Introduction
Sarcoidosis is a systemic disorder of unknown
etiology that is characterized by the presence of non-caseating
epithelioid cell granulomas (1).
However, recent studies have suggested that adverse autoimmune
reactions and microbial organisms can serve an important role in
its pathogenesis (2-4).
Lung involvement including pleural, pulmonary parenchyma and
trachea, is the most commonly observed presentation, followed by
skin, eyes and joints (1,5). In addition, mediastinal lymph nodes
are found to be affected in the majority of sarcoidosis cases
(6). Sarcoidosis has a wide range
of clinical phenotypes, ranging from acute to asymptomatic.
However, some patients do experience severe symptoms that
necessitate potent immunosuppressive treatments, including
corticosteroids, methotrexate or antitumor necrosis factor-α
agents. The majority of patients with sarcoidosis die from
pulmonary fibrosis (1,5).
Coronavirus disease 2019 (COVID-19) is a disease
induced by severe acute respiratory syndrome coronavirus 2
(SARS-CoV-2). COVID-19 can induce a series of immunoinflammatory
responses to disturb self-tolerance and trigger autoimmune
responses (7,8). Tana et al (9) proposed that there may be a link
between COVID-19 and sarcoidosis, since they have similar clinical
manifestations and may influence each other at multiple levels,
eventually affecting their clinical courses and prognosis (9).
Both sarcoidosis and tuberculosis (TB) are
characterized by typical epithelioid cell granulomas (10). Previous reports have proposed the
two diseases may have similarities in progression, whilst others
have suggested that tuberculosis-causing mycobacterial antigens are
the inciting agents in a proportion of sarcoidosis cases (11,12).
The coexistence of sarcoidosis and TB infection has also been
previously reported (13,14). This similarity in clinical features
renders the differential diagnosis between these two diseases
challenging.
The present report describes a case who presented
with multiple lymphadenopathies throughout the body after COVID-19
and was T-SPOT.TB positive, but without lung parenchyma
involvement. The present case report aims to suggest possible
connection between COVID-19 and sarcoidosis, and provide insights
to sarcoidosis diagnosis.
Case report
A 48-year-old male presenting with chest pain for 1
week presented himself into Jinling Hospital (Nanjing, China) in
January 2023. The pain was described as having no specific area, no
heart burn feeling or chest pressure. It was not provoked by
exertion, nor obviously relieved by rest. There were also no
complaints of fever, dizziness, fainting, dyspnea or coughing. The
patient had been diagnosed with SARS-CoV-2 by real time RT-PCR
(RT-qPCR) testing in early December 2022 (Fig. S1), when the patient had high-grade
fever (38-39˚C), cough and sore throat for 4 days. He received
symptomatic treatments, including cough suppressants and
antipyretics, at home and recovered within 1 week. The patient had
a history of hypertension for 10 years and received
sustained-release felodipine tablets (5 mg/per day), with no
previous history of TB. Physical examination revealed bilaterally
soft and swollen cervical lymph nodes in bean size but they were
not painful. All other systemic examinations and vital signs were
normal.
Extensive biochemical and radiological evaluations
were subsequently conducted. 12-lead ECG, coronary arteriography,
echocardiography and serum markers of myocardial damage, including
creatine kinase [84 U/l (normal range, 50-310 U/l)], the MB
isoenzyme of creatine kinase [1.7 ng/ml (normal range, 0-3.7
ng/ml)], troponin T [0.009 ng/ml (normal range, 0-0.014 ng/ml)] and
troponin I [0.03 ng/ml (normal range, <0.06 ng/ml)], were all
performed and there was no evidence of cardiovascular disease. The
creatine kinase level was detected using a Model 7600 Series
Automatic Analyzer (Hitachi, Ltd.). The MB isoenzyme of creatine
kinase level and troponin I level were detected using an AIA-2000
Automated Immunoassay Analyzer (Tosoh Bioscience). Troponin T level
was detected using a cobas e601 module (Roche Diagnostics).
