Introduction
Prostate cancer is the most frequently diagnosed
cancer and the second leading cause of cancer-related death in the
United States (1–4). In Japan, prostate cancer is estimated
to be the most frequently diagnosed cancer and sixth highest cause
of cancer-related death in the male population (5).
Cabazitaxel is a next-generation taxane that is
indicated for the treatment of patients with metastatic
castration-resistant prostate cancer (mCRPC) previously treated
with a docetaxel-containing regimen (6–8). The
phase III TROPIC study revealed that cabazitaxel provided an
overall survival (OS) benefit in patients with mCRPC progressing
during or after docetaxel. In a phase I study of cabazitaxel in
Japanese patients with mCRPC, the safety and antitumor activity
based on prostate-specific antigen (PSA) response rate in Japanese
patients were found to be similar to the results of previous
studies in Caucasian patients. Cabazitaxel was approved worldwide
for the treatment of patients with mCRPC previously treated with a
docetaxel-containing regimen (9–12).
However, the prognostic or predictive biomarker regarding OS have
not yet been fully characterized.
The aim of the present study was to investigate
prognostic biomarkers in patients treated with cabazitaxel in
Japanese mCRPC patients.
Patients and methods
Patients
In this retrospective observational study, 45
patients with mCRPC treated with cabazitaxel at Keio University
Hospital from 2014 to 2017 were identified. All patients were
histologically confirmed as having adenocarcinoma of the prostate
with clinical or radiologic evidence of metastatic disease and had
disease progression during treatment consisting of complete
androgen blockade hormone therapy and docetaxel. All patients
received cabazitaxel at 20–25 mg/m2 administered
intravenously every 3–4 weeks, together with prednisone 5 mg twice
daily. Prophylactic administration of granulocyte-colony
stimulating factor was prescribed to all patients.
For this study, clinico-pathologic and laboratory
data for each patient were obtained retrospectively from medical
records. These data were collected to examine the clinical
association with progression-free survival (PFS) and OS. PFS was
defined as an increase in PSA values ≥25% relative to the
pretreatment PSA value or radiologic progression according to the
Response Evaluation Criteria In Solid Tumors (RECIST) guidelines.
OS was calculated from the date of the start of cabazitaxel
treatment to the date of death or date of last follow-up. Adverse
events were classified in accordance with the Common Terminology
Criteria for Adverse Events (CTCAE) dictionary version 4.0.
Our study was designed as a retrospective analysis,
and approval was obtained from the Institutional Review Board of
our institution.
Statistical analysis
The continuous variables and categorical variables
of different groups were compared using the chi-square test and
Mann-Whitney U test, respectively. The Kaplan-Meier method was used
to estimate the event-time distributions for PFS and OS, and the
log-rank test was then used to assess significance. Univariate Cox
regression models were used to adjust for potential confounders in
predicting OS. Covariates with significant P-values (<0.05) in
univariate analysis were included in the multivariable analysis.
Categorized variables were assessed in multivariate models using
Cox proportional hazard regression models with a stepwise forward
selection method. For all statistical analyses, tests were
two-sided and P<0.05 was considered to indicate statistical
significance. All statistical analyses were performed using the
Statistical Package of the Social Sciences, version 24.0 (SPSS,
Chicago, IL, USA).
Results
Patient characteristics
A summary of the characteristics of the 45 mCRPC
patients in this study is shown in Table
I. Median age was 71 years. The Eastern Cooperative Oncology
Group performance status (ECOG PS) score was 0 and 1/2 in 87.8 and
12.2% of patients, respectively. The median baseline PSA level was
124.3 ng/ml (range, 0.17–11,660). Major sites of disease included
bone (97.8%). The median number of prior docetaxel cycles was 8
(range, 3–43). Cabazitaxel was applied as the second- or third-line
treatment in 11 (7.3%) patients and as fourth-line treatment or
more in 34 (75.6%) patients. Treatment was generally well
tolerated, with a median of 5 cycles (range, 1–26).
 | Table I.Characteristics of patients treated
with cabazitaxel. |
Table I.
