Introduction
Hepatitis B virus (HBV) infection is a major cause
of hepatocellular carcinoma (HCC) worldwide (1). In Japan, hepatitis B (HB)
immunoglobulin and HB vaccination have been used since 1986 to
prevent maternal-fetal transmission of HBV. As a result, the
incidence of HB surface antigen (HBsAg) positivity among blood
donors had decreased to 0.04% by 2006, indicating the effectiveness
of this program of vertical HBV transmission prevention (2). In addition, the first-generation
nucleot(s)ide analogues were approved in 2000 and their long-term
administration reduced the risk of HCC in patients with chronic HBV
infection (3,4). Thus, a reduction in the number of HCC
patients with chronic HBV infection is to be expected. However,
~16% of HCC patients are HBsAg-positive and the prevalence of HCC
among patients with chronic HBV infection has not decreased in
Japan since 1996 (5).
Several factors are associated with the development
of HCC in patients with chronic HBV infection. Hepatic inflammation
and fibrosis are well-documented risk factors (6). In addition, elevated serum HBV DNA
level, HBV genotype C and a high serum HBsAg level are risk factors
for HCC (7,8). Using a combination of these risk
factors, several HCC prediction scores have been developed for HBV
carriers (9,10). The HCC prediction score reported by
Wong et al (9) is a simple
scoring system that uses parameters such as age, serum albumin
level, serum bilirubin level, HBV DNA level and presence of liver
cirrhosis, all of which are available in routine clinical practice
and for field surveys.
Besides hepatic and viral factors, there are several
other risk factors for the development of HCC. Lifestyle factors,
such as alcohol intake and smoking, were shown to increase the risk
for HCC (11). Obesity and type 2
diabetes mellitus with insulin resistance are also considered as
risk factors (12,13). The percentage of patients diagnosed
with obesity- or type 2 diabetes mellitus-associated HCC has been
increasing annually in Japan (5,14).
Moreover, elderly patients are at higher risk for developing HCC,
even after being stratified by stage of hepatic fibrosis (15). Aging is a social issue in Japan and
is becoming one of the major risk factors for HCC (15). Although all the abovementioned risk
factors are considered to be independently associated with the
onset of HCC, the time trends for these risk factors remain unclear
in HCC patients with chronic HBV infection.
The aim of this study was to assess the time trends
of clinical characteristics in HCC patients with chronic HBV
infection.
Subjects and methods
Study design and subjects
We performed a field survey to assess the time
trends of clinical characteristics in HCC patients with chronic HBV
infection who visited Kurume University School of Medicine. The
inclusion criteria included presence of HCC, HBsAg positivity and
hepatitis C virus (HCV) antibody negativity. Patients with
autoimmune hepatitis, primary biliary cirrhosis or hemochromatosis
were excluded.
For evaluating the time trends for the annual number
of HCC patients with HBV infection, we enrolled a total of 264
patients between 1991 and 2012. In Japan, nucleot(s)ide analogues
were approved in 2000 and their use has markedly improved the
natural course of patients with chronic hepatitis B. Therefore, the
time trends of clinical characteristics were evaluated using 156
HCC patients with chronic HBV infection between 2000 and 2012.
Clinical characteristics and
lifestyle
Data on clinical characteristics and lifestyle
factors, including age, gender, alcohol intake and cumulative
cigarette consumption, were collected at the time of the first
medical examination. Body mass index (BMI) was calculated as body
weight in kilograms divided by the square of height in meters
(kg/m2). The cumulative cigarette consumption was
estimated using the Brinkman index (number of cigarettes smoked/day
× years of smoking) (16).
Biochemical examinations
Venous blood samples were collected in the morning
after a 12-h overnight fast. The following biochemical examinations
were then performed, using standard clinical methods as previously
described (17): blood platelet
count, white blood cell count, prothrombin time, plasma glucose
levels, hemoglobin A1c (HbA1c) levels and serum levels of aspartate
aminotransferase (AST), alanine aminotransferase (ALT), albumin,
total bilirubin, insulin, α-fetoprotein (AFP) and des-γ-carboxy
prothrombin (DCP).
Diagnosis of HCC
The diagnosis of HCC was based on the criteria of
the clinical practice manual proposed by the Japan Society of
Hepatology (JSH) (18) using serum
AFP and DCP levels and imaging techniques including
ultrasonography, computed tomography, magnetic resonance imaging,
hepatic angiography and/or tumor biopsy.
Staging and treatment of HCC
The Milan criteria (single nodule ≤5 cm or 3 nodules
<3 cm) were used for HCC staging (14). The treatment of HCC was categorized
as follows: i) local treatment such as hepatic resection,
percutaneous ethanol injection therapy and radiofrequency ablation;
ii) transcatheter arterial chemoembolization; iii) hepatic arterial
infusion chemotherapy; iv) best supportive care; and v) liver
transplantation.
HCC surveillance
The JSH proposed the Consensus-Based Clinical
Practice Guidelines for the Management of HCC in Japan (18). These guidelines recommend assessing
serum tumor marker levels and conducting imaging examinations,
including ultrasonography, at intervals of 3–6 months, according to
the HCC risk.
The patients were classified into the following 3
HCC surveillance categories: i) patients with no HCC surveillance;
ii) irregular surveillance (patients under HCC surveillance with
either serum tumor marker levels or imaging examination, or at
longer intervals than recommended); and iii) regular surveillance
(patients under HCC surveillance according to the guidelines).
Measurement of HBsAg, anti-HCV antibodies
and HBV DNA
Serum HBsAg and anti-HCV antibody levels were
measured using standard clinical methods (Department of Clinical
Laboratory Medicine, Kurume University Hospital, Kurume, Fukuoka,
Japan) (19). The serum HBV DNA
levels were measured using the COBAS TaqMan® HBV Auto
v2.0 kit (Roche Diagnostics, Tokyo, Japan), which has a lower
detection limit of 2.1 log copies/ml.