RT-qPCR testing for SARS-CoV-2 yielded negative
results. Serum autoantibody testing revealed that the anti-β2
glycoprotein-1 antibody level was 100.00 RU/ml (normal range,
<16 RU/ml), anti-β2 glycoprotein-1 IgG antibody level was 29.5
AU/ml (normal range, <16 AU/ml), the anti-β2 glycoprotein-1 IgM
antibody level was 56.2 AU/ml (normal range, <16 AU/ml), the
anticardiolipin antibody (ACA) level was 22.8 RU/ml (normal range,
<12 RU/ml) and the ACA IgM level was 26.8 MPLU/ml (normal <12
MPLU/ml). The serum level of angiotensin-converting enzyme was 25.0
U/l (normal range, <52.0 U/l). Antinuclear antibody and
erythrocyte sedimentation rate revealed no significant
abnormalities. Further biochemical examinations revealed positivity
in T-SPOT.TB [Panel A of early secreted antigenic target 6 (ESAT6),
2 spot-forming cells (SFC); panel B of 10-kDa culture filtrate
protein (CFP-10), 14 SFC; normal range for both, 0-6 SFC].
For RT-qPCR, the RNA of pharynx swab sample was
extracted by using the Stream SP96 Automatic Nucleic Acid
Extraction Machine (Daan Gene) and RNA Isolation Kit (cat. no.
ME-0012, Shanghai ZJ Bio-Tech Co., Ltd). RT-qPCR kits for
SARS-CoV-2 nucleic acid testing were obtained from Shanghai ZJ
Bio-Tech Co., Ltd (Novel Coronavirus 2019-nCoV Real Time Multiplex
RT-PCR Kit Detection for 3 Genes, W-RR-0479-02). RT-qPCR was
performed on an Applied Biosystems 7500 real-time RT-PCR system
(Thermo Fisher Scientific, Inc.) and the manufacturer's protocol
was followed. The program was set as follows: pre-amplification
45˚C for 10 min, 95˚C for 180 sec and 45 cycles of 95˚C for 15 sec
and 58˚C for 30 sec. The result was identified as positive if cycle
