Introduction
The ureter is a rare location of metastasis,
irrespective of the primary cancer lesion (1). The most common malignant tumors
metastasizing to the ureter are breast cancer and stomach cancer,
whereas colon, cervix and rectum cancers also metastasize to the
ureter with an appreciable frequency (1). However, ureteral metastasis from
prostate cancer is extremely rare (2). The present case study reported such an
incidence of a patient presenting hydronephrosis secondary to
ureteral metastasis of prostate cancer.
Case report
A 63-year-old man presented with asymptomatic right
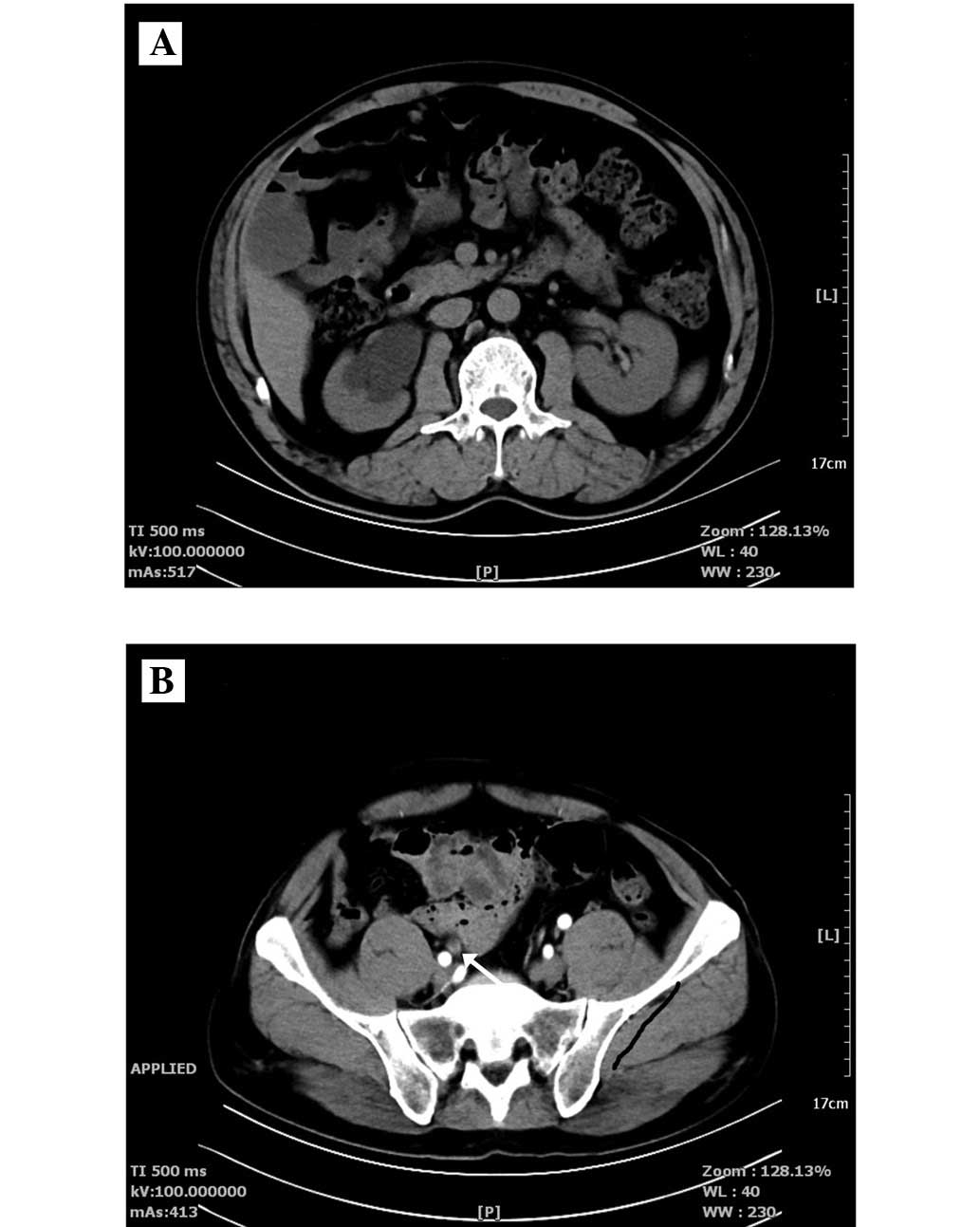
hydronephrosis, detected by ultrasound in our department. Computed
tomography urography (CTU; SOMATOM® Definition Flash, Siemens
Healthcare, Erlangen, Germany) demonstrated right hydronephrosis, a
dilated middle-upper ureter secondary to thickening of the distal
ureter (Fig. 1), and benign prostatic
hyperplasia (BPH). The result of the urine analysis was negative
for hematuria. The serum prostate specific antigen (PSA)
concentration was 111.400 ng/ml. A digital rectal examination
revealed an enlarged and stony hard prostate gland, and subsequent
prostate needle biopsy revealed prostate adenocarcinoma, with a
Gleason score of 4+5=9. Renal dynamic scintigraphy revealed that
the glomerular filtration rate was only 10.56 ml/min on the right
side. Fluorescence in situ hybridization of the exfoliated
cells in the urine did not reveal any evidence of malignancy.
