Introduction
Colorectal cancer most often disseminates to the
liver and lung and rarely to the skin (1,2). The
incidence of skin involvement for colorectal cancer is reported as
low as 2.3% (3). Cutaneous
metastases from colorectal cancer are generally caused by direct
tumor extension, dissemination, invasion of the embryonic
ligaments, or implantation during surgical resection (4). Massive invasion of rectal cancer to
the perineal skin is considered extremely rare, since the sensation
of a perianal lump, altered bowel habits, bleeding or soiling,
usually leads to diagnosis prior to the occurrence of massive
invasion to the perineal area (5).
Patients with perineal skin invasion by rectal cancer present with
symptoms of severe pain, continuous bleeding and distressing
discharge, which significantly affect their quality of life.
In some cases, cancer lesions may be localized,
allowing for surgical intervention as an effective treatment
modality (3). However, in general,
for these patients, the indication for radical resection is
controversial, as the survival benefits and surgical outcomes have
not been clearly determined (6–8).
In this study, we report 3 cases of rectal cancer
with perineal skin involvement who underwent multimodality
treatment, including effective extended radical resection.
Case report
Case 1
The patient was a 52-year-old man with rectal cancer
that had invaded the perineum. A colostomy was constructed in
September, 2003, as the tumor presented with extensive local