Characteristics of patients treated
with cabazitaxel.
| Characteristic | Value (N=45) |
|---|
| Age, years, median
(range) | 71 (46–85) |
| Age group, n (%) |
|
| <75
years | 37 (85.4) |
|
75-years | 8 (14.6) |
| ECOG PS, n (%) |
|
| 0 | 38 (87.8) |
| 1, 2 | 7 (12.2) |
| PSA at baseline,
ng/ml, median (range) | 124.3
(0.17–11,660) |
| Sites involved, n
(%) |
|
| Bone | 44 (97.8) |
| Lymph
nodes | 17 (38.6) |
| Visceral
metastasis | 13 (9.1) |
| Prior surgery, n
(%) | 10 (22.7) |
| Prior radiotherapy, n
(%) | 20 (43.2) |
| Prior 2nd AR
targeting lines, n (%) |
|
| ENZA/ABI | 29 (60.9)/22
(48.9) |
| Prior
docetaxel-containing regimens, n (%) |
|
| 1, 2 | 11 (7.3) |
| 3 | 17 (37.8) |
| 4 or
more | 17 (37.8) |
| Total prior docetaxel
cycle, median (range) | 8 (3–43) |
| PSA at baseline,
ng/ml, median (range) | 124.3
(0.17–11,660) |
| Hb at baseline, g/dl,
median (range) | 11.5 (9.2–14.8) |
| AMC at baseline, /µl,
median (range) | 398 (114–941) |
| NLR at baseline,
median (range) | 4.3 (1.2–16.0) |
| ALP at baseline,
IU/l, median (range) | 293 (313–3,146) |
Univariate and multivariate analysis
of overall survival
Median OS from the start of cabazitaxel treatment
was 16.1 months [95% confidence interval (CI) 6.8–25.5] (Fig. 1). PSA decline of >50 or >30%
was observed in 13 (26.1%) and 16 (34.8%) patients, respectively.
Our primary objective was to examine whether the laboratory data or
clinic-pathologic indicators before administering the first cycle
of cabazitaxel had any associations between OS in men with mCRPC
receiving cabazitaxel.
To identify the clinical-biologic parameters
associated with OS in patients treated with cabazitaxel
chemotherapy, univariate and multivariate analyses were performed
using a Cox proportional hazard regression model.
Univariate analysis revealed that poor PS
(P<0.001), visceral metastasis (P=0.036), hemoglobin <11
mg/dl (P<0.001), absolute monocyte count <400/µl (P=0.026),
PSA ≥100 ng/ml prior to cabazitaxel treatment (P=0.002) were
significantly associated with shorter OS (Table II). Multivariate analysis revealed
that PSA ≥100 ng/ml prior to cabazitaxel treatment [hazard ratio
(HR)=4.375; 95% CI 1.755–10.91, P=0.002], visceral metastasis
(HR=2.926; 95% CI 1.196–7.157, P=0.019), and absolute monocyte
count <400/µl (HR=2.955; 95% CI 1.219–7.165, P=0.026) were
independent prognostic indicators for OS.
| Table II.Results of unvariate and multivariate
analysis influencing OS. |
Table II.
Results of unvariate and multivariate
analysis influencing OS.