Diagnosis of liver cirrhosis
Hepatic fibrosis was evaluated using the
AST-to-platelet ratio index (APRI), as follows: serum AST level
(U/l)/upper limit of normal AST level (33 U/l) × 100/platelet count
(x104/ml) (20).
Patients with APRI values >1.5 were diagnosed with liver
cirrhosis, as previously described (20).
Clinical scoring system for the
prediction of HCC in chronic HBV carriers
We employed the HCC prediction score reported by
Wong et al (9). This score
is constructed from the following 5 parameters: age (>50 years,
+3 points); serum albumin level (≤3.5 g/dl, +20 points); serum
bilirubin level (>1.05 mg/dl, +1.5 points); serum HBV DNA level
(4–6 log copies/ml, +1 point, >6 log copies/ml, +4 points); and
liver cirrhosis (present, +15 points) (9). According to the total score, the
patients were classified as having low (<5), medium (5–19),
or high risk (>19), as previously described (9).
Diagnosis of diabetes mellitus
Diabetes mellitus was diagnosed if the fasting blood
glucose levels were >126 mg/dl or the HbA1c levels were
>6.9%, according to the Diagnostic Criteria for Diabetes
Mellitus (21), or by the
documented use of antidiabetic agents.
Statistical analysis
The alterations in the annual number of HCC patients
with chronic HBV infection were statistically evaluated using
regression analysis and the time trends of the patient
characteristics were analyzed by the Jonckheere-Terpstra proportion
trend test. The quoted P-values are two-sided and P<0.05 was
considered to indicate a statistically significant difference. All
the analyses were performed using SAS software, version 9.3 (SAS
Institute Inc., Cary, NC, USA).
Results
Number of patients
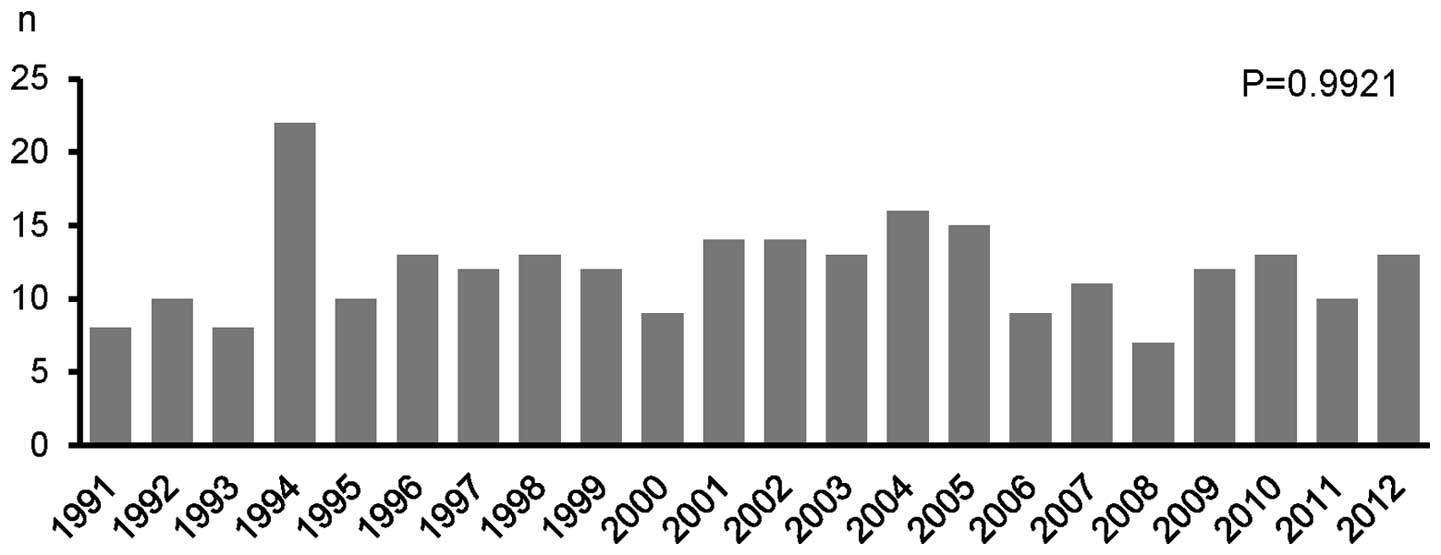
The annual number of HCC patients with chronic HBV
infection in the years between 1991 and 2012 is shown in Fig. 1. There was no significant decrease
in the annual number of patients during the study period (P=0.9921;
95% confidence interval, −0.23677 to 0.23451).