invasion and complete resection was impossible due to invasion of
the pelvic wall. After the operation, the patient received
chemotherapy with irinotecan (CPT-11) and doxifluridine and
radiotherapy (50 Gy). The patient achieved stable disease,
according to Response Evaluation Criteria in Solid Tumor (RECIST);
the tumor kept eroding the skin and the patient experienced
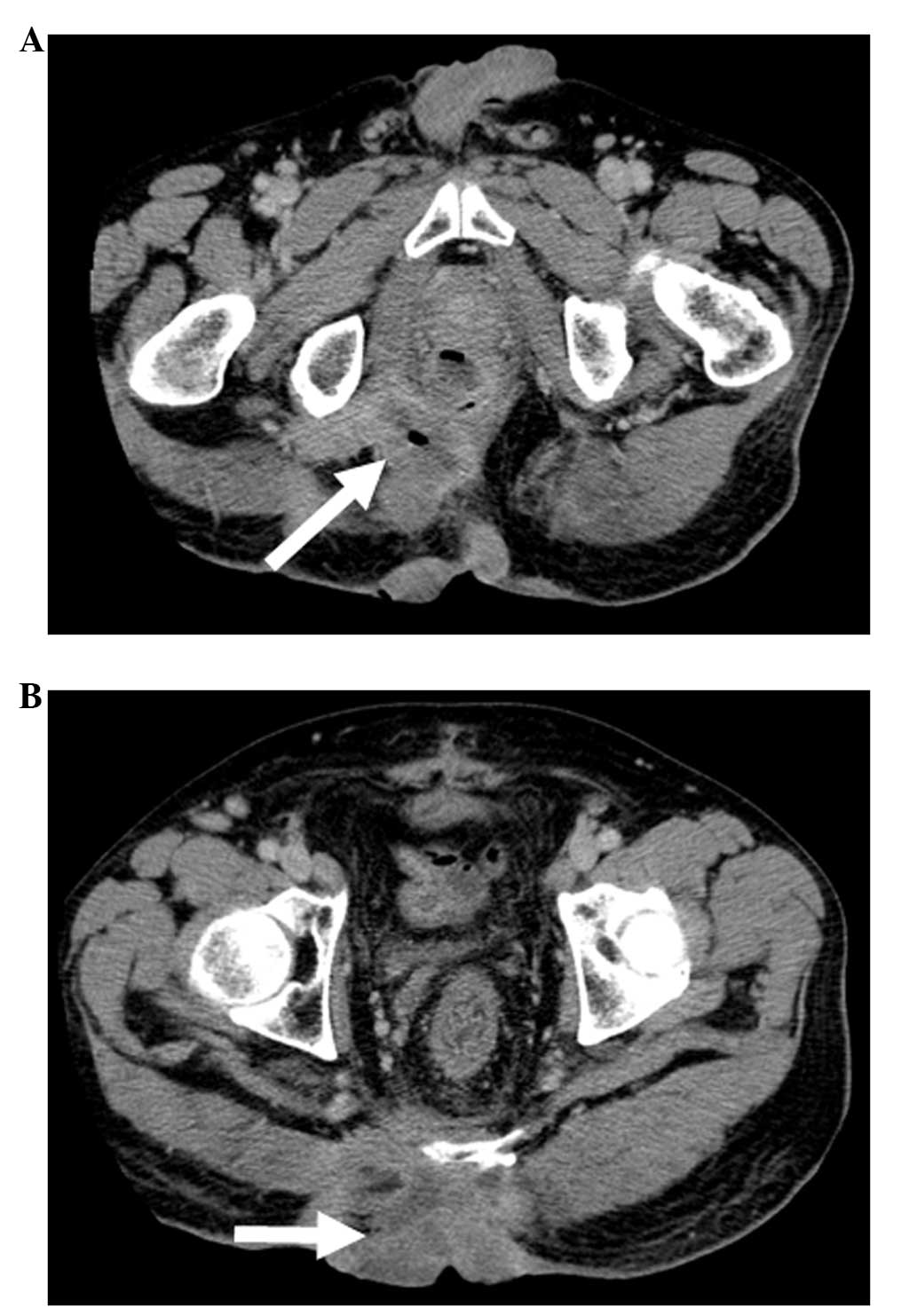
constant pain. Pelvic computed tomography (CT) revealed that the
rectal cancer had invaded the left levator ani and gluteus maximus
muscles, perineal skin, bladder, seminal vesicle and prostate gland
(Table I, Fig. 1A and B). The lesion was highly
advanced locally, but there was no evidence of distant metastasis;
therefore, we planned an extended radical resection with curative
intent.
 | Table IPatient profiles. |
Table I
Patient profiles.
| Cases | Age/gender | Stage | Operation | Preoperative
treatment | Outcome |
|---|
| Case 1 | 52/M | T4bN0M0 | TPE | CPT-11 + 5-DFUR and
stage IIc radiotherapy (50 Gy) | Died 3 years after
the operation |
| Case 2 | 38/M | T4bN1bM1a stage
IV | TPE | 6 cycles of
mFOLFOX6a and radiotherapy (40
Gy) | Alive |
| Case 3 | 50/F | T4bN0M0 stage
IIc | APR | UFT/LV + CPT-11 and
radiotherapy (45 Gy) | Alive |
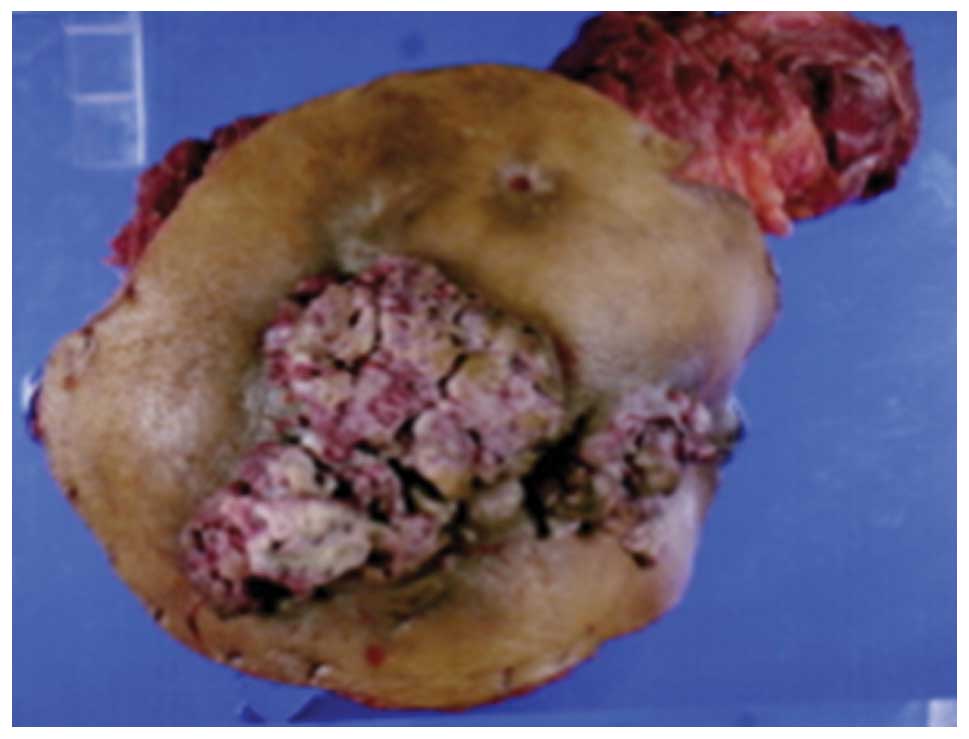
We performed a total pelvic exenteration (TPE) with
extended resection of adjacent organs, including the perineal skin,
in July, 2004 (Fig. 2). To reduce
