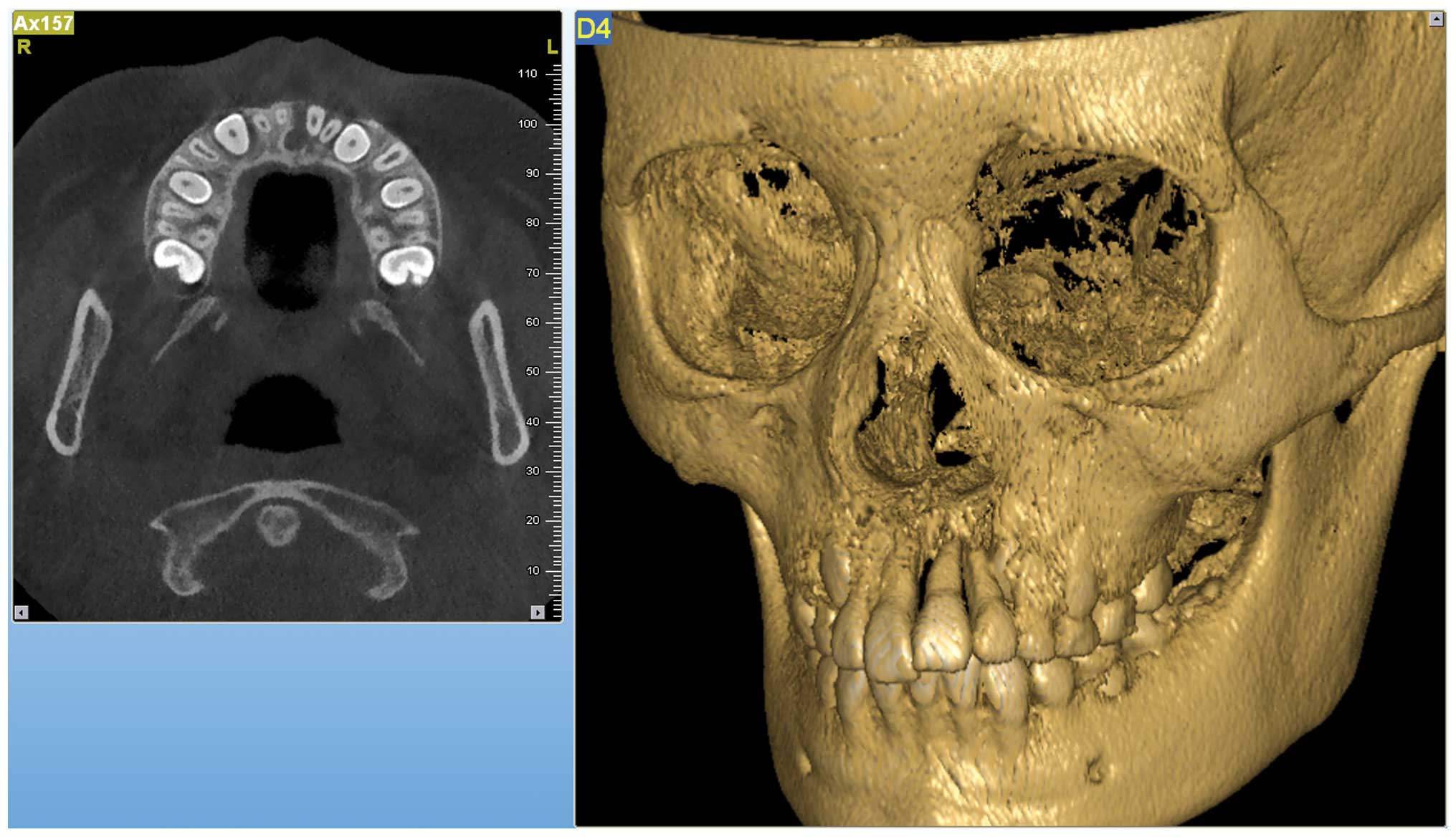
(3). An X-ray and cone beam computed
tomography revealed alveolar bone resorption between the affected
teeth (Fig. 2). Blood
investigations, including a full blood count with differential,
erythrocyte sedimentation rate, alkaline phosphatase and
antinuclear, anti-Scl-70, anti-centromere and
anti-ribonucleoprotein antibodies, were essentially normal, with
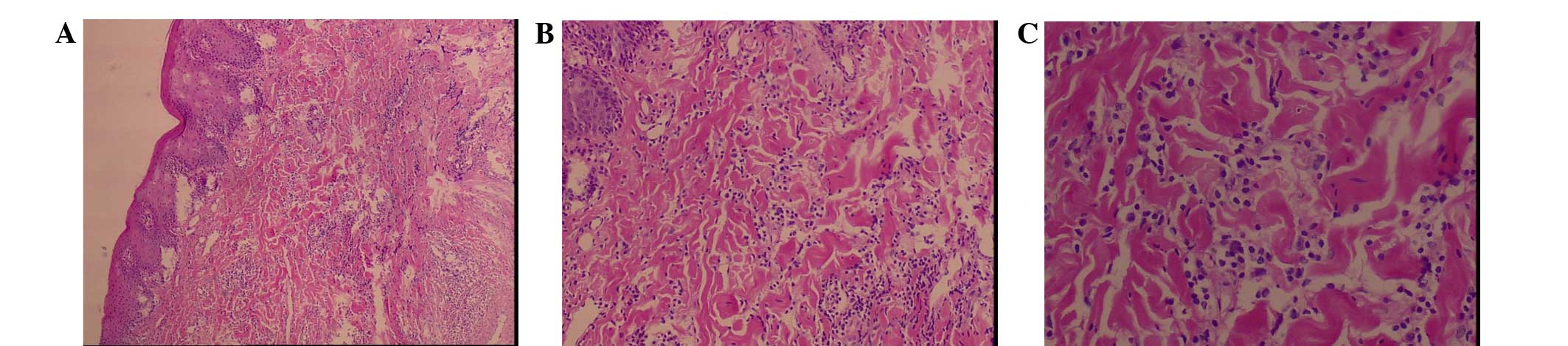
the exception of a raised rheumatoid factor level (33.7 IU/ml). A
biopsy from the labial gingivae in the region of the upper left
central incisor was found to be an irregularly thickened squamous
epithelium occupying the mucosal surface. The connective tissue
collagen under the squamous cell layer exhibited hyaline
degeneration and hardening (Fig. 3).
Excess collagen can lead to fibrosis, which is similar to scarring.
The patient was diagnosed with JLS, morphea-type, by a
dermatologist at the Affiliated Hospital of Beijing University
(Beijing, China) under remote consultation.
Glycyrrhizin capsules (Weifang Zhongshi
Pharmaceutical Co., Ltd., Weifang, China), escin (Cesra
Arzneimittel GmbH & Co. KG, Baden-Baden, Germany) and total
glucosides of paeony (Ningbo Lihua Pharmaceutical Co., Ltd.,
Ningbo, China) were prescribed to the patient in oral doses of 75
mg/day, 300 mg/day and 0.9 g/day, respectively, along with a
topical application of tacrolimus and mucopolysaccharide
polysulphate cream.