HCC prediction score
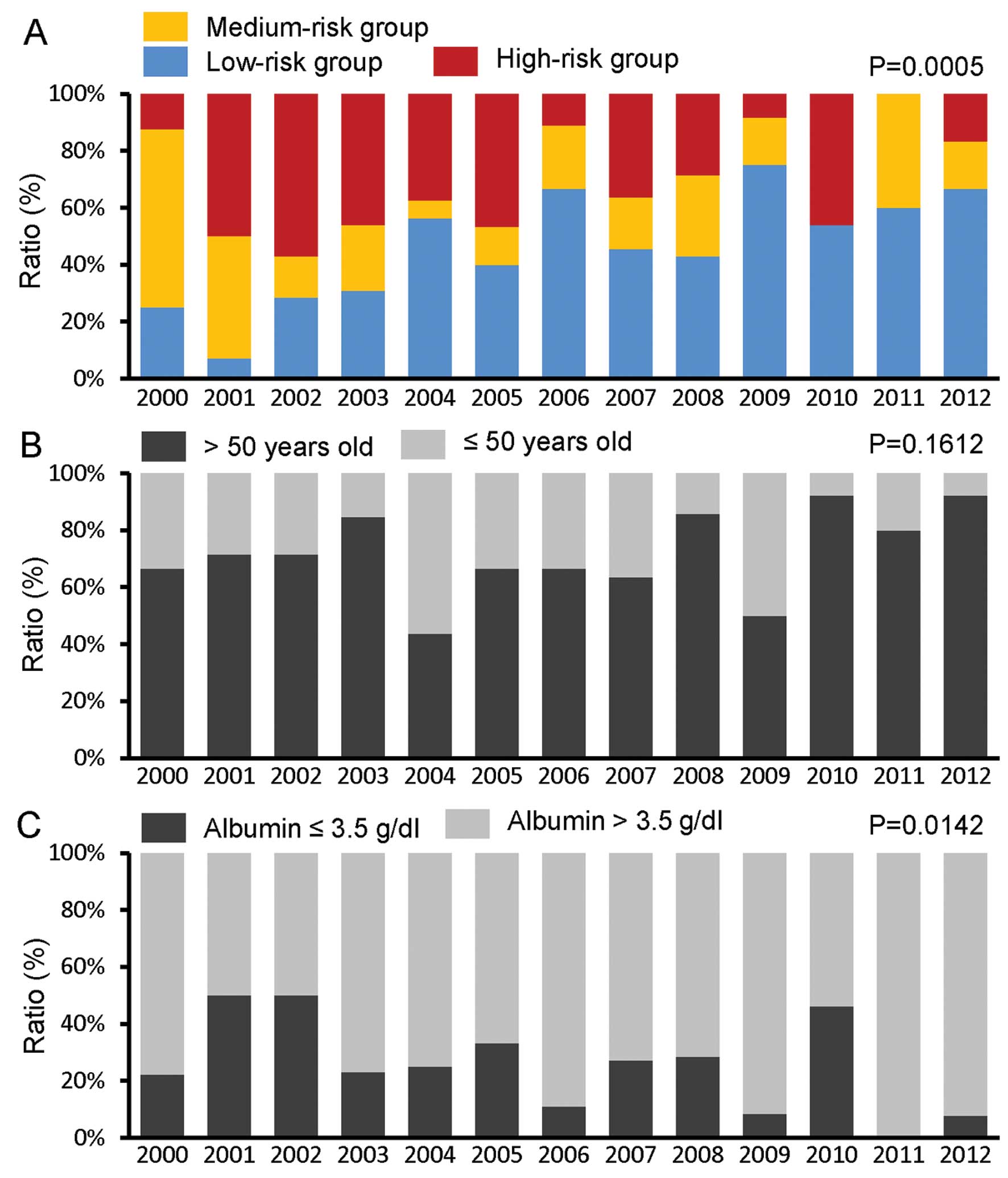
The proportion of patients with high and medium
risk, according to the HCC prediction score, was significantly
decreased, while the proportion of low-risk patients increased
significantly during the study period (P=0.0005) (Fig. 2A).
The HCC prediction score is constructed using
parameters such as age, serum albumin level, serum bilirubin level,
serum HBV DNA level and presence of liver cirrhosis. Although the
proportion of patients who were older than the threshold for
increased risk (>50 years) did not significantly change
(P=0.1612) (Fig. 2B), the
proportion of patients with serum albumin levels below the
threshold for increased risk (≤3.5 g/dl) was significantly
decreased (P=0.0142) (Fig. 2C).
The proportions of patients with elevated serum bilirubin levels
(>1.05 mg/dl) did not significantly change (P=0.2433) (Fig. 2D); however, the proportion of those
with elevated HBV DNA levels (>4 log copies/ml) and those with
liver cirrhosis was significantly decreased during the study period
(P=0.0072) (Fig. 2E) and
(P=0.0001) (Fig. 2F).
Age and gender
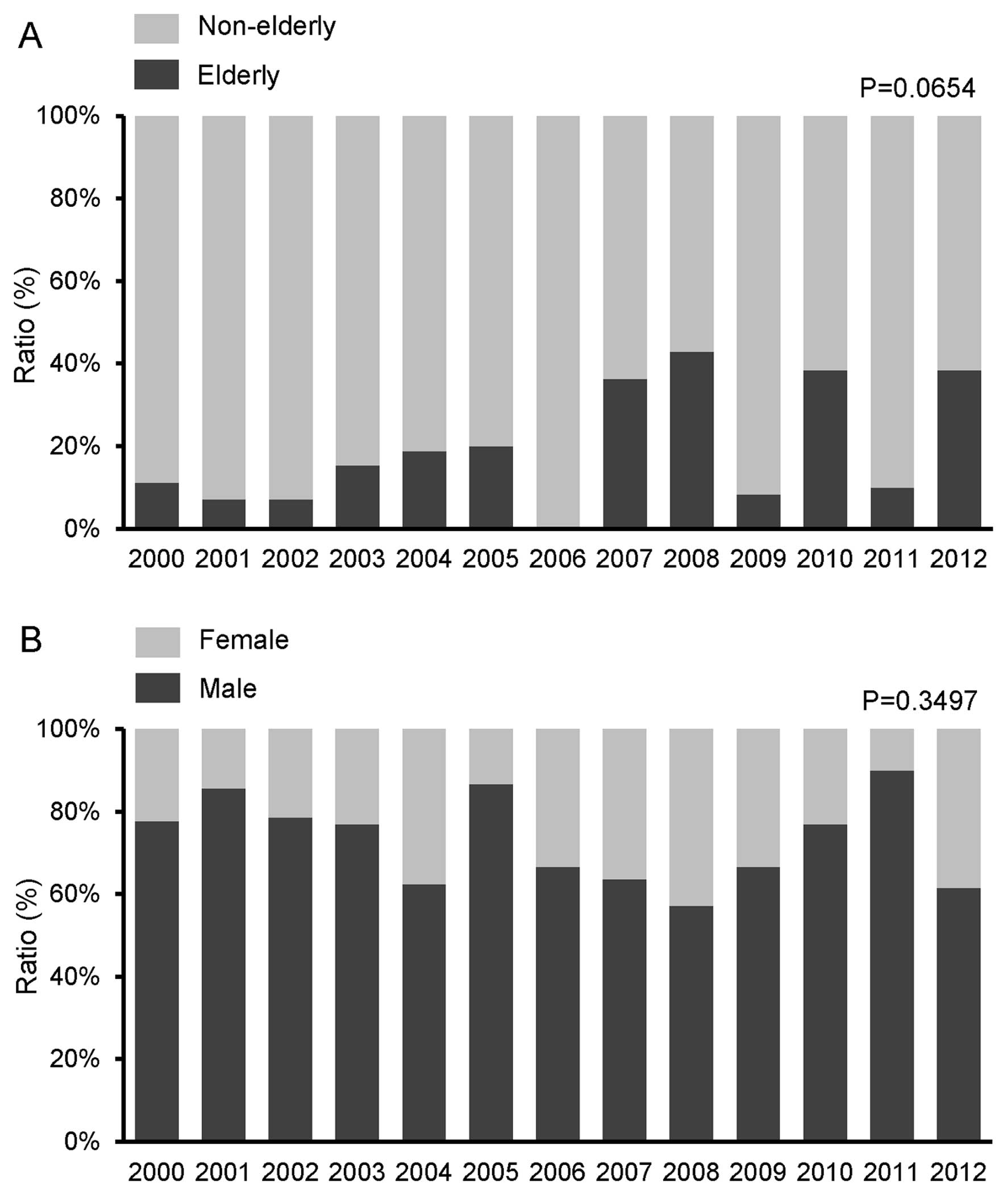
The proportion of elderly patients (≥65 years)
exhibited a tendency to increase during the study period (P=0.0654)
(Fig. 3A), whereas no significant
change was observed in the proportion of male patients (P=0.3497)
(Fig. 3B).