On the basis of the results mentioned above,
ureteroscopy was performed to determine whether the lesion of the
distal ureter was transitional cell carcinoma (TCC) or metastasis
of prostate cancer. The bladder wall and the right ureteral orifice
were thickened and stiff. The ureteroscopy was hard to pass the
stricture of the right distal ureter, thus rendering it impossible
to obtain any biopsy result. Considering the higher degree of
malignancy of TCC and the poor function of the right kidney, a
nephroureterectomy was performed. Following surgical excision, the
tissue was immediately placed in 4% formaldehyde solution prior to
paraffin embedding. Serial sections (4 µm thickness) were obtained
and stained with hematoxylin and eosin and 3,3′-diaminobenzidine
for immunohistochemical staining. The histology results
demonstrated a metastatic prostatic adenocarcinoma of the ureter.
Immunohistochemical staining revealed that the PSA and P504 were
positive. Combined androgen blockade therapy with bicalutamide (50
mg, once daily) and goserelin (3.6 mg, once a month) was then
administered to the patient. At 3 months of follow-up, the
patient's PSA levels had decreased to 0.322 ng/ml; at 6 months of
follow-up, the PSA levels had further decreased to 0.136 ng/ml.
Discussion
The most common metastatic sites of prostate cancer
are the lymph nodes and bone. The lung, bladder, liver and adrenal
gland are other sites where metastasis occurs comparatively
commonly. By contrast, ureteral metastasis of prostate cancer
rarely occurs. In 1999, a total of 38 cases of ureteral metastases
of prostate cancer were collected and reviewed by Haddad (2). Since then, several novel cases have been
reported over the last 10 years (3–7). Among
these cases, the most commonly reported symptom of ureteral
metastasis is flank pain (15–50%) due to ureteral obstruction.
Hematuria is not often identified. This may be due to the fact that
the majority of ureteral tumors from distant primary sites are made
by metastases beneath the mucosa, or they invade from surrounding
tissues of the ureter. In the present case study, the patient had
no subjective symptoms. CTU, retrograde pyelography and
ureteroscopy may be useful for differential diagnosis in patients
with prostate cancer who present with urinary obstruction
symptoms.
The most common malignant tumors metastasizing to
the ureter are breast cancer and stomach cancer (1), whereas colon, cervix, and rectum cancers
also metastasize to the ureter relatively commonly. However,
ureteral metastasis from prostate cancer is a rare occurrence. It
often arises as a consequence of direct invasion of a prostate
cancer or compression by lymphadenopathy. In the present case
study, the patient's prostate cancer had most likely been caused by
direct invasion, since the bladder wall and the right ureteral
orifice were thickened and stiffened, as observed during
ureteroscopy.
Hydronephrosis associated with ureteral
stenosis/obstruction may be an early indicator of when the ureter
is involved in prostatic cancer metastasis. Benign lesions, such as
BPH and stones, should be taken into consideration first of all for
differential diagnosis. In the present case, the possibility of
metastatic prostate cancer would have been considered when evidence
arose which indicated a malignant origin. However, the ureteroscopy
proved hard to pass the stricture of the distal ureter, and biopsy
results were not obtainable. Considering the higher degree of
malignancy of TCC and the poor function of the right kidney, a
nephroureterectomy was performed. A pathological examination
revealed metastatic prostate adenocarcinoma.
In conclusion, the present case study details an
unusual first presentation of prostate cancer without subjective
symptoms. Metastatic lesions to the ureter due to prostate cancer
occur very infrequently. Prostate cancer should be considered in
the differential diagnosis of elderly men with lesions in the
ureter, where a malignant origin is suspected. CTU, retrograde
pyelography and ureteroscopy may be useful for differential
diagnosis.
Acknowledgements
This study was supported by the National Natural
Science Foundation of China (no. 81101937).
References
|
1
|
Fitch WP, Robinson JR and Radwin HW:
Metastatic carcinoma of the ureter. Arch Surg. 111:874–876. 1976.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Haddad FS: Metastases to the ureter.
Review of the world literature and three new case reports. J Med
Liban. 47:265–271. 1999.PubMed/NCBI
|
|
3
|
Jung JY, Kim HK, Roh YT, Choi DY, Yoo TK
and Kim EK: Long-standing ureteral metastasis secondary to
adenocarcinoma of the prostate after bilateral orchiectomy. J Urol.
164:1298–1299. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chalasani V, Macek P, O'Neill GF and
Barret W: Ureteric stricture secondary to unusual extension of
prostatic adenocarcinoma. Can J Urol. 17:5031–5034. 2010.PubMed/NCBI
|
|
5
|
Schneider S, Popp D, Denzinger S and Otto
W: A rare location of metastasis from prostate cancer:
Hydronephrosis associated with ureteral metastasis. Adv Urol.
2012:6560232012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jallad S, Turo R, Kimuli M, Smith J and
Jain S: Ureteric stricture: An unusual presentation of metastatic
prostate adenocarcinoma. Ann R Coll Surg Engl. 94:e213–e214. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Huang TB, Yan Y, Liu H, Che JP, Wang GC,
Liu M, Zheng JH and Yao XD: Metastatic prostate adenocarcinoma
posing as urothelial carcinoma of the right ureter: A case report
and literature review. Case Rep Urol. 2014:2308522014.PubMed/NCBI
|