Introduction
Neuroendocrine neoplasms (NENs), originating from
neuroendocrine cells, represent a rare heterogenic group of solid
tumors, which can be involved in hormone homeostasis via the
release of bioactive peptides (1,2).
NENs can develop in several organs and more common in the lungs,
the intestine and pancreas (1).
Depending on the primary tumor, the occurrence of metastasis,
histological grading, hormone production in case of secreting NENs
and their association with hereditary syndromes, such as multiple
endocrine neoplasia or von Hippel-Lindau syndrome, the clinical
presentation of NENs varies from asymptomatic patients to patients
with specific and non-specific symptoms (3,4).
Pancreatic NENs (pNENs) are commonly non-secreting. However, when
hormones are produced, peptides, such as insulin, glucagon,
vasoactive intestinal peptide (VIP) and pancreatic polypeptide (PP)
are the most common, eventually resulting in hormone-specific
symptoms (3,5). The treatment options for pNENs
include the surgical resection of the primary tumor, administration
of somatostatin analogues, targeted therapy with tyrosine kinase
inhibitors and the mammalian target of rapamycin (mTOR) inhibitor
everolimus, peptide-receptor radiotherapy (PRRT) and chemotherapy
in metastasized disease (6-8).
Chromogranin A (CgA) and neuron specific enolase (NSE) are the most
commonly used established biomarkers for therapy monitoring and
clinical management of patients with pNEN (9,10).
Myasthenia gravis (MG) is an autoimmune neuromuscular junction
(NMJ) disorder, which is associated with the secretion of
autoantibodies directly targeting key molecules at the NMJ,
including acetylcholine receptor (AChR) in ~85% of all patients
with MG, muscle specific kinase (MuSK), titin and LDL receptor
related protein 3 (LRP3) (11-13).
In ~10% of patients with MG no autoantibodies are detected
(seronegative MG) (12). It has
been reported that in AChR antibody-positive MG, the thymus affects
the development of autoreactive T cells targeting AChR and the
induction of AChR-antibody producing B cells, which are involved in
the symptoms of MG (13,14). Therefore, in the majority of cases,
MG is associated with thymic pathologies, such as thymoma or thymic
hyperplasia. Less frequent other autoimmune diseases, such as
thyroiditis, lupus erythematosus, rheumatic arthritis and
hematologic neoplasia are also associated with MG (15,16).
Previous studies also demonstrated that several MG cases were