threshold (Cq) value <40(15).
The T-SPOT.TB test from Oxford Immunotec (T-SPOT.TB Multi-use
8-Well Strip Plate Format. Catalogue number: TB.300) was used and
we followed the manufacturer's instruction. The blood specimen was
collected and extracted by using CellSep® Pro Instrument (Eureka
bio, CS101) to create a standard peripheral blood mononuclear cell
suspension. They were then added into specially designed plates in
the kit and stimulated with TB-specific antigens, ESAT-6 and CFP10.
Cells responding to these antigens would release IFN-γ, which were
captured by the enzyme-labeled antibody and detection reagent to
produce spots. Spots were then counted manually under a light
microscope (magnification, x40).
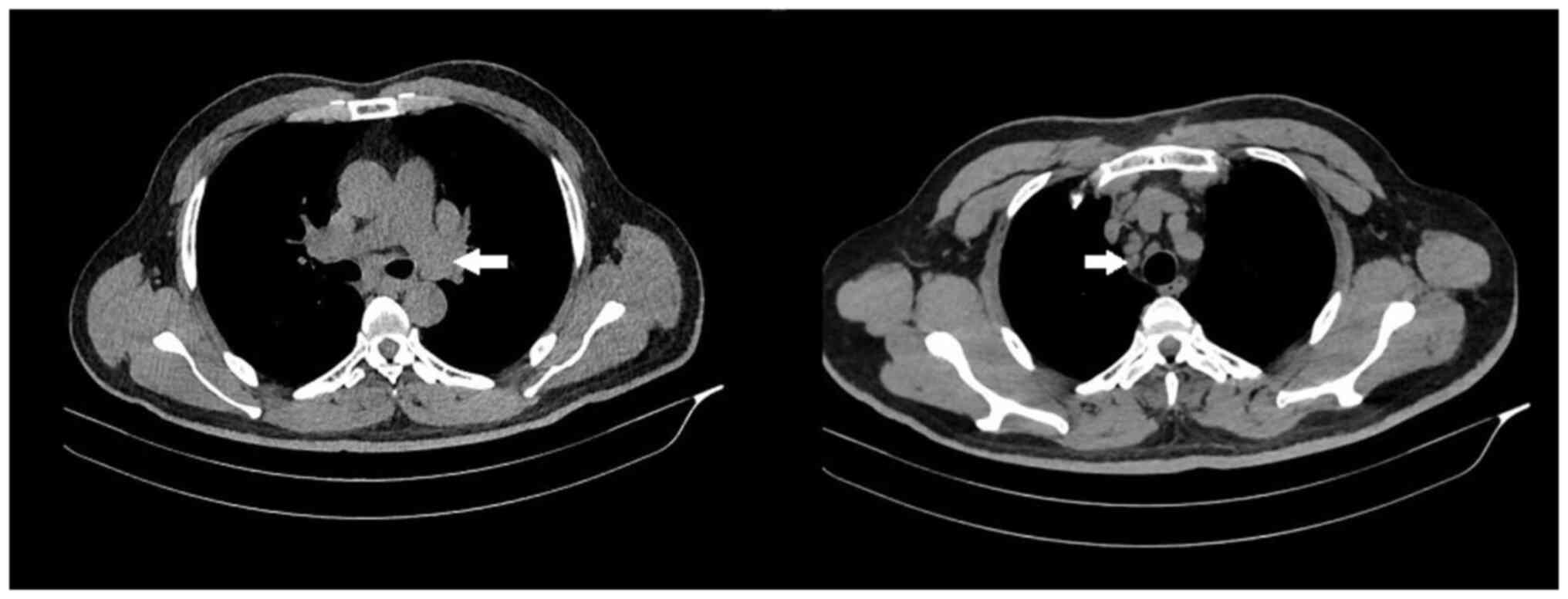
Chest CT revealed lymphadenopathies in the bilateral
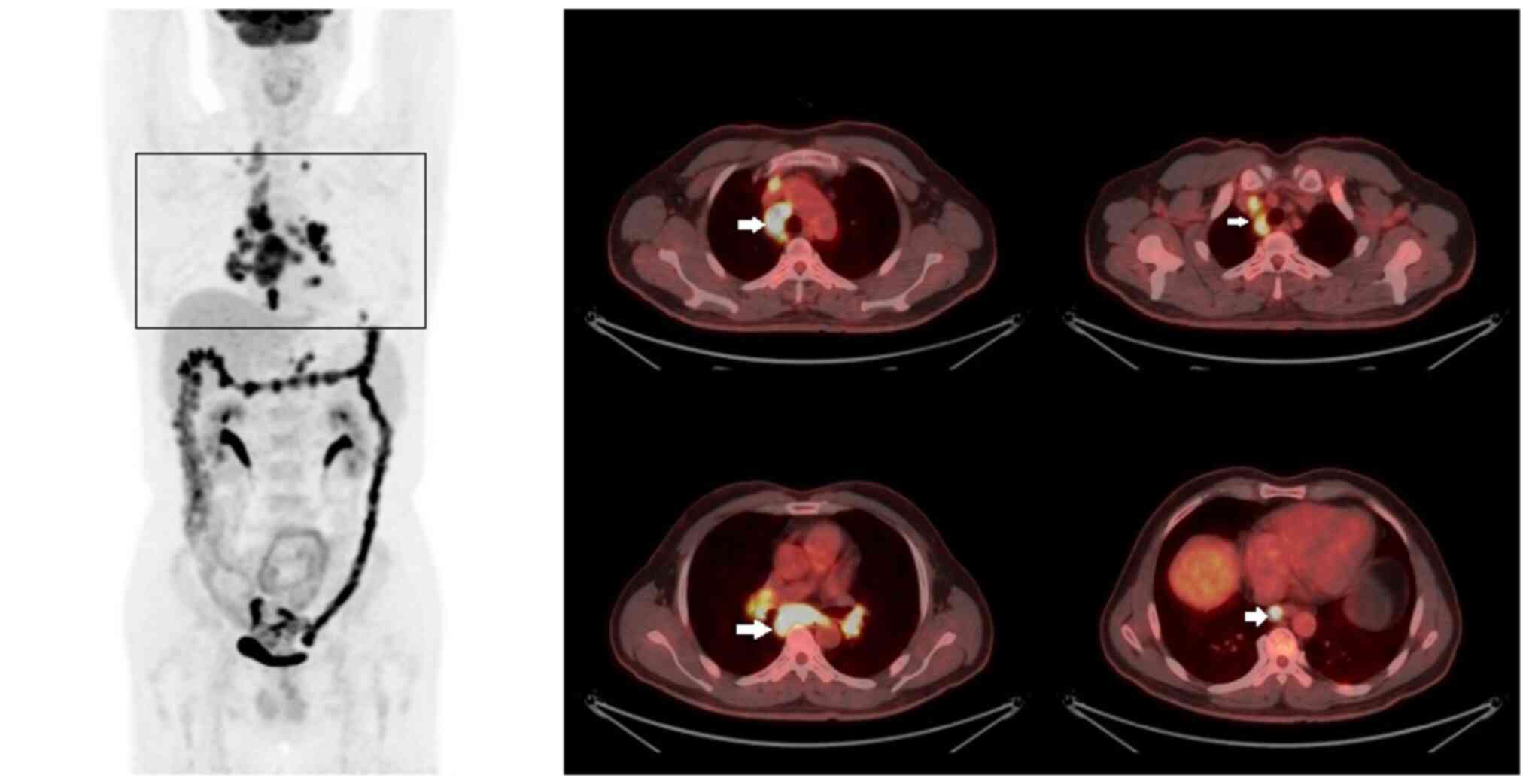
hilar, mediastinum and supraclavicular areas (Fig. 1). 18F-FDG PET-CT was
then performed to evaluate the whole-body condition and search for
the possibility of neoplastic foci, such as lymphoma. The results
demonstrated multiple lymphadenopathies in the bilateral
supraclavicular regions, mediastinum, bilateral hilar and left
cardio-diaphragmatic angle, with pathological uptake [maximum
standardized uptake value (SUVmax)=19.49], suggesting
the possibility of malignancy. It also showed nodal abnormality in
the bilateral pleura (SUVmax=2.55). In addition,
abdominal PET-CT showed lymphadenopathies with high metabolic
activity (SUVmax=9.98) in the retroperitoneal area and bilateral
diaphragmatic angle, along with striped shape high metabolic
