Introduction
For the majority of patients with early breast
cancer, adjuvant systemic therapy is recommended following primary
surgery to reduce the risk of breast cancer recurrence and to
increase the likelihood of a cure. Approximately 70% of breast
cancers express estrogen receptor (ER), and ER status is a powerful
predictor of response to therapies that inhibit estrogen synthesis
or block the action of its receptor (1). Endocrine therapies are established in
the adjuvant setting (2–4). It is important to distinguish patients
with ER-positive tumors at high risk for recurrence who require
additional chemotherapy, from those for whom adjuvant endocrine
therapy alone may suffice, as the economic burden and toxicities of
chemotherapy must be minimized (5).
Multi-gene assays are strong candidate tools for predicting the
risk of recurrence in ER-positive patients (6). However, classification using multi-gene
expression analyses is not appropriate for everyday practice.
According to the St. Gallen Consensus Conference held in 2013, the
intrinsic subtype affects the indication for adjuvant chemotherapy
and surrogate definitions of subtype may be obtained by
immunohistochemistry (IHC) of ER, progesterone receptor (PgR), Ki67
and human epidermal growth factor receptor 2 (HER2) (7).
For practical purposes, in order to reliably
distinguish between ‘luminal A’ (more endocrine-sensitive, more
indolent and better prognosis) and ‘luminal B (HER2-negative)’
(less endocrine-sensitive, more aggressive and worse prognosis)
breast cancer subtypes, Ki67 may be used as a proliferative index
in addition to ER and PgR status. At the St. Gallen Consensus
Conference, the majority of the expert panel voted that a threshold
of ≥20% should be defined as ‘high’ Ki-67 status (7). The cut-off value of Ki67 for high
proliferation remains unclear.
Breast cancers expressing high levels of Ki67, which
is a nuclear marker of cell proliferation, are associated with
worse outcomes (8–10). However, a standard operating procedure
has not been established, and the inter-laboratory and inter-study
comparabilities of Ki67 are limited (11–13).
Therefore, laboratory-specific procedures and cut-off values must
be examined in order to use Ki67 as an appropriate prognostic
marker (7).
Recent studies have demonstrated that abnormalities
of the p53 gene and accumulation of the p53 protein in the nuclei
are prognostic indicators in ER-positive and HER2-negative breast
cancer patients (14–17). Whole-genome analysis identified the
presence of a p53 gene mutation in 12% of luminal A and 32% of
luminal B breast cancers (18).
Therefore, the expression of p53 has been suggested to be useful in
distinguishing between luminal A and B subtypes. However, p53
assessment is not recommended for routine clinical use in breast
cancer.
The present study aimed to determine the clinical
value of Ki67 and p53 as prognostic markers in patients with
ER-positive and HER2-negative breast cancer, in order to help
stratify patients into prognostic subgroups with a better
predictive response to adjuvant treatment.
Patients and methods
Patients
Between February, 2002 and March, 2013, 697
consecutive patients with primary breast cancer underwent curative
surgery at our institution. Among 615 patients with invasive breast
cancer, 85 who received preoperative chemotherapy and 161 with
ER-negative, HER2-negative, or unknown subtypes were excluded from
the analysis. A total of 6 patients with unknown Ki67 labeling
indices and 55 who did not undergo endocrine therapy were also
excluded. Data from 308 patients with a median age of 59.0 years
(range, 26–91 years) and ER-positive/HER2-negative breast cancer,
who were treated with endocrine therapy, were finally analyzed
(Fig. 1). Patients who were
considered to be at high risk according to prevalent breast cancer
guidelines received chemotherapy (19–23). The
follow-up period (median, 57.9 months) was terminated on 31
December, 2013. Demographic and medical data including age, type of
breast surgery and a history of treatment for breast cancer and
endocrine therapy were collected from medical charts. The
institutional review board approved this study (approval no.
H25-98) and waived the requirement for informed consent from
individual patients.
Clinicopathological factors
Clinicopathological factors such as age, tumor size,
lymph node metastasis, nuclear grade, lymphovascular invasion
positivity and PgR positivity, which are established prognostic
factors for breast cancer, were compared between patients assigned
to groups based on Ki67 labeling index cut-offs. Nuclear grade was
determined according to the General Rules for Clinical and
Pathological Recording of Breast Cancer, 16th edition (24). ER and PgR positivity was assessed by
IHC and scored according to the Allred system (25). HER2 positivity was defined as 3+ by
IHC or 2+ by gene amplification using fluorescent in situ
hybridization (FISH) >2.0.
The surgical specimens were stained using mouse
monoclonal anti-Ki67 antibody (MIB-1; M7240; dilution 1:80; Dako,
Glostrup, Denmark) and mouse DO-7 anti-p53 antibody (DO-7; dilution
1:800; cat. no. NCL-L-p53-DO7; Leica-Novocastra Laboratories Ltd.,
Newcastle upon Tyne, UK). Areas of dense staining were selected
under a microscope, and >500 cancer cells were assessed to
determine the levels of Ki67 expression. Ki67 immunoreactivity was
recorded as a continuous variable based on the proportion of
positive tumor cells (0–100%), regardless of staining intensity.
