Population aging is becoming a difficult problem
faced by all countries worldwide, with the gradual improvement of
living standards, life expectancy increases, which implies an
increase in age-related diseases (1,2).
Alzheimer's disease (AD) is one of the biggest obstacles to coping
with a healthy aging population. AD is defined by the World Health
Organization (WHO) as a neurodegenerative disease of unknown
etiology, characterized by progressive deterioration of memory and
cognitive function, accounting for 50-75% of all dementia cases
(3,4). AD may present with clinical symptoms
such as progressive memory loss, impaired executive function,
difficulty in daily activities, altered thought and behavior
patterns and impaired language function (5). A total of two clinical manifestations
of AD are mainly recognized by the academic community: Senile
plaques composed of β amyloid (Aβ) and neurofibrillary tangles
composed of tau proteins with hyperphosphorylation (6). This series of processes slowly
deprives the patient of memory and cognitive ability, and the
patient gradually forgets recent events. The patient is unable to
analyze, think and judge the events, and finds it difficult to deal
with complex problems. Patients are unable to take care of
themselves in daily life, making them and their family helpless
over time (7,8). Although the exact process by which AD
molecular cascades are triggered remains unclear, a series of
epidemiological studies suggest that comorbid risk factors for
metabolic disease are crucial in the pathogenesis of this disease
(9-11).
This suggests that physicians also associate metabolic disease with
AD.
In the early nineties, some investigators noticed
common mechanistic features between metabolic diseases and AD, and
proposed the concept of type 3 diabetes (12-14).
Researchers focused on close links between diabetes mellitus (DM)
and AD, such as insulin, insulin-like growth factor, oxidative
stress, glycogen synthase kinase 3β, Aβ and tau
hyperphosphorylation (15-17).
Since then, several studies have been carried out worldwide to
explore possible links between metabolic diseases and AD, and to
turn attention to AD as a type 3 diabetes; therefore, new
therapeutic options for AD are explored from the perspective of
metabolic disease (13,18,19).
In light of recent research, it has become increasingly apparent
that AD and various metabolic diseases exhibit numerous common
characteristics.
However, the mechanism by which metabolic diseases
affect the progression of AD remains unclear and the selection of
therapeutic drugs and animal models for AD remains to be further
discussed. Moreover, the relevant literature has not been fully
reviewed at present. In the present study, using ‘Alzheimer's
disease’, ‘metabolic disease’, ‘obesity’, ‘hypercholesterolemia’
and ‘animal model’ as keywords, four electronic databases such as
Springer (https://link.springer.com/), PUBMED
(https://pubmed.ncbi.nlm.nih.gov/),
ScienceDirect (https://www.sciencedirect.com/search) and Wiley
(https://onlinelibrary.wiley.com/), were
searched for relevant literature. The present article
systematically discusses the research progress of metabolic
diseases and the pathogenesis of AD, and summarizes the different
roles of animal models in AD research, to provide a reference for
researchers (for the use of acronyms see Table I).
DM is the most common metabolic disorder and the
direct cause of its occurrence is usually due to defective insulin
action or insufficient insulin secretion (20,21).
Several real-world clinical cases suggest that brain-related mild
cognitive impairment complications in diabetes may lead to
cognitive deficits, which gradually develops into AD (22,23).
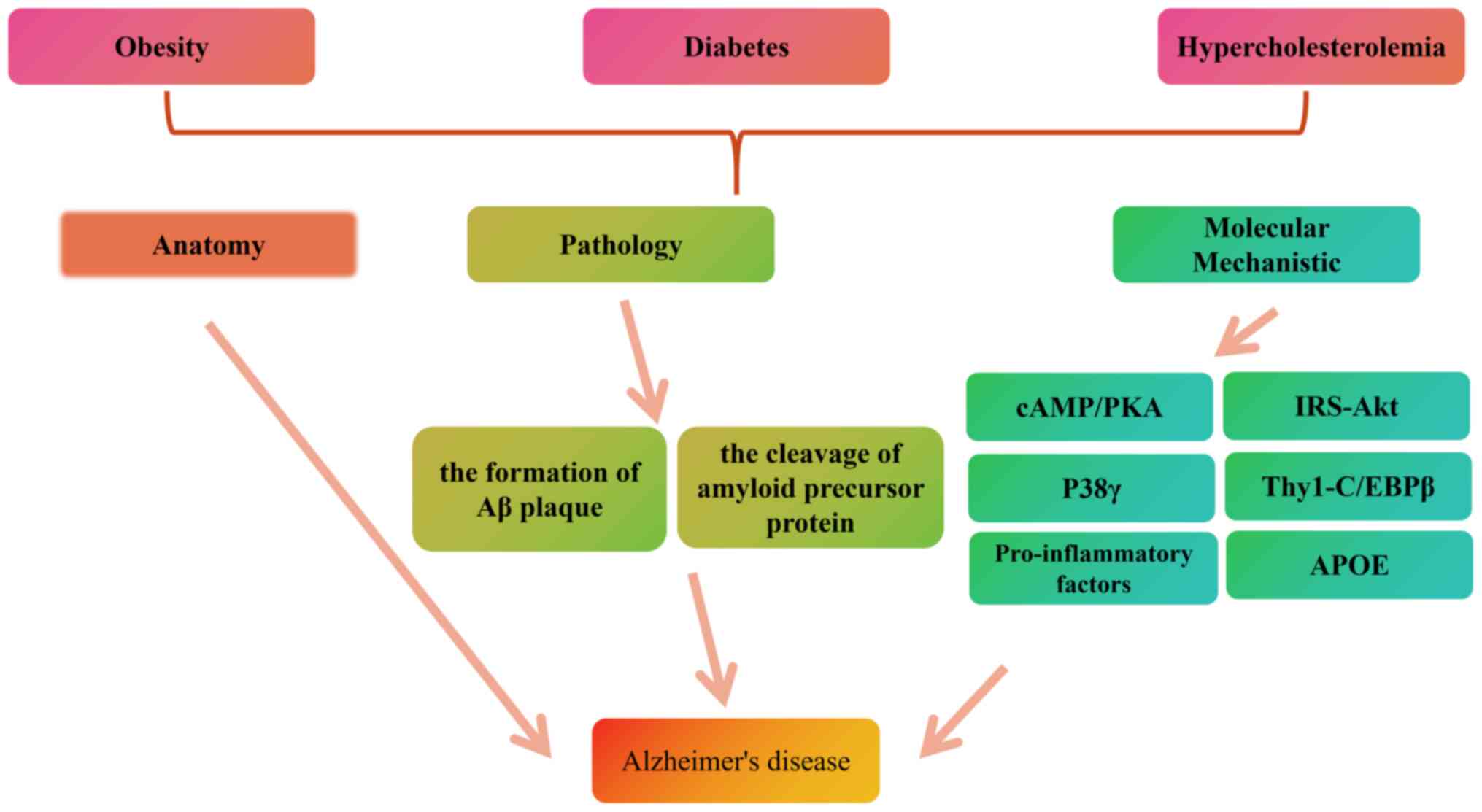
To date, several groups have focused on exploring
and explaining the link between DM and AD. Based on anatomy, some
parameters showed that the Alzheimer-like pathology of diabetic
rats is increased; these parameters include increased levels of Aβ
plaques in the hippocampus and frontal cortex, reduced hippocampal
volume, reduced protein levels in the cerebral cortex and reduced
dendritic spine density in diabetic animals (24,25).
