1. Introduction
Normal pregnancy is associated with significant
maternal cardiovascular hemodynamic alterations, necessary for the
optimal development of the growing fetus and the protection of the
mother (1,2). Maternal blood volume progressively
increases from the first weeks of gestation and reaches a peak of
40-50% above non-pregnant volumes at ~34-36 weeks of gestation,
where it remains at these levels until term (1,3,4).
The increase in maternal blood volume is required to provide
increased blood flow throughout the placenta, a highly vascular
organ, which is the primary site for maternal-fetal exchange of
nutrients, gases and waste. Placental vascular network development
requires vasculogenesis, and branching and non-branching
angiogenesis, which are regulated by the coordination between
different vascular endothelial growth factors and cell types
(5). The dysregulation of
placental vascular development leads to placental dysfunction
associated with various serious obstetric complications, such as
preeclampsia (PE), intrauterine growth restriction (IUGR), pre-term
birth and stillbirth (5,6).
PE is a pregnancy-specific multisystem disorder,
affecting 2-7% of all pregnancies (7,8).
It is a major cause of maternal and fetal/perinatal morbidity and
mortality worldwide (15-20% in developed countries), leading to
~70,000 direct maternal deaths and ~500,000 perinatal deaths
annually (7,9). The main criteria for the clinical
diagnosis of PE are the new onset of hypertension and proteinuria
or in the absence of proteinuria, new-onset hypertension with the
new onset of any of the following: Thrombocytopenia, elevated
levels of liver transaminases, pulmonary edema, new-onset renal
insufficiency, or cerebral or visual disturbances (8). Moreover, women who develop PE are at
an increased risk of also developing cardiovascular complications
later on in life (7). PE is
classified as early-onset PE (EOPE), which accounts for 5-20% of
all PE cases and develops prior to 34 weeks of gestation and
late-onset (LOPE), which accounts for 80-95% of cases worldwide and
develops after 34 weeks of gestation (10,11). EOPE is usually more severe and is
associated with a high rate of IUGR, while LOPE is associated with
eclampsia and hemolysis, elevated liver enzymes, and low platelets
(HELLP) (10,11).
Although it is commonly acknowledged that PE is
caused by placental dysfunction, its underlying pathophysiology
remains incompletely understood (7). In 1991, Redman (12) introduced the two-stage model of PE
pathophysiology: Stage 1 (preclinical, placental stage), which
occurs during the 1st half of pregnancy, is caused by placental
dysfunction with unremodeling of spiral arteries and uteroplacental
malperfusion, leading to placental hypoxia (ischemia); and stage 2
(clinical, maternal stage), which occurs during the 2nd half of the
pregnancy and is hypothesized to be a consequence of stage 1, as
hypoxic placenta causes the increased release of numerous
biological factors into the maternal circulation leading to
endothelial dysfunction (Fig.
1A). An updated two-stage model was suggested in 2019 (11), in which at least two or more
different pathways lead to stage 1 (Fig. 1B). The extrinsic placental
pathway, is the classical dysfunctional placentation pathway
leading to secondary syncytiotrophoblast (STB) stress and the
release of pro-inflammatory factors into the maternal circulation,
which develops early in pregnancy and leads to EOPE accompanied
very often by IUGR. The intrinsic placental pathway arises due to
the placental outgrowing uterine capacity with restricted
intervillous perfusion, also causing STB stress, which develops
late in pregnancy and leads to LOPE with normal fetal growth
(11). Another potential pathway
leading to STB stress is the excessive trophoblast senescence of
ageing placenta. STB stress has been shown to stimulate the release
of multiple factors in the maternal circulation including
hypoxia-inducible factor 1α, endothelin-1, syncytiotrophoblast
microparticles, angiotensin II 1 receptor autoantibodies (AT1-AA),
nitric oxide (NO), oxidative stress, endoplasmic reticulum stress
and angiogenic factors and their receptors (13,14). The updated model also incorporates
maternal factors, including genetic, genetic, behavioral,
immunological and environmental factors, which may affect both
stages of PE.
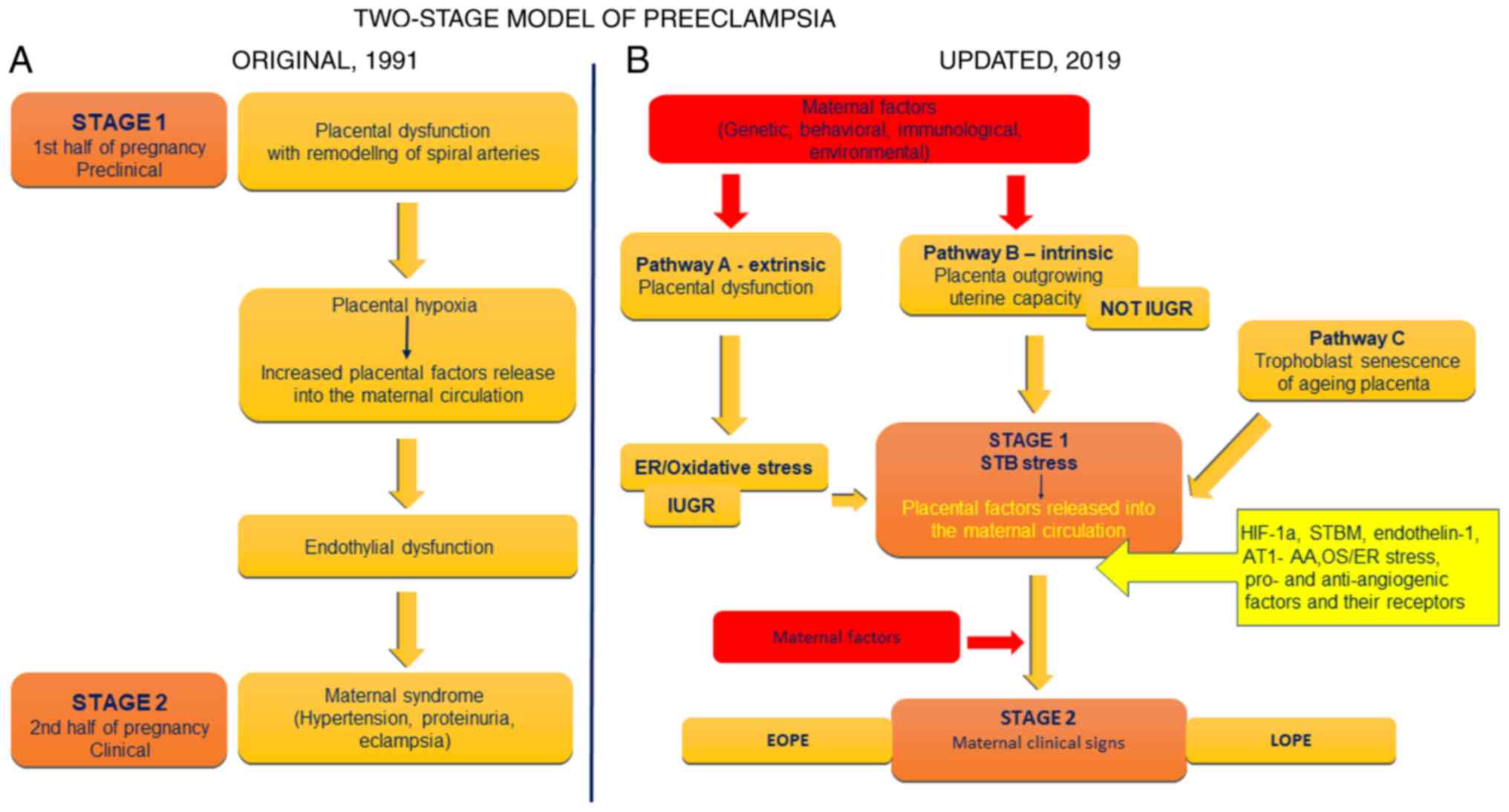 | Figure 1Two-stage model of PE
pathophysiology. (A) Original model proposed in 1991 and (B)
updated model suggested in 2019. PE, preeclampsia; ER, endoplasmic
reticulum; IUGR, intrauterine growth retardation; EOPE, early-onset
PE; STB, secondary syncytiotrophoblast; HIF-1α, hypoxia-induced
factor 1α; STBM, syncytiotrophoblast microparticles; OS, oxidative
stress; AT1-AA, angiotensin II 1 receptor autoantibodies; LOPE,
late-onset preeclampsia. |
2. Angiogenic growth factors and their
receptors in PE
In normal placental vasculogenesis, extravillous
cytotrophoblasts invade the myometrium spiral arteries and replace
the endothelial layer of the uterine vessels, transforming them
into elastic, soft, wide, low-resistance blood vessels, thus
allowing increased uterine blood flow and adequate oxygen and
nutrients supplies to the fetus (Fig.
2) (5,6,15).
In PE, there is trophoblast dysfunction and the incomplete
remodeling of spiral uterine arteries, causing placental hypoxia,
oxidative stress and endothelial dysfunction responsible for the
clinical symptoms (Fig. 2)
(6,15-22). Interactions between angiogenic
factors and their receptors contribute to placental angiogenic
balance and are responsible for the maintenance and development of
the placental vasculature (Fig.
2) (5,15,23-26).
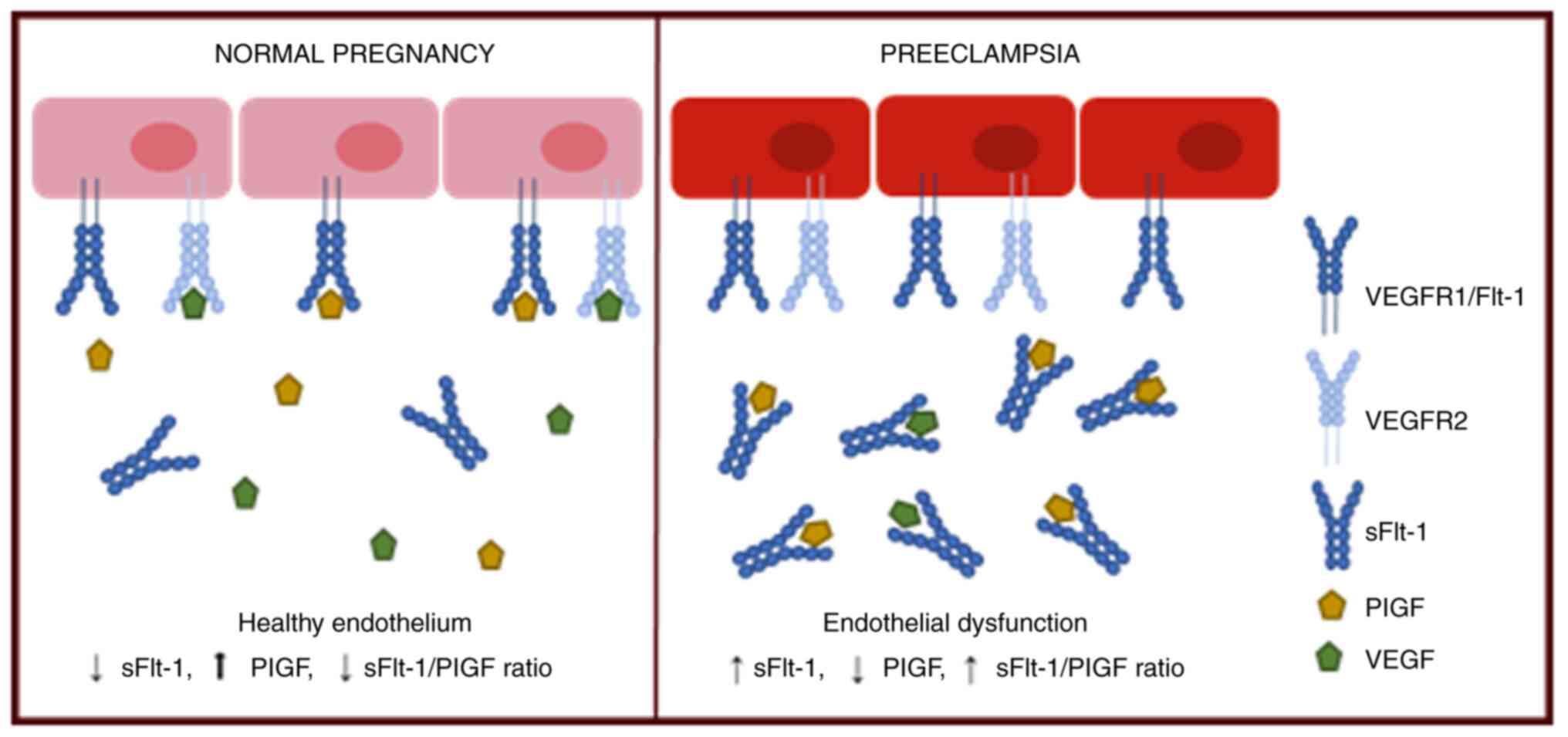
VEGF and PlGF belong to the VEGF family and have
angiogenic properties, while sFlt-1 and sEng exert anti-angiogenic
effects (6). Reference values for
pro- and anti-angiogenic factors and their protein tyrosine kinase
receptors (VEGFRs) in the serum of normal pregnant women have been
established (27) and different
serum concentrations of these factors have been found in women with
PE compared to those in women with normotensive pregnancies,
indicating their inolvement in the pathogenesis of PE (Fig. 2) (5,6,13-15,18-22). The complex etiology and
pathophysiology of PE emphasizes the need for a clinically useful
biochemical marker for the diagnosis and subsequent prediction and
management of PE.