the risk of severe pelvic infection (9), a reconstruction was concomitantly
performed, using a vertical rectus abdominis myocutaneous (VRAM)
flap. The histological examination of the tumor revealed a
moderately differentiated adenocarcinoma with extensive venous and
lymphatic invasion and the examination of the 32 resected lymph
nodes confirmed the absence of lymph node metastasis. A
histologically complete resection was performed.
The patient succumbed to the disease 3 years after
surgery, due to local re-recurrence diagnosed 6 months prior to
death. Up to the diagnosis of local re-recurrence, the daily
quality of life of the patient was not significantly affected.
Case 2
The patient was a 38-year-old man, complaining of
anal discharge, due to rectal cancer with rectoperineal fistula.
The tumor was diagnosed as unresectable, due to a highly advanced
primary tumor and the presence of liver metastasis. A colostomy was
constructed in December, 2006, prior to the initiation of
chemoradiotherapy. The patient received 6 cycles of chemotherapy
with mFOLFOX6 and radiotherapy (40 Gy) and achieved a partial
response (PR), according to RECIST (Table I).
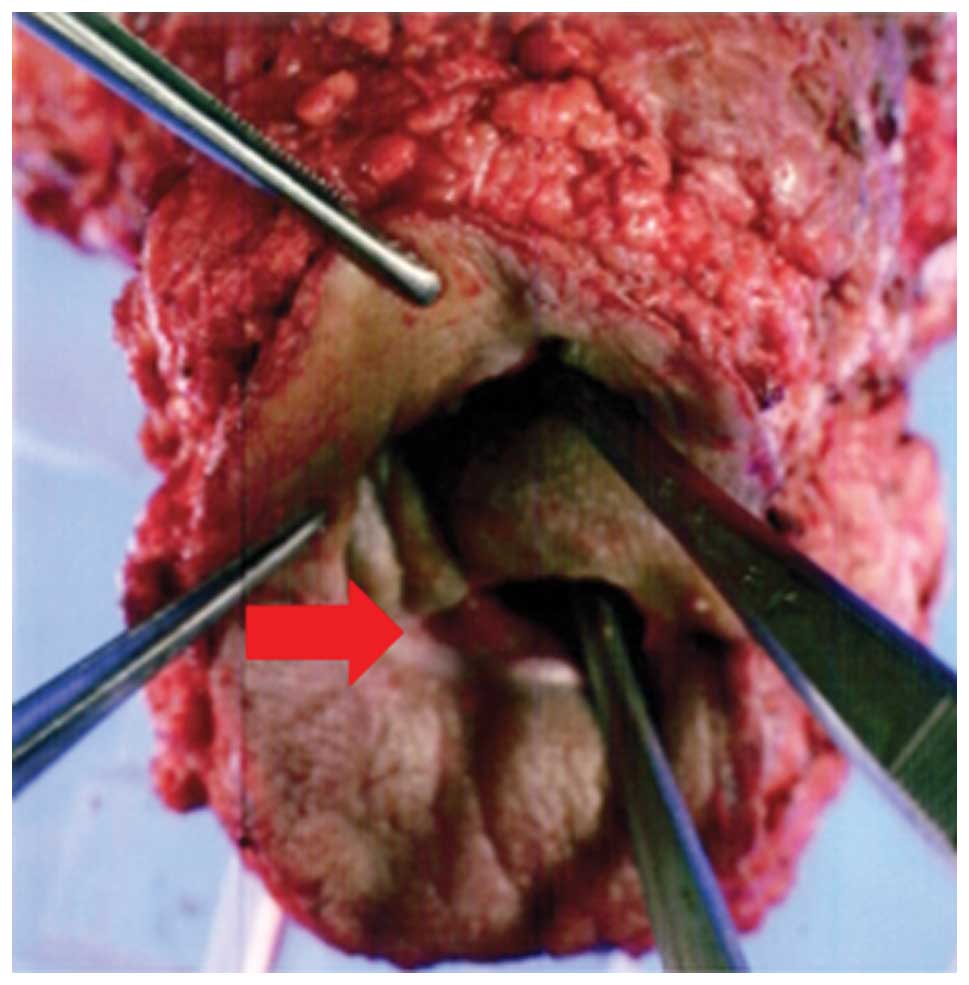
We performed a TPE on the patient, with extended
resection of the perineal skin, followed by reconstruction, using a
VRAM flap, in May, 2007 (Fig. 3).
The histological examination of the tumor revealed a moderately
differentiated adenocarcinoma with extensive venous and lymphatic