Similarly, clinical evidence suggests that amygdala and hippocampal
volumes in patients with diabetes are altered compared with normal
patients, with a trend toward decline (26).
From a pathological perspective, the cleavage of
amyloid precursor protein (APP) and the formation of Aβ plaque
requires the involvement of β-secretase, which also regulates the
cleavage of insulin receptor, this strengthens the link between AD
and diabetes mellitus (27,28).
Furthermore, soluble (s)APPβ, a product of β-secretase, is a major
determinant of insulin resistance (29). Glycotoxicity can lead to structural
and functional damage of brain cells and nerves, cerebral vascular
hemorrhage and increased β-amyloid protein accumulation (30). These are potential mechanisms of
diabetes-related dementia.
From a molecular mechanistic perspective, it has
been suggested that the protein kinase A system (cAMP/PKA)
signaling pathway and insulin-degrading enzyme may contribute to
the type 2 diabetes-accelerated AD pathological process by causing
Aβ accumulation and neuronal apoptosis (31). In addition, studies focused on
protein phosphorylation have demonstrated that overexpression of
protein kinase Cα (PKCα) is associated with insulin signaling
interfering with insulin receptor substrate (IRS)-1 and Akt
phosphorylation in skeletal muscles (32-34).
PKCα inhibits insulin signaling through the IRS-Akt pathway, and
inhibition and silencing of PKC-α enhances insulin sensitivity by
increasing GLUT-4 translocation to the plasma membrane and glucose
uptake (32). The aforementioned
results demonstrate the role of PKCα in regulating neuronal insulin
resistance and diabetes and open new avenues for the treatment of
metabolic disorders and neurodegeneration (34). P38γ signal transduction is
characterized by its unique reciprocal regulation of the
phosphatase protein tyrosine phosphatase H1 antibody, and by its
direct binding to promoter DNA, which is also involved in the
pathogenesis of diabetes and AD, suggesting its potential as a
therapeutic target (35).
Several prospective trials have used sodium-glucose
co-transporter-2 (SGLT2) inhibitors (is) as an anti-diabetic drug
(36,37). Inhibition of SGLT2, which accounts
for ~90% of glucose reabsorption, leads to a significant reduction
in blood glucose levels (36). The
activation of insulin signaling associated with neuronal survival,
in particular the canonical pathway of Nev (pIR, pY-IRS-1, Pakt),
has been demonstrated (36). In
addition, brain magnetic resonance spectroscopy has been used to
detect decreased concentrations of the excitatory neurotransmitter
glutamate and its precursor glutamine after administration, given
that glutamate excitotoxicity has been consistently associated with
AD pathology (37). These findings
may inspire the reuse of anti-diabetic drugs (such as SGLT2is) in
AD and other related diseases characterized by downregulation of
IGF-1/insulin signaling and excitotoxicity in neurons (37). Thus, several studies conducted in
this direction have shown a link between diabetes and AD (36,37),
and more links between these two diseases remain to be
explored.
Obesity refers to a state of being overweight or
obese, often caused by excessive accumulation of fat in the body,
and is closely associated with cognitive impairment and AD
(38-41).
Body mass index (BMI) is the most common measure of obesity
worldwide. BMI is calculated as weight (kg) divided by height
(m2) squared. Obesity is defined as BMI ≥30
kg/m2 (42,43). However, BMI does not represent
regional fat distribution, which varies by sex, age, ethnicity and
residential area (44). Regional
fat distribution may have different effects on cognitive decline
and AD-related brain changes (45). However, different regions of the
fat pool may have different cognitive outcomes and have different
effects on the brain.
To date, several groups have focused on exploring
and explaining the link between obesity and AD. The authors
classify fat as visceral adipose tissue (VAT) and subcutaneous
adipose tissue (SAT). Hepatic fat in VAT and non-alcoholic
steatosis (NAFLD) is the most studied regional fat (46). Researcher has used MRI and
functional MRI for structural brain measurements to assess the
strong association between obesity and brain changes in different
regions (47). A study has
demonstrated that increased VAT is associated with decreased grey
matter density and cognitive function and that such a relationship
is age-dependent (48). For
patients with NAFLD, hepatic fat deposits are significantly
associated with smaller overall brain volumes as well as smaller
cingulate and hippocampal volumes (49). Even after weight loss, NAFLD is
still associated with smaller total brain volume (50). Structural measures indicate that
higher VAT and SAT are associated with smaller total brain volumes
(51). Elevated VAT is associated
with cortical thinning, particularly with decreased hippocampal
volume (52). The aforementioned
study showed that higher VAT is associated with higher brain
network damage in cognitive decline, suggesting a strong link
between VAT and accelerated brain ageing.
From a pathological point of view, existing
experimental results compare individuals with higher VAT metabolism
(higher metabolic capacity of visceral adipose tissue) with
individuals with lower VAT metabolism (lower metabolic capacity of
visceral adipose tissue) (53,54).
Individuals with higher VAT metabolism have been found to exhibit
higher brain Aβ levels, suggesting a close relationship between VAT
dysfunction and AD disease development (53). In addition, another study using
brain 18F-fludeoxyglucose positron emission tomography (PET) as a
neurodegenerative biomarker of AD yielded the same results
(54).