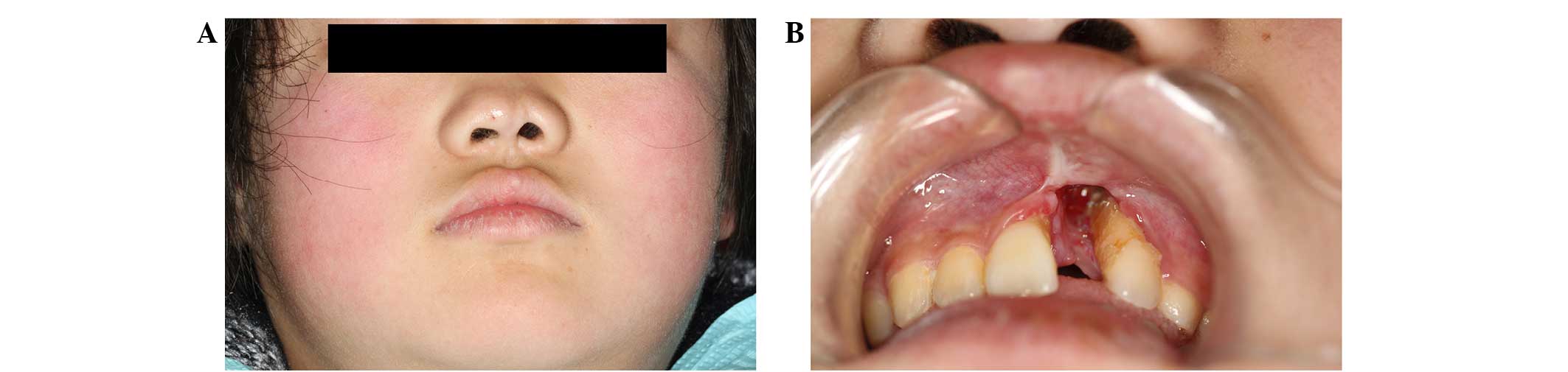
At the 6-month follow-up appointment, softening and
significant lightening of the lesion of the face (nose and upper
lip) were found (Fig. 4A), which
prevented the lesion from being noticed due to its similarity in
colour to the skin; however, no change in the healing of the mucosa
or hard tissue of the mouth was apparent. The treatment plan
included the extraction of the maxillary left central incisor,
which was impossible to preserve; however, the parents initially
refused the procedure due to the desire to preserve the tooth as
long as possible. After 2 months, the maxillary left central
incisor had to be pulled out due to mastication forces. Following
the removal of the tooth, the extraction wound did not heal or
close, even after 6 months (Fig.
4B).
Discussion
The more common subtypes of JLS include linear,
plaque and mixed linear and plaque types. The exact cause of JLS is
unknown, but a positive family history of rheumatic or autoimmune
diseases and environmental factor triggers have been implicated
(4). Similarly to other connective
tissue diseases, JLS mainly involves females aged 7–10 years, which
is consistent with previous studied (5,6).
Linear lesions can invade the subcutaneous tissue,
muscle and bone, resulting in tissue contracture and functional
disabilities or severe cosmetic disfigurement (7). In the present case, the JLS had
extended into the deep skin, involving the underlying muscle and
alveolar bone. Due to the lack of understanding regarding JLS in
clinicians who are not rheumatologists or dermatologists, this
patient did not receive an exact diagnosis or effective therapy in
the local hospital. The present case suggests that clinicians
should improve their knowledge of JLS. In this case,
histopathological examination was crucial for establishing a
definite diagnosis.
There is no standard modality of treatment for JLS.
Studies have shown that topical tacrolimus ointment can effectively
reduce the skin thickening, pigment loss, hardness, erythema,
capillary expansion and contraction (8,9).
Systemic medication with methotrexate (MTX) or combined treatment
with MTX and glucocorticoids can be taken orally. Studies have
shown that long-term MTX therapy is beneficial and well-tolerated
for JLS (10,11). In addition, photochemotherapy with
ultraviolet A in combination with the photosensitiser psoralen has
been successfully used to reduce skin fibrosis in localised
scleroderma (morphea) (12).