VEGF (or VEGF-A) is a member of the human VEGF
family, which also includes VEGF-B, VEGF-C, VEGF-D and PlGF, and
their signals are mediated by their receptors, VEGFR-1/sFlt-1,
VEGFR-2/KDR and VEGFR-3/Flt-4 (6,20,21,26,28). VEGF is produced by several cell
types, including macrophages, keratinocytes, T-cells, tumor cells
and cytotrophoblasts, and plays a key role in the regulation and
differentiation of the vascular system (6,20,21,26,28). VEGF-A in the placenta induces
vascular permeability and endothelial cell proliferation, maintains
the integrity of newly formed capillaries and regulates trophoblast
proliferation, differentiation and invasion (6,20).
VEGF is a 45-kDa glycoprotein encoded by the VEGF gene, which is
located on chromosome 6p21.1 (28,29). Through alternative mRNA splicing,
several VEGF-A subtypes are generated, with VEGF-A165 being the
predominant one (26,28).
PlGF was first identified in a placenta cDNA library
in 1991 (30). It belongs to the
cysteine-knot growth factor family and it has both angiogenic and
pro-inflammatory functions (6,31).
PlGF is expressed in trophoblasts, endothelial and epithelial
cells, the skin, certain tumors, and the heart, lungs, thyroid and
skeletal muscle (31). PIGF is a
45-50-kDa dimeric glycoprotein produced by the PIGF gene, which is
located on chromosome 14q24 (6,31).
Due to alternative mRNA splicing, four isoforms are encoded
composed of 131, 152, 203 and 224 amino acids (31). PlGF shares a 53% homology with
VEGF (6,30,31).
VEGF binds with high affinity to both sFlt-1 and KDR
receptors and promotes branching angiogenesis (first trimester of
pregnancy), while PlGF binds with high affinity exclusively to
sFlt-1 and leads to non-branching angiogenesis (second trimester)
(5,6,26,31-33). sFlt-1 and KDR receptors both have
an extra cellular ligand binding domain, a transmembrane domain and
an intracellular tyrosine kinase domain (6,15).
The Flt-1 gene is located on chromosome 13q12 and
encodes a 186-kDa glycoprotein (6,15,34). The sFlt-1 protein is a splice
variant of VEGFR-1, a 100-kDa variably glycosylated protein, which
includes the extracellular ligand-binding domain and lacks the
transmembrane and intracellular domains, thus it is secreted
(soluble), and acts as a VEGF and PlGF antagonist, thus preventing
their activity (15,26,33,34). sFlt1 is found in endothelial
cells, monocytes, trophoblasts, vascular smooth muscle cells,
dendritic cells, renal mesangial cells and various human tumor cell
types (6,15,33). Multiple isoforms of sFlt1 have
been reported, which are differentially expressed and distributed
in human tissues, and may be associated with a variety of
physiological and pathological roles (34,35). In humans, sFLT-1 i13 is the main
sFLT-1 variant and is widely expressed in the majority of tissues,
whereas the sFLT-1 e15a variant appears to be the main protein in
the circulation of women with PE (34,35). Although sFLt-1 placental
derivation is well known, the upstream mechanisms regulating its
release are poorly characterized. A recent study identified that
epidermal growth factor receptor and mitochondrial signaling
pathways positively regulated the placental release of sFlt-1 and
may play central roles in the pathogenesis of PE (36).
Other factors have also been observed in the plasma
of women with PE, such as increased sEng, NO, AT1-AA, cellular
fibronectin and decreased heme oxygenase-1 and prostacyclin levels,
suggesting a possible involvement in the pathogenesis of PE
(Fig. 3) (19,37).
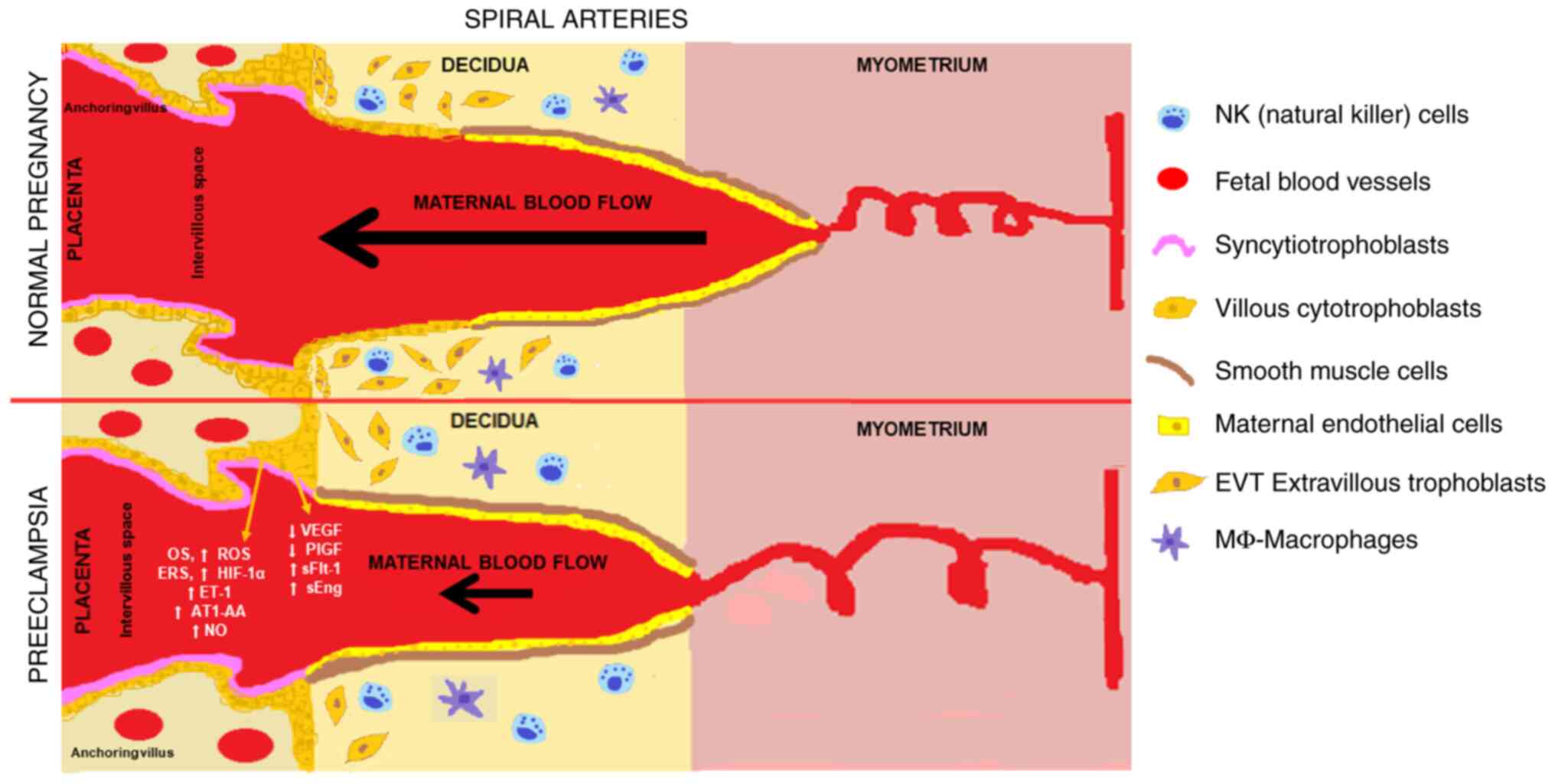 | Figure 3Spiral arteries remodeling in normal
pregnancy and in preeclampsia. OS, oxidative stress; ROS, reactive
oxygen species; ERS, endoplasmic reticulum stress; HIF-1α,
hypoxia-induced factor 1α; NO, nitric oxide; AT1-AA, angiotensin II
1 receptor autoantibodies; PlGF, placental growth factor; VEGF,
vascular endothelial growth factor; sFlt-1, soluble fms-like
tyrosine kinase 1; sEng, soluble endoglin. |
3. PlGF and sFlt-1 in PE
Extensive research has demonstrated the role of VEGF
angiogenic factors and their receptors in the pathophysiology of PE
and numerous scientists have been focused on their evaluation as
candidate biomarkers in order to develop an efficient screening
test with diagnostic and predictive potential for PE (6,15-19). Free VEGF plasma concentrations
during pregnancy are low and often below the detection limit of
most commercially available diagnostic kits (18).
Increased levels of sFlt-1 and decreased levels of
PlGF in maternal serum have been observed from early pregnancy in
women with PE, suggesting a blockade of PlGF action by sFlt-1
(15-20,33,38-59) (Table
I). In 2003, Maynard et al (38) demonstrated almost 5-fold higher
placental and serum sFlt-1 levels in women with PE compared to
normotensive pregnant women. Of note, the sFlt-1 levels decreased
in preeclamptic women 48 h after delivery, suggesting its placental
origin (38). Moreover, decreased
levels of free serum VEGF and PlGF were found in patients with PE
compared to normal controls, which was proportionate to the rise in
serum sFlt1 levels in these patients (38). Another two studies demonstrated
significantly higher serum levels of sFlt-1 (an almost 6-fold
increase) and lower free PlGF levels in women with PE than those
from non-pregnant women (16,17).
 | Table IPIGF and sFlt-1 in PE. |
Table I
PIGF and sFlt-1 in PE.