Alcohol intake and cumulative cigarette
consumption
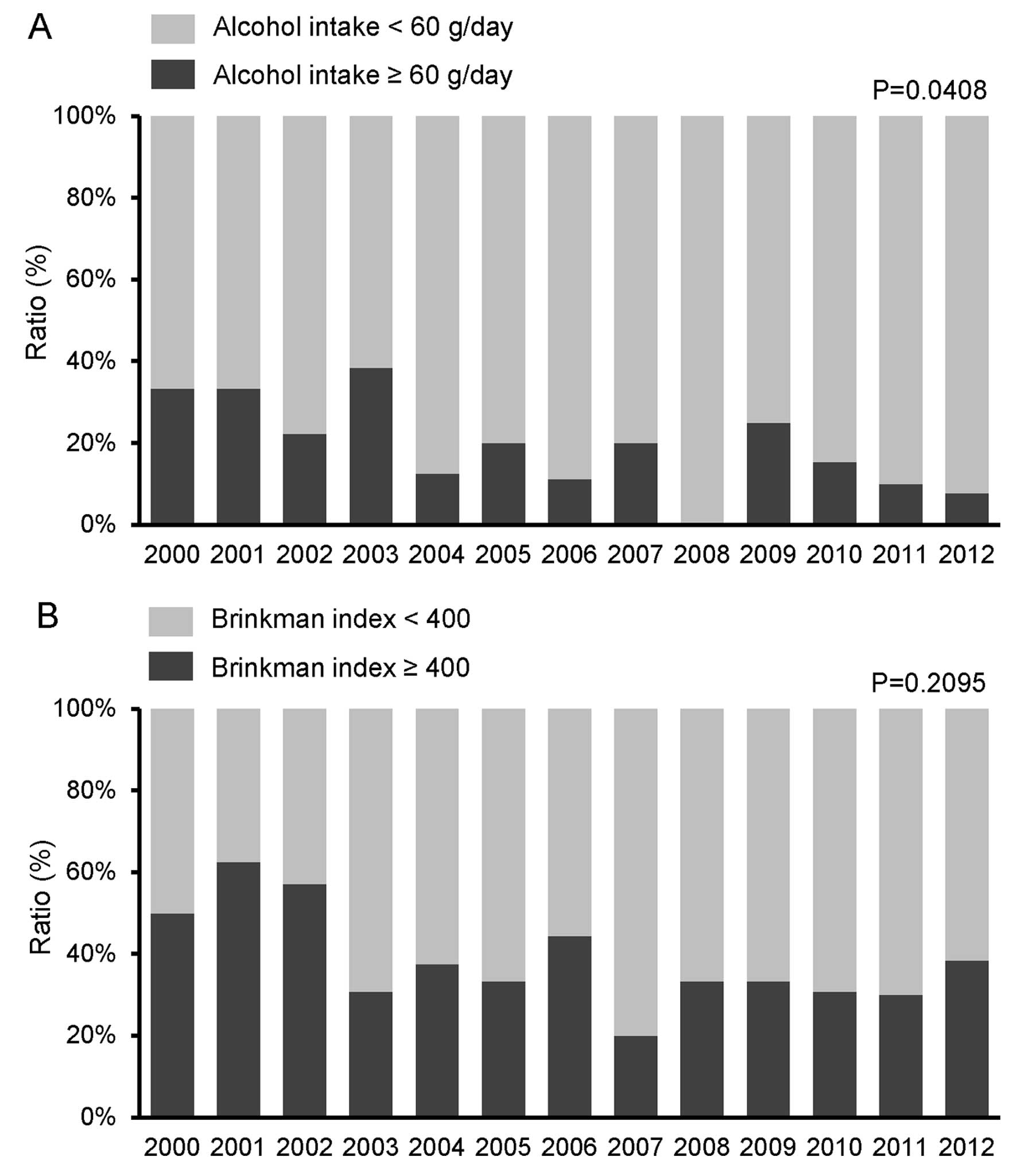
The proportion of patients with a habitual alcohol
intake of ≥60 g/day significantly decreased during the study period
(P=0.0408) (Fig. 4A). By contrast,
no significant change was observed in the proportion of patients
with a high Brinkmann index (>400; P=0.2095) (Fig. 4B).