invasion and the examination of the 38 resected lymph nodes
confirmed the absence of lymph node metastasis.
After the operation, the patient received
chemotherapy with mFOLFOX and bevasizumab (Bev), followed by
partial hepatectomy. After the hepatectomy, the patient received
adjuvant chemotherapy with FOLFIRI and Bev. The patient is
currently free from recurrence, 5 years after the hepatectomy.
Case 3
The patient was a 50-year-old woman, complaining of
general fatigue and anemia. The patient had a sizeable tumor,
visible at the anus (Fig. 4). A
rectal biopsy confirmed the diagnosis of poorly differentiated
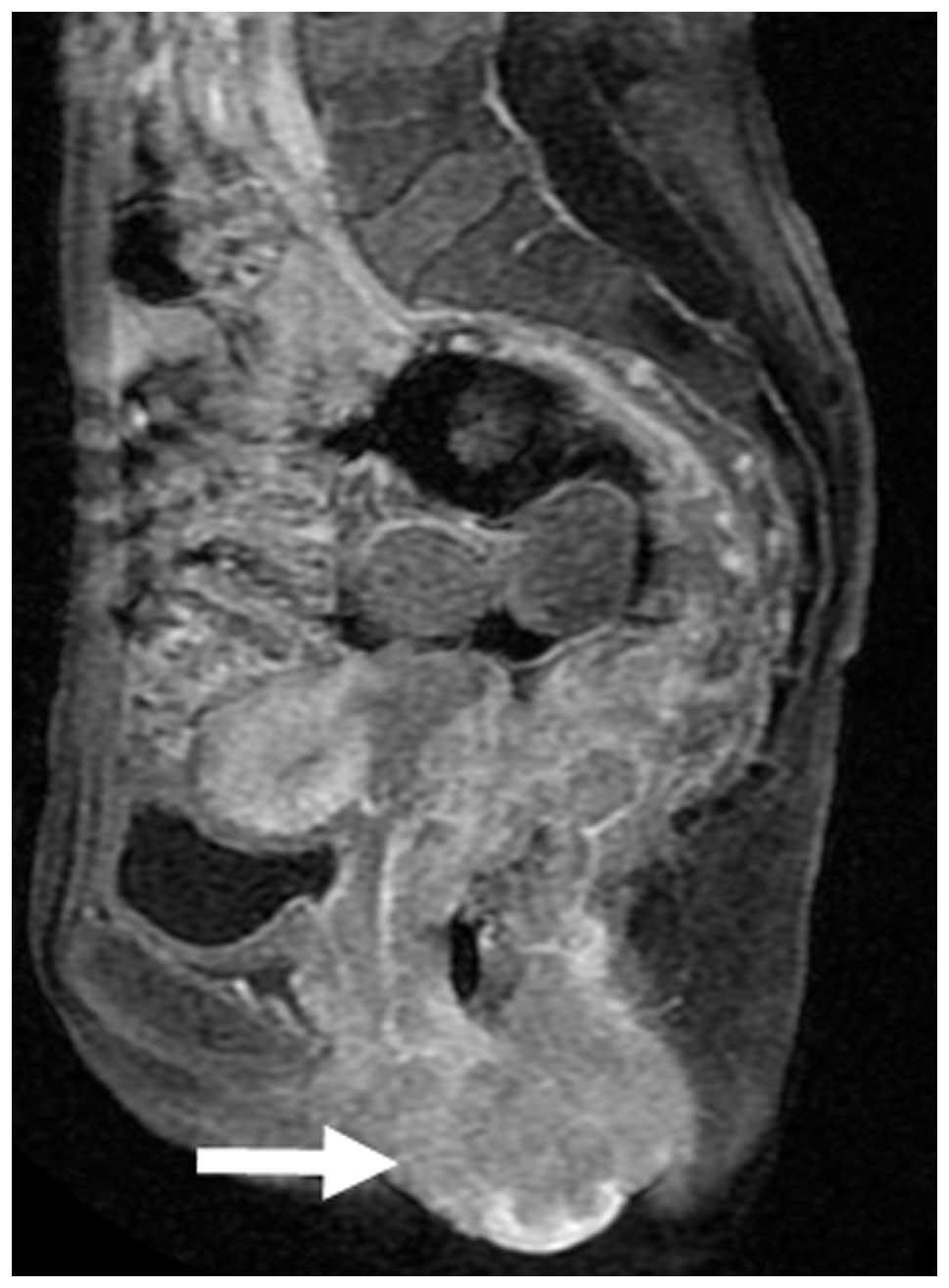
adenocarcinoma. Pelvic magnetic resonance imaging revealed that the
rectal cancer had invaded the uterus, cervix, vagina, levator ani
muscle and perianal skin (Fig.
5).
The patient received chemotherapy treatment with
uracil/tegafur/leucovorin plus CPT-11 and radiotherapy (45 Gy) and
achieved a PR, according to RECIST (Table I). We performed abdominoperineal
resection with extended resection of the perineal skin, followed by
reconstruction using a VRAM flap, in March, 2011. The histological
examination of the tumor revealed a poorly differentiated
adenocarcinoma with extensive lymphatic invasion and the
examination of the 31 resected lymph nodes confirmed the absence of
lymph node metastasis.
Seven months after surgery, in October, 2011, the
cancer metastasized to the lung. The patient received 3 cycles of
chemotherapy with XELOX + Bev, which effectively controlled the