| Authors/year of
publication | Patient
population | Sample size | Findings | (Refs.) |
|---|
| Maynard et
al, 2003 | Mild and severe
PE | 11 women with mild
PE, 10 women with severe PE, 10 normal pregnant after 30th week of
pregnancy | Serum sFlt-1 level
was 5-fold higher in patients with severe PE than in normotensive
pregnant women sFlt-1 levels felt in preeclamptic women 48 h after
delivery. Decreased levels of free serum VEGF and PlGF in PE
patients compared to normal controls | (38) |
| Koga et al,
2003 | PE | 31 women with PE
between 18-40 weeks of pregnancy, 52 nonpregnant women | Serum sFlt-1
concentrations in women with PE were >6-fold higher than
non-pregnant women | (16) |
| Tsatsaris et
al, 2004 | Severe PE/IUGR | 60 pregnant women
(19 with severe PE, 10 with IUGR infant, 31 with no complicated
pregnancy used as controls) | Significantly
higher serum sFlt-1 levels and lower free PlGF levels in
pregnancies with PE and IUGR, compared with normal pregnancies at
term or matched for gestational age | (17) |
| Levine et
al, 2004 | Mild and severe
PE | 120 women with PE
(80 had mild and 40 had severe PE), 120 normotensive controls
[calcium for preeclampsia prevention (CPEP) trial] | sFlt-1
concentrations begin to increase 5 weeks before the onset of PE
with a parallel decrease in the free PlGF and VEGF levels;
association between serum sFlt-1 levels and the severity of PE as
women with pre-term PE or PE and IUGR infant had higher serum
sFlt-1 levels and lower PlGF levels at 21-32 weeks and at 33-41
weeks than those with an onset of PE at term or PE without an IUGR
infant, respectively. Increased sFlt-1 levels in normotensive
pregnancy and decreased PlGF levels during the last 2 months of
pregnancy | (18) |
| Thadhani et
al, 2004 | PE with gestational
hypertension/ IUGR | 40 women who
developed PE, 40 women with gestational hypertension, 40 women with
an IUGR infant, 80 normal pregnant women in the 1st trimester of
pregnancy | The combination of
1st trimester serum levels of sFlt-1 and PlGF identify women who
are at a high risk of developing PE | (39) |
| Chaiworapongsa
et al, 2005 | PE | 44 patients with
PE, 44 normal pregnant women | Elevation of serum
plasma sFlt-1 6-10 weeks prior to clinical signs of PE Plasma
sFlt-1 concentration raised both in early-onset and late-onset
disease, but in early-onset PE plasma sFlt-1 concentration was
elevated earlier than the late-onset. The optimal time forthe
determination of plasma sFlt-1 concentrations for diagnostic
purposes is 28-32 weeks of gestation (mean, 30 weeks) for EOPE and
30-34 weeks of gestation (mean, 32 weeks) for LOPE, or ~1 month
before its clinical diagnosis | (40) |
| Buhimschi et
al, 2005 | PE/pregnant
hypertensive/ proteinuric women | 17 women with
severe PE, 21 pregnant hypertensive and pro teinuric women who did
not meet criteria for severe PE, 16 healthy pregnant control, 14
non-pregnant reproductive age | Increased urinary
levels of sFlt-1 but decreased urinary PlGF expression in
hypertensive pregnant women Urinary sFlt-1-to-PlGF (uFP) ratio has
highsensitivity and specificity in differentiating women with
severe PE from normotensive controls and even more could
discriminate severe PE from other hypertensive disorders | (41) |
| Hirashima et
al, 2005 | PE | 148 women (4 with
PE who delivered at <37 weeks of gestation, 2 with PE who
delivered at ≥37 weeks of gestation and 142 normal pregnant women)
at 10, 18, 28, and 37 weeks of gestation | In normal
pregnancies, the concentration of serum sFlt-1 decreased from 8-12
weeks to 16-20 weeks, gradually increased at 26-30 weeks and
rapidly increased at 35-39 weeks of gestation Serum free PlGF
concentration increased from 8-12 weeks to 26-30 weeks and then
decreased at 35-39 weeks of gestation Decrease in serum free PlGF
levels in women with PE in both the first and the second trimester
before the onset of PE Higher serum sFlt-1 levels after 21 weeks of
gestation, but not before 21 weeks | (27) |
| Ohkuchi et
al, 2007 | Severe EOPE (<32
weeks)/ severe LOPE (≥32 weeks) | 14 women with EOPE
(<32 weeks) severe PE, 20 women with LOPE (≥32 weeks) severe PE,
65 normotensive controls (28-34 weeks of gestation) | Decreased serum
PlGF and increased serum sFlt-1 levels in EOPE and LOPE women with
PE compared to normotensive controls at 28 and 37 weeks Decreased
serum PlGF with concomitant increased sFlt-1 levels were more
pronounced in EOPE than in LOPE The sFlt-1/PlGF ratios at around 28
weeks of gestation before the onset of severe preeclampsia were
increased in 83% of cases | (42) |
| Levine et
al, 2006 | Term PE/pre-term
PE/gestational hyperten sion/IUGR | 120 women with term
PE, 72 women with preterm PE, 120 with gestational hypertension,
120 normotensive women with an IUGR infant, 120 normal pregnant
women | sFlt-1/PlGF ratio
increases in women with PE beginning 2 to 3 months before the onset
of the disease | (37) |
| Stepan et
al, 2007 | Abnormal uterine
perfusion | 63 sec trimester
pregnant women with abnormal uterine perfusion: 25 developed a
later complication (12 with PE, 11 with IUGR and 2 with
intrauterine death), 38 had a normal course of pregnancy | Significantly
higher serum sFlt1 and lower PlGF levels in pregnancies with
adverse pregnancy outcome compared with those with normal outcomes
Alterations were more pronounced in pregnancies with subsequent PE
compared with IUGR and early-onset diseases (delivery <34 weeks)
compared with late-onset diseases) | (43) |
| De Vivo et
al, 2008 | EOPE (<37 weeks)
and LOPE (≥32 weeks) | 26 women with EOPE
(<37 weeks) and 26 women with LOPE (≥32 weeks), 52 healthy
pregnant women collected between 24-28 weeks of gestation | Increased
sFlt-1/PlGF ratio during gestation in both preeclamptic and control
group in both trimesters, but in the control group the increase was
moderate (51%), while in the preeclamptic group the increase was
notable (285%) Serum PlGf levels decreased in the 3rd trimester in
this group In the 2nd trimester, the sFlt-1/PlGF ratio was the
optimal predictor of PE with a specificity, a sensitivity, a
diagnostic accuracy, a positive predictive value and a negative
predictive value of 88.5% using a cut-off of 38.47 | (44) |
| Romero et
al, 2008 | PE/IUGR | 144 singleton
pregnant women (46 women with uncomplicated pregnancies who
delivered appropriate for gestational age neonates, 56 women who
delivered an IUGR neonate but did not develop PE, 42 women patients
who developed PE) | Changes in the
maternal plasma concentration of s-Eng, sFlt-1 and PlGF precede the
clinical presentation of PE, while only changes in s-Eng and PlGF
precede the delivery of an IUGR neonate | (45) |
| Ohkuchi et
al, 2010 | PE | 144 normal pregnant
women at 19-25, 27-31 and 34-38 weeks of gestation, from 34 women
with PE | The sFlt-1/PlGF
ratio was shown to have the optimal diagnostic power for both EOPE
and LOPE The cut-off value of 85 for the sFlt-1/ PlGF ratio might
assist in the diagnosis of preeclampsia, especially for EOPE | (46) |
| Verlohren et
al, 2010 | PE | 351 patients (71
patients with PE and 280 gestational age-matched control subjects)
from 5 European study centers | sFlt-1/PIGF ratio
had an area under the receiver operating characteristic curve (ROC)
of 0.95 and the optimal performance was obtained in the
identification of early-onset PE in an area under the curve of
0.97 | (47) |
| Sunderji et
al, 2010 | PE | 457 subjects (409
without PE and 48 with PE) at 20-36 weeks of gestation | A new system
clearly separated normotensive women from those with pre-term PE
with excellent sensitivity and specificity (95% for each biomarker)
with the sFlt-1/PlGF ratio exhibiting the optimal performance | (48) |
| Chaiworapongsa
et al, 2011 | PE | 87 patients
presenting to the to the obstetrical triage area with the suspicion
of PE (divided into four groups based on clinical severity of PE
and gestational age at delivery-term or preterm) at <37 weeks of
gestation, 180 women with uncomplicated pregnancies | Plasma
concentrations of angiogenic/ anti-angiogenic factors are of
prognostic value in the obstetrical triage area in identifying
patients with severe PE requiring preterm delivery within 2
weeks | (49) |
| Rana et al,
2012 | PE | 616 plasma samples
from women presenting to obstetrical triage <34 weeks of
gestation with suspected PE | Plasma sFlt1/PlGF
ratio >85 at presentation was predictive of adverse outcomes
occurring within 2 weeks and in these women this marker had better
results than other laboratory tests currently used | (50) |
| Moore et al,
2012 | Pregnancy
complications | 276 pregnant women
(78 with complications, 198 without complications) after 20 weeks
of gestation | Increased serum
sFlt1/PlGF ratio was associated with an increased odds of
complications among women presenting <37 weeks Multivariable
model combining the sFlt1:PlGF ratio with clinical variables was
more predictive of complications (AUC, 0.91; 95% CI, 0.85-0.97)
than a model using clinical variables alone (AUC, 0.82; 95% CI,
0.79-0.90) | (51) |
| Verlohren et
al, 2012 | PE/GH/CH | 630 women (388
singleton pregnancies with normal pregnancy outcome, 164 singleton
pregnancies with PE outcome, 36 subjects with gestational
hypertension (GH), 42 patients with chronic hypertension | Patients with PE
had significantly elevated sFlt-1/PlGF ratios as compared with
controls and with patients with chronic and gestational
hypertension in <34 weeks and ≥34 weeks of gestation Patients
with a sFlt-1/PlGF ratio in the highest quartile (P<0.001) had a
significantly reduced time to delivery In the <34 weeks PE
group, the early identification of high risk for delivery women was
strongly associated with maternal and fetal morbidity and mortality
as and the timely referral to an intensive care unit alone could
reduce perinatal morbidity and mortality by 20% | (52) |
| Herraiz et
al, 2014 | Fetal growth
restriction/PE or HELLP/ PE/HELLP/ fetal growth restriction | 171 women with
singleton pregnancies, complicated by fetal growth restriction
(n=27), PE or HELLP (n=105) or PE or HELLP and fetal growth
restriction (n=39), 171 gestational age matched healthy pregnant
women | Increased
sFlt-1/PlGF ratios in cases with fetal growth restriction, PE or
HELLP, and preeclampsia or HELLP and fetal growth restriction than
control pregnancies both <34 weeks and ≥34 weeks | (53) |
| Chaiworapongsa
et al, 2014 | Severe PE | 85 patients who
presented to the obstetrical triage area at 20-36 weeks with a
diagnosis of 'rule out PE' were included in the study (37 remained
stable until term (group I), 48 developed severe PE requiring
preterm delivery (group II) | Maternal plasma
concentrations of angiogenic/anti-angiogenic factors have prog
nostic value for patients presenting with suspected PE before 34
weeks of gestation | (54) |
| Rana et al,
2013 | PE/non-angiogenic
PE/angiogenic PE | 97 women presented
at GA <37 weeks in triage who deve loped PE within 2 weeks; 46
of the 97 women had non-angiogenic PE (sFlt1/PlGF ratio <85), 51
had angiogenic PE (sFlt1/ PlGF ratio ≥85) | Women with
non-angiogenic form of PE had a very low risk of adverse
outcomes | (55) |
| Gómez-Arriaga et
al, 2014 | PE | 51 singleton
pregnancies withearly-onset PE | Mean uterine artery
pulsatility index (UtA-PI) and sFlt-1/PlGF ratio in combination
with gestational age are useful for the prognostic assessment of
perinatal complications at the time of diagnosis of early-onset PE,
but not of maternal complications sFlt-1/PlGF ratio >655 is
closely related to the need to deliver within 48 h | (56) |
| Garcia-Tizon
Larroca et al, 2014 | PE | 2,140 women that
developed PE and 83,615 that were unaffected by PE | Screening by
biophysical and biochemical testing at 30-33 weeks could identify
most pregnancies developing PE and requiring delivery within the
subsequent 4 weeks | (57) |
| Verlohren et
al, 2014 | PE | 234 women with PE
and 915 controls | The use of
individual two cut-off values, one for EOPE and one for LOPE allows
maximized accuracy of diagnosis For EOPE, between 20+0
and 33+6 weeks of gestation, the cut-offs at ≤33 was
negative and at ≥85 was positive for PE/HELLP syndrome with a
sensitivity/ specificity of 95/94 and 88/99.5%, respectively For
LOPE, ≥34 weeks, the cut-offs at ≤33 and ≥110 resulted in lower
sensitivity/specificity of 89.6/73.1 and 58.2/95.5%,
respectively | (58) |
| Schoofs et
al, 2014 | PE/IUGR | 43 women with PE
including nine samples with EOPE <34 weeks, 24 with IUGR and 244
controls | Repeated
measurements of the sFlt-1/ PlGF ratio along with or in addition to
calculating the slope between two measurements seems to be superior
inpredicting preeclampsia to a single measurement of the
sFlt-1/PlGF ratio alone | (59) |
In 2004, Levine et al (18) demonstrated an increase in serum
sFlt-1 concentrations 5 weeks prior to the onset of PE with a
parallel decrease in the free PlGF and VEGF levels, which may have
been due to sFlt-1 binding. In addition, they demonstrated an
association between serum sFlt-1 levels and the severity of the
disease (18). In normotensive
pregnancy, the serum sFlt-1 levels were increased and PlGF levels
were decreased during the last 2 months of pregnancy (18). Their study suggested the relevance
of these markers to the early identification of PE and the
prediction of its severity (18).