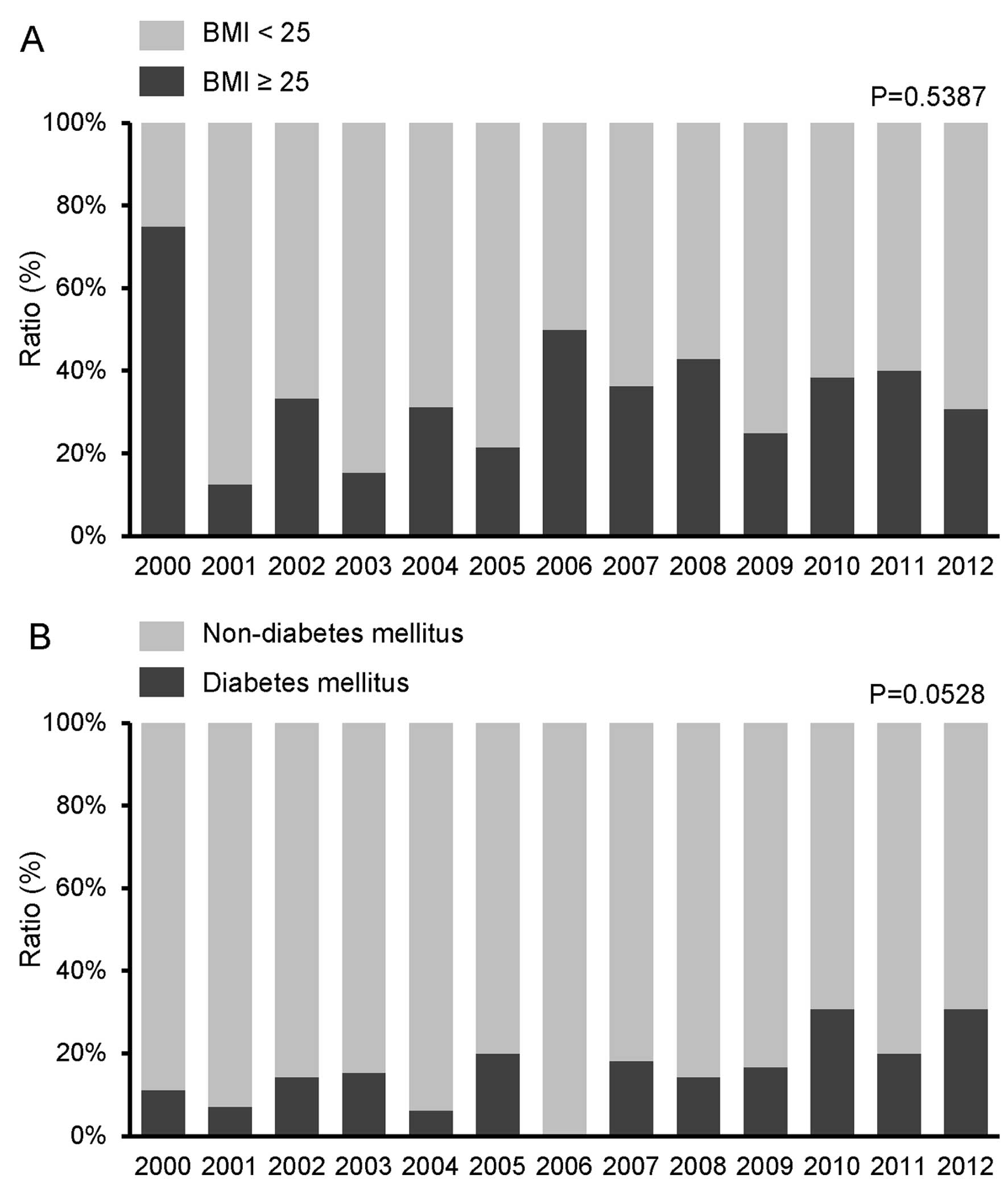
Obesity and diabetes mellitus
No significant change was observed in the proportion
of obese patients (BMI ≥25 kg/m2) during the study
period (P=0.5387) (Fig. 5A).
However, the proportion of patients with diabetes mellitus
exhibited a tendency to increase (P=0.0528) (Fig. 5B).
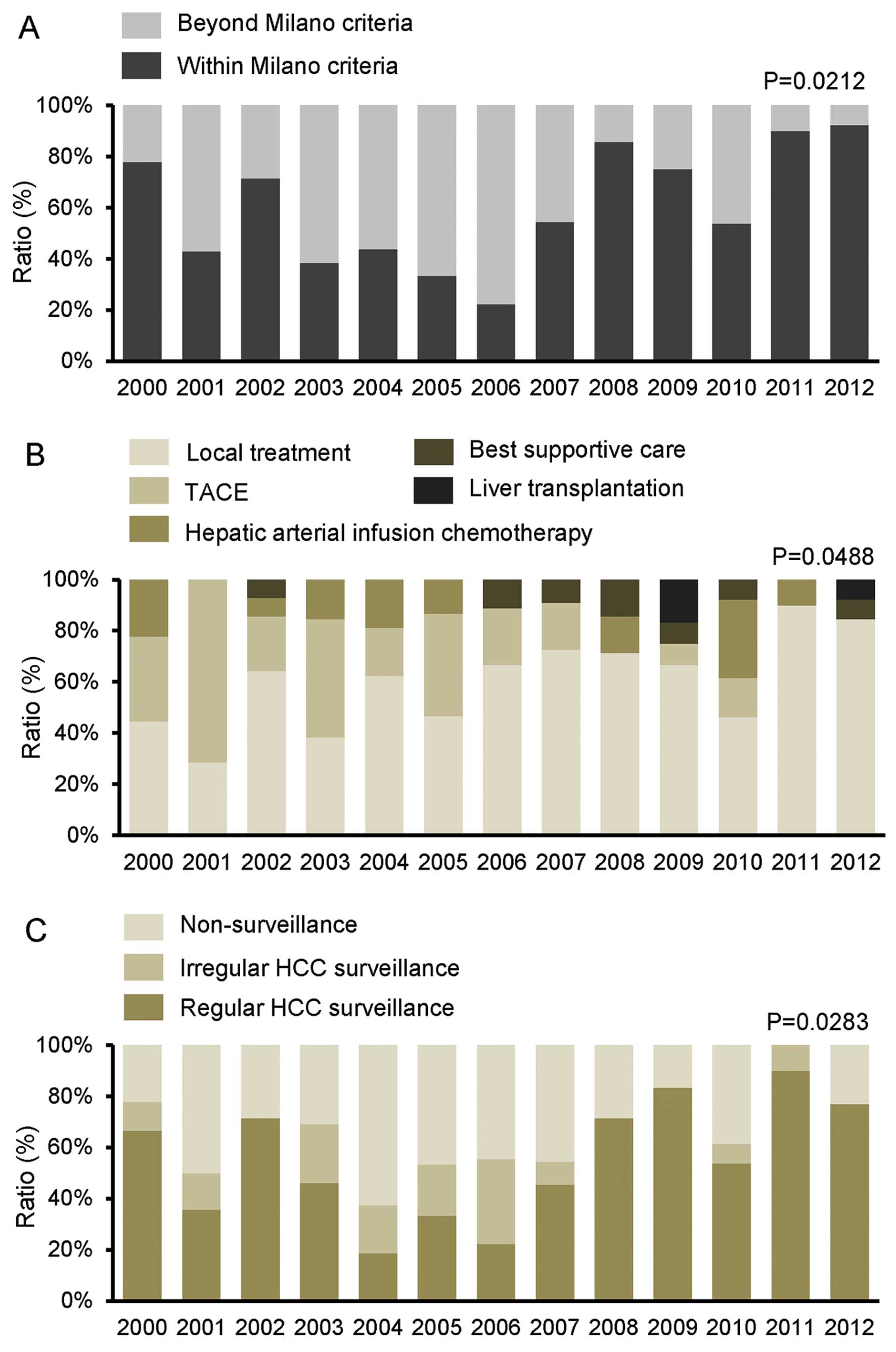
Stage, treatment and surveillance of
HCC
A significant increase was observed in the
proportion of HCC patients who met the Milan criteria during the
study period (P=0.0212) (Fig. 6A).
A significant increase was also observed in the proportion of
patients receiving local treatment during the study period
(P=0.0488) (Fig. 6B). The
proportion of patients who were followed up with regular
surveillance also increased significantly during the study period
(P=0.0283) (Fig. 6C).
Discussion
In this study, we demonstrated that the annual
number of HCC patients with chronic HBV infection did not
significantly decrease, although the patient characteristics were
significantly altered between 2000 and 2012 in Japan. The
proportion of HCC patients in the high-risk group of the HCC
prediction score was significantly decreased, whereas the
proportion of elderly patients and patients with diabetes mellitus
exhibited a tendency to increase. We also demonstrated that the
proportion of HCC patients who met the Milan criteria and those who
received local treatment increased significantly during the study
period.
We observed that the annual number of HCC patients
with chronic HBV infection did not decrease between 1991 and 2012.
We had previously reported that the incidence of HBsAg positivity
among HCC patients did not change in a Japanese cohort study
conducted between 1996 and 2008 (5). The HCC prediction score classifies
the risk of HCC in HBV carriers as low, medium and high risk
(9). We demonstrated that the
proportion of patients at high risk for HCC was significantly
decreased during the study period. The estimation of the HCC
prediction score is based on age, serum albumin level, serum
bilirubin level, HBV DNA level and the presence of liver cirrhosis.
We observed significant decreases for each factor, except for age
and serum bilirubin level, in the proportion of patients who met
the criteria for increased HCC risk. Thus, liver function is
currently better preserved and HBV DNA levels are more efficiently
controlled in HCC patients with chronic HBV infection. Taken
together, these data suggest that, besides HBV-related viral and
hepatic factors, other risk factors may play significant roles in