Cells with nuclear p53 immunostaining were defined as positive.
When <10 or ≥10% of tumor cells expressed p53, the specimens
were defined as negative or positive, respectively, for p53
expression (26).
Follow-up
All the patients were followed up from the day of
surgery onwards. Follow-up care plans included regular physical
examinations and annual mammograms. Recurrence was defined as any
unequivocal occurrence of new cancer foci in a hitherto
disease-free patient. The site of the first cancer recurrence and
the interval between surgery and recurrence were determined. The
recurrence-free interval (RFI) was calculated as the elapsed time
between the date of surgery and that of the first confirmation of
cancer recurrence or the last clinical contact attesting to
recurrence-free status. Overall survival (OS) was defined as the
interval from the day of surgery until death from any cause.
Statistical analysis
Data are presented as numbers (%) or as means unless
otherwise stated. Frequencies were compared using the χ2 test for
categorical variables, and small samples were assessed using the
Fisher's exact test. The patient population was subdivided
according to the Ki67 labeling index cut-offs, and the duration of
RFI was determined using Kaplan-Meier analyses. Differences in RFI
were assessed using the log-rank test. The potential independent
effects of the Ki67 labeling index on RFI and OS were determined by
multivariate analyses using a Cox proportional hazards model that
included variables with p<0.05 in the univariate analyses and
p<0.05 was considered to indicate a statistically significant
difference. Receiver operating characteristic (ROC) curves of the
Ki67 labeling index for the prediction of recurrence were generated
to determine the cut-off that yielded optimal sensitivity and
specificity according to the Youden index. Data were statistically
analyzed using EZR (27), which is a
graphical user interface for R (version 2.13.0; The R Foundation
for Statistical Computing, Vienna, Austria). More precisely, it is
a modified version of R commander (version 1.6–3) that was designed
to add statistical functions frequently used in biostatistics.
Results
Characteristics of patients and
tumors
The clinicopathological characteristics of the 308
patients included in this study are summarized in Table I. The tumors were mainly ductal
(91.6%) or lobular (1.6%) invasive carcinomas. The majority of the
patients had pathological T1-stage tumors, 20 (6.5%) had lymph node
involvement, 248 (80.5%) of the tumors were positive for
lymphovascular invasion, and 257 (83.5%) were PgR-positive on IHC.
Adjuvant chemotherapy had been administered to 86 (27.9%) patients.
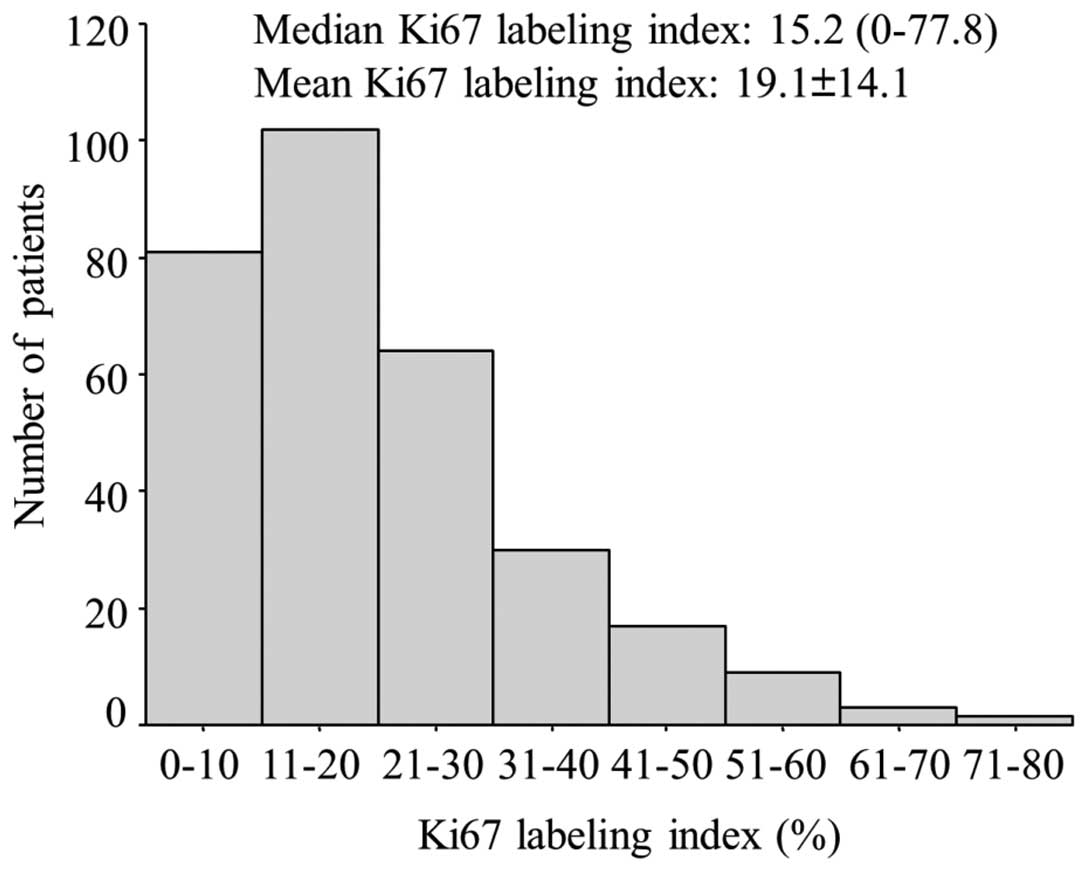
A total of 24 patients developed recurrence and 8 succumbed to the
disease during the follow-up period. the distribution of the
patients according to the Ki67 labeling index, ranging from 0 to
77.8% (median, 15.2%), is shown in Fig.