|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|
|---|
| Variables | No. (%) | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
|
|
|
|
|
| ≤75 | 9 (20) | 0.808 |
|
|
|
|
>75 | 36 (80) |
|
|
|
|
| PS |
|
|
|
|
|
| 1, 2 | 7 (15.6) | <0.001 |
|
|
|
| 0 | 38 (84.4) |
|
|
|
|
| Visceral
metastasis |
|
|
|
|
|
| Yes | 13 (28.9) | 0.036 | 2.926 | 1.196–7.157 | 0.019 |
| No | 32 (71.1) |
|
|
|
|
| PSA (ng/ml) |
|
|
|
|
|
|
>100 | 23 (51.1) | 0.002 | 4.375 | 1.755–10.91 | 0.002 |
| ≤100 | 22 (48.9) |
|
|
|
|
| Hb (mg/dl) |
|
|
|
|
|
| ≤11 | 18 (40) | <0.001 |
|
|
|
|
>11 | 27 (60) |
|
|
|
|
| AMC (/µl) |
|
|
|
|
|
|
<400 | 25 (55.6) | 0.026 | 2.955 | 1.219–7.165 | 0.017 |
| ≥400 | 20 (44.4) |
|
|
|
|
| NLR |
|
|
|
|
|
| ≥4.3 | 23 (51.1) | 0.097 |
|
|
|
|
<4.3 | 22 (48.9) |
|
|
|
|
| ALP (IU/l) |
|
|
|
|
|
|
>350 | 17 (37.8) | 0.268 |
|
|
|
|
≤350 | 28 (62.2) |
|
|
|
|
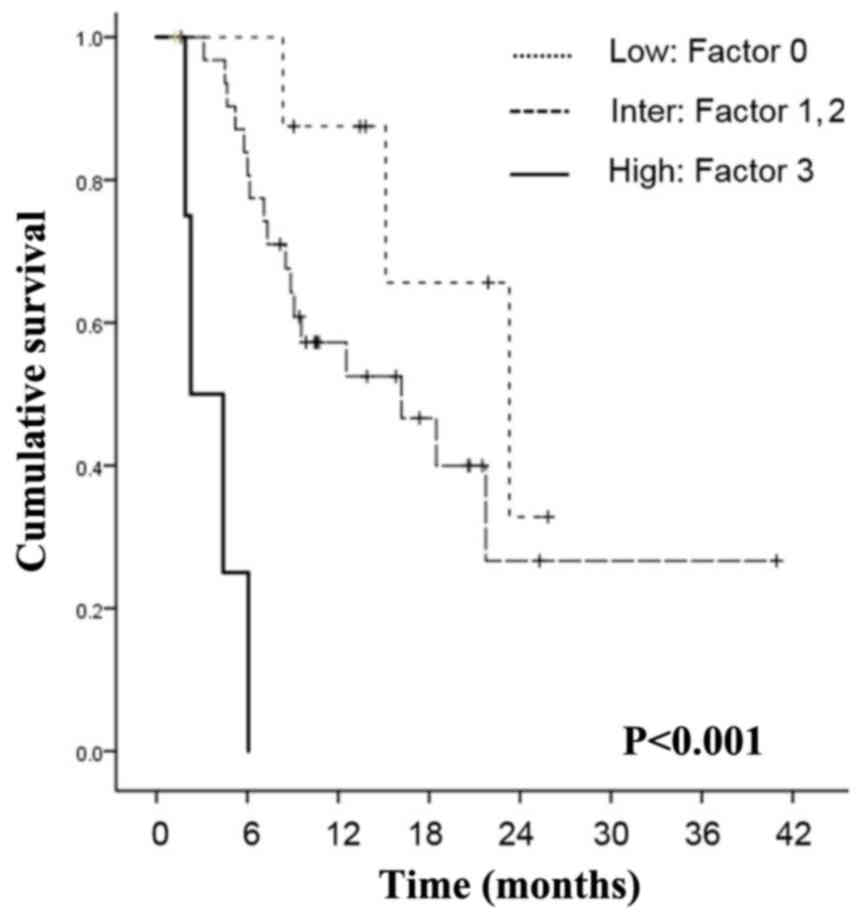
Risk stratification according to three
variables: PSA, visceral metastasis, and absolute monocyte
count
We distributed the patients into three different
groups according to PSA, visceral metastasis, and absolute monocyte
count, which were the three statistically significant variables
found by the multivariate Cox regression analysis (Fig. 2). The relative risk of death was
calculated using the formula, exp (4.375 × PSA + 2.955 × monocyte
count + 2.926 × visceral metastasis) for OS. In this equation the
PSA equaled 1 if the PSA level was >100 ng/ml, and it equaled 0
if the PSA level was ≤100 ng/ml. Absolute monocyte count equaled 1
if the count was <400/µl and 0 if it was ≥400/µl. Visceral
metastasis equaled 1 if visceral metastasis was present and 0 if
there was no metastasis. Based on the relative risk of death,
patients with mCRPC before cabazitaxel therapy were divided into
three risk groups: Low (0 factors, relative risk=1), intermediate
(1 or 2 factors; relative risk=2.926–7.33 for OS), and high (3
factors; relative risk=10.26 for OS). According to the risk
stratification based on prognostic factors, 9 patients (20.0%) were
in the low-risk group, 5 patients (11.1%) were in the high-risk
group, and 31 patients (68.9%) were in the intermediate-risk group.