Analyzed from a possible molecular mechanism
standpoint, potential factors related to brain changes and
cognition may be explained by the release of different secretory
factors from different fat deposits (55,56).
These different fat deposits release different secreted factors
that can cross the blood-brain barrier (BBB) and cause damage,
increase cognitive impairment and accelerate AD progression
(55). Pro-inflammatory factors
secreted by adipocytes, such as leptin, IL-6 and TNF-α, can cross
the BBB and lead to neuroinflammation, thus playing a role in
cognitive impairment and AD (56).
Another study showed that a high-fat diet stimulates diabetes and
insulin resistance in Thy1-C/EBPβ transgenic (TG) mice, with
significant Aβ accumulation and hyperphosphorylation of Tau protein
in the brain, triggering cognitive impairment (57). A study investigated the
anti-inflammatory effects of M. parviflora leaf
hydroalcoholic extract (MpHE) on obese mice with AD, showing that
MpHE effectively reduces astrocyte proliferation, the presence of
insoluble Aβ peptides in the hippocampus and spatial learning
impairment in lean and obese 5XFAD mice (57). Furthermore, a study investigated
the association between AD and obesity from the perspective of the
gut microbiota. Endogenous melatonin reduction can cause systemic
changes mediated by dysbiosis of the gut microbiota, which may be
one of the causative factors of AD and obesity (58). Thus, several studies in this
direction demonstrate a link between obesity and AD, and more links
between these two diseases remain to be explored.
Familial hypercholesterolemia is a particularly
severe type of hyperlipidemia. The clinical features were
hypercholesterolemia, characteristic xanthoma and family history of
early-onset cardiovascular disease (59). Patients have abnormally high levels
of low-density lipoprotein (LDL) cholesterol, which is 4-6 times
higher in patients with homozygous LDL cholesterol compared with in
normal individuals (60). Animal
studies showed that diet-induced hypercholesterolemia increases the
accumulation of Aβ and accelerates the pathological process of AD
(61).
To date, several research groups have focused on
exploring and explaining the association between
hypercholesterolemia and AD. The researchers used fludeoxyglucose
(18F) PET to study different populations, revealing common
anatomical structures between individuals at risk for
hypercholesterolemia and AD (62-65).
The analysis showed that higher serum total cholesterol levels are
associated with lower bilateral CMRgl in areas of the anterior
cuneiform, parietal-temporal and prefrontal lobes previously found
to be preferentially affected by AD, as well as other frontal
regions previously found to be preferentially affected by normal
aging (65). In certain brain
regions affected by AD, the association is greater in
apolipoprotein E (APOE)-4 carriers compared with in non-carriers
(66). A study showed that higher
serum total cholesterol levels in middle age would accelerate brain
processes associated with normal aging and act in concert with
other risk factors for AD predisposition (67).
The APOE gene is the strongest genetic risk factor
for AD, accounting for 60-80% of all dementia cases (68,69).
APOE plays an important role in lipid transport and metabolism,
accounting for ~7% of phenotypic variation in serum total
cholesterol and 14% of polygenic variation (68). APOE also contributes ~1-8.3% of
phenotypic variation and 16% of genetic variation in LDL
cholesterol (70). Compared with
non-carriers, APOE4 carriers tend to have higher total and LDL
cholesterol as well as lower HDL cholesterol levels (71). Furthermore, higher levels of total
and LDL cholesterol are associated with greater deposition of
neuropathological markers of AD in the cerebrum (72). Given that lipids in APOE4 carriers
are most sensitive to diet, these findings suggested that lipid
management through dietary adjustment can reduce AD risk (73). Menopause itself is associated with
a more adverse lipid profile compared with premenopause, especially
for APOE3 and APOE4 carriers. Furthermore, APOE4-related AD risk is
stronger in females compared with in males (74).
A reasonable mechanism by which diet and lipids may
contribute to dementia pathology is by altering levels of
oxymethanol, the oxidized product of cholesterol (75). Dyslipidemia and dietary cholesterol
intake may result in unbalanced oxidant levels, which appear to
result in an unbalanced oxidative type of reduction (75). Studies in mice further support the
possibility of reducing AD risk through dietary adjustment. For
example, mice fed with a high-cholesterol diet subsequently have
higher levels of total cholesterol in plasma and Aβ protein in the
brain compared with controls (76). Similarly, a high-fat diet results
in greater Aβ deposition and impaired neuroinflammation,
sensorimotor function and social interaction, as well as a tendency
for APP/PS1 mice to have poorer short-term memory compared with
mice fed a control diet, but this trend was not significant
(77). Thus, several studies
conducted in this direction showed a link between
hypercholesterolemia and AD, and more links between these two
diseases remain to be explored.
To find effective therapeutic measures, researchers
construct different animal models based on pathogenesis, but
different animal models of AD have different advantages and
disadvantages (76,77).
Human beings and animals have great similarities in
physiology and pathology. It is a common research method to
simulate disease in animals to explore its biological mechanism. In
the research history of AD, common AD model-making animals include
Caenorhabditis elegans, Drosophila melanogaster, zebrafish,
mice, rats, dogs, rhesus monkeys and chimpanzees, among others
(78,79).
These experimental animals differ in species and
conditions, each with different strengths and weaknesses. For
Caenorhabditis elegans, Drosophila melanogaster and
zebrafish, their small size and short life span make them
convenient for researchers to reproduce and manipulate, but their
brain structures differ considerably from those of humans and lack
high-level cognitive behavior (80,81).
For rhesus monkeys and chimpanzees, these mammalian primates have
the most human-like brain structures and are ideal for receiving
sensory tasks that mimic cognitive impairment. At the same time,
rhesus macaques and chimpanzees as animal models are expensive and
their use requires careful ethical consideration (82,83).
Canines are also ideal animal models, which can exhibit age-related
cognitive impairment similarly to humans, but canines do not
present with neural plaques and tangles (84). Mice and rats are the most
economical choice in most laboratories. They have similar mammalian
physiology, similar brain structure to humans and lower feeding
costs. However, their selection is not perfect, and they must face
the disadvantages of a long breeding cycle and high time cost
(85,86). Nevertheless, mice and rats are
preferred animal models in most brain science laboratories (for a
classification of artificial intervention AD animal models see
Table II) (87-95).
Injection of streptozotocin (STZ) into the lateral
ventricles of animals disrupts brain energy metabolism, and it is a
common method to model AD in animals with corresponding Aβ
deposition, hyperphosphorylation of tau protein, abnormal
cholinergic function and oxidative stress (96-98).