2.
 | Table I.Patient characteristics (n=308). |
Table I.
Patient characteristics (n=308).
| Characteristics | No. (%) |
|---|
| age, years [median
(range)] | 59.0 (26–91) |
| Histology |
|
| IDC | 282 (91.6) |
| ILC | 5 (1.6) |
|
Others | 21 (6.8) |
| pT stage |
|
| T1 | 226 (73.4) |
| T2 | 67 (21.8) |
| T3 | 1 (0.3) |
| T4 | 14 (4.5) |
| Nodal status |
|
|
Negative | 288 (93.5) |
|
Positive | 20 (6.5) |
| Nuclear grade |
|
| I | 38 (12.3) |
| II | 214 (69.5) |
|
III | 32 (10.4) |
|
Unknown | 24 (7.8) |
| Lymphovascular
invasion |
|
|
Negative | 57 (18.5) |
|
Positive | 248 (80.5) |
|
Unknown | 3 (1.0) |
| Progesterone
receptor status |
|
|
Negative | 50 (16.2) |
|
Positive | 257 (83.5) |
|
Unknown | 1 (0.3) |
| Ki67 labeling
index, % [median (range)] | 15.2
(0.0–77.8) |
| p53 status |
|
|
Positive | 83 (26.9) |
|
Negative | 225 (73.1) |
| Type of
surgery |
|
|
Breast-conserving surgery | 221 (71.8) |
|
Modified radical
mastectomy | 87 (28.2) |
| Endocrine
therapy |
|
|
Tamoxifen | 88 (28.5) |
|
Tamoxifen + Gn-RH agonist | 40 (13.0) |
| Gn-RH
agonist | 3 (1.0) |
|
Anastrozole | 97 (31.5) |
|
Letrozole | 76 (24.7) |
|
Exemestane | 4 (1.3) |
| Chemotherapy | 86 (27.9) |
| Oral
5-FU | 4 (1.3) |
|
Anthracycline | 29 (9.4) |
|
Anthracycline + taxane | 35 (11.4) |
|
CMF | 2 (0.6) |
| TC | 16 (5.2) |
| Recurrence |
|
|
Local | 11 (3.6) |
|
Distant | 13 (4.2) |
| No
event | 284 (92.2) |
| Death | 8 (2.5) |
Univariate and multivariate analyses
of RFI and OS
The variables included in the univariate analysis of
RFI of the 308 patients were age, tumor size, nodal status, nuclear
grade, lymphovascular invasion status, PgR status, Ki67 labeling
index, p53 status and adjuvant chemotherapy. Positive nodal status
and a high Ki67 labeling index were significantly associated with a
short RFI. Moreover, a multivariate analysis that included nodal
status and the Ki67 labeling index, identified positive nodal
status [hazard ratio (HR)=8.92, 95% confidence interval (CI):
3.79–21.0, p<0.001] and a high Ki67 labeling index (HR=1.03, 95%
CI: 1.01–1.06, p=0.004) as independent prognostic factors for RFI
(Table II). Larger tumors, positive
nodal status and a high Ki67 labeling index were significantly
associated with a short OS. A multivariate analysis that included
tumor size, nodal status and Ki67 labeling index identified
positive nodal status (HR=29.5, 95% CI: 4.91–177.0, p<0.001) as
an independent prognostic factor for OS. A high Ki67 labeling index
was marginally associated with OS (HR=1.04, 95% CI: 0.996–1.09,
p=0.074) (Table II).
| Table II.Univariate and multivariate analyses
of recurrence-free interval and overall survival. |
Table II.