activity of the small and large intestine (SUVmax=12.19), likely an
inflammatory disease due to the presence (Fig. 2). Gastrointestinal endoscopy
revealed intestinal polyps (data not shown), where further
pathological examination indicated hyperplastic polyps to rule out
cancer.
For histopathological examinations, samples of
tissues from right supraclavicular lymph node and mediastinal
masses were fixed in 10% neutral buffered formalin for 24 h at room
temperature. The samples were then embedded in paraffin and
sectioned into 4-µm sections. For H&E staining, tissue sections
were washed successively with xylene, 95% ethanol, 85% ethanol, 70%
ethanol, and double distilled water, then hematoxylin stain was
used for 5 min and eosin for 1 min, both at room temperature. The
samples were observed using a light microscope (magnification,
x200). For Ziehl-Neelsen staining, the following protocol was
applied: i) For the primary stain, Carbol fuchsin was prepared by
dissolving 1 g basic fuchsin in 10 ml ethanol (100%), whilst 5 g
carbolic acid was dissolved in 100 ml distilled water at the same
time, before these two aforementioned reagents were mixed together.
A piece of filter paper was first placed on the paraffin section
before the carbol fuchsin was dropped onto the paper. This was left
to stain for 30 min at room temperature; ii) the section was rinsed
with water, followed by 5% hydrochloric acid in ethanol for 10 sec
at room temperature; and iii) the section was covered with 0.7%
methylene blue for 5-10 sec at room temperature and observed with a
light microscope (magnification, x200). Bacteria would be stained
with bright red color.