It is worth mentioning that STZ is also the primary modeling drug
for diabetes. This underscores the potential co-morbid mechanisms
of metabolic disease with AD in another way.
The WHO estimates that the proportion of the
population of the world aged >60 years old will rise to 22% by
2050 (97,98). Emerging evidence now indicates an
increasing trend in patients with AD and related age-related
diseases (97). For example, in
the United States, the number of patients aged ≥65 years with AD
and related dementia is increasing and is expected to reach 13.9
million by 2060(98). These
epidemiological studies suggest that the decline in quality of life
in older adults and the increased risk of AD and related
aging-related diseases pose a serious threat to global health
(Fig. 1).
As the relationship between metabolic diseases and
AD deepens, it is necessary to understand the reasonable
relationship between the two. The present review discusses the new
role of diabetes, obesity and hypercholesterolemia in AD. Changes
in the hippocampus and frontal cortex have been found in both
patients with metabolic disease and those with AD, using a variety
of diagnostic instruments or anatomical studies. Most of these
changes occur in the volume of different brain regions and the
level of cortical proteins. This series of changes points to
commonalities between metabolic diseases and cognitive changes in
brain injury (13,19,20,41,55-57).
Another study found that long-term high-sugar and high-fat diets
can induce metabolic syndrome in experimental animals, and their
brain tissue can exhibit typical characteristic changes of AD
(99). Excessive lipid deposition
in brain tissue can induce chronic inflammation, which plays an
important role in the onset of AD. Exploring safe and effective
intervention measures is currently one of the urgent issues that
need to be addressed in the interdisciplinary treatment of
metabolic syndrome. Excessive nutrition can cause changes in the
hypothalamic immune system, leading to a hypothalamic inflammatory
response, The activation of pro-inflammatory factors and other
pro-inflammatory molecules persists in the pathological processes
associated with metabolic syndrome, indicating the importance of
improving obesity and other metabolic syndromes in the treatment of
AD (100,101).
From a pathological perspective, the amyloid
hypothesis has long been the dominant theory asserting that AD is
caused by the accumulation of Aβ protein in the brain, leading to
neuronal toxicity in the central nervous system (58). Metabolic diseases also happen to
influence the pathogenesis of AD from different perspectives. These
metabolic diseases are involved either through a process of Aβ
plaque formation or increased Aβ accumulation (21-24,67).
In addition, the aforementioned metabolic diseases
also affect the course of AD through some potential mechanisms. The
cAMP/PKA signaling pathway, the IRS-Akt pathway, neuronal
apoptosis, neuroinflammation and oxidative stress are all factors
that have been verified by several research groups; they become
common ground between metabolic diseases and cognitive impairment
(25-28,46-49,65-67).
These commonalities lead the present authors to focus on the
potential of drugs commonly used to treat metabolic diseases for
the treatment of AD. There are rich pathophysiological links
between AD and diabetes. It is not difficult to imagine that some
anti-diabetic drugs may be used to treat AD. Among them, insulin is
the most prominent example. Aβ senile plaque formation and tau
protein hyperphosphorylation are the main histopathological
manifestations of AD, and insulin signaling and insulin resistance
play important regulatory roles (102). Research shows that insulin can
protect the brains of rats from Aβ formation, thereby having
beneficial effects on them (103). Another example is metformin. The
effect of metformin on insulin is achieved through AMP-activated
protein kinase (104). In
previous experiments, metformin has been shown to reduce tau
phosphorylation and prevent pathological changes in AD neurons
(105).
Animal models play an important role in the study of
the pathogenesis and potential treatment of AD. The present review
summarizes the common animal models and their advantages and
disadvantages to provide a reference for researchers. Although
several groups studied the subtle link between metabolic disease
and AD, several questions remain to be answered. A common question
is about the causal relationship that exists between metabolic
disease and cognitive impairment. The present study has a clear
understanding that these two diseases usually occur together, but
the sequence and causality between them are not yet supported by
strong experimental results. In addition, the criteria for
characterizing AD and metabolic disease in different animal models
are not consistent, which makes it difficult to map to clinical
patients, which requires more data.
Not applicable.
Funding: This work was supported by the General Project of the
Natural Science Foundation of Hubei Province (grant no.
2021CFB585), the General Project of Health Commission of Hubei
Province (grant no. WJ2021M030).
Not applicable.
FL contributed to the design of the review. HL and
SZ prepared the manuscript. LT, WC, GY, HG, XW and QH made
substantial contributions to conception and design. All authors
have read and approved the final version of the manuscript. Data
authentication is not applicable.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Kovács Z, Brunner B and Ari C: Beneficial
effects of exogenous ketogenic supplements on aging processes and
age-related neurodegenerative diseases. Nutrients.
13(2197)2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Jensen L, Monnat SM, Green JJ, Hunter LM
and Sliwinski MJ: Rural population health and aging: Toward a
multilevel and multidimensional research agenda for the 2020s. Am J
Public Health. 110:1328–1331. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Li Y, Xu H, Wang H, Yang K, Luan J and
Wang S: TREM2: Potential therapeutic targeting of microglia for
Alzheimer's disease. Biomed Pharmacother.
165(115218)2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Maria C and Rauter AP: Nucleoside
analogues: N-glycosylation methodologies, synthesis of antiviral
and antitumor drugs and potential against drug-resistant bacteria
and Alzheimer's disease. Carbohydr Res. 532(108889)2023.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Stocker H, Trares K, Beyer L, Perna L,
Rujescu D, Holleczek B, Beyreuther K, Gerwert K, Schöttker B and
Brenner H: Alzheimer's polygenic risk scores, APOE, Alzheimer's
disease risk, and dementia-related blood biomarker levels in a
population-based cohort study followed over 17 years. Alzheimers
Res Ther. 15(129)2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Weller J and Budson A: Current
understanding of Alzheimer's disease diagnosis and treatment.
F1000Res 7: F1000 Faculty Rev-1161, 2018.
|
|
7
|
Ismail Z, Leon R, Creese B, Ballard C,
Robert P and Smith EE: Optimizing detection of Alzheimer's disease
in mild cognitive impairment: A 4-year biomarker study of mild
behavioral impairment in ADNI and MEMENTO. Mol Neurodegener.