metastases. The patient subsequently received a left upper
lobectomy in March, 2012, followed by a right S6 segmental
resection in June of the same year. The patient experienced local
re-recurrence in May, 2013 and is currently under treatment.
Discussion
Approximately 10% of patients with colorectal cancer
exhibit locally advanced disease with peritoneal involvement (T4a)
or invasion of adjacent organs (T4b) at the time of diagnosis
(10). In this type of cancer, the
most frequently invaded organ is the urinary bladder, followed by
the small intestine (11). A
literature search revealed that locally advanced rectal cancer
directly invading the perineal skin, is rare.
Direct invasion of the tumor into the skin primarily
occurs through ulceration or inflammation. Once the malignant
ulcers are infected, they are often foul-smelling, painful and
bleeding, severely compromising the quality of life of the
patients.
According to the National Comprehensive Cancer
Network guidelines, neoadjuvant therapy should be administered for
the treatment of locally advanced rectal cancer. In addition, it
was suggested that extracolonic invasion is not necessarily a poor
prognostic factor (11). Rödel
et al (12) reported that
curative operations may be performed on 94% of patients with
contiguous or adherent-to-adjacent pelvic organs, following CRT
with 5-fluorouracil regimen. A resection of the pelvic tumor with
negative margins was achieved in 84% of patients.