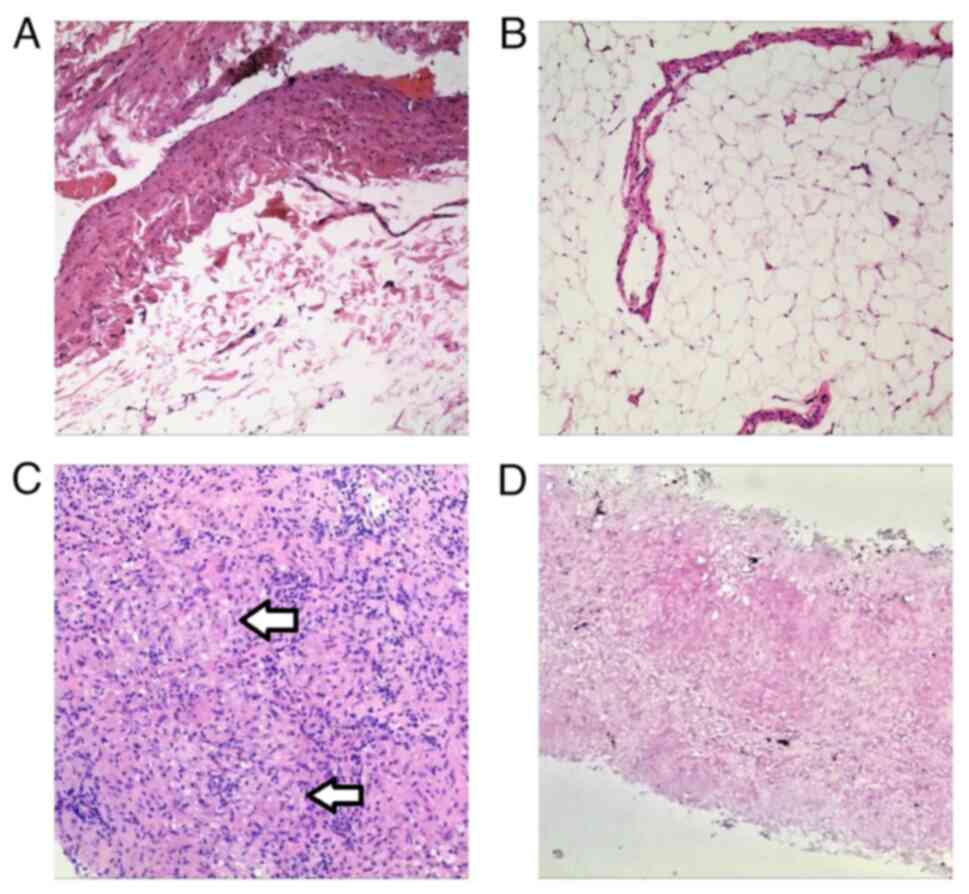
Pathological examination was performed 3 days after
the patient's admission to the hospital, right supraclavicular
lymph node dissection was performed at first due to its
approachable position, the result revealed reactive adenopathy
(Fig. 3A and B). Subsequently CT-guided biopsy of the
mediastinal masses was performed 1 week later, where non-caseating
epithelioid granulomas and negative Ziehl-Neelsen staining were
observed (Fig. 3C and D).
The patient had no cough or sputum, meaning sputum
culture that is normally used for detecting tubercle
bacillus was not available. However, the patient had no prior
history of tuberculosis, no symptoms of tuberculosis and his
pathological granulomas region showed negative Ziehl-Neelsen
staining, which all suggested that the patient did not have active
tuberculosis. Considering the clinical features, disease history
and the pathological examination results of the patient, there were
no concrete elements supporting cancer, therefore sarcoidosis was
deemed the most likely diagnosis. The patient was diagnosed with
sarcoidosis manifesting as multiple lymphadenopathies. The
patient's chest pain was gradually relieved without treatment and
discharged one week after he presented, and condition of the
patient remained stable at last follow-up in August 2023.
Discussion
A dysregulated immunoinflammatory response against
antigens can be observed in sarcoidosis and other granuloma-forming
diseases caused by acute or chronic bacterial and viral infections
(16). Some patients with
SARS-CoV-2 developed subcutaneous nodules with granulomatous
histology similar to sarcoidosis (17-19).