18(50)2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Antoniou A, Stavrou M, Evripidou N,
Georgiou E, Kousiappa I, Koupparis A, Papacostas SS, Kleopa KA and
Damianou C: FUS-mediated blood-brain barrier disruption for
delivering anti-Aβ antibodies in 5XFAD Alzheimer's disease mice. J
Ultrasound: Jul 29, 2023 (Epub ahead of print). doi:
10.1007/s40477-023-00805-4.
|
|
9
|
Śliwińska S and Jeziorek M: The role of
nutrition in Alzheimer's disease. Rocz Panstw Zakl Hig. 72:29–39.
2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fan R, Peng X, Xie L, Dong K, Ma D, Xu W,
Shi X, Zhang S, Chen J, Yu X, et al: Importance of Bmal1 in
Alzheimer's disease and associated aging-related diseases.
Mechanisms and interventions. Aging Cell. 21(e13704)2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Carvalho C and Moreira PI: Metabolic
defects shared by Alzheimer's disease and diabetes: A focus on
mitochondria. Curr Opin Neurobiol. 79(102694)2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Nguyen TT, Ta QTH, Nguyen TKO, Nguyen TTD
and Giau VV: Type 3 diabetes and its role implications in
Alzheimer's disease. Int J Mol Sci. 21(3165)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Janoutová J, Machaczka O, Zatloukalová A
and Janout V: Is Alzheimer's disease a type 3 diabetes? A review.
Cent Eur J Public Health. 30:139–143. 2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kandimalla R, Thirumala V and Reddy PH: Is
Alzheimer's disease a type 3 diabetes? A critical appraisal.
Biochim Biophys Acta Mol Basis Dis. 1863:1078–1089. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Michailidis M, Moraitou D, Tata DA,
Kalinderi K, Papamitsou T and Papaliagkas V: Alzheimer's disease as
type 3 diabetes: Common pathophysiological mechanisms between
Alzheimer's disease and type 2 diabetes. Int J Mol Sci.
23(2687)2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Diniz Pereira J, Gomes Fraga V, Morais
Santos AL, Carvalho MDG, Caramelli P and Braga Gomes K: Alzheimer's
disease and type 2 diabetes mellitus: A systematic review of
proteomic studies. J Neurochem. 156:753–776. 2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Arnold SE, Arvanitakis Z, Macauley-Rambach
SL, Koenig AM, Wang HY, Ahima RS, Craft S, Gandy S, Buettner C,
Stoeckel LE, et al: Brain insulin resistance in type 2 diabetes and
Alzheimer disease: Concepts and conundrums. Nat Rev Neurol.
14:168–181. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hamzé R, Delangre E, Tolu S, Moreau M,
Janel N, Bailbé D and Movassat J: Type 2 diabetes mellitus and
Alzheimer's disease: Shared molecular mechanisms and potential
common therapeutic targets. Int J Mol Sci. 23(15287)2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Chen Z and Zhong C: Decoding Alzheimer's
disease from perturbed cerebral glucose metabolism: Implications
for diagnostic and therapeutic strategies. Prog Neurobiol.
108:21–43. 2013.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Candasamy M, Mohamed Elhassan SA, Kumar
Bhattamisra S, Hua WY, Sern LM, Binti Busthamin NA, Mohamad Ilni
NB, Shun NS, Baohong L, Ya NS and Ying NW: Type 3 diabetes
(Alzheimer's disease): New insight for promising therapeutic
avenues. Panminerva Med. 62:155–163. 2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Zhang Y, Huang NQ, Yan F, Jin H, Zhou SY,
Shi JS and Jin F: Diabetes mellitus and Alzheimer's disease: GSK-3β
as a potential link. Behav Brain Res. 339:57–65. 2018.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Moayedi K, Orandi S, Ebrahimi R, Tanhapour
M, Moradi M, Abbastabar M and Golestani A: A novel approach to type
3 diabetes mechanism: The interplay between noncoding RNAs and
insulin signaling pathway in Alzheimer's disease. J Cell Physiol.
237:2838–2861. 2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
de la Monte SM: The full spectrum of
Alzheimer's disease is rooted in metabolic derangements that drive
type 3 diabetes. Adv Exp Med Biol. 1128:45–83. 2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ma LY, Fei YL, Wang XY, Wu SD, Du JH, Zhu
M, Jin L, Li M, Li HL, Zhai JJ, et al: The research on the
relationship of RAGE, LRP-1, and Aβ accumulation in the
hippocampus, prefrontal lobe, and amygdala of STZ-Induced diabetic
rats. J Mol Neurosci. 62:1–10. 2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
XiaoMing Z, Xi Z, Fang S and Jilin Z:
Specific changes of somatostatin mRNA expression in the frontal
cortex and hippocampus of diabetic rats. J Anat. 204:221–225.
2004.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lachmann G, Spies C, Windmann V,
Wollersheim T, Engelhardt LJ, Winterer G and Kuehn S: BIOCOG Study
Group. Impact of intraoperative hyperglycemia on brain structures
and volumes. J Neuroimaging. 29:260–267. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Bao H, Liu Y, Zhang M, Chen Z, Zhang W, Ge
Y, Kang D, Gao F and Shen Y: Increased β-site APP cleaving enzyme
1-mediated insulin receptor cleavage in type 2 diabetes mellitus
with cognitive impairment. Alzheimers Dement. 17:1097–1108.
2021.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Braun M, Ramracheya R and Rorsman P:
Autocrine regulation of insulin secretion. Diabetes Obes Metab. 14
(Suppl 3):S143–S151. 2012.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Botteri G, Salvadó L, Gumà A, Lee Hamilton
D, Meakin PJ, Montagut G, Ashford MLJ, Ceperuelo-Mallafré V,
Fernández-Veledo S, Vendrell J, et al: The BACE1 product sAPPβ
induces ER stress and inflammation and impairs insulin signaling.
Metabolism. 85:59–75. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Wang Q, Duan L, Li X, Wang Y, Guo W, Guan
F and Ma S: Glucose metabolism, neural cell senescence and
Alzheimer's disease. Int J Mol Sci. 23(4351)2022.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Li H, Yang S, Wu J, Ji L, Zhu L, Cao L,
Huang J, Jiang Q, Wei J, Liu M, et al: cAMP/PKA signaling pathway
contributes to neuronal apoptosis via regulating IDE expression in
a mixed model of type 2 diabetes and Alzheimer's disease. J Cell
Biochem. 119:1616–1626. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Farr SA, Roesler E, Niehoff ML, Roby DA,
McKee A and Morley JE: Metformin improves learning and memory in
the SAMP8 mouse model of Alzheimer's disease. J Alzheimers Dis.