HCC patients with chronic HBV infection.
Aging, gender and lifestyle are involved in the
development of HCC. In this study, the proportion of male patients
and of patients with a high Brinkman index was unchanged during the
study period and the proportion of habitual drinkers was decreased.
By contrast, the proportion of elderly patients exhibited a
tendency to increase during the study period. It was recently
established that elderly patients with HCV are at higher risk for
HCC and that eradication of HCV exerts a less significant
preventive effect on hepatocarcinogenesis in elderly patients
(15). Moreover, hepatocyte aging,
as assessed by relative nuclear size, was found to be associated
with hepatocarcinogenesis in patients with non-HBV non-HCV
non-alcoholic chronic liver injury (22). Although the mechanisms underlying
age-related hepatocarcinogenesis have not been fully elucidated,
aging is associated with telomere shortening, which in turn results
in chromosomal instability and the inactivation of cell cycle
checkpoints (23,24). In addition, aging is known to
enhance DNA hypermethylation of tumor suppressor genes, which is
associated with the onset of HCC (25). Thus, our findings, along with those
of previous clinical and basic research, suggest that aging may be
an significant factor in HCC patients with chronic HBV
infection.
The proportion of patients with diabetes mellitus
exhibited a tendency to increase during the study period. However,
Chen et al (26) reported
that diabetes mellitus was not found to be a risk factor for HCC in
an HBV- and HCV-endemic area of Southern Taiwan. The reasons for
the discrepancy between our findings and theirs remain unclear;
however, it should be noted that diabetes mellitus was defined only
by the presence of a fasting blood glucose level >126 mg/dl in
the study by Chen et al (26). Since fasting blood glucose levels
are lower in patients with chronic liver disease, owing to the
depletion of hepatic glycogen stores, it is possible that the
number of patients with diabetes mellitus was underestimated in the
study of Chen et al (26).
In HBV carriers, diabetes mellitus was reported to be an
independent risk factor for HCC by large-scale prospective studies
(27,28). Moreover, HCC was shown to be a
major cause of death among patients with diabetes mellitus in Japan
(29). Furthermore, a
characteristic of diabetic patients with chronic liver disease is
hyperinsulinemia (30,31). Insulin is known to bind both
insulin and insulin-like growth factor-1 (IGF-1) receptors and to
activate cell mitogenic and growth pathways (13,32).