Subcutaneous nodules on the arms, shins, lateral thighs, glabella,
submental and bilateral pulmonary hilar lymphadenopathy have been
detected in patients within 1-2 weeks of a positive RT-qPCR result
for SARS-CoV-2(20). It was
hypothesized that the two diseases may share common pathological
activities, including the regulation of apoptosis and immune
tolerance through the programmed cell death protein-1/programmed
death ligand-1 axis (21-23).
In the present case, the patient was diagnosed with sarcoidosis 1
month after infection with SARS-CoV-2. Although the patient did not
have chest radiography when SARS-CoV-2 was detected, on the basis
of his symptoms and clinical history, it was hypothesized that
there was a potential link between sarcoidosis and COVID-19.
T-SOPT.TB is a type of IFN-γ release assay (IGRA)
that is widely used to identify infection by tubercle
bacillus (24). A previous
meta-analysis by Sester et al (20) indicated that the sensitivity of
IGRAs in patients with bacteriologically confirmed tuberculosis was
80-81%, whilst the specificity was 59% (20). By contrast, in another study, the
sensitivity was reported to be 87.5% whereas the specificity was
86% (25). In addition, there
appeared to be a low rate of T-SPOT.TB positivity in patients with
sarcoidosis regardless of the stage, where the possible mechanism
may be associated with shared immune response (26). According to the WHO-consolidated
guidelines on tuberculosis, Module 3: Diagnosis-Tests for
tuberculosis infection (27),
T-SPOT.TB can be used to test for tuberculosis infection but with
exceptionally low certainty of evidence. Therefore, IGRAs alone are
insufficient for the diagnosis of TB in patients with sarcoidosis
and requires both pathological and microbiological evidence.
Traditional diagnostic approaches, such as CT and
X-ray, are particularly useful for the detection of pulmonary
sarcoidosis, but they have limits for the evaluation of
extrapulmonary involvement. 18F-FDG PET-CT is widely
used for the diagnosis, staging and therapeutic assessment of
malignancies and inflammatory diseases. It can reveal the
anatomical localization of residual FDG uptake throughout the whole
body, providing guidance for further diagnostic tests (28,29).
Previous studies have demonstrated the good diagnostic performance
of 18F-FDG PET-CT for several inflammatory and
infectious diseases, including fever of unknown origin and
inflammation of unknown origin (30,31).
The 18F-FDG PET-CT result of the present patient
revealed extrathoracic involvement that traditional CT examination
could not fully detect, such that the value of FDG uptake further
guided subsequent lymph node biopsy.
The diagnosis of sarcoidosis is mainly based on the
exhibition of non-caseating epithelioid granulomas (5). In the present case, the pathological
examination of right supraclavicular lymph node showed only
reactive lymphadenopathy. Therefore, the pathological diagnosis of
sarcoidosis will likely require biopsy procedures of more than one
site and whether mediastinal biopsy will yield a superior
pathological positive rate compared with other sites for diagnosing
thoracic sarcoidosis needs further validation.
Although sarcoidosis developing after COVID-19 has
been reported previously (32),
the patient in the present case had a unique clinical performance
other than the typical respiratory symptoms. In addition, the
patient was tested T-SPOT.TB-positive, which necessitated
additional procedures in delineating the diagnosis from active
tuberculosis. Therefore, to the best of our knowledge, the present
case was the first to document the convergence of all three
diseases into discussion. In conclusion, results of the present
case suggest a possible link between SARS-CoV-2 infection and
sarcoidosis pathogenesis. In addition, T-SPOT.TB positivity alone
will likely not be sufficient for diagnosing TB in patients with
sarcoidosis. A diagnostic case with radiological examinations using
18F-FDG PET-CT and multisite biopsy reported in the
present account potentially provides a guide for the accurate
diagnosis of sarcoidosis.