Rectal cancer with massive perineal skin invasion
should be managed differently from locally advanced rectal cancer,
since, once tumor cells have invaded the perineal skin, tumor
dissemination may occur via hematogenous and lymphatic routes
(13). There are currently no
reports on the appropriate treatment for such significantly
advanced local rectal cancer.
In our cases, the patients did not achieve a
complete cure. All the patients requested a surgical resection as
they all suffered from severe and annoying symptoms. Therefore, we
planned a multimodality treatment with curative intent, despite the
lack of firm evidence. None of the cases had severe postoperative
complications. The patients almost fully returned to their daily
activities. In particular, the multimodal treatment was highly
effective in Case 2, although the patient had liver metastasis.
The outcome of these cases shed light on the
multimodal treatment, including extended surgery, for rectal
cancers with massive perineal skin invasion. There are currently no
data on the effectiveness of various treatment modalities for this
type of cancer, as there are simply too few cases to make
definitive conclusions. An extensive study should be conducted to
determine the prognostic factors for long-term survival. Such
studies could be informative to the selection of patients who
should receive multimodal treatment with curative intent.
In conclusion, for rectal cancer patients with
massive invasion to the perineum, multimodal treatment, including
extended radical surgery, can be an effective treatment of choice,
in terms of balancing cancer control and quality of life.
References
|
1
|
Sgambati SA and Barrows GH: Cutaneous
metastasis of colon carcinoma: a case report. Conn Med. 57:665–667.
1993.PubMed/NCBI
|
|
2
|
Goris Gbenou MC, Wahidy T, Llinares K, et
al: Atypical phimosis secondary to a preputial metastasis from
rectal carcinoma. Case Rep Oncol. 4:542–546. 2011.PubMed/NCBI
|
|
3
|
Lookingbill DP, Spangler N and Sexton FM:
Skin involvement as the presenting sign of internal carcinoma-a
retrospective study of 7316 cancer-patients. J Am Acad Dermatol.
22:19–26. 1990.PubMed/NCBI
|
|
4
|
Reilly WT, Nelson H, Schroeder G, et al:
Wound recurrence following conventional treatment for colorectal
cancer. A rare but perhaps underestimated problem. Dis Colon
Rectum. 39:200–207. 1996. View Article : Google Scholar
|
|
5
|
Jensen SL, Shokouh-Amiri MH, Hagen K, et
al: Adenocarcinoma of the anal ducts. A series of 21 cases. Dis
Colon Rectum. 31:268–272. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lo S and Crew J: Penile metastasis from
rectal carcinoma. Singapore Med J. 45:2992004.PubMed/NCBI
|
|
7
|
Maestro MA, Martinez-Pineiro L, Moreno SS,
et al: Penile metastasis of rectal carcinoma. Case report and
bibliographic review. Arch Esp Urol. 64:981–984. 2011.(In English,
Spanish).
|
|
8
|
Yildirim M, Coskun A, Purten M, et al: A
clinical case of the penile metastasis from the rectal carcinoma.
Radiol Oncol. 44:121–123. 2011.PubMed/NCBI
|
|
9
|
Uemura M, Ikeda M, Sekimoto M, et al:
Prevention of severe pelvic abscess formation following extended
radical surgery for locally reccurent of rectal cancer. Ann Surg
Oncol. 16:2204–2210. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lehnert T, Methner M, Pollok A, et al:
Multiviscerral resection for locally advanced primary colon and
rectal cancer: An analysis of prognostic factors in 201 patients.
Ann Surg. 235:217–225. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Poeze M, Houbiers JG, van de Velde CJ, et
al: Radical resection of locally advanced colorectal cancer. Br J
Surg. 82:1386–1390. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rödel C, Grabenbauer GG, Schick C, et al:
Preoperative radiation with concurrent 5-fluorouracil for locally
advanced T4-primary rectal cancer. Strahlenther Onkol. 176:161–167.
2000.PubMed/NCBI
|
|
13
|
Kauffman CL and Sina B: Metastatic
inflammatory carcinoma of the rectum: tumor spread by three routes.
Am J Dermatopathol. 19:528–532. 1997. View Article : Google Scholar : PubMed/NCBI
|