Median OS from the start of cabazitaxel treatment was 23.3 months
in the low-risk group, 16.1 months in the intermediate-risk group,
and 2.5 months in the high-risk group. The differences among the
groups were significant (P<0.001).
Discussion
A phase I cabazitaxel study in Japan did not
demonstrate efficacy, and the efficacy and prognostic indicators
for cabazitaxel in Japan are still unclear, although cabazitaxel
was the first agent demonstrating a survival benefit in men with
mCRPC progressing during or after docetaxel (6,13,14).
In the PSA era, PSA has played a crucial role in
prostate cancer diagnosis, the definition of castration-resistant
prostate cancer (CRPC), and the introduction of cabazitaxel
indicating the extent of disease progression. It has been reported
that PSA does not necessarily follow the exacerbation of the
disease in the metastatic stage, suggesting that relying only on
PSA changes in mCRPC patients may be misleading to clinicians with
respect to making critical decisions with regard to whether to
continue or change the current treatment (15,16).
However, in this study, univariate and multivariate analysis
revealed PSA ≥100 ng/ml prior to cabazitaxel treatment (P=0.002)
was significantly associated with shorter OS, suggesting the
importance of PSA and the earlier introduction of cabazitaxel
(Table II). Regarding the
prognostic factors for PFS or OS in mCRPC patients treated with
cabazitaxel, a recent paper reported the significance of anemia,
low albumin, alkaline phosphatase level, the burden of bone
metastasis or quantitative evaluation by automated bone scan index
(17–19). A post hoc analysis of the TROPIC
trial and a retrospective analysis have suggested that the
occurrence of severe neutropenia with cabazitaxel was associated
with a prolonged OS (20,21).
There is a growing body of evidence suggesting that
an interactive relationship between hemostatic factors and tumor
biology might play a pivotal role in tumor development and
progression. Monocytes are known to be able to alter the tumor
microenvironment when recruited to tumor sites. An elevated
absolute monocyte count was reported to be an adverse prognostic
factor for hematological malignant diseases. Previous studies
suggested that tumor-associated macrophages detected in tumor sites
were described as a differentiated form of circulating monocytes
outside the vasculature; a monocyte-macrophage lineage. The
association of peripheral monocyte count and prostate cancer
progression is not well characterized. Our recent study in CRPC
patients receiving docetaxel therapy revealed that the elevated
absolute monocyte count was associated with shorter OS (22). Of note, in this study, univariate and
multivariate analysis revealed reduced absolute monocyte count
(P=0.002) were significantly associated with shorter OS (HR=2.955;
95% CI 1.219–7.165, P=0.026), suggesting an inverse immune
microenvironment between the patients treated with docetaxel and
cabazitaxel. As shown in Fig. 2,
significant differences in OS were shown by stratifying the cohort
study by the number of risk factors. To the best of our knowledge,
this is the first study to identify the prognostic value of reduced
absolute monocyte count in patients with mCRPC receiving
cabazitaxel.
The strength of study was the indicated independence
of absolute monocyte count from other prognostic factors, such as
visceral metastasis or high PSA value. In addition, these
prognostic factors can be easily obtained from laboratory test
results and imaging studies, which are conducted routinely before
the assessment of mCRPC with no additional financial burden.