Univariate and multivariate analyses
of recurrence-free interval and overall survival.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Recurrence-free
interval |
|
|
|
|
| Age
(years) |
|
|
|
|
|
High | 1.02
(0.984–1.05) | 0.327 |
|
|
| pT
stage |
|
|
|
|
|
pT2,3,4 | 2.04
(0.910–4.57) | 0.084 |
|
|
| Nodal
status |
|
|
|
|
|
Positive | 9.10
(3.88–21.3) | 0.007 | 8.92
(3.79–21.0) | <0.001 |
| Nuclear
grade |
|
|
|
|
|
III | 1.91
(0.640–5.67) | 0.247 |
|
|
|
Lymphovascular invasion |
|
|
|
|
|
Positive | 5.17
(0.697–38.4) | 0.108 |
|
|
|
Progesterone receptor
status |
|
|
|
|
|
Negative | 0.827
(0.367–1.86) | 0.646 |
|
|
| Ki67
labeling index |
|
|
|
|
|
High | 1.03
(1.02–1.05) | 0.003 | 1.03
(1.01–1.06) | 0.004 |
| p53
status |
|
|
|
|
|
Positive | 1.32
(0.576–3.02) | 0.512 |
|
|
|
Chemotherapy |
|
|
|
|
|
Yes | 1.51
(0.647–3.54) | 0.339 |
|
|
| Overall
survival |
|
|
|
|
| Age
(years) |
|
|
|
|
|
High | 1.05
(0.985–1.11) | 0.140 |
|
|
| pT
stage |
|
|
|
|
|
pT2,3,4 | 6.45
(1.29–32.3) | 0.023 | 1.52
(0.257–9.03) | 0.643 |
|
|
| Nodal
status |
|
|
|
|
|
Positive | 40.0
(7.94–201.0) | <0.001 | 29.5
(4.91–177.0) | <0.001 |
| Nuclear
grade |
|
|
|
|
|
III | 4.05
(0.740–22.2) | 0.107 |
|
|
|
Lymphovascular invasion |
|
|
|
|
|
Positive | 27.2
(0.009–84.3) | 0.420 |
|
|
|
Progesterone receptor
status |
|
|
|
|
|
Negative | 0.697
(0.170–2.86) | 0.616 |
|
|
| Ki67
labeling index |
|
|
|
|
|
High | 1.04
(1.01–1.08) | 0.021 | 1.04
(0.996–1.09) | 0.074 |
| p53
status |
|
|
|
|
|
Positive | 2.02
(0.503–8.11) | 0.321 |
|
|
|
Chemotherapy |
|
|
|
|
|
Yes | 3.14
(0.784–12.6) | 0.106 |
|
|
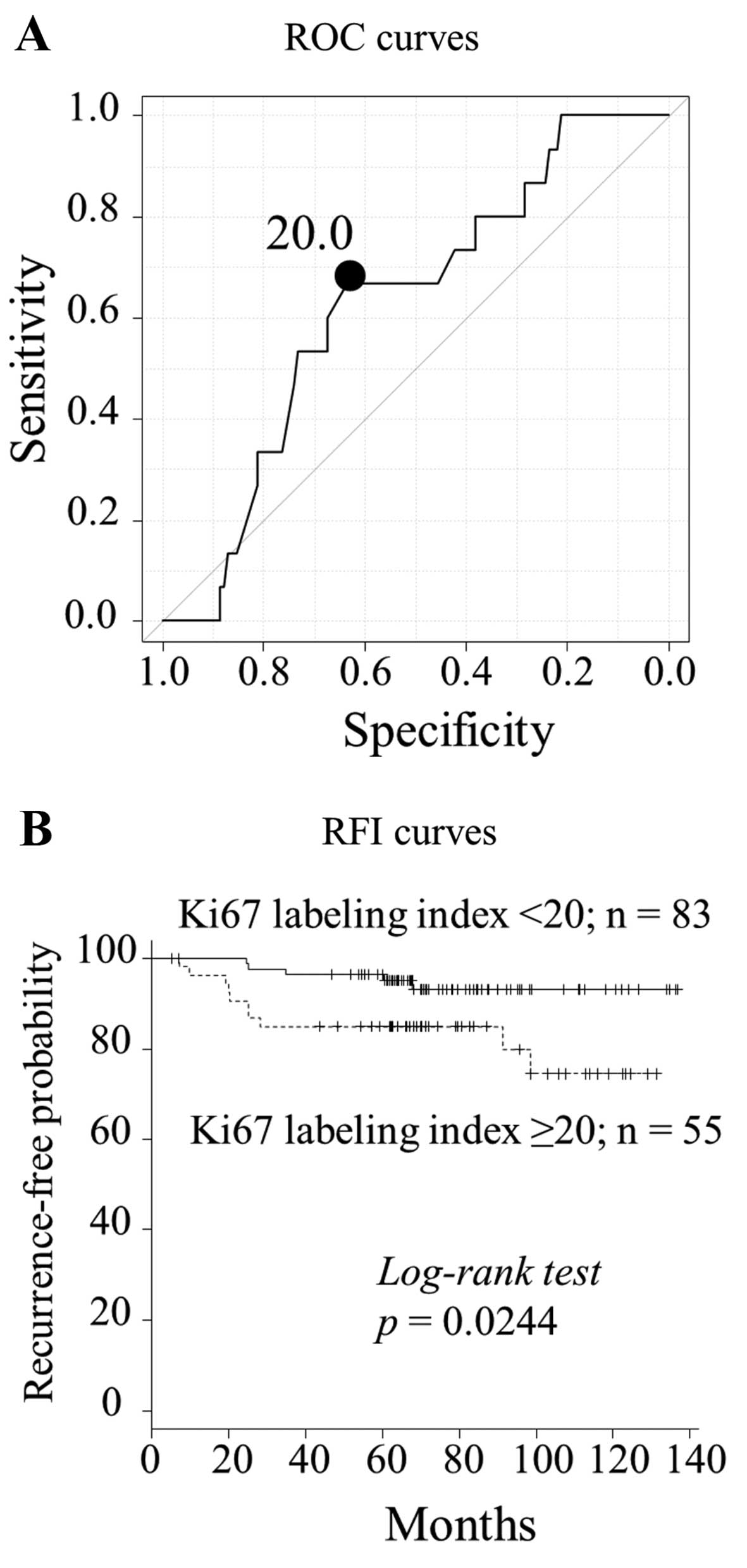
The predictive value of the Ki67 labeling index
should be determined when considering additional chemotherapy
decisions. Therefore, whether Ki67 may be used to determine the
likelihood of a poor prognosis among patients who did not receive
chemotherapy, and who had undergone breast surgery before the Ki67
labeling index was adopted as a breast cancer guideline (18) for implementing decisions regarding
adjuvant therapy. The ROC curve revealed an optimal Ki67 labeling
index cut-off value of 20.0% for predicting recurrence in 138