Supplementary Material
Amplification plot of the patient in
early December 2022. The Ct values for ORFlab gene, N gene and E
gene of the patient were all <40, indicating severe acute
respiratory syndrome coronavirus 2-positivity.
Acknowledgements
Not applicable.
Funding
Funding: The present case was supported by the National Natural
Science Foundation of China (grant nos. 82072725 and 81972333) and
the Natural Science Foundation of Jiangsu Province (grant no.
BK20211134).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
QW and XC designed and supervised the study. XL and
JG analyzed the data and images. QW and CC performed the literature
review and wrote the manuscript. QW, CC and XL confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Drent M, Crouser ED and Grunewald J:
Challenges of sarcoidosis and its management. N Engl J Med.
385:1018–1032. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Shahgaldi S, Abbasi A and Rahmani-Kukia N:
A rapid qualitative review of sarcoidosis: Clinical manifestations,
immunopathogenesis, diagnosis and treatment. Mini Rev Med Chem.
22:1619–1630. 2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Dubaniewicz A: Mycobacterial heat shock
proteins in sarcoidosis and tuberculosis. Int J Mol Sci.
24(5084)2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Belperio JA, Fishbein MC, Abtin F,
Channick J, Balasubramanian SA and Lynch Iii JP: Pulmonary
sarcoidosis: A comprehensive review: Past to present. J Autoimmun:
Oct 19, 2023 (Epub ahead of print).
|
|
5
|
Sève P, Pacheco Y, Durupt F, Jamilloux Y,
Gerfaud-Valentin M, Isaac S, Boussel L, Calender A, Androdias G,
Valeyre D and El Jammal T: Sarcoidosis: A clinical overview from
symptoms to diagnosis. Cells. 10(766)2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Bonham CA, Strek ME and Patterson KC: From
granuloma to fibrosis: Sarcoidosis associated pulmonary fibrosis.
Curr Opin Pulm Med. 22:484–491. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Yazdanpanah N and Rezaei N: Autoimmune
complications of COVID-19. J Med Virol. 94:54–62. 2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Liu Y, Sawalha AH and Lu Q: COVID-19 and
autoimmune diseases. Curr Opin Rheumatol. 33:155–162.
2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Tana C, Cinetto F, Mantini C,
Bernardinello N, Tana M, Ricci F, Ticinesi A, Meschi T, Scarpa R,
Cipollone F, et al: Sarcoidosis and COVID-19: At the cross-road
between immunopathology and clinical manifestation. Biomedicines.
10(2525)2022.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Tana C, Donatiello I, Caputo A, Tana M,
Naccarelli T, Mantini C, Ricci F, Ticinesi A, Meschi T, Cipollone F
and Giamberardino MA: Clinical features, histopathology and
differential diagnosis of sarcoidosis. Cells. 11(59)2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gupta D, Agarwal R, Aggarwal AN and Jindal
SK: Sarcoidosis and tuberculosis: The same disease with different
manifestations or similar manifestations of different disorders.
Curr Opin Pulm Med. 18:506–516. 2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Agrawal R, Kee AR, Ang L, Tun Hang Y,
Gupta V, Kon OM, Mitchell D, Zierhut M and Pavesio C: Tuberculosis
or sarcoidosis: Opposite ends of the same disease spectrum?
Tuberculosis (Edinb). 98:21–26. 2016.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Cho HS, Kim SJ and Yoo JY: Sarcoidosis
during treatment of pulmonary tuberculosis: A rare case report and
review of the literature. J Int Med Res.
49(3000605211001632)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kaur H, Singh D and Pandhi N: Co-existence
of pulmonary tuberculosis with sarcoidosis. Int J Mycobacteriol.
10:341–343. 2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Yang M, Cao S, Liu Y, Zhang Z, Zheng R, Li
Y, Zhou J, Zong C, Cao D and Qin X: Performance verification of
five commercial RT-qPCR diagnostic kits for SARS-CoV-2. Clin Chim
Acta. 525:46–53. 2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Timmermans WM, van Laar JA, van Hagen PM
and van Zelm MC: Immunopathogenesis of granulomas in chronic
autoinflammatory diseases. Clin Transl Immunology.