Therefore, adopting monocyte count evaluation into practice may
provide additional information for clinical decision-making.
We acknowledge there were several limitations in our
study. The study design was retrospective and involved a relatively
small population. Therefore, the conclusions of this retrospective
study need to be further explored and validated. A prospective
study based on our study results is warranted to prove whether or
not these predictive factors could be useful in a Japanese clinical
setting.
In conclusion, we identified reduced monocyte count,
as well as PSA ≥100 ng/ml and visceral metastasis, as potential
predictors of worse prognosis during cabazitaxel therapy in
Japanese mCRPC patients. The practical implications of our results
may lead to tailoring of cabazitaxel introduction.
Acknowledgements
Not applicable.
Funding
The present study was supported in part by a
Grant-in-Aid for Scientific Research (grant no. 17K11158 to Takeo
Kosaka) from the Ministry of Education, Culture, Sports, Science,
and Technology of Japan.
Availability of data and materials
The datasets generated and/or analyzed during the
current study are not publicly available due to the lack of ethics
approval for the purpose, but are available from the corresponding
author on reasonable request.
Authors' contributions
TK contributed to the conception, design,
acquisition, analysis and interpretation of data, and drafting of
the manuscript. HH, RM and MO took part in acquisition and analysis
of data. MO took part in interpretation of data and drafting of the
manuscript. All the authors have read and approved the final
version of this manuscript.
Ethics approval and consent to
participate
This study complied with the standards of the
Declaration of Helsinki and the current ethical guidelines, and was
approved by the Institutional Ethics Board of Keio University
Hospital, which exempted obtaining informed consent because our
study design was retrospective and all identifying information was
removed.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of
interest for this study.
References
|
1
|
Negoita S, Feuer EJ, Mariotto A, Cronin
KA, Petkov VI, Hussey SK, Benard V, Henley SJ, Anderson RN, Fedewa
S, et al: Annual Report to the Nation on the Status of Cancer, part
II: Recent changes in prostate cancer trends and disease
characteristics. Cancer. 124:2801–2814. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cronin KA, Lake AJ, Scott S, Sherman RL,
Noone AM, Howlader N, Henley SJ, Anderson RN, Firth AU, Ma J, et
al: Annual Report to the Nation on the Status of Cancer, part I:
National cancer statistics. Cancer. 124:2785–2800. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Akaza H, Onozawa M and Hinotsu S: Prostate
cancer trends in Asia. World J Urol. 35:859–865. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
de Bono JS, Oudard S, Ozguroglu M, Hansen
S, Machiels JP, Kocak I, Gravis G, Bodrogi I, Mackenzie MJ, Shen L,
et al: Prednisone plus cabazitaxel or mitoxantrone for metastatic
castration-resistant prostate cancer progressing after docetaxel
treatment: A randomised open-label trial. Lancet. 376:1147–1154.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mita AC, Denis LJ, Rowinsky EK, Debono JS,
Goetz AD, Ochoa L, Forouzesh B, Beeram M, Patnaik A, Molpus K, et
al: Phase I and pharmacokinetic study of XRP6258 (RPR 116258A), a
novel taxane, administered as a 1-hour infusion every 3 weeks in
patients with advanced solid tumors. Clin Cancer Res. 15:723–730.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pivot X, Koralewski P, Hidalgo JL, Chan A,
Gonçalves A, Schwartsmann G, Assadourian S and Lotz JP: A
multicenter phase II study of XRP6258 administered as a 1-h i.v.