Glycyrrhizin and escin are well-known Chinese herbal medicines that
have been used to inhibit inflammation, oxidation and
immunoregulation. Research has shown that total glucosides of
paeony can decrease the inflammatory reaction and enhance wound and
ulcer healing (13). In the present
case, oral glycyrrhizin capsules, escin and total glucosides of
paeony were prescribed to the patient, along with a topical
application of tacrolimus and mucopolysaccharide polysulphate
cream. After 6 months of treatment, the fibrosis of the facial skin
was alleviated significantly, and the colour and hardness of the
local facial area were similar to those of the normal skin. Based
on these results, it appears that the joint application of these
three medications may be a valid alternative in the treatment of
local scleroma. There was no change, however, in the healing of the
mucosa and hard tissue of the mouth. Good oral health care is
essential for patients with scleroderma, in order to prevent
gingivitis and alveolar bone destruction. When a tooth is lost,
referral to a restorative specialist is also required. A temporary
partial denture should be used to maintain the clearance. Following
stabilization, plastic surgery can help to reshape the face, and
transplants using healthy tissue can restore the diseased tissue.
Furthermore, loss of alveolar bone should be restored by means of
bone graft, and a fixed prosthesis or an implant denture should be
used to replace the missing incisor.
Acknowledgements
The present study was supported by the ‘Taishan
Scholars’ Foundation (no. TSHW20120233) from Shandong Provincial
Government. The authors would like to thank Professor Ping Ye
(Institute of Dental Research, Centre for Oral Health, Westmead
Hospital, Sydney, Australia) for the revision of the present
manuscript.
References
|
1
|
Peterson LS, Nelson AM and Su WP:
Classification of morphea (localized scleroderma). Mayo Clin Proc.
70:1068–1076. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zulian F and Martini G: Preliminary
classification criteria for juvenile systemic sclerosis. Zulian F
and Ruperto N: Proceedings of the II Workshop on nomenclature and
diagnostic criteria for Juvenile Scleroderma Syndromes (Padua).
5–16. 2005.
|
|
3
|
Newman MG, Takei H, Klokkevoid PR and
Carranza FA: Carranzas Clinical Periodontology (11th).
Philadelphia, PA: Elsevier Saunders. 3472012.
|
|
4
|
Browning JC: Pediatric morphea. Dermatol
Clin. 31:229–237. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Murray KJ and Laxer RM: Scleroderma in
children and adolescents. Rheum Dis Clin North Am. 28:603–624.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Uziel Y, Krafchik BR, Silverman ED,
Thorner PS and Laxer RM: Localized scleroderma in childhood: A
report of 30 cases. Semin Arthritis Rheum. 23:328–340. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Laxer RM and Zulian F: Localized
scleroderma. Curr Opin Rheumatol. 18:606–613. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cantisani C, Miraglia E, Richetta AG,
Mattozzi C and Calvieri S: Generalized morphea successfully treated
with tacrolimus 0.1% ointment. J Drugs Dermatol. 12:14–15.
2013.PubMed/NCBI
|
|
9
|
Kroft EB, Groeneveld TJ, Seyger MM and de
Jong EM: Efficacy of topical tacrolimus 0.1% in active plaque
morphea: randomized, double-blind, emollient-controlled pilot
study. Am J Clin Dermatol. 10:181–187. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zulian F, Vallongo C, Patrizi A,
Belloni-Fortina A, Cutrone M, Alessio M, Martino S, Gerloni V,
Vittadello F and Martini G: A long-term follow-up study of
methotrexate in juvenile localized scleroderma (morphea). J Am Acad
Dermatol. 67:1151–1156. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Inamo Y and Ochiai T: Successful
combination treatment of a patient with progressive juvenile
localized scleroderma (morphea) using imatinib, corticosteroids,
and methotrexate. Pediatr Dermatol. 30:e191–e193. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gambichler T, Terras S and Kreuter A:
Treatment regimens, protocols, dosage and indications for UVA1
phototherapy: Facts and controversies. Clin Dermatol. 31:438–454.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jia XY, Chang Y, Sun XJ, Wu HX, Wang C, Xu
HM, Zhang L, Zhang LL, Zheng YQ, Song LH and Wei W: Total
glucosides of paeony inhibit the proliferation of fibroblast-like
synoviocytes through the regulation of G proteins in rats with
collagen-induced arthritis. Int Immunopharmacol. 18:1–6. 2014.
View Article : Google Scholar : PubMed/NCBI
|