5(e118)2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Tana C, Mantini C, Cipollone F and
Giamberardino MA: Chest imaging of patients with sarcoidosis and
SARS-CoV-2 Infection. Current evidence and clinical perspectives.
Diagnostics (Basel). 11(183)2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Behbahani S, Baltz JO, Droms R, Deng AC,
Amano SU, Levin NA, O'Brien MC and Wiss K: Sarcoid-like reaction in
a patient recovering from coronavirus disease 19 pneumonia. JAAD
Case Rep. 6:915–917. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Polat Ekinci A, Büyükbabani N, Meşe S,
Pehlivan G, Okumuş NG, Ağaçfidan A and Özkaya E: COVID-19-triggered
sarcoidal granulomas mimicking scar sarcoidosis. J Eur Acad
Dermatol Venereol. 35:e477–e480. 2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Sester M, Sotgiu G, Lange C, Giehl C,
Girardi E, Migliori GB, Bossink A, Dheda K, Diel R, Dominguez J, et
al: Interferon-γ release assays for the diagnosis of active
tuberculosis: A systematic review and meta-analysis. Eur Respir J.
37:100–111. 2011.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Zhao M, Tian C, Cong S, Di X and Wang K:
From COVID-19 to Sarcoidosis: How similar are these two diseases?
Front Immunol. 13(877303)2022.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Mazzoni A, Maggi L, Capone M, Spinicci M,
Salvati L, Colao MG, Vanni A, Kiros ST, Mencarini J, Zammarchi L,
et al: Cell-mediated and humoral adaptive immune responses to
SARS-CoV-2 are lower in asymptomatic than symptomatic COVID-19
patients. Eur J Immunol. 50:2013–2024. 2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Jubel JM, Barbati ZR, Burger C, Wirtz DC
and Schildberg FA: The Role of PD-1 in acute and chronic infection.
Front Immunol. 11(487)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kim KJ, Ryu SE, Lee HN, Oh SH and Chang
CL: Evaluation of a new chemiluminescent immunoassay-based
interferon-gamma release assay for detection of latent tuberculosis
infection. Medicina (Kaunas). 59(1734)2023.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Diel R, Loddenkemper R and Nienhaus A:
Evidence-based comparison of commercial interferon-gamma release
assays for detecting active TB: A metaanalysis. Chest. 137:952–968.
2010.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Kempisty A, Białas-Chromiec B, Borkowska D
and Kuś J: Interferon gamma release assays based on M.
tuberculosis-specific antigens in sarcoidosis patients. Pneumonol
Alergol Pol. 83:126–134. 2015.PubMed/NCBI View Article : Google Scholar
|
|
27
|
https://www.who.int/publications/i/item/9789240056084.
|
|
28
|
Chen X, Xu X, Chrysikos S, Zhao M and Zhou
Y: Value of 18-fluorodeoxyglucose positron emission
tomography/computed tomography (18F-FDG PET/CT) in the differential
diagnosis of sarcoidosis and lung cancer with lymph node
metastasis: A retrospective study. Transl Lung Cancer Res.
11:1926–1935. 2022.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Tetikkurt C, Yanardag H, Sayman BH, Bilir
M, Tetikkurt S, Bilgic S, Kubat B and Bilgin S: Diagnostic utility
of 68Ga-citrate and 18FDG PET/CT in sarcoidosis patients. Monaldi
Arch Chest Dis. 90:2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Kouijzer IJE, Mulders-Manders CM,
Bleeker-Rovers CP and Oyen WJG: Fever of unknown origin: The Value
of FDG-PET/CT. Semin Nucl Med. 48:100–107. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Régis C, Benali K and Rouzet F: FDG PET/CT
imaging of sarcoidosis. Semin Nucl Med. 53:258–272. 2023.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Racil H, Znegui T, Maazoui S, Touil A,
Habibech S, Henda N and Chaouch N: Can coronavirus disease 2019
induce sarcoidosis: A case report. Thorac Res Pract. 24:45–58.
2023.PubMed/NCBI View Article : Google Scholar
|