patients who did not receive adjuvant chemotherapy (area under the
curve = 0.650; sensitivity, 66.7%; specificity, 63.4%) (Fig. 3A).
Comparison of clinicopathological
parameters between Ki67 labeling index <20 and ≥20%
At a cut-off value of 20.0%, a high Ki67 labeling
index was significantly associated with large tumors, lymph node
positivity and p53 positivity (Table
III). The 5-year RFI for patients with Ki67 labeling indices
<20 and ≥20% was 97.2 and 86.6%, respectively (p=0.0244;
Fig. 3B). The univariate analysis
demonstrated that a high Ki67 labeling index (≥20%), lymph node
metastasis and PgR negativity were significantly worse prognostic
factors for RFI (p=0.0333, 0.0116 and 0.0573, respectively)
(Table IV).
| Table III.Comparison of clinicopathological
parameters between Ki67 labeling index <20 and ≥20% in patients
who did not receive chemotherapy (n=138). |
Table III.
Comparison of clinicopathological
parameters between Ki67 labeling index <20 and ≥20% in patients
who did not receive chemotherapy (n=138).
| Variables | Ki67 labeling index
<20% (n=83) | Ki67 labeling index
≥20% (n=55) | P-value |
|---|
| Age, years (median
± SD) | 61.1±13.0 | 62.7±13.1 | 0.497 |
| pT stage, n
(%) |
|
| 0.00420 |
| T1 | 68 (81.9) | 32 (58.2) |
|
| T2, T3,
T4 | 15 (18.1) | 23 (41.8) |
|
| Nodal status, n
(%) |
|
| 0.0236 |
|
Negative | 83 (100) | 51 (92.7) |
|
|
Positive | 0 (0.0) | 4 (7.27) |
|
| Nuclear grade, n
(%) |
|
| 0.739 |
|
I,II | 66 (79.5) | 44 (80.0) |
|
|
III | 5 (6.02) | 5
(9.09) |
|
| Lymphovascular
invasion, n (%) |
|
| 0.296 |
|
Negative | 22 (26.5) | 10 (18.2) |
|
|
Positive | 58 (69.9) | 45 (81.8) |
|
| Progesterone
receptor status, n (%) |
|
| 1.00 |
|
Negative | 16 (19.3) | 11 (20.0) |
|
|
Positive | 68 (81.9) | 44 (80.0) |
|
| p53 status, n
(%) |
|
| <0.001 |
|
Negative | 68 (81.9) | 25 (45.5) |
|
|
Positive | 15 (18.1) | 30 (54.5) |
|
| Table IV.Univariate and multivariate analyses
of the recurrence-free interval in patients who did not receive
chemotherapy (n=138). |
Table IV.
Univariate and multivariate analyses
of the recurrence-free interval in patients who did not receive
chemotherapy (n=138).