infusion every 3 weeks in taxane-resistant metastatic breast cancer
patients. Ann Oncol. 19:1547–1552. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Pezaro CJ, Omlin AG, Altavilla A, Lorente
D, Ferraldeschi R, Bianchini D, Dearnaley D, Parker C, de Bono JS
and Attard G: Activity of cabazitaxel in castration-resistant
prostate cancer progressing after docetaxel and next-generation
endocrine agents. Eur Urol. 66:459–465. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Al Nakouzi N, Le Moulec S, Albigès L, Wang
C, Beuzeboc P, Gross-Goupil M, de La Motte Rouge T, Guillot A,
Gajda D, Massard C, et al: Cabazitaxel remains active in patients
progressing after docetaxel followed by novel androgen receptor
pathway targeted therapies. Eur Urol. 68:228–235. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kosaka T and Oya M: Hemorrhagic cystitis
in a patient without a past history of radiation therapy who was
treated with cabazitaxel for CRPC. Ann Oncol. 26:2355–2356. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Watanabe K, Kosaka T, Hongo H, Tamaki S
and Oya M: Headache caused by brain metastases of
castration-resistant prostate cancer during cabazitaxel therapy.
Keio J Med. 66:65–71. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mukai H, Takahashi S, Nozawa M, Onozawa Y,
Miyazaki J, Ohno K and Suzuki K: TED 11576 investigators: Phase I
dose-escalation and pharmacokinetic study (TED 11576) of
cabazitaxel in Japanese patients with castration-resistant prostate
cancer. Cancer Chemother Pharmacol. 73:703–710. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nozawa M, Mukai H, Takahashi S, Uemura H,
Kosaka T, Onozawa Y, Miyazaki J, Suzuki K, Okihara K, Arai Y, et
al: Japanese phase I study of cabazitaxel in metastatic
castration-resistant prostate cancer. Int J Clin Oncol.
20:1026–1034. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Armstrong AJ, Garrett-Mayer E, Yang Ou YC,
Carducci MA, Tannock I, de Wit R and Eisenberger M:
Prostate-specific antigen and pain surrogacy analysis in metastatic
hormone-refractory prostate cancer. J Clin Oncol. 25:3965–3970.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Armstrong AJ, Garrett-Mayer E, de Wit R,
Tannock I and Eisenberger M: Prediction of survival following
first-line chemotherapy in men with castration-resistant metastatic
prostate cancer. Clin Cancer Res. 16:203–211. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bando Y, Hinata N, Terakawa T, Furukawa J,
Harada KI, Nakano Y and Fujisawa M: Activity of cabazitaxel in
patients with metastatic castration-resistant prostate cancer after
treatment with single or dual regimens of novel androgen
receptor-targeting agents. Med Oncol. 34:1632017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Belderbos BPS, de Wit R, Hoop EO,
Nieuweboer A, Hamberg P, van Alphen RJ, Bergman A, van der Meer N,
Bins S, Mathijssen RHJ and van Soest RJ: Prognostic factors in men
with metastatic castration-resistant prostate cancer treated with
cabazitaxel. Oncotarget. 8:106468–106474. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Uemura K, Miyoshi Y, Kawahara T, Ryosuke
J, Yamashita D, Yoneyama S, Yokomizo Y, Kobayashi K, Kishida T, Yao
M and Uemura H: Prognostic value of an automated bone scan index
for men with metastatic castration-resistant prostate cancer
treated with cabazitaxel. BMC Cancer. 18:5012018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Meisel A, von Felten S, Vogt DR, Liewen H,
de Wit R, de Bono J, Sartor O and Stenner-Liewen F: Severe
neutropenia during cabazitaxel treatment is associated with
survival benefit in men with metastatic castration-resistant
prostate cancer (mCRPC): A post-hoc analysis of the TROPIC phase
III trial. Eur J Cancer. 56:93–100. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kosaka T, Shinojima T, Morita S and Oya M:
Prognostic significance of grade 3/4 neutropenia in Japanese
prostate cancer patients treated with cabazitaxel. Cancer Sci.
109:1570–1575. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shigeta K, Kosaka T, Kitano S, Yasumizu Y,
Miyazaki Y, Mizuno R, Shinojima T, Kikuchi E, Miyajima A, Tanoguchi
H, et al: High absolute monocyte count predicts poor clinical
outcome in patients with castration-resistant prostate cancer
treated with docetaxel chemotherapy. Ann Surg Oncol. 23:4115–4122.
2016. View Article : Google Scholar : PubMed/NCBI
|