Thadhani et al (39) suggested that the combination of
first trimester serum sFlt-1 and PlGF levels can identify women who
are at a high risk of developing PE. A subsequent study concluded
that the plasma sFlt-1 concentration began to increase 6-10 weeks
prior to the clinical manifestations of PE with a more pronounced
increase at 2-5 weeks before the diagnosis, as well as at clinical
presentation (40). Furthermore,
it was observed that the plasma sFlt-1 concentration increased both
in early- and late-onset disease, although in EOPE the elevation
occurred earlier than in LOPE; it was thus suggested that the
optimal time for the determination of plasma sFlt-1 concentrations
for diagnostic purposes was at 28-32 weeks of gestation for EOPE
and at 30-34 weeks of gestation for LOPE, or ~1 month before its
clinical diagnosis (40).
Buhimschi et al (41) observed that the urinary
sFlt-1-to-PlGF (uFP) ratio had a high sensitivity and specificity
in differentiating women with severe PE from normotensive controls,
as well as other hypertensive disorders; it was suggested that the
uFP ratio would be a better indicator for defining the severity of
the disease (41).
Hirashima et al (27) established the reference values for
serum sFlt-1, free PlGF and the sFlt-1/PlGF ratio with a 90%
confidence interval (90% CI) throughout pregnancy, useful for
identifying pregnant women who are at a high risk of developing PE.
In normal pregnancies, the serum concentration of sFlt-1 decreased
from 8-12 weeks to 16-20 weeks, gradually increased at 26-30 weeks
and rapidly increased at 35-39 weeks of gestation, while the serum
free PlGF concentration increased from 8-12 weeks to 26-30 weeks
and then decreased at 35-39 weeks of gestation, implying that the
cut-off value for PE should be changed according to the gestational
period (27). Furthermore, in
women with PE, they indicated a decrease in serum free PlGF levels
in both the first and the second trimester prior to the onset of
PE, and they reported that higher serum sFlt-1 levels after 21
weeks of gestation, but not before 21 weeks, was probably
associated with an increased risk of developing PE (27).
Using the newly developed reference values, Ohkuchi
et al (42) observed that
women with EOPE and LOPE exhibited decreased serum levels of PlGF
and increased serum levels of sFlt-1 compared to normotensive
controls at 28 and 37 weeks, with more pronounced changes in EOPE
than in LOPE. In addition, they found that the sFlt-1/PlGF ratios
at ~28 weeks of gestation prior to the onset of severe PE were
increased in 83% of cases, suggesting its role as s putative marker
for the prediction of both early- and late-onset PE (42). Levine et al (37) concluded that the sFlt-1/PlGF ratio
in women with PE began to increase 2 to 3 months prior to the onset
of the disease and was more strongly predictive of PE than were
individual biomarkers.
In 2007, Stepan et al (43) demonstrated significantly higher
serum levels of sFlt1 and lower levels of PlGF in pregnancies with
adverse pregnancy outcomes compared with those with normal
outcomes, with more noticeable alterations in pregnancies with
subsequent PE compared with IUGR and in early-onset diseases
(delivery <34 weeks) compared with late-onset diseases.
Moreover, they concluded that the concurrent measurement of uterine
perfusion with Doppler sonography and angiogenic factors may be a
useful tool for the prediction of early-onset pregnancy
complications, particularly PE (43).
De Vivo et al (44), found that the serum sFlt-1/PlGF
ratio increased during gestation in both the PE and control group
in both trimesters; however, in the control group, the increase was
moderate (51%), while in the PE group, the increase was prominent
(285%) due to the significant decrease in serum PlGF levels in the
third trimester in this group. Romero et al (45) demonstrated that women who
delivered an IUGR neonate had changes in the plasma concentration
of pro- and anti-angiogenic factors from the first trimester of
pregnancy onwards, indicating that differences in their response to
intrauterine insults may determine whether a patient will deliver
an IUGR neonate, develop PE, or both (45).
All the aforementioned studies relied exclusively on
ELISA kits and their results could not be used in clinical
practice. The need for a rapid and reliable diagnostic test led to
the introduction of automated, commercially available systems for
the determination of sFlt-1 and PlGF levels. In 2010, Ohkuchi et
al (46) introduced automated
electrochemiluminescence immunoassay systems; they demonstrated in
only 18 min, that the sFlt-1/PlGF ratio had the optimal diagnostic
power for both EOPE and LOPE and that a cut-off value of 85 may
assist in the diagnosis of PE, particularly for EOPE (46). In addition, Verlohren et al
(47) evaluated the newly
developed automated Elecsys (Roche Diagnostics, GmbH) assay and
they confirmed the results of the aformentioned study,
demonstrating that the cut-off value of 85 for the sFlt-1/PIGF
ratio had a 82% sensitivity and 95% specificity for diagnosing PE.
Notably, for EOPE, the same cut-off value had a 89% sensitivity and
97% specificity, indicating the usefulness of this platform for the
establishment of a reliable test that could be used as a diagnostic
tool in obstetrics. In a subsequent study, Sunderji et al
(48), using a novel automated
immunoassay (Beckman Coulter), revealed that the sFlt-1/PlGF ratio
was the optimal biomarker for the separation of normotensive women
from those with pre-term PE. They also demonstrated the potential
of the markers to differentiate pregnant women with chronic
hypertension and PE from those with chronic hypertension only
(48).
Chaiworapongsa et al (49) demonstrated that the plasma
concentrations of angiogenic/anti-angiogenic factors are of
prognostic value in the obstetrical triage area in identifying
patients with severe PE requiring pre-term delivery within 2 weeks,
strengthening their clinical value in obstetrics for better
management of at-risk patients. Subsequent studies confirmed the
usefulness of the sFlt-1/PlGF ratio measurement in the triage. Rana
et al (50) indicated that
a plasma sFlt1/PlGF ratio >85 at presentation was predictive of
adverse outcomes occurring within 2 weeks and that in these women,
this marker had better results than other laboratory tests
currently used to predict such outcomes. In another study, Moore
et al (51) demonstrated
that an increased serum sFlt1/PlGF ratio was associated with an
increased risk of complications among women presenting <37 weeks
and that multivariable model combining the sFlt1:PlGF ratio with
clinical variables was more predictive of complications than a
model using clinical variables alone.
In a following multicenter study, Verlohren et
al (52) performed serum
sFlt-1 and PlGF measurements using the fully automated Elecsys
system and they reported significantly elevated sFlt-1/PlGF ratios
in patients with PE compared to the controls and to patients with
chronic and gestational hypertension at <34 weeks and ≥34 weeks,
thus allowing the discrimination between different types of
pregnancy-related hypertensive disorders. Moreover, it was shown
for the first time that patients with a sFlt-1/PlGF ratio in the
highest quartile (P<0.001) had a significantly reduced time to
delivery. It was noted that particularly in the <34 weeks PE
group, the early identification of high risk for delivery women was
strongly associated with maternal and fetal morbidity and mortality
as and the timely referral to an intensive care unit alone could
reduce perinatal morbidity and mortality by 20% (52). Herraiz et al (53) observed increased serum sFlt-1/PlGF
ratios in cases with fetal growth restriction, PE or HELLP, and PE
or HELLP and fetal growth restriction than control pregnancies both
<34 weeks and ≥34 weeks of gestation.
In 2014, Chaiworapongsa et al (54) demonstrated that the maternal
plasma concentrations of angiogenic/anti-angiogenic factors have
prognostic value for patients presenting to the obstetrical triage
area with suspected PE before 34 weeks of gestation and that these
biomarkers allow for the prospective categorization of patients
requiring pre-term delivery or who are at risk of adverse maternal
and/or neonatal outcomes. Rana et al (55) observed that women with a
non-angiogenic form of PE (sFlt-1/PlGF ratio <85) had very low
risk of adverse outcomes.
Gómez-Arriaga et al (56) demonstrated that the mean uterine
artery pulsatility index (UtA-PI) and sFlt-1/PlGF ratio in
combination with gestational age were useful for the prognostic
assessment of perinatal complications at the time of diagnosis of
EOPE, but not of maternal complications. Furthermore, they proposed
that a serum sFlt-1/PlGF ratio >655 was closely related to the
need to deliver within 48 h (56). Garcia-Tizon Larroca et al
(57) concluded that screening by
biophysical and biochemical testing at 30-33 weeks could identify
the majority of pregnancies developing PE and requiring delivery
within the subsequent 4 weeks.
In 2014, Verlohren et al (58) demonstrated that the use of
individual two cut-off values, one for EOPE and one for LOPE
allowed for the maximized accuracy of diagnosis. For EOPE, between
20+ 0 and 33+ 6 weeks of gestation, the
cut-off value at ≤33 was negative and at ≥85 was positive for
PE/HELLP syndrome with a sensitivity/specificity of 95/94% and
88/99.5%, respectively and for LOPE, ≥34 weeks, the cut-off values
at ≤33 and ≥110 resulted in a lower sensitivity/specificity of
89.6/73.1 and 58.2/95.5%, respectively. Schoofs et al
(59) indicated that repeated
measurements of the sFlt-1/PlGF ratio along with or in addition to
calculating the slope between two measurements appeared to be
superior in predicting PE to a single measurement of the
sFlt-1/PlGF ratio alone.
4. sFlt-1/PlGF ratio as second and third
trimester diagnostic biomarkers for the prediction of PE
Hypertension and proteinuria are currently the
classical clinical criteria used to diagnose PE, which however,
develop after 20 weeks of pregnancy and their positive predictive
value (PPV) for detecting severe adverse maternal and perinatal
outcomes was only 20% (60,61). Aspirin administration commenced in
early pregnancy before 16 weeks of pregnancy has been proven to
reduce the risk of developing PE by ~50% (62). Therefore, the development of an
effective screening test to identify women who are at a high risk
of developing PE early in pregnancy is of utmost importance; this
would prevent pre-term birth, facilitating both maternal and fetal
outcomes and decreasing healthcare costs associated with
hospitalization. Women who are at a high risk would benefit from
often and intensive surveillance, and drug administration for the
optimal birth time.
Extensive research has provided evidence that
angiogenic factors and their receptors may be used as biomarkers,
either alone or in combination with other markers, for predicting
PE (Table II). The sFlt-1/PlGF
ratio appears to be the optimal predictive tool and several
national societies, including the German Society of Obstetrics and
Gynecology, the American College of Obstetrics and Gynecology, the
National Institute for Care and Health Excellence, the Italian
Advisory Board, the Swiss Society for Gynaecology and Obstetrics,
have published a guidance regarding PlGF-based diagnostic testing
for suspected PE and how clinicians should implement this testing
in order to improve patient safety and to deliver benefits to the
healthcare system (63-65). The recommended cut-off values for
the Elecsys immunoassay sFlt-1/PLGF ratio in these guidelines are
of 33, 38, 85 and 110, with 38 and 85 being the mostly used
(63-65).
| Table IIsFlt-1/PlGF ratio as second and third
trimester diagnostic biomarkers for the prediction of PE. |
Table II
sFlt-1/PlGF ratio as second and third
trimester diagnostic biomarkers for the prediction of PE.