associated with extrathymic solid tumors, while the association
between MG and pNEN has only been described in three cases
worldwide (17-20).
The clinical presentation of ocular MG (OMG) commonly includes
weakness of the extraorbital muscle, accompanied by fluctuating
ptosis and diplopia (21). A
previous study also showed that generalization of MG could lead to
exercise-induced fatigue and muscle weakness in 50-60% of MG cases
within the first two years (21).
Therapy schemes for OMG include symptomatic treatment with
acetylcholine esterase inhibition, long-term immunosuppression for
generalized MG and thymectomy in younger adults with thymic
pathologies (22,23).
Case presentation
The present study presents a case of a 76-year-old
patient with a history of age-related macular degeneration was
presented. Physical examination at the Ophthalmologic Department of
University Hospital Tuebingen revealed an asymmetric ptosis of the
left eye and an anamnestic progressive weakness of the left eyelid
over the course of one week. Besides recurrent thromboembolic
events in the past, treated by anticoagulation with rivaroxaban, no
underlying diseases were detected. The initial cerebral computed
tomography (CT) and magnetic resonance imaging (MRI) scan revealed
no evidence of thromboembolic events. In addition, no endocardial
thromboembolic vegetations or persistent foramen ovale were
diagnosed. Interestingly, during the Simpson's test, accentuating
ptosis in upward gaze (after one minute), as well as horizontal
non-exhaustive nystagmus of the left eye in leftward gaze were
observed. The patient showed no signs of muscle weakness or
autonomic dysfunction. Deep tendon reflexes were within normal
ranges. Further neurological examination, including
electrophysiological testing (ENG) of facial nerve/orbicularis
oculi muscle showed a significant decrement in low frequency
repetitive nerve stimulation, thus indicating a neuromuscular
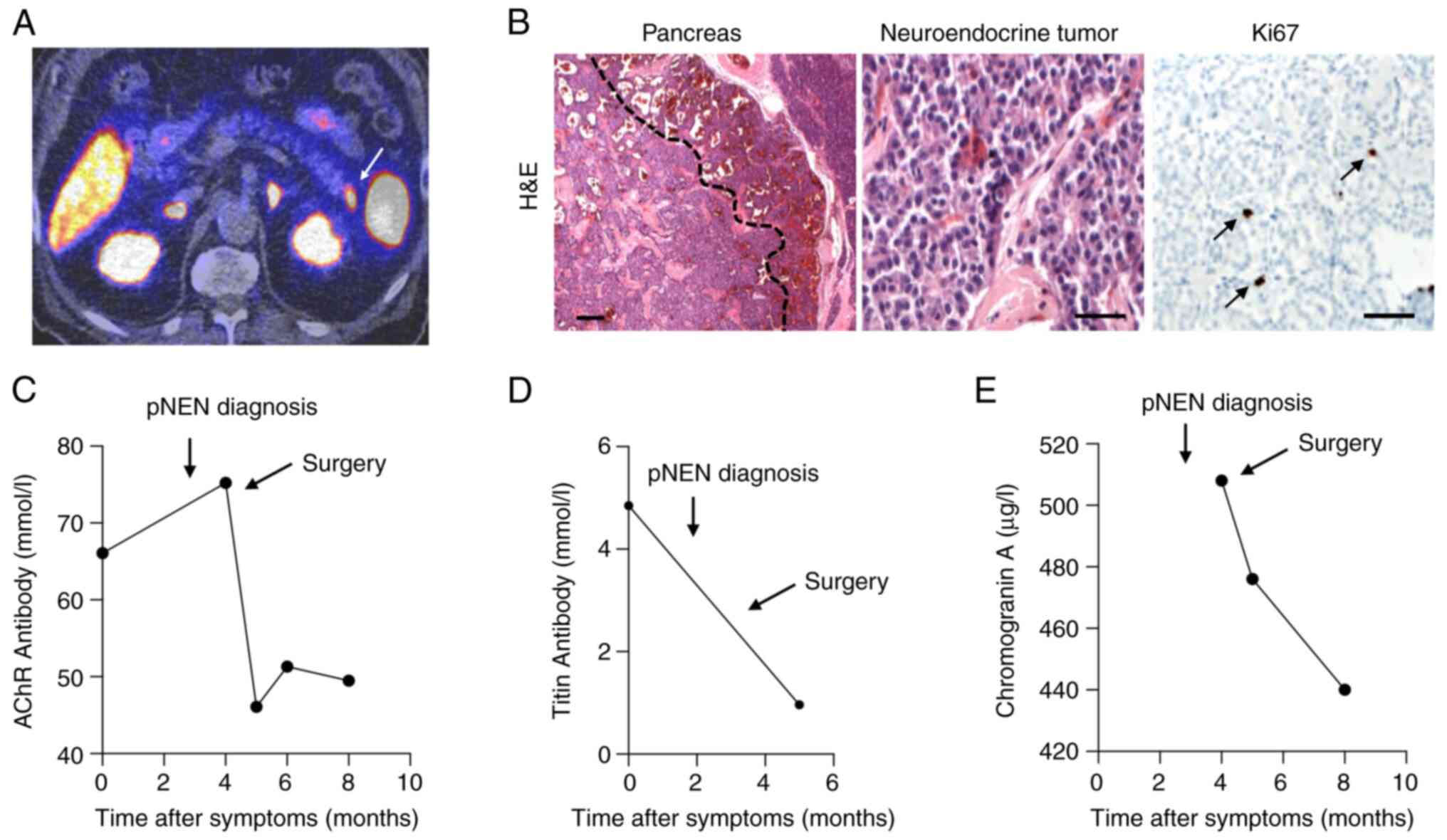
transmission defect (Table I). In
addition, serological tests revealed high levels of anti-AChR
autoantibodies (66 nmol/l) and the presence of anti-titin
antibodies (Fig. 1C and D), supporting the diagnosis of OMG.
 | Table IElectroneurography of repetitive
facial nerve stimulation at first diagnosis. |
Table I
Electroneurography of repetitive
facial nerve stimulation at first diagnosis.
| 3 Hz frequency
stimulation (facial nerve/left orbicularis oculi muscle) | Amplitude CMAP 1 vs.