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age (years) |
|
|
|
|
|
High | 1.03
(0.985–1.07) | 0.216 |
|
|
| pT stage |
|
|
|
|
|
pT2,3,4 | 1.66
(0.587–4.63) | 0.341 |
|
|
| Nodal status |
|
|
|
|
|
Positive | 6.84
(1.54–30.5) | 0.0116 | 4.12
(0.872–19.5) | 0.0739 |
| Nuclear grade |
|
|
|
|
|
III | 0.868
(0.113–6.68) | 0.892 |
|
|
| Lymphovascular
invasion |
|
|
|
|
|
Positive | 4.10
(0.537–31.3) | 0.174 |
|
|
| Progesterone
receptor status |
|
|
|
|
|
Negative | 2.74
(0.970–7.74) | 0.0573 |
|
|
| Ki67 labeling
index |
|
|
|
|
|
≥20% | 3.22
(1.10–9.43) | 0.0333 | 2.73
(0.892–8.36) | 0.0785 |
| p53 status |
|
|
|
|
|
Positive | 1.05
(0.357–3.06) | 0.935 |
|
|
Discussion
The clinical value of Ki67 and p53 as prognostic
markers in patients with ER-positive and HER2-negative breast
cancer was investigated. The present findings confirmed that Ki67
expression is a prognostic factor for both RFI and OS in patients
with ER-positive and HER2-negative breast cancer. The multivariate
model demonstrated that Ki67 expression remained significant for
RFI, a trend was evident for OS, and these results were consistent
with the majority of published data (10,28).
The predictive value of Ki67 IHC for adjuvant
treatment of ER-positive and HER2-negative breast cancer has not
been investigated in a prospective, randomized study. In the
present study, a cut-off Ki67 labeling index of 20.0% identified
patients with a poor prognosis among those who did not receive
adjuvant chemotherapy. Although this retrospective study included
significant selection bias for adjuvant chemotherapy, the results
indicated that patients with a Ki67 labeling index ≥20.0% should
not be treated with adjuvant endocrine therapy alone. Likewise,
Criscitiello et al (29)
retrospectively analyzed the ability of Ki67 to predict adjuvant
chemotherapy in patients with ER-positive/HER2-negative,
node-positive breast cancer, using propensity scores to minimize
bias related to the non-random assignment of treatment. Their
analysis of Subpopulation Treatment Effect Pattern Plots found that
Ki67 was dichotomous at the 32% level. Certainly, not only the Ki67
labeling index but also nodal status, PgR status and other
prognostic factors, should be considered in the decision regarding
adjuvant treatment (7). Further
prospective validation studies are required to evaluate the
appropriateness of the Ki67 labeling index cut-off value as a
predictive factor.
There is a lack of consensus regarding the use of
the Ki67 labeling index, which results in inconsistencies in
inter-laboratory methodology (11–13). In
particular, the method of assessing Ki67 has been argued. It may be
done by several scoring approaches: Hot-spot scoring, inclusion of
hot spots in general across the section scoring, and by overall
average score across the whole section only. A working party of the
International Ki67 in Breast Cancer Working Group has been
established to assess which method is more robust (30). Although it remains under evaluation,
Honma et al (31) reported
that Ki67 estimation at the ‘hottest spot’ was found to be superior
to that determined by the average score across the whole section as
a predictor of outcome in patients with ER-positive and
HER2-negative breast cancer treated with tamoxifen. In the present
study, hot-spot scoring was used, and it demonstrated the
prognostic significance of the Ki67 labeling index. However,
establishment of an international standard methodology for using
Ki67 is required.
The results of the present study did not reveal a
prognostic significance for p53. The prognostic significance of p53
protein expression in ER-positive and HER2-negative breast cancer
has been reported in a limited number of studies (14–17).
However, several items of information are required for the
interpretation of p53 protein expression. The correlation between
p53 accumulation measured using IHC and p53 mutations detected
using sequencing has been estimated to be <75% in breast cancer
(32). Not all mutations yield a
stable protein, and certain mutations lead to a truncated protein
that cannot be detected using IHC. Done et al (33) demonstrated strong p53 nuclear staining
in all tumors known to harbour missense mutations, but in no tumors
with truncation mutations. Wild-type p53 may also accumulate in
certain tumors as a result of a response to DNA damage or by
binding to other cellular proteins (34). Moreover, at the single-tumor level,
p53 mutations are distributed in a heterogeneous manner (35). It is necessary to collect evidence
regarding p53 accumulation and establish the methodology for
clinical practice. Further studies on p53 as a predictive factor
for late recurrence and adjuvant chemotherapy are required, along
with the findings of previous reports (15,17).
This study's limitations include its retrospective
design at a single institution, the heterogeneity of the
administered treatments, and the short follow-up period.
Nonetheless, a clear statistical significance was identified for
the Ki67 labeling index.
In conclusion, Ki67 was found to be an independent
prognostic factor for patients with ER-positive and HER2-negative
breast cancer, and its cut-off values for making a decision
regarding adjuvant treatment were validated.
Glossary
Abbreviations
Abbreviations:
|
AUC
|
area under the curve
|
|
CI
|
confidence interval
|
|
ER
|
estrogen receptor
|
|
FISH
|
fluorescent in situ
hybridization
|
|
HER2
|
human epidermal growth factor receptor
2
|
|
HR
|
hazard ratio
|
|
IHC
|
immunohistochemistry
|
|
OS
|
overall survival
|
|
PgR
|
progesterone receptor
|
|
RFI
|
recurrence-free interval
|
|
ROC
|
receiver operating characteristic
|
References
|
1
|
Badve S and Nakshatri H:
Oestrogen-receptor-positive breast cancer: Towards bridging
histopathological and molecular classifications. J Clin Pathol.