| Authors/year of
publication | Patient
population/sample size | Findings | (Refs.) |
|---|
| Hund et al,
2014; Zeisler et al, 2016 | PROGNOSIS study
with 1,050 pregnant women (24 weeks 0 days to 36 weeks 6 days of
gestation) | Among women at
<37 weeks, an sFLT-1:PIGF ratio ≤38 can accurately rule out the
risk of developing PE in the subsequent week, with a NPV of 99.3%
(95% CI, 97.0-99.9), with 80% sensitivity and 78.3% specificity An
sFLT-1:PIGF ratio >38 can accurately predict PE/HELLP within 4
weeks, with a PPV of 36.7, with 66.2% sensitivity and 83.1%
specificity | (66,67) |
| Hund et al,
2015; Klein et al, 2016 | 192 women with a
gestational age of ≥24 weeks with suspicion of PE | The use of
sFlt-1/PlGF ratio influenced clinical decision making towards
appropriate hospitalization in a considerable proportion of women
with suspected PE | (68,69) |
| Perales et
al, 2017 | 729 women at risk
for PE at <34weeks | The sFlt-1/PlGF
ratio was significantly increased in women with EOPE compared to
LOPE and controls | (70) |
| Herraiz et
al, 2018 | 5,601 consecutive
singleton pregnancies (4.3% women were selected for intensive
monitoring by combining maternal history and second trimester
uterine artery Doppler data) | The sFlt1/PlGF
ratio measurement is useful in previously selected women to predict
mostly early PE/IUGR, with optimal diagnostic accuracy for values
>95th centile as the cut-off | (71) |
| Sabriá et
al, 2018 | 495 women (24+
0 to 36+ 6 weeks of gestation with clinically
suspected PE and evaluated the effectiveness of NT-proBNP | The addition of
NT-proBNP assessment yields superior results for the prediction of
delivery with PE in the subsequent week compared with the use of
sFlt-1/PlGF ratio alone | (72) |
| Lafuente-Ganuza
et al, 2020 | 309 women in the
development phase and 276 in the validation phase between 24 to
33=6 weeks of gestation with suspected PE | Two sFlt-1/PlGF
ratio cut-off values of 23 and 45 can rule out and rule in EOPE at
any time between 24 and 33+6 weeks of gestation | (73) |
| Sovio et al,
2015 | 4,099 nulliparous
women at 20, 28, and 36 weeks of gestation | An sFlt-1:PlGF
ratio >38 at 28 weeks had a 32% PPV for PE and preterm birth,
with a similar PPV in both high- and low-risk women and at 36
weeks, it had 20% PPV for severe PE in high-risk women and 6.4% in
low-risk women At 36 weeks, an sFlt-1/PlGF ratio >110 had a PPV
of 30% for severe preeclampsia, and for low- and high-risk women
Among low-risk women at 36 weeks, an sFlt-1/ PlGF ratio ≤38 had a
NPV value for severe PE of 99.2% | (74) |
| Zeisler et
al, 2019 | Exploratory
post-hoc analysis of data from the PROGNOSIS study | A sFlt-1/PlGF ratio
≤38 can rule out the onset of PE for up to 4 weeks in women with
suspected PE with a NPV of 94.3% (95% CI, 91.7-96.3%) and that
repeat testing of the sFlt-1/PlGF ratio in these women could
further elucidate the risk of developing PE | (75) |
| Bian et al,
2019 | PROGNOSIS Asia
study with 764 pregnant Asian women [20+ 0 (18+
0 days in Japan) to 36+ 6 weeks of gestation] | The NPV for ruling
out preeclampsia within 1 week using an sFlt-1/PlGF ratio of ≤38
was 98.6% (95% CI, 97.2-99.4%), with 76.5% sensitivity and 82.1%
specificity and the PPV ofa sFlt-1/ PlGF ratio >38 for ruling in
preeclampsia within 4 weeks was 30.3% (95% CI,23.0-38.5%), with
62.0% sensitivity and 83.9% specificity | (76) |
| Cerdeira et
al, 2019 | 370 women between
24+0 and 37+0 weeks of gestation with
suspected PE | A sensitivity of
100% and a NPV of 100% compared with a sensitivity of 83.3% and NPV
of 97.8% with clinical practice alone | (77) |
| Cerdeira et
al, 2022 | Post hoc analysis
of the INSPIRE trial | The
sFlt-1/PlGF-ratio at the cut-off of 85 predicts preeclampsia within
4 weeks with a PPV of 71.4% | (78) |
| Perry et al,
2020 | 302 pregnant women
with hypertension >20 weeks of gestation | sFlt-1/PIGF ratio
could predict a PE-related delivery within 1 and 2 weeks,
particularly in gestational ages <35 weeks | (79) |
| Dröge et al,
2021 | 1,117 women
(>20+0 weeks of gestation) with symptoms of PE | The addition of
sFlt-1/PlGF ratio to a multi-marker model including maternal
characteristics and routine clinical examination improves the
predictive validity | (64) |
| Peguero et
al, 2021 | 86 women with
confirmed EOPE (<34 weeks) | Longitudinal
changes in maternal angiogenic factors levels improve the
prediction capacity for EO-PE of adverse outcome and time interval
to delivery | (80) |
| Dathan-Stumpf et
al, 2022 | 283 singleton
pregnancies with suspected PE | Positive
associatino between the sFlt-1/PlGF ratio and severity of placental
dysfunction and a negative association with time to delivery | (81) |
| Hughes et
al, 2023 | 222 women
(20+0 and 36+6 weeks gestation) from New
Zealand | In participants
< 37 weeks, an sFlt-1/PlGF ratio ≤38 ruled out PE in the
subsequent week with a NPV of 96.2% (95% CI, 92.3-98.2) and ruled
in PE within 4 weeks with a PPV of 75% (95% CI, 65.0-82.9) | (65) |
| Kifle et al,
2022 | Pregnant women
between 24+0 to 37+0 weeks of gestation with
PE clinical suspicion | Models using
continuous values of sFlt-1 only or sFlt1/PIGF ratio had better
predictive performance compared to a PIGF only or the model with
sFlt-1/PIGF ratio as a cut-off at 38 | (82) |
The PRediction of short-term Outcome in preGNant
wOmen with Suspected preeclampsIa Study (PROGNOSIS) was the first
clinical study designed to demonstrate the utility of the
sFlt-1/PlGF ratio in the short-term (up to 4 weeks) prediction of
PE using Elecsys immunoassays for sFlt-1 and PlGF (66). PROGNOSIS was conducted between
2010-2013 in 14 countries and demonstated that among pregnant women
at <37 weeks of gestation, an sFLT-1:PIGF ratio ≤38 can
accurately rule out the likelihood of developing PE in the
subsequent week, with a negative predictive value (NPV) of 99.3%,
with 80% sensitivity and 78.3% specificity. It was also
demonstrated that an sFLT-1:PIGF ratio >38 can accurately
predict PE/HELLP within 4 weeks, with a PPV of 36.7%, with 66.2%
sensitivity and 83.1% specificity (66,67).
The Preeclampsia Open Study (PreOS) was the first
prospective, multicenter study in pregnant women with suspected PE
aiming to evaluate the clinical utility of the fully automated
Elecsys sFlt-1/PlGF test in the diagnosis of PE and how it
influences their clinical management (68). Its results demonstrated that the
use of sFlt-1/PlGF ratio influenced clinical decision-making
towards appropriate hospitalization in a considerable proportion of
women with suspected PE (69).
Perales et al (70) performed the Study of Early
Pre-eclampsia in Spain (STEPS) study in order to evaluate the
sFlt-1/PlGF ratio at 20, 24 and 28 weeks as a predictive marker for
EOPE (<34 weeks). They found that the sFlt-1/PlGF ratio was
significantly increased in women with EOPE compared to those with
LOPE and the controls, and they developed a prediction model for
EOPE combining sFlt-1/PlGF ratio with considerably increased
specificity and sensitivity compared with using UtA-PI or
sFlt-1/PlGF ratio alone (70).
Herraiz et al (71) designed a study to analyze the
usefulness of the sFlt-1/PlGF ratio measurement at 24-28 weeks for
the prediction of early (requiring delivery <32 weeks),
intermediate (delivery at 32 to <36 weeks) and late (delivery
≥36 weeks) PE/IUGR. Their results demonstrated the sFlt1/PlGF ratio
measurement was useful in previously selected women to predict
mostly early PE/IUGR, with optimal diagnostic accuracy for values
>95th centile as the cut-off (71).
Sabriá et al (72) evaluated the effectiveness of
N-terminal pro-B natriuretic peptide (NT-proBNP), which is released
from cardiac myocytes in response to myocardial stretch or ischemia
and is increased in women with PE, uric acid and the sFlt-1/PlGF
ratio >38 for the prediction of delivery within 1 week. They
observed that the addition of NT-proBNP assessment yields superior
results for the prediction of delivery with PE in the subsequent
week compared with the use of the sFlt-1/PlGF ratio alone (72). Lafuente-Ganuza et al
(73) conducted a study for
identifying and validating cut-off values for the sFlt-1/PlGF ratio
and NT-proBNP predictive model of EOPE and they demonstrated that
two sFlt-1/PlGF ratio cut-off values of 23 and 45 can rule out and
rule in EOPE at any time between 24 and 33+6 weeks of
gestation.
In the Pregnancy Outcome Prediction (POP) study,
Sovio et al (74)
demonstrated that an sFlt-1:PlGF ratio >38 at 28 weeks had a 32%
PPV for PE and pre-term birth, with a similar PPV in both high- and
low-risk women and at 36 weeks, it had 20% PPV for severe PE in
high-risk women and 6.4% in low-risk women. At 36 weeks, an
sFlt-1/PlGF ratio >110 had a PPV of 30% for severe PE, and the
PPV was similar comparing low- and high-risk women (74). Among low-risk women at 36 weeks,
an sFlt-1/PlGF ratio ≤38 had a NPV value for severe PE of 99.2%,
indicating that the sFlt-1/PlGF ratio provides clinically useful
prediction of the risk of the most important manifestations of
preeclampsia in a cohort of unselected nulliparous women (74).
An exploratory post hoc analysis of data from the
PROGNOSIS study by Zeisler et al (75) demonstrated that a sFlt-1/PlGF
ratio ≤38 can rule out the onset of PE for up to 4 weeks in women
with suspected PE (24+0 to 36+6 weeks'
gestation) with a NPV of 94.3% and that repeat testing of the
sFlt-1/PlGF ratio in these women could further elucidate the risk
of developing PE.
PROGNOSIS Asia was a prospective, multicenter study
conducted at 25 sites in Asia designed to investigate the value of
the sFlt-/PlGF ratio for predicting adverse outcomes (76). The NPV for ruling out preeclampsia
within 1 week using an sFlt-1/PlGF ratio of ≤38 was 98.6%, with
76.5% sensitivity and 82.1% specificity and the PPV of a >38
sFlt-1/PlGF ratio for ruling in preeclampsia within 4 weeks was
30.3% with 62.0% sensitivity and 83.9% specificity (76).
Cerdeira et al (77) performed the Interventional Study
Evaluating the Short-Term Prediction of Preeclampsia/Eclampsia In
Pregnant Women With Suspected Preeclampsia (INSPIRE) study, the
first randomized clinical trial for assessing the use of angiogenic
biomarkers sFlt-1/PlGF using a ratio cut-off of 38. They yielded a
sensitivity of 100% and a NPV of 100% compared with a sensitivity
of 83.3% and NPV of 97.8% with clinical practice alone, indicating
that the sFlt-1/PlGF ratio in combination with standard clinical
practice both identifies and leads to correct admission of women
with increased risks of preeclampsia without changing the admission
rate (77). Cerdeira et al
(78) performed a post hoc
analysis of the INSPIRE trial and their finding that the
sFlt-1/PlGF-ratio at the cut-off of 85 predicts PE within 4 weeks
with a PPV of 71.4% confirmed the predictive utility of this cutoff
and suggested that combining this cut-off of 85 with the rule out
cut-off of 38 could improve the management of patients with
suspected PE.
Perry et al (79) demonstrated that the combination of
the sFlt-1/PIGF ratio and maternal characteristics could predict a
PE-related delivery within 1 and 2 weeks, particularly in
gestational ages <35 weeks, and they emphasized the superior
performance of a continuous scale of sFlt-1/PlGF ratio in the
model.
Dröge et al (64) performed the first retrospective
real-world study in order to evaluate the clinical use of serum
sFlt-1/PlGF ratio cut-off values of 38 and 85 alone or integrating
into a multi-marker model for the prediction of adverse maternal of
fetal outcomes. They observed that the addition of sFlt-1/PlGF
ratio to a multi-marker model including maternal characteristics
and routine clinical examination improved the predictive validity
(64).
Peguero et al (80) measured the levels of PlGF, sFlt-1
and the sFlt-1/PlGF ratio from admission and before delivery at
fixed time points, and demonstrated that longitudinal changes in
maternal angiogenic factors levels improved the predictive capacity
for EOPE with adverse outcomes and time interval to delivery.