68:1699–1710. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Mishra D, Reddy I and Dey CS: PKCα Isoform
inhibits insulin signaling and aggravates neuronal insulin
resistance. Mol Neurobiol. 60:6642–6659. 2023.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Oriente F, Andreozzi F, Romano C, Perruolo
G, Perfetti A, Fiory F, Miele C, Beguinot F and Formisano P:
Protein kinase C-alpha regulates insulin action and degradation by
interacting with insulin receptor substrate-1 and 14-3-3 epsilon. J
Biol Chem. 280:40642–40649. 2005.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Qi XM and Chen G: p38γ MAPK inflammatory
and metabolic signaling in physiology and disease. Cells.
12(1674)2023.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Esterline R, Oscarsson J and Burns J: A
role for sodium glucose cotransporter 2 inhibitors (SGLT2is) in the
treatment of Alzheimer's disease? Int Rev Neurobiol. 155:113–140.
2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Talbot K, Wang HY, Kazi H, Han LY, Bakshi
KP, Stucky A, Fuino RL, Kawaguchi KR, Samoyedny AJ, Wilson RS, et
al: Demonstrated brain insulin resistance in Alzheimer's disease
patients is associated with IGF-1 resistance, IRS-1 dysregulation,
and cognitive decline. J Clin Invest. 122:1316–1338.
2012.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Frith E and Loprinzi PD: Fitness Fatness
Index and Alzheimer-specific mortality. Eur J Intern Med. 42:51–53.
2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Pugazhenthi S, Qin L and Reddy PH: Common
neurodegenerative pathways in obesity, diabetes, and Alzheimer's
disease. Biochim Biophys Acta Mol Basis Dis. 1863:1037–1045.
2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Silva MVF, Loures CMG, Alves LCV, de Souza
LC, Borges KBG and Carvalho MDG: Alzheimer's disease: Risk factors
and potentially protective measures. J Biomed Sci.
26(33)2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Flores-Cordero JA, Pérez-Pérez A,
Jiménez-Cortegana C, Alba G, Flores-Barragán A and Sánchez-Margalet
V: Obesity as a risk factor for dementia and Alzheimer's disease:
The Role of Leptin. Int J Mol Sci. 23(5202)2022.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Khanna D, Peltzer C, Kahar P and Parmar
MS: Body mass index (BMI): A screening tool analysis. Cureus.
14(e22119)2022.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Flegal KM, Kit BK, Orpana H and Graubard
BI: Association of all-cause mortality with overweight and obesity
using standard body mass index categories: A systematic review and
meta-analysis. JAMA. 309:71–82. 2013.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Ashwell M, Gunn P and Gibson S:
Waist-to-height ratio is a better screening tool than waist
circumference and BMI for adult cardiometabolic risk factors:
Systematic review and meta-analysis. Obes Rev. 13:275–286.
2012.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Diehl-Wiesenecker E, von Armin CA, Dupuis
L, Müller HP, Ludolph AC and Kassubek J: Adipose tissue
distribution in patients with Alzheimer's disease: A whole body MRI
Case-Control study. J Alzheimers Dis. 48:825–832. 2015.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Boccara E, Golan S and Beeri MS: The
association between regional adiposity, cognitive function, and
dementia-related brain changes: A systematic review. Front Med
(Lausanne). 10(1160426)2023.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Gómez-Apo E, Mondragón-Maya A,
Ferrari-Díaz M and Silva-Pereyra J: Structural Brain Changes
associated with overweight and obesity. J Obes.
2021(6613385)2021.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Li X, Chen H, Lv Y, Chao HH, Gong L, Li CR
and Cheng H: Diminished gray matter density mediates chemotherapy
dosage-related cognitive impairment in breast cancer patients. Sci
Rep. 8(13801)2018.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Miao Y, Zhang B, Sun X, Ma X, Fang D,
Zhang W, Wu T, Xu X, Yu C, Hou Y, et al: The presence and severity
of NAFLD are associated with cognitive impairment and hippocampal
damage. J Clin Endocrinol Metab. 108:3239–3249. 2023.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Weinstein G, Zelber-Sagi S, Preis SR,
Beiser AS, DeCarli C, Speliotes EK, Satizabal CL, Vasan RS and
Seshadri S: Association of nonalcoholic fatty liver disease with
lower brain volume in healthy Middle-aged adults in the framingham
study. JAMA Neurol. 75:97–104. 2018.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Ruchinskas R, Nguyen T, Womack K, Khera A,
Yu FF and Kelley BJ: Diagnostic utility of hippocampal volumetric
data in a memory disorder clinic setting. Cogn Behav Neurol.
35:66–75. 2022.PubMed/NCBI View Article : Google Scholar
|
|
52
|
van Oostveen WM and de Lange ECM: Imaging
techniques in Alzheimer's disease: A review of applications in
early diagnosis and longitudinal monitoring. Int J Mol Sci.
22(2110)2021.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Prem Kumar A, Singh N, Nair D and Justin
A: Neuronal PET tracers for Alzheimer's disease. Biochem Biophys
Res Commun. 587:58–62. 2022.PubMed/NCBI View Article : Google Scholar
|
|
54
|
So SW, Fleming KM, Nixon JP and Butterick
TA: Early life obesity increases neuroinflammation, amyloid beta
deposition, and cognitive decline in a mouse model of Alzheimer's
disease. Nutrients. 15(2494)2023.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Jayaraman A, Lent-Schochet D and Pike CJ:
Diet-induced obesity and low testosterone increase
neuroinflammation and impair neural function. J Neuroinflammation.
11(162)2014.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Liu P, Wang ZH, Kang SS, Liu X, Xia Y,
Chan CB and Ye K: High-fat diet-induced diabetes couples to
Alzheimer's disease through inflammation-activated C/EBPβ/AEP
pathway. Mol Psychiatry. 27:3396–3409. 2022.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Medrano-Jiménez E, Jiménez-Ferrer Carrillo
I, Pedraza-Escalona M, Ramírez-Serrano CE, Álvarez-Arellano L,
Cortés-Mendoza J, Herrera-Ruiz M, Jiménez-Ferrer E, Zamilpa A,
Tortoriello J, et al: Malva parviflora extract ameliorates the
deleterious effects of a high fat diet on the cognitive deficit in
a mouse model of Alzheimer's disease by restoring microglial
function via a PPAR-γ-dependent mechanism. J Neuroinflammation.