5 (%) |
|---|
| Decrement prior to
stimulation | -14.2 |
| Decrement 5 sec after
muscle stimulation (duration, 60 sec) | -23.8 |
| Decrement 1 min after
muscle stimulation (duration, 60 sec) | -14.8 |
| Decrement 3 min after
muscle stimulation (duration, 60 sec) | -22.1 |
After starting a symptomatic treatment with
pyridostigmine (180 mg/daily), the patient underwent diagnostic
tests for thymic pathologies, autoimmune diseases and malignant
neoplasms. A CT scan showed a 11x9-mm lesion in the pancreatic
cauda. At three weeks after initial presentation, the patient
reported progressive diplopia, difficulty in maintaining head
posture, as well as progressive weakening of the limbs.
Furthermore, dysarthria worsened throughout the day. Therefore, the
patient was treated with an additional immunosuppressive therapy
with 500 mg/three days methylprednisolone (following gradually
reduction) and azathioprine (2 mg/kg/day). Following further
escalation of the pyridostigmine dose (220 mg/daily), the
progressive symptoms declined. Furthermore, the somatostatin
receptor (SSR)/positron emission tomography (PET)/computed
tomography (CT) scan showed that the lesion in the pancreas
intensively expressed SSR (Fig.
1A; indicated by arrow). However, extrapancreatic lesions were
not identified. Interestingly, the levels of CgA (Fig. 1E) and NSE were moderately elevated,
with values of 508 µg/l and 13 µg/l, respectively. However, the
serum levels of the bioactive peptides, insulin, gastrin, glucagon,
VIP and PP, and the urine levels of 5-hydroxy-indole acetic acid
(5-HIAA) were within physiological ranges. Therefore, the
SSR-positive pancreatic tumor was surgically resected. The
histopathology results revealed a neuroendocrine tumor of 1.3 cm in
diameter with a proliferation rate (Ki67 staining) of 0.7%
(Fig. 1B). The initial tumor stage
was pT1 pN0 cM0 L0 V0 Pn0 R0 G1.
After the surgical resection, the patient
experienced a myasthenic crisis with worsening dyspnea. Therefore,
the patient received symptomatic treatment that required
pyridostigmine dose escalation, combined with neostigmine perfusion
and a 5-day course of intravenous immunoglobulins (0.4 mg/kg body
weight). Following three days of intensive care monitoring, the
patient rapidly improved. Of note, the anti-myasthenic therapy was
continued with pyridostigmine and azathioprine. Post-interventional
SSR/PET/CT scan did not display any SSR-positive lesions.
Furthermore, the clinical symptoms in terms of ptosis and
dysarthria improved quickly. At three months after the surgical
resection, the patient showed no residual symptoms. Additionally,
the antibody titers, as well as the levels of the tumor marker CgA
were steeply declined immediately after surgery (Fig. 1C-E).
Discussion
In the present case report the patient was diagnosed
with MG based on the typical clinical presentation of fluctuating
oculo-bulbar weakness, elevated anti-AChR antibody titer and
neurophysiological tests. The response to myasthenic therapy with
pyridostigmine and immunosuppression led to the diagnosis of MG
over other NMJ diseases, such as the Lambert-Eaton myasthenic
syndrome (LEMS). However, the differentiation between MG and LEMS
proves to be challenging, since several coexisting and overlapping
syndromes have been reported in the literature (24,25).
The majority of neuroendocrine neoplasms of the
pancreas are non-secreting and patients are often asymptomatic or
present with unspecific clinical symptoms (26). This poses a limiting factor for
timely diagnosis and, therefore, tumors are usually diagnosed at
advanced stages (26).
The present study reported a rare case of late-onset
MG, which led to the early diagnosis of an underlying pancreatic
malignancy. Due to early diagnosis and lack of metastasis, the
effective treatment of the pNEN by surgical resection was
possible.
Furthermore, the underlying diseases of MG are
commonly thymic pathologies or autoimmune diseases, and
significantly less often, extrathymic solid tumors (15-18).
With the increasing improvement of the diagnostic approaches, the
presence of extrathymic malignancies should be sought in all
patients with MG without evidence of thymic pathology or autoimmune
diseases.
Furthermore, ~90% of MG cases are seropositive, thus
indicating that autoantibodies, such as anti-AChR or anti-titin,
are detectable in the blood serum of patients (11-13).
The present study detected anti-AChR antibodies, which were
significantly reduced after the surgical resection of the pNEN.
Therefore, anti-AChR antibodies, combined with established tumor
markers in NENs, such as CgA and NSE, could be prospectively
considered as additional biomarkers in patients with NENs and
seropositive MG. However, there is currently no other available
evidence to support this hypothesis.