62:6–12. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hortobagyi GN: Treatment of breast cancer.
N Engl J Med. 339:974–984. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Early Breast Cancer Trialists'
Collaborative Group: Tamoxifen for early breast cancer: An overview
of the randomised trials. Early Breast Cancer Trialists'
Collaborative Group. Lancet. 351:1451–1467. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Mauri D, Pavlidis N, Polyzos NP and
Ioannidis JP: Survival with aromatase inhibitors and inactivators
versus standard hormonal therapy in advanced breast cancer:
Meta-analysis. J Natl Cancer Inst. 98:1285–1291. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cheang MC, Chia SK, Voduc D, Gao D, Leung
S, Snider J, Watson M, Davies S, Bernard PS, Parker JS, et al: Ki67
index, HER2 status, and prognosis of patients with luminal B breast
cancer. J Natl Cancer Inst. 101:736–750. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Azim HA Jr, Michiels S, Zagouri F,
Delaloge S, Filipits M, Namer M, Neven P, Symmans WF, Thompson A,
André F, et al: Utility of prognostic genomic tests in breast
cancer practice: The IMPAKT 2012 Working Group Consensus Statement.
Ann Oncol. 24:647–654. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Goldhirsch A, Winer EP, Coates AS, Gelber
RD, Piccart-Gebhart M, Thürlimann B, Senn HJ, Albain KS, Andre F,
Bergh J, et al: Panel members: Personalizing the treatment of women
with early breast cancer: Highlights of the St. Gallen
International Expert Consensus on the Primary Therapy of Early
Breast Cancer 2013. Ann Oncol. 24:2206–2223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Domagala W, Markiewski M, Harezga B,
Dukowicz A and Osborn M: Prognostic significance of tumor cell
proliferation rate as determined by the MIB-1 antibody in breast
carcinoma: Its relationship with vimentin and p53 protein. Clin
Cancer Res. 2:147–154. 1996.PubMed/NCBI
|
|
9
|
Trihia H, Murray S, Price K, Gelber RD,
Golouh R, Goldhirsch A, Coates AS, Collins J, Castiglione-Gertsch M
and Gusterson BA: International Breast Cancer Study Group: Ki-67
expression in breast carcinoma: Its association with grading
systems, clinical parameters, and other prognostic factors - a
surrogate marker? Cancer. 97:1321–1331. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
de Azambuja E, Cardoso F, de Castro G Jr,
Colozza M, Mano MS, Durbecq V, Sotiriou C, Larsimont D,
Piccart-Gebhart MJ and Paesmans M: Ki-67 as prognostic marker in
early breast cancer: A meta-analysis of published studies involving
12,155 patients. Br J Cancer. 96:1504–1513. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gnant M, Harbeck N and Thomssen C: St.
Gallen 2011: Summary of the Consensus Discussion. Breast Care
(Basel). 6:136–141. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Untch M, Gerber B, Möbus V, Schneeweiss A,
Thomssen C, von Minckwitz G, Beckmann MW, Blohmer JU, Costa SD,
Diedrich K, et al: Zurich Consensus: Statement of German Experts on
St. Gallen Conference 2011 on Primary Breast Cancer (Zurich 2011).
Breast Care (Basel). 6:144–152. 2011. View Article : Google Scholar
|
|
13
|
Untch M, Gerber B, Harbeck N, Jackisch C,
Marschner N, Möbus V, von Minckwitz G, Loibl S, Beckmann MW,
Blohmer JU, et al: 13th St. Gallen international breast cancer
conference 2013: Primary therapy of early breast cancer evidence,
controversies, consensus - opinion of a German team of experts
(Zurich 2013). Breast Care (Basel). 8:221–229. 2013.PubMed/NCBI
|
|
14
|
Millar EK, Graham PH, McNeil CM, Browne L,
O'Toole SA, Boulghourjian A, Kearsley JH, Papadatos G, Delaney G,
Fox C, et al: Prediction of outcome of early ER+ breast
cancer is improved using a biomarker panel, which includes Ki-67
and p53. Br J Cancer. 105:272–280. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kobayashi T, Iwaya K, Moriya T, Yamasaki
T, Tsuda H, Yamamoto J and Matsubara O: A simple
immunohistochemical panel comprising 2 conventional markers, Ki67
and p53, is a powerful tool for predicting patient outcome in
luminal-type breast cancer. BMC Clin Pathol. 13:52013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Boyle DP, McArt DG, Irwin G,
Wilhelm-Benartzi CS, Lioe TF, Sebastian E, McQuaid S, Hamilton PW,
James JA, Mullan PB, et al: The prognostic significance of the
aberrant extremes of p53 immunophenotypes in breast cancer.