16(143)2019.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Zhang B, Chen T, Cao M, Yuan C, Reiter RJ,
Zhao Z, Zhao Y, Chen L, Fan W, Wang X, et al: Gut microbiota
dysbiosis induced by decreasing endogenous melatonin mediates the
pathogenesis of Alzheimer's disease and obesity. Front Immunol.
13(900132)2022.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Obradovic M, Zaric B, Sudar-Milovanovic E,
Ilincic B, Stokic E, Perovic M and Isenovic ER: PCSK9 and
hypercholesterolemia: Therapeutic Approach. Curr Drug Targets.
19:1058–1067. 2018.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Mannarino MR, Ministrini S and Pirro M:
Nutraceuticals for the treatment of hypercholesterolemia. Eur J
Intern Med. 25:592–599. 2014.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Loera-Valencia R, Goikolea J,
Parrado-Fernandez C, Merino-Serrais P and Maioli S: Alterations in
cholesterol metabolism as a risk factor for developing Alzheimer's
disease: Potential novel targets for treatment. J Steroid Biochem
Mol Biol. 190:104–114. 2019.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Appleton JP, Scutt P, Sprigg N and Bath
PM: Hypercholesterolaemia and vascular dementia. Clin Sci (Lond).
131:1561–1578. 2017.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Sandebring-Matton A, Goikolea J, Björkhem
I, Paternain L, Kemppainen N, Laatikainen T, Ngandu T, Rinne J,
Soininen H, Cedazo-Minguez A, et al: 27-Hydroxycholesterol,
cognition, and brain imaging markers in the FINGER randomized
controlled trial. Alzheimers Res Ther. 13(56)2021.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Reiman EM, Chen K, Langbaum JB, Lee W,
Reschke C, Bandy D, Alexander GE and Caselli RJ: Higher serum total
cholesterol levels in late middle age are associated with glucose
hypometabolism in brain regions affected by Alzheimer's disease and
normal aging. Neuroimage. 49:169–176. 2010.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Gottesman RF, Schneider AL, Zhou Y, Coresh
J, Green E, Gupta N, Knopman DS, Mintz A, Rahmim A, Sharrett AR, et
al: Association between midlife vascular risk factors and estimated
brain amyloid deposition. JAMA. 317:1443–1450. 2017.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Serrano-Pozo A, Das S and Hyman BT: APOE
and Alzheimer's disease: Advances in genetics, pathophysiology, and
therapeutic approaches. Lancet Neurol. 20:68–80. 2021.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Martens YA, Zhao N, Liu CC, Kanekiyo T,
Yang AJ, Goate AM, Holtzman DM and Bu G: ApoE Cascade Hypothesis in
the pathogenesis of Alzheimer's disease and related dementias.
Neuron. 110:1304–1317. 2022.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Raulin AC, Doss SV, Trottier ZA, Ikezu TC,
Bu G and Liu CC: ApoE in Alzheimer's disease: Pathophysiology and
therapeutic strategies. Mol Neurodegener. 17(72)2022.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Koutsodendris N, Nelson MR, Rao A and
Huang Y: Apolipoprotein E and Alzheimer's Disease: Findings,
hypotheses, and potential mechanisms. Annu Rev Pathol. 17:73–99.
2022.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Lanfranco MF, Ng CA and Rebeck GW: ApoE
lipidation as a therapeutic target in Alzheimer's disease. Int J
Mol Sci. 21(6336)2020.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Zhao N, Liu CC, Qiao W and Bu G:
Apolipoprotein E, receptors, and modulation of Alzheimer's disease.
Biol Psychiatry. 83:347–357. 2018.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Fernández-Calle R, Konings SC,
Frontiñán-Rubio J, García-Revilla J, Camprubí-Ferrer L, Svensson M,
Martinson I, Boza-Serrano A, Venero JL, Nielsen HM, et al: APOE in
the bullseye of neurodegenerative diseases: Impact of the APOE
genotype in Alzheimer's disease pathology and brain diseases. Mol
Neurodegener. 17(62)2022.PubMed/NCBI View Article : Google Scholar
|
|
73
|
McNamara DJ: Dietary cholesterol, heart
disease risk and cognitive dissonance. Proc Nutr Soc. 73:161–166.
2014.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Lee SB, Kim HG, Lee JS, Kim WY, Lee MM,
Kim YH, Lee JO, Kim HS and Son CG: Intermittent restraint-induced
sympathetic activation attenuates hepatic steatosis and
inflammation in a high-fat diet-fed mouse model. Am J Physiol
Gastrointest Liver Physiol. 317:G811–G823. 2019.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Ettcheto M, Petrov D, Pedrós I, Alva N,
Carbonell T, Beas-Zarate C, Pallas M, Auladell C, Folch J and
Camins A: Evaluation of neuropathological effects of a High-Fat
diet in a presymptomatic Alzheimer's disease stage in APP/PS1 Mice.
J Alzheimers Dis. 54:233–251. 2016.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Bromley-Brits K, Deng Y and Song W: Morris
water maze test for learning and memory deficits in Alzheimer's
disease model mice. J Vis Exp. 20(2920)2011.PubMed/NCBI View
Article : Google Scholar
|
|
77
|
Song J: Animal model of aluminum-induced
Alzheimer's disease. Adv Exp Med Biol. 1091:113–127.
2018.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Drummond E and Wisniewski T: Alzheimer's
disease: Experimental models and reality. Acta Neuropathol.
133:155–175. 2017.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Zhang L, Chen C, Mak MS, Lu J, Wu Z, Chen
Q, Han Y, Li Y and Pi R: Advance of sporadic Alzheimer's disease
animal models. Med Res Rev. 40:431–458. 2020.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Thawkar BS and Kaur G: Zebrafish as a
promising tool for modeling Neurotoxin-Induced Alzheimer's disease.
Neurotox Res. 39:949–965. 2021.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Tsuda L and Lim YM: Alzheimer's disease
model system using drosophila. Adv Exp Med Biol. 1076:25–40.