Paraneoplastic MG may often lead to a distinctive
clinical pattern characterized by more severe demonstration and
commonly involves bulbar, respiratory and neck muscles (27), as shown in the current case.
Paraneoplastic syndromes are associated with substances secreted by
the tumor. However, these substances are not directly specific to
their tissue of origin (28). The
surgical resection of the pNEN improved the clinical symptoms and
notably attenuated the titers of anti-AChR antibodies in the
present study. Therefore, the therapy of the underlying diseases
should also be considered when planning the treatment approach for
MG.
In conclusion, the present case study reported a
rare case of MG as an initial paraneoplastic syndrome associated
with pNEN. The early diagnosis of both pNEN and MG enabled the
curative targeted treatment of the tumor and led to the efficient
treatment of MG. In addition to early diagnosis, monitoring of the
paraneoplastic syndrome could be a useful tool to manage the
clinical course and treatment response of the underlying neoplasm.
Since the efficient treatment of NENs is instrumental in achieving
a complete remission of MG, screening for rare neuroendocrine
malignancies, including pNEN, could be considered in the diagnostic
evaluation.
Acknowledgements
The authors wish to thank the study nurses Mrs
Kristina MacMillan, Mrs Simone Braun and Mrs Ines Hildebrand of the
Center for Neuroendocrine Tumors Tuebingen (Tuebingen, Germany) for
their assistance in conducting various investigations and
collecting medical findings.
Funding
Funding: The present study was funded by the German Research
Foundation under Germany's Excellence Strategy (grant no. EXC
2180-390900677).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CH and MHi conceived and designed the study. ES, JD,
PB, DN, SS, MHo, UML and LZ analyzed the patient data and medical
records. ES, PB, CH and MHi analyzed the data. ES and MHi confirm
the authenticity of all the raw data. ES, CH and MHi prepared the
figure. ES, JD, CH and MHi wrote the first draft of the manuscript.
CH and MHi contributed to the interpretation of the data and edited
the manuscript. All authors critically reviewed the manuscript. All
authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present case study was performed in accordance
with the Declaration of Helsinki. The patient provided written
informed consent.
Patient consent for publication
The patient provided their consent for the
publication of their data.
Competing interest
The authors declare that they have no competing
interests.
References
|
1
|
Perren A, Couvelard A, Scoazec JY, Costa
F, Borbath I, Delle Fave G, Gorbounova V, Gross D, Grossma A, Jense
RT, et al: ENETS consensus guidelines for the standards of care in
neuroendocrine tumors: Pathology: Diagnosis and prognostic
stratification. Neuroendocrinology. 105:196–200. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rickman DS, Beltran H, Demichelis F and
Rubin MA: Biology and evolution of poorly differentiated
neuroendocrine tumors. Nat Med. 23:1–10. 2017.PubMed/NCBI View
Article : Google Scholar
|
|
3
|
Cives M and Strosberg JR:
Gastroenteropancreatic neuroendocrine tumors. CA Cancer J Clin.
68:471–487. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Soczomski P, Jurecka-Lubieniecka B,
Krzywon A, Cortez AJ, Zgliczynski S, Rogozik N, Oczko-Wojciechowska
M, Pawlaczek A, Bednarczuk T and Jarzab B: A direct comparison of
patients with hereditary and sporadic pancreatic neuroendocrine
tumors: Evaluation of clinical course, prognostic factors and
genotype-phenotype correlations. Front Endocrinol (Lausanne).
12(681013)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Guilmette JM and Nosé V: Neoplasms of the
neuroendocrine pancreas: An update in the classification,
definition, and molecular genetic advances. Adv Anat Pathol.
26:13–30. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Krug S, Schrader J and Rinke A: Updates on
Diagnostic and therapeutic management of gastrointestinal and
pancreatic NET. Cancers (Basel). 14(2628)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kurita Y, Kobayashi N, Hara K, Mizuno N,
Kuwahara T, Okuno N, Haba S, Tokuhisa M, Hasegawa S, Kubota K, et
al: Clinical outcomes of everolimus rechallenge in patients with
pancreatic neuroendocrine neoplasms with no other treatment
options. Cancers (Basel). 14(5669)2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Camus B, Cottereau AS, Palmieri LJ,
Dermine S, Tenenbaum F, Brezault C and Coriat R: Indications of
peptide receptor radionuclide therapy (PRRT) in
gastroenteropancreatic and pulmonary neuroendocrine tumors: An
updated review. J Clin Med. 10(1267)2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yu F, Fu J, Zhang C, Wu W, Ai S, Yao X,
Meng Q, Huang Y, Lu G, Wang F and Qu W: Use of chromogranin a for
monitoring patients with pancreatic neuroendocrine neoplasms.