Histopathology. 65:340–352. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yamamoto M, Hosoda M, Nakano K, Jia S,
Hatanaka KC, Takakuwa E, Hatanaka Y, Matsuno Y and Yamashita H: p53
accumulation is a strong predictor of recurrence in estrogen
receptor-positive breast cancer patients treated with aromatase
inhibitors. Cancer Sci. 105:81–88. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cancer Genome Atlas Network: Comprehensive
molecular portraits of human breast tumours. Nature. 490:61–70.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Goldhirsch A, Glick JH, Gelber RD, Coates
AS, Thürlimann B and Senn HJ: Panel members: Meeting highlights:
International Expert Consensus on the primary therapy of early
breast cancer 2005. Ann Oncol. 16:1569–1583. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Goldhirsch A, Wood WC, Gelber RD, Coates
AS, Thürlimann B and Senn HJ: 10th St. Gallen conference: Progress
and promise: Highlights of the International Expert Consensus on
the primary therapy of early breast cancer 2007. Ann Oncol.
18:1133–1144. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Goldhirsch A, Ingle JN, Gelber RD, Coates
AS, Thürlimann B and Senn HJ: Panel members: Thresholds for
therapies: Highlights of the St. Gallen International Expert
Consensus on the primary therapy of early breast cancer 2009. Ann
Oncol. 20:1319–1329. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Goldhirsch A, Wood WC, Coates AS, Gelber
RD, Thürlimann B and Senn HJ: Panel members: Strategies for
subtypes - dealing with the diversity of breast cancer: Highlights
of the St. Gallen International Expert Consensus on the Primary
Therapy of Early Breast Cancer 2011. Ann Oncol. 22:1736–1747. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
National Comprehensive Cancer Network:
Breast Cancer. http://ww.nccn.org/professionals/physician_gls/f_guidelines.asp
|
|
24
|
The Japanese Breast Cancer Society:
General Rules for Clinical and Pathological Recording of Breast
Cancer (16th). Kanehara Shuppan, Tokyo: 2008.
|
|
25
|
Allred DC, Harvey JM, Berardo M and Clark
GM: Prognostic and predictive factors in breast cancer by
immunohistochemical analysis. Mod Pathol. 11:155–168.
1998.PubMed/NCBI
|
|
26
|
Iwaya K, Tsuda H, Hiraide H, Tamaki K,
Tamakuma S, Fukutomi T, Mukai K and Hirohashi S: Nuclear p53
immunoreaction associated with poor prognosis of breast cancer. Jpn
J Cancer Res. 82:835–840. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kanda Y: Investigation of the freely
available easy-to-use software ‘EZR’ for medical statistics. Bone
Marrow Transplant. 48:452–458. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yerushalmi R, Woods R, Ravdin PM, Hayes MM
and Gelmon KA: Ki67 in breast cancer: Prognostic and predictive
potential. Lancet Oncol. 11:174–183. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Criscitiello C, Disalvatore D, De
Laurentiis M, Gelao L, Fumagalli L, Locatelli M, Bagnardi V,
Rotmensz N, Esposito A, Minchella I, et al: High Ki-67 score is
indicative of a greater benefit from adjuvant chemotherapy when
added to endocrine therapy in luminal B HER2 negative and
node-positive breast cancer. Breast. 23:69–75. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dowsett M, Nielsen TO, A'Hern R, Bartlett
J, Coombes RC, Cuzick J, Ellis M, Henry NL, Hugh JC, Lively T, et
al: International Ki-67 in Breast Cancer Working Group: Assessment
of Ki67 in breast cancer: Recommendations from the International
Ki67 in Breast Cancer Working Group. J Natl Cancer Inst.
103:1656–1664. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Honma N, Horii R, Iwase T, Saji S, Younes
M, Ito Y and Akiyama F: Ki-67 evaluation at the hottest spot
predicts clinical outcome of patients with hormone
receptor-positive/HER2-negative breast cancer treated with adjuvant
tamoxifen monotherapy. Breast Cancer. 22:71–78. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Norberg T, Lennerstrand J, Inganäs M and
Bergh J: Comparison between p53 protein measurements using the
luminometric immunoassay and immunohistochemistry with detection of
p53 gene mutations using cDNA sequencing in human breast tumors.
Int J Cancer. 79:376–383. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Done SJ, Arneson CR, Ozçelik H, Redston M
and Andrulis IL: p53 protein accumulation in non-invasive lesions
surrounding p53 mutation positive invasive breast cancers. Breast
Cancer Res Treat. 65:111–118. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lacroix M, Toillon RA and Leclercq G: p53
and breast cancer, an update. Endocr Relat Cancer. 13:293–325.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Geisler S, Lønning PE, Aas T, Johnsen H,
Fluge O, Haugen DF, Lillehaug JR, Akslen LA and Børresen-Dale AL:
Influence of TP53 gene alterations and c-erbB-2 expression on the
response to treatment with doxorubicin in locally advanced breast
cancer. Cancer Res. 61:2505–2512. 2001.PubMed/NCBI
|