Dathan-Stumpf et al (81) in a real-world study with
sFlt-1/PlGF ratio measurements at admission and follow-up
measurements before delivery and confirming previous studies they
observed a positive correlation between the sFlt-1/PlGF ratio and
severity of placental dysfunction and a negative association with
time to delivery.
Hughes et al (65) evaluated the sFlt-1/PlGF value for
predicting PE and they demonstrated that in participants at <37
weeks of gestation, an sFlt-1/PlGF ratio ≤38 ruled out PE in the
subsequent week with a NPV of 96.2% and ruled in PE within 4 weeks
with a PPV of 75%; these results were comparable to those reported
in international trials, indicating the predictive value of the
sFlt-1/PlGF ratio in PE and emphasizing its incorporation into
national guidelines.
Kifle et al (82) designed a secondary analysis of
INSPIRE trial in order to compare the prognostic utility of models
using the continuous values of sFlt-1, PIGF, sFlt-1/PIGF ratio or
sFlt-1/PIGF ratio as a cut-off at 38 for predicting PE within 7
days of screening among women with suspected PE. They observed that
models using continuous values of sFlt-1 only or sFlt-1/PIGF ratio
had a better predictive performance compared to a PIGF only or the
model with sFlt-1/PIGF ratio as a cut-off at 38 (82).
5. sFlt-1/PlGF ratio in first trimester
prediction models for PE
Considerable efforts have been made to develop first
trimester prediction models for PE, which need to be evaluated and
undergo external validation in an independent population with
different demographics and geographic settings than those of the
original models (Table III)
(83). Thus far, the Fetal
Medicine Foundation (FMF) first trimester prediction model (namely
the triple test), which combines maternal factors, biophysical
parameters (MAP and UtA-PI) and serum pregnancy-associated plasma
protein A (PAPP-A) has undergone successful internal and external
validation (83). The FMF triple
test has detection rates of 90 and 75% for the prediction of early
and pre-term PE, respectively, with a 10% false-positive rate (FPR)
(83).
| Table IIIsFlt-1/PlGF ratio in first trimester
prediction models for PE. |
Table III
sFlt-1/PlGF ratio in first trimester
prediction models for PE.
| Authors, year of
publication | Patient
population/sample size | Findings | (Refs.) |
|---|
| Crovetto et
al, 2014 | 5,759 women (28
cases of early PE, 84 cases of late PE, 84 controls) | For early PE, the
prediction model observed 77.8 and 88.9% detection rates for 5 and
10% FPR, respectively, and for late PE, the detection rates were
51.2 and 69% at 5 and 10% FPR, respectively (AUC, 0.888; 95% CI,
0.840-0.936) | (84) |
| Crovetto et
al, 2015 | 9,462 pregnant
women undergoing routine pregnancy care | For early PE, the
prediction model observed 87.7 and 91.2% detection rates for 5% and
10% FPR, respectively and for late PE, the detection rates were
68.3 and 76.4% at 5 and 10% of FPR, respectively | (85) |
| Lamain-de Ruite
et al, 2019 | External validation
of the above studies in a Dutch study including 3,736 women with 87
(2.3%) affected by preeclampsia | Showed suboptimal
calibration and discrimination for PE | (86) |
| Tsiakkas et
al, 2016 | 7,066 cases of PE
at 11-13 weeks, 8,079 cases at 19-24 weeks, 8,472 at 30-34 weeks
and 4,043 at 35-37 weeks | Confirmed the
superior performance for the detection of early, compared to late,
PE and improvement with advancing gestational age at screening. The
integration of sFlt-1 measurement at 11-13 weeks did not improve
the prediction of PE achieved by maternal factors alone | (87) |
| Diguisto et
al, 2017 | 226 women with a
high risk of PE | The optimal
prediction model was the combination of UAD and serum PlGF, while
the combination of UAD and sFlt-1 did not significantly improve the
prediction of preeclampsia or other outcomes compared with serum
PlGF alone | (88) |
Crovetto et al (84) explored the independent and
combined integration of VEGF, PlGF, sFlt-1 along with maternal
characteristics, biophysical parameters and biochemical
measurements in first trimester predictive models of early and late
PE. For early PE, the model achieved 77.8 and 88.9% detection rates
for 5 and 10% FPR, respectively, and for late PE, the detection
rates were 51.2 and 69% at 5 and 10% FPR, respectively (area under
the curve, 0.888; 95% CI, 0.840-0.936) (84).
In 2015, the same scientific group (85) performed a study aiming to confirm,
in a substantially larger sample size, their previous results and
to develop the optimal first trimester screening model for PE based
on the combination of maternal characteristics, biophysical
parameters and biochemical markers, including PAPP-A, PlGF and
sFlt1 in a low-risk population. The optimal model for early PE
achieved 87.7 and 91.2% detection rates for 5 and 10% FPR,
respectively and for late PE, the detection rates were 68.3 and
76.4% at 5 and 10% of FPR, respectively, indicating that the
inclusion of angiogenic factors in existing predicting models for
PE can substantially improve their detection rate with high
accuracy in general low-risk obstetric populations (85). However, the aforementioned models
had undergone external validation in a Dutch study including 3,736
women with 87 (2.3%) affected by PE and suboptimal calibration and
discrimination for PE was observed (86).
Tsiakkas et al (87) examined the combined screening with
maternal factors, medical history and serum sFlt-1 and their
results confirmed the superior performance for the detection of
early, compared to late, PE and improvement with advancing
gestational age at screening. Moreover, they demonstrated that the
integration of sFlt-1 measurement at 110-13 weeks did not improve
the prediction of PE achieved by maternal factors alone (87).
Diguisto et al (88) examined whether first-trimester
Uterine artery Doppler (UAD) combined with angiogenic markers could
help to predict PE and other adverse outcomes. They found that the
optimal prediction model was the combination of UAD and serum PlGF,
while the combination of UAD and sFlt-1 did not significantly
improve the prediction of PE or other outcomes compared with serum
PlGF alone, confirming the poor performance of sFlt-1 in
first-trimester screening of PE (88).
Recently, Verlohren et al (89) published an article following a
meeting of international experts with the aim of providing
clinicians guidance for the use of sFlt-1/PlGF ratio in the
management of women with PE and improving clinical care, as well as
suggestions for further research on their clinical utility in
various circumstances.
6. Conclusions and future perspectives
The present review summarized the role of the
sFlt-1/PlGF ratio in the prediction and diagnosis of PE. The
sFlt-1/PlGF ratio represents an additional and advanced diagnostic
tool for PE, independent of blood pressure or laboratory markers of
HELLP syndrome, to identify patients who develop PE or develop
severe PE requiring pre-term birth. Estimated maternal/fetal
complications are highly desirable and are urgently required.
Furthermore, the economic impact of the routine clinical use of the
sFlt-1/PlGF ratio has been demonstrated in a number of studies, as
the sFlt-1/PlGF ratio is easy to be measured and its use results in
shorter hospital stays (90). The
use of highly specific tests, such as sFlt1 and PlGF, risk
stratification and the management of patients with suspected PE
will reduce unnecessary investigations, introductions and even
pre-term births and at the same time, will provide better focus on
patients who are at an increased risk of adverse outcomes. In
addition, there is a double benefit: Tailor resources to women at
highest risk, while minimizing overestimation and intervention for
women at lower risk. It is therefore a useful tool for individual
risk stratification and further studies/larger trials are warranted
in order to improve its clinical applicability and to provide
guidance for its global use in order to obtain a better homogeneous
clinical management of women with PE.
Availability of data and materials
Not applicable.
Authors' contributions
All the authors (AV, PF, EK, SS) contributed to the
conception and design of the study. PF and EK searched the
literature for inclusion in the study that was then examined and
reviewed by AV and SS. PF and EK drafted and wrote the manuscript.
AV and SS provided advice and critically revised the manuscript.
All authors have read and approved the final version of the
manuscript. Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Abbreviations:
|
PE
|
preeclampsia
|
|
IUGR
|
intrauterine growth retardation
|
|
EOPE
|
early-onset PE
|
|
LOPE
|
late-onset preeclampsia
|
|
HELLP
|
hemolysis, elevated liver enzymes,
and low platelets
|
|
STB
|
secondary syncytiotrophoblast
|
|
HIF-1α
|
hypoxia-inducible factor 1α
|
|
ET-1
|
endothelin-1
|
|
STBM
|
syncytiotrophoblast
microparticles
|
|
AT1-AA
|
angiotensin II 1 receptor
autoantibodies
|
|
NO
|
nitric oxide
|
|
OS
|
oxidative stress
|
|
ER
|
endoplasmic reticulum
|
|
VEGF
|
vascular endothelial growth
factor
|
|
PlGF
|
placental growth factor
|
|
sFlt-1
|
soluble fms-like tyrosine kinase
1
|
|
sEng
|
soluble endoglin
|
|
VEGFRs
|
vascular endothelial growth factor
(angiogenic) receptors
|
|
KDR
|
kinase domain region
|
|
EGFR
|
epidermal growth factor receptor
|
|
CPEP
|
calcium for preeclampsia
prevention
|
|
uFP ratio
|
urinary sFlt-1-to-PlGF ratio
|
|
CI
|
confidence interval
|
|
ROC
|
receiver operating characteristics
curve
|
|
PPV
|
positive predictive value
|
|
NPV
|
negative predictive value
|
|
UtA-PI
|
mean uterine artery pulsatility
index, MAP, mean arterial pressure
|
|
PROGNOSIS
|
PRediction of short-term Outcome in
preGNant wOmen with Suspected preeclampsIa Study
|
|
PreOS
|
Preeclampsia Open Study
|
|
STEPS
|
study of early preeclampsia in
Spain
|
|
NT-proBNP
|
N-terminal pro-B natriuretic
peptide
|
|
POP
|
pregnancy outcome prediction,
INSPIRE, interventional study evaluating the short-term prediction
of preeclampsia/eclampsia in pregnant women with suspected
preeclampsia
|
|
FPR
|
false-positive rate
|
|
FMF
|
Fetal Medicine Foundation
|
|
PAPP-A
|
serum pregnancy-associated plasma
protein A
|
|
UAD
|
uterine artery Doppler
|
Acknowledgments
Not applicable.
Funding
No funding was received.
References
|
1
|
Troiano NH: Physiologic and hemodynamic
changes during pregnancy. AACN Adv Crit Care. 29:273–283. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sierra-Laguado J, Garcia RG and
López-Jaramillo P: Flow-mediated dilatation of the brachial artery
in pregnancy. Int J Gynaecol Obstet. 93:60–61. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cid M and González M: Potential benefits
of physical activity during pregnancy for the reduction of
gestational diabetes prevalence and oxidative stress. Early Hum
Dev. 94:57–62. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sibai BM and Frangieh A: Maternal
adaptation to pregnancy. Curr Opin Obstet Gynecol. 7:420–426. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ahmed A and Perkins J: Angiogenesis and
intrauterine growth restriction. Baillieres Best Pract Res Clin
Obstet Gynaecol. 14:981–998. 2000. View Article : Google Scholar
|
|
6
|
Vrachnis N, Kalampokas E, Sifakis S,
Vitoratos N, Kalampokas T, Botsis D and Iliodromiti Z: Placental
growth factor (PlGF): A key to optimizing fetal growth. J Matern
Fetal Neonatal Med. 26:995–1002. 2013. View Article : Google Scholar
|
|
7
|
Sibai B, Dekker G and Kupferminc M:
Pre-eclampsia. Lancet. 365:785–799. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
No authors listed. Gestational
hypertension and preeclampsia: ACOG practice bulletin, number 222.
Obstet Gynecol. 135:e237–e260. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Brown MA, Magee LA, Kenny LC, Karumanchi
SA, McCarthy FP, Saito S, Hall DR, Warren CE, Adoyi G and Ishaku S;
International Society for the Study of Hypertension in Pregnancy
(ISSHP): The hypertensive disorders of pregnancy: ISSHP
classification, diagnosis and management recommendations for
international practice. Hypertension. 72:24–43. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xiong X, Demianczuk NN, Saunders LD, Wang
FL and Fraser WD: Impact of preeclampsia and gestational
hypertension on birth weight by gestational age. Am J Epidemiol.