Insulin also binds to IGF-binding protein, leading to an increase
in the serum levels of IGF-1 (13,32).
Thus, diabetes mellitus with hyperinsulinemia is considered to
accelerate hepatocarcinogenesis.
We also demonstrated that the proportion of HCC
patients who met the Milan criteria and of those who received local
treatment increased significantly during the study period. Although
this study was not intended to determine the cause for the increase
in early detection rates of HCC and treatment with local therapy,
the sensitivity and accuracy of DCP and lens culinaris
agglutinin-reactive fraction of AFP diagnostic systems have been
improved (33). The diagnostic
ability of magnetic resonance imaging for HCC has significantly
improved through the use of gadolinium ethoxybenzyl
diethylenetriamine pentaacetic acid (34). Hepatic fibrosis and liver function
have also improved after the introduction of nucleot(s)ide
analogues (35,36). Radiofrequency ablation therapy has
supplanted ethanol injection therapy and has allowed for the
treatment of HCCs of greater dimensions (37). In addition, the proportion of
patients who were followed up with regular surveillance increased
significantly during the study period. Surveillance is an important
factor for the early detection of HCC (38,39).
Taken together, these facts suggest that the increase in the rate
of early detection and the treatment with local therapy is likely
due to the recent advances in HCC diagnostic and treatment
methodologies, as well as the improvements in the management of
HBV-infected patients.
In conclusion, we demonstrated that there were
significant alterations in the clinical characteristics of HCC
patients with chronic HBV infection between 2000 and 2012. The
proportion of HCC patients with conventional risk factors, such as
liver cirrhosis and high serum HBV DNA levels, decreased
significantly. By contrast, the proportion of elderly patients and
patients with diabetes mellitus exhibited a tendency to increase.
Moreover, we demonstrated that the proportion of HCC patients who
met the Milan criteria and of those who underwent local treatment
increased significantly during the study period. This field survey
provides important information that may be used when developing
strategies for improving the outcome of HCC patients with chronic
HBV infection in the era of nucleot(s)ide analogue therapy.
Acknowledgements
This study was supported, in part, by a Grant-in-Aid
for Scientific Research (C) (no. 21590865 to M.S.) from the
Ministry of Education, Culture, Sports, Science and Technology of
Japan and by Health and Labour Sciences Research Grants for
Research on Hepatitis from the Ministry of Health, Labour and
Welfare of Japan (H24-Hepatitis-General-007).
Abbreviations:
|
HBV
|
hepatitis B virus
|
|
HCC
|
hepatocellular carcinoma
|
|
HB
|
hepatitis B
|
|
HBsAg
|
HB surface antigen
|
|
BMI
|
body mass index
|
|
WBC
|
white blood cell
|
|
AST
|
aspartate aminotransferase
|
|
ALT
|
alanine aminotransferase
|
|
AFP
|
α-fetoprotein
|
|
DCP
|
des-γ-carboxy prothrombin
|
|
APRI
|
AST-to-platelet ratio index
|
References
|
1
|
El-Serag HB: Epidemiology of viral
hepatitis and hepatocellular carcinoma. Gastroenterology.
142:1264–1273. e12612012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yoshikawa A, Suzuki K, Abe A, et al:
Effect of selective vaccination on a decrease in the rate of
hepatitis B virus-positive Japanese first-time blood donors.
Transfus Med. 19:172–179. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hosaka T, Suzuki F, Kobayashi M, et al:
Long-term entecavir treatment reduces hepatocellular carcinoma
incidence in patients with hepatitis B virus infection. Hepatology.
58:98–107. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Matsumoto A, Tanaka E, Rokuhara A, et al;
Inuyama Hepatitis Study Group. Efficacy of lamivudine for
preventing hepatocellular carcinoma in chronic hepatitis B: A
multicenter retrospective study of 2795 patients. Hepatol Res.
32:173–184. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Taura N, Fukushima N, Yastuhashi H, et al:
The incidence of hepatocellular carcinoma associated with hepatitis
C infection decreased in Kyushu area. Med Sci Monit. 17:PH7–PH11.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
McMahon BJ: The natural history of chronic
hepatitis B virus infection. Hepatology. 49(Suppl 5): S45–S55.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chen CJ, Yang HI, Su J, et al; REVEAL-HBV
Study Group. Risk of hepatocellular carcinoma across a biological
gradient of serum hepatitis B virus DNA level. JAMA. 295:65–73.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kao JH, Chen PJ, Lai MY and Chen DS:
Hepatitis B genotypes correlate with clinical outcomes in patients
with chronic hepatitis B. Gastroenterology. 118:554–559. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wong VW, Chan SL, Mo F, et al: Clinical
scoring system to predict hepatocellular carcinoma in chronic
hepatitis B carriers. J Clin Oncol. 28:1660–1665. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wong GL and Wong VW: Risk prediction of
hepatitis B virus-related hepatocellular carcinoma in the era of
antiviral therapy. World J Gastroenterol. 19:6515–6522. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Purohit V, Rapaka R, Kwon OS and Song BJ:
Roles of alcohol and tobacco exposure in the development of
hepatocellular carcinoma. Life Sci. 92:3–9. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Farrell G: Insulin resistance, obesity and
liver cancer. Clin Gastroenterol Hepatol. 12:117–119. 2014.
View Article : Google Scholar
|
|
13
|
Kawaguchi T, Izumi N, Charlton MR and Sata
M: Branched-chain amino acids as pharmacological nutrients in
chronic liver disease. Hepatology. 54:1063–1070. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kawaguchi T, Kakuma T, Yatsuhashi H, et
al: Data mining reveals complex interactions of risk factors and
clinical feature profiling associated with the staging of
non-hepatitis B virus/non-hepatitis C virus-related hepatocellular
carcinoma. Hepatol Res. 41:564–571. 2011. View Article : Google Scholar
|
|
15
|
Asahina Y, Tsuchiya K, Tamaki N, et al:
Effect of aging on risk for hepatocellular carcinoma in chronic
hepatitis C virus infection. Hepatology. 52:518–527. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yamada S, Kawaguchi A, Kawaguchi T, et al:
Serum albumin level is a notable profiling factor for non-B, non-C
hepatitis virus-related hepatocellular carcinoma: A data-mining
analysis. Hepatol Res. Jul 2–2013.(Epub ahead of print). View Article : Google Scholar
|
|
17
|
Kawaguchi T, Shiba N, Maeda T, et al:
Hybrid training of voluntary and electrical muscle contractions
reduces steatosis, insulin resistance, and IL-6 levels in patients
with NAFLD: a pilot study. J Gastroenterol. 46:746–757. 2011.