2018.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Souder DC, Dreischmeier IA, Smith AB,
Wright S, Martin SA, Sagar MAK, Eliceiri KW, Salamat SM, Bendlin
BB, Colman RJ, et al: Rhesus monkeys as a translational model for
late-onset Alzheimer's disease. Aging Cell.
20(e13374)2021.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Edler MK, Munger EL, Meindl RS, Hopkins
WD, Ely JJ, Erwin JM, Mufson EJ, Hof PR, Sherwood CC and Raghanti
MA: Neuron loss associated with age but not Alzheimer's disease
pathology in the chimpanzee brain. Philos Trans R Soc Lond B Biol
Sci. 375(20190619)2020.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Dewey CW, Davies ES, Xie H and Wakshlag
JJ: Canine cognitive dysfunction: Pathophysiology, diagnosis, and
treatment. Vet Clin North Am Small Anim Pract. 49:477–499.
2019.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Esquerda-Canals G, Montoliu-Gaya L,
Güell-Bosch J and Villegas S: Mouse models of Alzheimer's Disease.
J Alzheimers Dis. 57:1171–1183. 2017.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Puzzo D, Gulisano W, Palmeri A and Arancio
O: Rodent models for Alzheimer's disease drug discovery. Expert
Opin Drug Discov. 10:703–711. 2015.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Hefti F, Dravid A and Hartikka J: Chronic
intraventricular injections of nerve growth factor elevate
hippocampal choline acetyltransferase activity in adult rats with
partial septo-hippocampal lesions. Brain Res. 293:305–311.
1984.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Washida K, Hattori Y and Ihara M: Animal
models of chronic cerebral hypoperfusion: From mouse to primate.
Int J Mol Sci. 20(6176)2019.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Yi J, Liu BY and Cai GX: Study on effect
of Ultra-powder Liuwei Dihuang decoction on recognize and bFGF in
Alzheime's disease rats bFGF. Chin J Exp Tradit Med Formulae.
17:139–142. 2011.
|
|
90
|
Chen HF, Mo YS and Yang C: Protective
effect and mechanism of quercetin on hippocampal neurons in
IBO-injured rats. Tradit Chin Drug Res Clin Pharmacol. 29:552–556.
2018.
|
|
91
|
Lester-Coll N, Rivera EJ, Soscia SJ,
Doiron K, Wands JR and de la Monte SM: Intracerebral Streptozotocin
model of type 3 diabetes: Relevance to sporadic Alzheimer's
disease. J Alzheimers Dis. 9:13–33. 2006.PubMed/NCBI View Article : Google Scholar
|
|
92
|
Wang C, Cai Z, Wang W, Wei M, Si X, Shang
Y, Yang Z, Li T, Guo H and Li S: Piperine regulates glycogen
synthase kinase-3β-related signaling and attenuates cognitive
decline in D-galactose-induced aging mouse model. J Nutr Biochem.
75(108261)2020.PubMed/NCBI View Article : Google Scholar
|
|
93
|
Mustafa HN: Neuro-amelioration of
cinnamaldehyde in aluminum-induced Alzheimer's disease rat model. J
Histotechnol. 43:11–20. 2020.PubMed/NCBI View Article : Google Scholar
|
|
94
|
Song XY, Hu JF, Chu SF, Zhang Z, Xu S,
Yuan YH, Han N, Liu Y, Niu F, He X and Chen NH: Ginsenoside Rg1
attenuates okadaic acid induced spatial memory impairment by the
GSK3β/tau signaling pathway and the Aβ formation prevention in
rats. Eur J Pharmacol. 710:29–38. 2013.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Haider S, Tabassum S and Perveen T:
Scopolamine-induced greater alterations in neurochemical profile
and increased oxidative stress demonstrated a better model of
dementia: A comparative study. Brain Res Bull. 127:234–247.
2016.PubMed/NCBI View Article : Google Scholar
|
|
96
|
Zangerolamo L, Vettorazzi JF, Solon C,
Bronczek GA, Engel DF, Kurauti MA, Soares GM, Rodrigues KS, Velloso
LA, Boschero AC, et al: The bile acid TUDCA improves glucose
metabolism in streptozotocin-induced Alzheimer's disease mice
model. Mol Cell Endocrinol. 521(111116)2021.PubMed/NCBI View Article : Google Scholar
|
|
97
|
Liu RM: Aging, cellular senescence, and
Alzheimer's Disease. Int J Mol Sci. 23(1989)2022.PubMed/NCBI View Article : Google Scholar
|
|
98
|
Stern Y: Cognitive reserve in ageing and
Alzheimer's disease. Lancet Neurol. 11:1006–1012. 2012.PubMed/NCBI View Article : Google Scholar
|
|
99
|
Leuti A, Fazio D, Fava M, Piccoli A, Oddi
S and Maccarrone M: Bioactive lipids, inflammation and chronic
diseases. Adv Drug Deliv Rev. 159:133–169. 2020.PubMed/NCBI View Article : Google Scholar
|
|
100
|
Kälin S, Heppner FL, Bechmann I, Prinz M,
Tschöp MH and Yi CX: Hypothalamic innate immune reaction in
obesity. Nat Rev Endocrinol. 11:339–351. 2015.PubMed/NCBI View Article : Google Scholar
|
|
101
|
de Git KC and Adan RA: Leptin resistance
in diet-induced obesity: The role of hypothalamic inflammation.
Obes Rev. 16:207–224. 2015.PubMed/NCBI View Article : Google Scholar
|
|
102
|
Boccardi V, Murasecco I and Mecocci P:
Diabetes drugs in the fight against Alzheimer's disease. Ageing Res
Rev. 54(100936)2019.PubMed/NCBI View Article : Google Scholar
|
|
103
|
Kellar D and Craft S: Brain insulin
resistance in Alzheimer's disease and related disorders: Mechanisms
and therapeutic approaches. Lancet Neurol. 19:758–766.
2020.PubMed/NCBI View Article : Google Scholar
|
|
104
|
Campbell JM, Stephenson MD, de Courten B,
Chapman I, Bellman SM and Aromataris E: Metformin use associated
with reduced risk of dementia in patients with diabetes: A
systematic review and Meta-Analysis. J Alzheimers Dis.
65:1225–1236. 2018.PubMed/NCBI View Article : Google Scholar
|
|
105
|
Briggs R, Kennelly SP and O'Neill D: Drug
treatments in Alzheimer's disease. Clin Med (Lond). 16:247–253.
2016.PubMed/NCBI View Article : Google Scholar
|