155:203–209. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Staff AC: The two-stage placental model of
preeclampsia: An update. J Reprod Immunol. 134-135:1–10. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Redman CW: Current topic: pre-eclampsia
and the placenta. Placenta. 12:301–308. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pankiewicz K, Szczerba E, Fijalkowska A,
Szamotulska K, Szewczyk G, Issat T and Maciejewski TM: The
association between serum galectin-3 level and its placental
production in patients with preeclampsia. J Physiol Pharmacol.
71:845–856. 2020.
|
|
14
|
Redman CWG and Staff AC: Preeclampsia,
biomarkers, syncytiotrophoblast stress, and placental capacity. Am
J Obstet Gynecol. 213(Suppl 4): S9.e1–S9.e4. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Maynard SE, Venkatesha S, Thadhani R and
Karumanchi SA: Soluble Fms-like tyrosine kinase 1 and endothelial
dysfunction in the pathogenesis of preeclampsia. Pediatr Res.
57:1R–7R. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Koga K, Osuga Y, Yoshino O, Hirota Y,
Ruimeng X, Hirata T, Takeda S, Yano T, Tsutsumi O and Taketani Y:
Elevated serum soluble vascular endothelial growth factor receptor
1 (sVEGFR-1) levels in women with preeclampsia. J Clin Endocrinol
Metab. 88:2348–2351. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tsatsaris V, Goffin F and Foidart JM:
Circulating angiogenic factors and preeclampsia. N Engl J Med.
350:2003–2004. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Levine RJ, Maynard SE, Qian C, Lim KH,
England LJ, Yu KF, Schisterman EF, Thadhani R, Sachs BP, Epstein
FH, et al: Circulating angiogenic factors and the risk of
preeclampsia. N Engl J Med. 350:672–683. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Maynard SE and Karumanchi SA: Angiogenic
factors and preeclampsia. Semin Nephrol. 31:33–46. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pratt A, Da Silva Costa F, Borg AJ,
Kalionis B, Keogh R and Murthi P: Placenta-derived angiogenic
proteins and their contribution to the pathogenesis of
preeclampsia. Angiogenesis. 18:115–123. 2015. View Article : Google Scholar
|
|
21
|
Helmo FR, Lopes AMM, Carneiro ACDM, Campos
CG, Silva PB, Dos Reis Monteiro MLG, Rocha LP, Dos Reis MA,
Etchebehere RM, Machado JR and Corrêa RRM: Angiogenic and
antiangiogenic factors in preeclampsia. Pathol Res Pract. 214:7–14.
2018. View Article : Google Scholar
|
|
22
|
Ferrara N and Kerbel RS: Angiogenesis as a
therapeutic target. Nature. 438:967–974. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kendall RL and Kenneth AT: Inhibition of
vascular endothelial cell growth factor activity by an endogenously
encoded soluble receptor. Proc Natl Acad Sci USA. 90:10705–10709.
1993. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Clark DE, Smith SK, He Y, Day KA, Licence
DR, Corps AN, Lammoglia R and Charnock-Jones DS: A vascular
endothelial growth factor antagonist is produced by the human
placenta and released into the maternal circulation. Biol Reprod.
59:1540–1548. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Taylor RN, Grimwood J, Taylor RS, McMaster
MT, Fisher SJ and North RA: Longitudinal serum concentrations of
placental growth factor: Evidence for abnormal placental
angiogenesis in pathologic pregnancies. Am J Obstet Gynecol.
188:177–182. 2003. View Article : Google Scholar
|
|
26
|
Ferrara N, Gerber HP and LeCouter J: The
biology of VEGF and its receptors. Nat Med. 9:669–676. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hirashima C, Ohkuchi A, Arai F, Takahashi
K, Suzuki H, Watanabe T, Kario K, Matsubara S and Suzuki M:
Establishing reference values for both total soluble Fms-like
tyrosine kinase 1 and free placental growth factor in pregnant
women. Hypertens Res. 28:727–732. 2005. View Article : Google Scholar
|
|
28
|
Azimi-Nezhad M: Vascular endothelial
growth factor from embryonic status to cardiovascular pathology.
Rep Biochem Mol Biol. 2:59–69. 2014.PubMed/NCBI
|
|
29
|
Vincenti V, Cassano C, Rocchi M and
Persico G: Assignment of the vascular endothelial growth factor
gene to human chromosome 6p21.3. Circulation. 93:1493–1495. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Maglione D, Guerriero V, Viglietto G,
Delli-Bovi P and Persico MG: Isolation of a human placenta cDNA
coding for a protein related to the vascular permeability factor.
Proc Natl Acad Sci USA. 88:9267–9271. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
De Falco S: The discovery of placenta
growth factor and its biological activity. Exp Mol Med. 44:1–9.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Park JE, Chen HH, Winer J, Houck KA and
Ferrara N: Placenta growth factor. Potentiation of vascular
endothelial growth factor bioactivity, in vitro and in vivo, and
high affinity binding to Flt-1 but not to Flk-1/KDR. J Biol Chem.
269:25646–25654. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lee ES, Oh MJ, Jung JW, Lim JE, Seol HJ,
Lee KJ and Kim HJ: The levels of circulating vascular endothelial
growth factor and soluble Flt-1 in pregnancies complicated by
preeclampsia. J Korean Med Sci. 22:94–98. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Roberts JM and Rajakumar A: Preeclampsia
and soluble fms-like tyrosine kinase 1. J Clin Endocrinol Metab.
94:2252–2254. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Palmer KR, Kaitu'u-Lino TJ, Hastie R,
Hannan NJ, Ye L, Binder N, Cannon P, Tuohey L, Johns TG, Shub A and
Tong S: Placental-specific sFLT-1 e15a protein is increased in
preeclampsia, antagonizes vascular endothelial growth factor
signaling, and has antiangiogenic activity. Hypertension.
66:1251–1259. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hastie R, Brownfoot FC, Pritchard N,
Hannan NJ, Cannon P, Nguyen V, Palmer K, Beard S, Tong S and
Kaitu'u-Lino TJ: EGFR (epidermal growth factor receptor) signaling
and the mitochondria regulate sFlt-1 (soluble FMS-Like tyrosine
kinase-1) secretion. Hypertension. 73:659–670. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Levine RJ, Lam C, Qian C, Yu KF, Maynard
SE, Sachs BP, Sibai BM, Epstein FH, Romero R, Thadhani R, et al:
Soluble endoglin and other circulating antiangiogenic factors in
preeclampsia. N Engl J Med. 355:992–1005. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Maynard SE, Min JY, Merchan J, Lim KH, Li
J, Mondal S, Libermann TA, Morgan JP, Sellke FW, Stillman IE, et
al: Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may
contribute to endothelial dysfunction, hypertension, and
proteinuria in preeclampsia. J Clin Invest. 111:649–658. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Thadhani R, Mutter WP, Wolf M, Levine RJ,
Taylor RN, Sukhatme VP, Ecker J and Karumanchi SA: First trimester
placental growth factor and soluble fms-like tyrosine kinase 1 and
risk for preeclampsia. J Clin Endocrinol Metab. 89:770–775. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chaiworapongsa T, Romero R, Kim YM, Kim
GJ, Kim MR, Espinoza J, Bujold E, Gonçalves L, Gomez R, Edwin S and
Mazor M: Plasma soluble vascular endothelial growth factor
receptor-1 concentration is elevated prior to the clinical
diagnosis of pre-eclampsia. J Matern Fetal Neonatal Med. 17:3–18.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Buhimschi CS, Norwitz ER, Funai E, Richman
S, Guller S, Lockwood CJ and Buhimschi IA: Urinary angiogenic
factors cluster hypertensive disorders and identify women with
severe preeclampsia. Am J Obstet Gynecol. 192:734–741. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ohkuchi A, Hirashima C, Matsubara S,
Suzuki H, Takahashi K, Arai F, Watanabe T, Kario K and Suzuki M:
Alterations in placental growth factor levels before and after the
onset of preeclampsia are more pronounced in women with early onset
severe preeclampsia. Hypertens Res. 30:151–159. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Stepan H, Unversucht A, Wessel N and Faber
R: Predictive value of maternal angiogenic factors in second
trimester pregnancies with abnormal uterine perfusion.
Hypertension. 49:818–824. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
De Vivo A, Baviera G, Giordano D,
Todarello G, Corrado F and D'anna R: Endoglin, PlGF and sFlt-1 as
markers for predicting pre-eclampsia. Acta Obstet Gynecol Scand.
87:837–842. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Romero R, Nien JK, Espinoza J, Todem D, Fu
W, Chung H, Kusanovic JP, Gotsch F, Erez O, Mazaki-Tovi S, et al: A
longitudinal study of angiogenic (placental growth factor) and
anti-angiogenic (soluble endoglin and soluble vascular endothelial
growth factor receptor-1) factors in normal pregnancy and patients
destined to develop preeclampsia and deliver a small for
gestational age neonate. J Matern Fetal Neonatal Med. 21:9–23.
2008. View Article : Google Scholar :
|
|
46
|
Ohkuchi A, Hirashima C, Suzuki H,
Takahashi K, Yoshida M, Matsubara S and Suzuki M: Evaluation of a
new and automated electrochemiluminescence immunoassay for plasma
sFlt-1 and PlGF levels in women with preeclampsia. Hypertens Res.
33:422–427. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Verlohren S, Galindo A, Schlembach D,
Zeisler H, Herraiz I, Moertl MG, Pape J, Dudenhausen JW, Denk B and
Stepan H: An automated method for the determination of the
sFlt-1/PIGF ratio in the assessment of preeclampsia. Am J Obstet
Gynecol. 202:161.e1–161.e11. 2010. View Article : Google Scholar
|
|
48
|
Sunderji S, Gaziano E, Wothe D, Rogers LC,
Sibai B, Karumanchi SA and Hodges-Savola C: Automated assays for
sVEGF R1 and PlGF as an aid in the diagnosis of preterm
preeclampsia: A prospective clinical study. Am J Obstet Gynecol.
202:40.e1–e77. 2010. View Article : Google Scholar
|
|
49
|
Chaiworapongsa T, Romero R, Savasan ZA,
Kusanovic JP, Ogge G, Soto E, Dong Z, Tarca A, Gaurav B and Hassan
SS: Maternal plasma concentrations of angiogenic/anti-angiogenic
factors are of prognostic value in patients presenting to the
obstetrical triage area with the suspicion of preeclampsia. J
Matern Fetal Neonatal Med. 24:1187–1207. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Rana S, Powe CE, Salahuddin S, Verlohren
S, Perschel FH, Levine RJ, Lim KH, Wenger JB, Thadhani R and
Karumanchi SA: Angiogenic factors and the risk of adverse outcomes
in women with suspected preeclampsia. Circulation. 125:911–919.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Moore AG, Young H, Keller JM, Ojo LR, Yan
J, Simas TA and Maynard SE: Angiogenic biomarkers for prediction of
maternal and neonatal complications in suspected preeclampsia. J
Matern Fetal Neonatal Med. 25:2651–2657. 2012. View Article : Google Scholar
|
|
52
|
Verlohren S, Herraiz I, Lapaire O,
Schlembach D, Moertl M, Zeisler H, Calda P, Holzgreve W, Galindo A,
Engels T, et al: The sFlt-1/PlGF ratio in different types of
hypertensive pregnancy disorders and its prognostic potential in
preeclamptic patients. Am J Obstet Gynecol. 206:58.e1–e8. 2012.
View Article : Google Scholar
|
|
53
|
Herraiz I, Dröge LA, Gómez-Montes E,
Henrich W, Galindo A and Verlohren S: Characterization of the
soluble fms-like tyrosine kinase-1 to placental growth factor ratio
in pregnancies complicated by fetal growth restriction. Obstet
Gynecol. 124:265–273. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Chaiworapongsa T, Romero R, Korzeniewski
SJ, Cortez JM, Pappas A, Tarca AL, Chaemsaithong P, Dong Z, Yeo L
and Hassan SS: Plasma concentrations of angiogenic/anti-angiogenic
factors have prognostic value in women presenting with suspected
preeclampsia to the obstetrical triage area: a prospective study. J
Matern Fetal Neonatal Med. 27:132–144. 2014. View Article : Google Scholar :
|
|
55
|
Rana S, Schnettler WT, Powe C, Wenger J,
Salahuddin S, Cerdeira AS, Verlohren S, Perschel FH, Arany Z, Lim
KH, et al: Clinical characterization and outcomes of preeclampsia
with normal angiogenic profile. Hypertens Pregnancy. 32:189–201.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Gómez-Arriaga PI, Herraiz I, López-Jiménez
EA, Escribano D, Denk B and Galindo A: Uterine artery Doppler and
sFlt-1/PlGF ratio: Prognostic value in early-onset pre-eclampsia.