View Article : Google Scholar
|
|
18
|
Kudo M, Izumi N, Kokudo N, et al; HCC
Expert Panel of Japan Society of Hepatology. Management of
hepatocellular carcinoma in Japan: Consensus-Based Clinical
Practice Guidelines proposed by the Japan Society of Hepatology
(JSH) 2010 updated version. Dig Dis. 29:339–364. 2011. View Article : Google Scholar
|
|
19
|
Kawaguchi T, Ide T, Taniguchi E, et al:
Clearance of HCV improves insulin resistance, beta-cell function,
and hepatic expression of insulin receptor substrate 1 and 2. Am J
Gastroenterol. 102:570–576. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wai CT, Greenson JK, Fontana RJ, et al: A
simple noninvasive index can predict both significant fibrosis and
cirrhosis in patients with chronic hepatitis C. Hepatology.
38:518–526. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Seino Y, Nanjo K, Tajima N, et al: Report
of the Committee on the classification and diagnostic criteria of
diabetes mellitus. Diabetol Int. 1:2–20. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Nakajima T, Nakashima T, Yamaoka J, et al:
Greater age and hepatocellular aging are independent risk factors
for hepatocellular carcinoma arising from non-B non-C non-alcoholic
chronic liver disease. Pathol Int. 61:572–576. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Plentz RR, Schlegelberger B, Flemming P,
et al: Telomere shortening correlates with increasing aneuploidy of
chromosome 8 in human hepatocellular carcinoma. Hepatology.
42:522–526. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Plentz RR, Park YN, Lechel A, et al:
Telomere shortening and inactivation of cell cycle checkpoints
characterize human hepatocarcinogenesis. Hepatology. 45:968–976.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang Y, Cheng J, Xu C, et al: Quantitative
methylation analysis reveals gender and age differences in p16INK4a
hypermethylation in hepatitis B virus-related hepatocellular
carcinoma. Liver Int. 32:420–428. 2012.PubMed/NCBI
|
|
26
|
Chen CT, Chen JY, Wang JH, et al: Diabetes
mellitus, metabolic syndrome and obesity are not significant risk
factors for hepatocellular carcinoma in an HBV- and HCV-endemic
area of Southern Taiwan. Kaohsiung J Med Sci. 29:451–459. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gao C, Zhao HC, Li JT and Yao SK: Diabetes
mellitus and hepatocellular carcinoma: comparison of Chinese
patients with and without HBV-related cirrhosis. World J
Gastroenterol. 16:4467–4475. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chen CL, Yang HI, Yang WS, et al:
Metabolic factors and risk of hepatocellular carcinoma by chronic
hepatitis B/C infection: a follow-up study in Taiwan.
Gastroenterology. 135:111–121. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hotta N, Nakamura J, Iwamoto Y, Ohno Y,
Kasuga M, Kikkawa R and Toyota T: Causes of death in Japanese
diabetics: A questionnaire survey of 18,385 diabetics over a
10-year period. J Diabetes Investig. 1:66–76. 2010.PubMed/NCBI
|
|
30
|
Eslam M, Aparcero R, Kawaguchi T, Del
Campo JA, Sata M, Khattab MA and Romero-Gomez M: Meta-analysis:
insulin resistance and sustained virological response in hepatitis
C. Aliment Pharmacol Ther. 34:297–305. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kawaguchi T, Yoshida T, Harada M, et al:
Hepatitis C virus down-regulates insulin receptor substrates 1 and
2 through up-regulation of suppressor of cytokine signaling 3. Am J
Pathol. 165:1499–1508. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Calle EE and Kaaks R: Overweight, obesity
and cancer: epidemiological evidence and proposed mechanisms. Nat
Rev Cancer. 4:579–591. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kobayashi M, Hosaka T, Ikeda K, et al:
Highly sensitive AFP-L3% assay is useful for predicting recurrence
of hepatocellular carcinoma after curative treatment pre- and
postoperatively. Hepatol Res. 41:1036–1045. 2011.
|
|
34
|
Inoue T, Kudo M, Komuta M, et al:
Assessment of Gd-EOB-DTPA-enhanced MRI for HCC and dysplastic
nodules and comparison of detection sensitivity versus MDCT. J
Gastroenterol. 47:1036–1047. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Koga H, Ide T, Oho K, et al: Lamivudine
treatment-related morphological changes of esophageal varices in
patients with liver cirrhosis. Hepatol Res. 37:503–509. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chang TT, Liaw YF, Wu SS, et al: Long-term
entecavir therapy results in the reversal of fibrosis/cirrhosis and
continued histological improvement in patients with chronic
hepatitis B. Hepatology. 52:886–893. 2010. View Article : Google Scholar
|
|
37
|
Tateishi R, Shiina S, Teratani T, et al:
Percutaneous radiofrequency ablation for hepatocellular carcinoma.
An analysis of 1000 cases. Cancer. 103:1201–1209. 2005.PubMed/NCBI
|
|
38
|
Ando E, Kuromatsu R, Tanaka M, et al:
Surveillance program for early detection of hepatocellular
carcinoma in Japan: results of specialized department of liver
disease. J Clin Gastroenterol. 40:942–948. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Nakano M, Ando E, Kuromatsu R, et al:
Recent progress in the management of hepatocellular carcinoma
detected during a surveillance program in Japan. Hepatol Res.
40:989–996. 2010. View Article : Google Scholar
|