Pancreas. 50:882–889. 2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fuksiewicz M, Kowalska M,
Kolasinska-Cwikla A and Kotowicz B: Serum levels of neuron-specific
enolase as a prognostic factor for disease progression in patients
with GET/NEN in the pancreas and the small intestine. Endocr
Connect. 11(e210647)2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Koneczny I and Herbst R: Myasthenia
gravis: Pathogenic effects of autoantibodies on neuromuscular
architecture. Cells. 8(671)2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Lazaridis K and Tzartos SJ: Myasthenia
gravis: Autoantibody specificities and their role in MG management.
Front Neurol. 11(596981)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Lazaridis K and Tzartos SJ: Autoantibody
specificities in myasthenia gravis; Implications for improved
diagnostics and therapeutics. Front Immunol. 11(212)2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Yi JS, Guptill JT, Stathopoulos P, Nowak
RJ and O'Connor KC: B cells in the pathophysiology of myasthenia
gravis. Muscle Nerve. 57:172–184. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Shelly S, Agmon-Levin N, Altman A and
Shoenfeld Y: Thymoma and autoimmunity. Cell Mol Immunol. 8:199–202.
2011.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ali M, Riad M, Adhikari P, Bhattarai S,
Gupta A, Ali E and Mostafa JA: Association between myasthenia
gravis and systemic lupus erythematosus as a comorbid state.
Cureus. 13(e14719)2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Tanovska N, Novotni G, Sazdova-Burneska S,
Kuzmanovski I, Boshkovski B, Kondov G, Jovanovski-Srceva M,
Kokareva A and Isjanovska R: Myasthenia gravis and associated
diseases. Open Access Maced J Med Sci. 6:472–478. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Verwijst J, Westerberg E and Punga AR:
Cancer in myasthenia gravis subtypes in relation to
immunosuppressive treatment and acetylcholine receptor antibodies:
A Swedish nationwide register study. Eur J Neurol. 28:1706–1715.
2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Hermans MA, Stelten BM, Haak HR, de Herder
WW and Dercksen MW: Two patients with a neuroendocrine tumour of
the small intestine and paraneoplastic myasthenia gravis.
Endocrinol Diabetes Metab Case Rep. 2014(140013)2014.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Gay SA and Nawras SA: Myasthenia gravis
with coexisting primary pancreatic neuroendocrine tumor in a young
female patient. Am J Gastroenterol. 106(S235)2011.
|
|
21
|
Wong SH, Huda S, Vincent A and Plant GT:
Ocular myasthenia gravis: Controversies and updates. Curr Neurol
Neurosci Rep. 14(421)2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Alhaidar MK, Abumurad S, Soliven B and
Rezania K: Current treatment of myasthenia gravis. J Clin Med.
11(1597)2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Farrugia ME and Goodfellow JA: A practical
approach to managing patients with myasthenia gravis-opinions and a
review of the literature. Front Neurol. 11(604)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kim JA, Lim YM, Jang EH and Kim KK: A
patient with coexisting myasthenia gravis and lambert-eaton
myasthenic syndrome. J Clin Neurol. 8:235–237. 2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Oh SJ: Myasthenia gravis Lambert-Eaton
overlap syndrome. Muscle Nerve. 53:20–26. 2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Falconi M, Eriksson B, Kaltsas G, Bartsch
DK, Capdevila J, Caplin M, Kos-Kudla B, Kwekkeboom D, Rindi G,
Klöppel G, et al: ENETS consensus guidelines update for the
management of patients with functional pancreatic neuroendocrine
tumors and non-functional pancreatic neuroendocrine tumors.
Neuroendocrinology. 103:153–171. 2016.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Skeie GO and Romi F: Paraneoplastic
myasthenia gravis: Immunological and clinical aspects. Eur J
Neurol. 15:1029–1033. 2008.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Graus F, Delattre JY, Antoine JC, Dalmau
J, Giometto B, Grisold W, Honnorat J, Smitt PS, Vedeler Ch,
Verschuuren JJ, et al: Recommended diagnostic criteria for
paraneoplastic neurological syndromes. J Neurol Neurosurg
Psychiatry. 75:1135–1140. 2004.PubMed/NCBI View Article : Google Scholar
|