Ultrasound Obstet Gynecol. 43:525–532. 2014. View Article : Google Scholar
|
|
57
|
Garcia-Tizon Larroca S, Tayyar A, Poon LC,
Wright D and Nicolaides KH: Competing risks model in screening for
preeclampsia by biophysical and biochemical markers at 30-33 weeks'
gestation. Fetal Diagn Ther. 36:9–17. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Verlohren S, Herraiz I, Lapaire O,
Schlembach D, Zeisler H, Calda P, Sabria J, Markfeld-Erol F,
Galindo A, Schoofs K, et al: New gestational phase-specific cutoff
values for the use of the soluble fms-like tyrosine
kinase-1/placental growth factor ratio as a diagnostic test for
preeclampsia. Hypertension. 63:346–352. 2014. View Article : Google Scholar
|
|
59
|
Schoofs K, Grittner U, Engels T, Pape J,
Denk B, Henrich W and Verlohren S: The importance of repeated
measurements of the sFlt-1/PlGF ratio for the prediction of
preeclampsia and intrauterine growth restriction. J Perinat Med.
42:61–68. 2014. View Article : Google Scholar
|
|
60
|
Zhang J, Klebanoff MA and Roberts JM:
Prediction of adverse outcomes by common definitions of
hypertension in pregnancy. Obstet Gynecol. 97:261–267.
2001.PubMed/NCBI
|
|
61
|
No authors listed. ACOG practice bulletin
no. 202: Gestational hypertension and preeclampsia. Obstet Gynecol.
133:12019.
|
|
62
|
Bujold E, Roberge S, Lacasse Y, Bureau M,
Audibert F, Marcoux S, Forest JC and Giguère Y: Prevention of
preeclampsia and intrauterine growth restriction with aspirin
started in early pregnancy: A meta-analysis. Obstet Gynecol.
116:402–414. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
National Institute for Health and Care
Excellence (NICE): PlGF-based testing to help diagnose suspected
preterm pre-eclampsia. https://www.nice.org.uk/guidance/dg49. Accessed July
27, 2022
|
|
64
|
Dröge LA, Perschel FH, Stütz N, Gafron A,
Frank L, Busjahn A, Henrich W and Verlohren S: Prediction of
preeclampsia-related adverse outcomes with the sFlt-1 (soluble
fms-like tyrosine kinase 1)/PlGF (placental growth factor)-ratio in
the clinical routine: A real-world study. Hypertension. 77:461–471.
2021. View Article : Google Scholar
|
|
65
|
Hughes RCE, Phillips I, Florkowski CM and
Gullam J: The predictive value of the sFlt-1/PlGF ratio in
suspected preeclampsia in a New Zealand population: A prospective
cohort study. Aust N Z J Obstet Gynaecol. 63:34–41. 2023.
View Article : Google Scholar
|
|
66
|
Hund M, Allegranza D, Schoedl M, Dilba P,
Verhagen-Kamerbeek W and Stepan H: Multicenter prospective clinical
study to evaluate the prediction of short-term outcome in pregnant
women with suspected preeclampsia (PROGNOSIS): Study protocol. BMC
Pregnancy Childbirth. 14:3242014. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Zeisler H, Llurba E, Chantrain F, Vatish
M, Staff AC, Sennström M, Olovsson M, Brennecke SP, Stepan H,
Allegranza D, et al: Predictive value of the sFlt-1:PlGF ratio in
women with suspected preeclampsia. New Engl J Med. 374:13–22. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Hund M, Verhagen-Kamerbeek W, Reim M,
Messinger D, van der Does R and Stepan H: Influence of the
sFlt-1/PlGF ratio on clinical decision-making in women with
suspected preeclampsia-the PreOS study protocol. Hypertens
Pregnancy. 34:102–115. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Klein E, Schlembach D, Ramoni A, Langer E,
Bahlmann F, Grill S, Schaffenrath H, van der Does R, Messinger D,
Verhagen-Kamerbeek WD, et al: Influence of the sFlt-1/PlGF ratio on
clinical decision-making in women with suspected preeclampsia. PLoS
One. 11:e01560132016. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Perales A, Delgado JL, de la Calle M,
García-Hernández JA, Escudero AI, Campillos JM, Sarabia MD, Laíz B,
Duque M, Navarro M, et al: sFlt-1/PlGF for prediction of
early-onset pre-eclampsia: STEPS (study of early pre-eclampsia in
Spain). Ultrasound Obstet Gynecol. 50:373–382. 2017. View Article : Google Scholar
|
|
71
|
Herraiz I, Simón E, Gómez-Arriaga PI,
Quezada MS, García-Burguillo A, López-Jiménez EA and Galindo A:
Clinical implementation of the sFlt-1/PlGF ratio to identify
preeclampsia and fetal growth restriction: A prospective cohort
study. Pregnancy Hypertens. 13:279–285. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Sabriá E, Lequerica-Fernández P,
Lafuente-Ganuza P, Eguia-Ángeles E, Escudero AI, Martínez-Morillo
E, Barceló C and Álvarez FV: Addition of N-terminal pro-B
natriuretic peptide to soluble fms-like tyrosine kinase-1/placental
growth factor ratio >38 improves prediction of pre-eclampsia
requiring delivery within 1 week: A longitudinal cohort study.
Ultrasound Obstet Gynecol. 51:758–767. 2018. View Article : Google Scholar
|
|
73
|
Lafuente-Ganuza P, Lequerica-Fernandez P,
Carretero F, Escudero AI, Martinez-Morillo E, Sabria E, Herraiz I,
Galindo A, Lopez A, Martinez-Triguero ML and Alvarez FV: A more
accurate prediction to rule in and rule out pre-eclampsia using the
sFlt-1/PlGF ratio and NT-proBNP as biomarkers. Clin Chem Lab Med.
58:399–407. 2020. View Article : Google Scholar
|
|
74
|
Sovio U, White IR, Dacey A, Pasupathy D
and Smith GCS: Screening for fetal growth restriction with
universal third trimester ultrasonography in nulliparous women in
the pregnancy outcome prediction (POP) study: A prospective cohort
study. Lancet. 386:2089–2097. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Zeisler H, Llurba E, Chantraine FJ, Vatish
M, Staff AC, Sennström M, Olovsson M, Brennecke SP, Stepan H,
Allegranza D, et al: Soluble fms-like tyrosine kinase-1 to
placental growth factor ratio: Ruling out pre-eclampsia for up to 4
weeks and value of retesting. Ultrasound Obstet Gynecol.
53:367–375. 2019. View Article : Google Scholar :
|
|
76
|
Bian X, Biswas A, Huang X, Lee KJ, Li TK,
Masuyama H, Ohkuchi A, Park JS, Saito S, Tan KH, et al: Short-term
prediction of adverse outcomes using the sFlt-1 (soluble fms-like
tyrosine kinase 1)/PlGF (placental growth factor) ratio in Asian
women with suspected preeclampsia. Hypertension. 74:164–172. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Cerdeira AS, O'Sullivan J, Ohuma EO,
Harrington D, Szafranski P, Black R, Mackillop L, Impey L,
Greenwood C, James T, et al: Randomized interventional study on
prediction of preeclampsia/eclampsia in women with suspected
preeclampsia: INSPIRE. Hypertension. 74:983–990. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Cerdeira AS, O'Sullivan J, Ohuma EO, James
T, Papageorghiou AT, Knight M and Vatish M: Ruling out preeclampsia
in the next 4 weeks using a soluble fms-like tyrosine kinase
1/placental growth factor ratio ≤38: Secondary analysis of the
interventional study on prediction of preeclampsia/eclampsia in
women with suspected preeclampsia. Am J Obstet Gynecol.
226:443–445. 2022. View Article : Google Scholar
|
|
79
|
Perry H, Binder J, Kalafat E, Jones S,
Thilaganathan B and Khalil A: Angiogenic marker prognostic models
in pregnant women with hypertension. Hypertension. 75:755–761.
2020. View Article : Google Scholar
|
|
80
|
Peguero A, Fernandez-Blanco L, Mazarico E,
Benitez L, Gonzalez A, Youssef L, Crispi F, Hernandez S and
Figueras F: Added prognostic value of longitudinal changes of
angiogenic factors in early-onset severe pre-eclampsia: A
prospective cohort study. BJOG. 128:158–165. 2021. View Article : Google Scholar
|
|
81
|
Dathan-Stumpf A, Czarnowsky V, Hein V,
Andraczek T and Stepan H: Real-world data on the clinical use of
angiogenic factors in pregnancies with placental dysfunction. Am J
Obstet Gynecol. 226(2S): S1037–S1047.e2. 2022. View Article : Google Scholar
|
|
82
|
Kifle MM, Dahal P, Vatish M, Cerdeira AS
and Ohuma EO: The prognostic utility of soluble fms-like tyrosine
kinase-1 (sFlt-1) and placental growth factor (PIGF) biomarkers for
predicting preeclampsia: A secondary analysis of data from the
INSPIRE trial. BMC Pregnancy Childbirth. 22:5202022. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Chaemsaithong P, Sahota DS and Poon LC:
First trimester preeclampsia screening and prediction. Am J Obstet
Gynecol. 226(2S): S1071–S1097.e2. 2022. View Article : Google Scholar
|
|
84
|
Crovetto F, Figueras F, Triunfo S, Crispi
F, Rodriguez-Sureda V, Peguero A, Dominguez C and Gratacos E: Added
value of angiogenic factors for the prediction of early and late
preeclampsia in the first trimester of pregnancy. Fetal Diagn Ther.
35:258–266. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Crovetto F, Figueras F, Triunfo S, Crispi
F, Rodriguez-Sureda V, Dominguez C, Llurba E and Gratacós E: First
trimester screening for early and late preeclampsia based on
maternal characteristics, biophysical parameters, and angiogenic
factors. Prenat Diagn. 35:183–191. 2015. View Article : Google Scholar
|
|
86
|
Lamain-de Ruiter M, Kwee A, Naaktgeboren
CA, Louhanepessy RD, De Groot I, Evers IM, Groenendaal F, Hering
YR, Huisjes AJM, Kirpestein C, et al: External validation of
prognostic models for preeclampsia in a Dutch multicenter
prospective cohort. Hypertens Pregnancy. 38:78–88. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Tsiakkas A, Mendez O, Wright A, Wright D
and Nicolaides KH: Maternal serum soluble fms-like tyrosine
kinase-1 at 12, 22, 32 and 36 weeks' gestation in screening for
pre-eclampsia. Ultrasound Obstet Gynecol. 47:478–483. 2016.
View Article : Google Scholar
|
|
88
|
Diguisto C, Piver E, Gouge AL, Eboue F,
Vaillant CL, Maréchaud M, Goua V, Giraudeau B and Perrotin F: First
trimester uterine artery Doppler, sFlt-1 and PlGF to predict
preeclampsia in a high-risk population. J Matern Fetal Neonatal
Med. 30:1514–1519. 2017. View Article : Google Scholar
|
|
89
|
Verlohren S, Brennecke SP, Galindo A,
Karumanchi SA, Mirkovic LB, Schlembach D, Stepan H, Vatish M,
Zeisler H and Rana S: Clinical interpretation and implementation of
the sFlt-1/PlGF ratio in the prediction, diagnosis and management
of preeclampsia. Pregnancy Hypertens. 27:42–50. 2022. View Article : Google Scholar
|
|
90
|
Dathan-Stumpf A, Rieger A, Verlohren S,
Wolf C and Stepan H: sFlt-1/PlGF ratio for prediction of
preeclampsia in clinical routine: A pragmatic real-world analysis
of healthcare resource utilisation. PLoS One. 17:e02634432022.
View Article : Google Scholar : PubMed/NCBI
|