Introduction
Patients with metastatic castration-resistant
prostate cancer (mCRPC) treated with radium-223 have osteoblastic
and/or osteolytic symptomatic/mildly symptomatic bone disease; bone
metastases correlate with increased risk of symptomatic skeletal
adverse events (1). In addition,
such patients generally have a long history of androgen deprivation
therapy and/or steroid therapy [co-administration of which is
recommended, for example, in association with the hormonal agent
abiraterone acetate (2) for
treatment of prostate cancer] that leads to bone weakening and
causes osteoporosis. The association of these two factors with the
presence of metastatic bone lesions elevates the risk of bone
fractures and decreases the time to symptomatic skeletal events
(SSE), defined as the first use of external-beam radiation therapy
to relieve skeletal symptoms, new symptomatic pathologic vertebral
or non-vertebral bone fractures, spinal cord compression, or
tumor-related orthopedic surgical intervention (3). This process negatively affects not only
prognosis quoad vitam but also results in a significant
deterioration in the quality of life (4–6). For
this reason, it is essential to understand which patients are at
higher risk of osteoporosis and to provide, where possible,
adequate therapy with a bisphosphonate or anti-RANKL antibody and
calcium/vitamin D supplementation to prevent or treat the
osteoporotic process (7–9).
Case report
M.G.C., an 84-year-old man, had received a biopsy
diagnosis of prostate adenocarcinoma, with a Gleason Score of 7
(4+3) in 2005 at the age of 72 and was treated with an exclusive
external radiation therapy to the prostate gland (total dose=76 Gy
in 38 fractions) and monthly hormonal therapy with leuprorelin
(Enantone®) 3.75 mg. In his remote clinical history,
there was a right eye enucleation for a non-specific uveitis
process in 1948, a coronary angioplasty for a cardiologic pathology
in 1998, hypercholesterolemia and hepatitis B virus-related chronic
liver disease. In 2011 he underwent brachytherapy on the prostate
gland (total dose=23 Gy) for a local relapse documented by biopsy
and external radiation therapy to pelvic lymph nodes (total
dose=58.8 Gy in 28 fractions), and bicalutamide was added to his
androgen deprivation therapy. At the end of 2016, elevation of
prostate-specific antigen (PSA) level and a technetium-99m bone
scintigraphy (99mTc-BS) documented progression of bone disease with
the appearance of multiple bone metastasis to the skull, the spine,
to the ribs bilaterally and to the pelvis (Fig. 1A and B). There was no evidence of
visceral metastases and/or lymphadenopathy greater than 3 cm at
restaging computed tomography.
The patient, who also reported pain in the spine,
particularly the cervical spine [Numeric Rating Scale (NRS)=3], was
then scheduled for alpha-emitting therapy and from 21 December 2016
to 11 May 2017 he underwent six administrations of intravenous
radium-223, with good clinical tolerance to therapy. In January
2017, after the first radium-223 cycle, he underwent external
radiation therapy to the cervical spine, with good pain response
(NRS from 3 to 0/1). Because of the presence of multi-metastatic
disease and his long history of androgen deprivation therapy, he
was evaluated by a maxillo-facial specialist, who recommended that
zoledronic acid therapy should be started. However, this was
refused by the patient, who also declined supplementation with
calcium and vitamin D. During the six administrations of
radium-223, the pains related to the spine gradually decreased
(from 2/3 to 0/1 on a NRS), without the need for any
pharmacological analgesic therapy. There was also a >30%
decrease of alkaline phosphatase (ALP) values, showing an ALP
response to radium-223 therapy (3).
Furthermore, a 99mTc-BS performed one month after
the end of radium-223 treatment showed a slight diffuse decrease of
tracer uptakes on metastatic bones. Only a faint tracer uptake on
L4-L5 appeared, which was attributed to an
inflammatory/osteodegenerative process (Fig. 1C and D). Nevertheless, only two
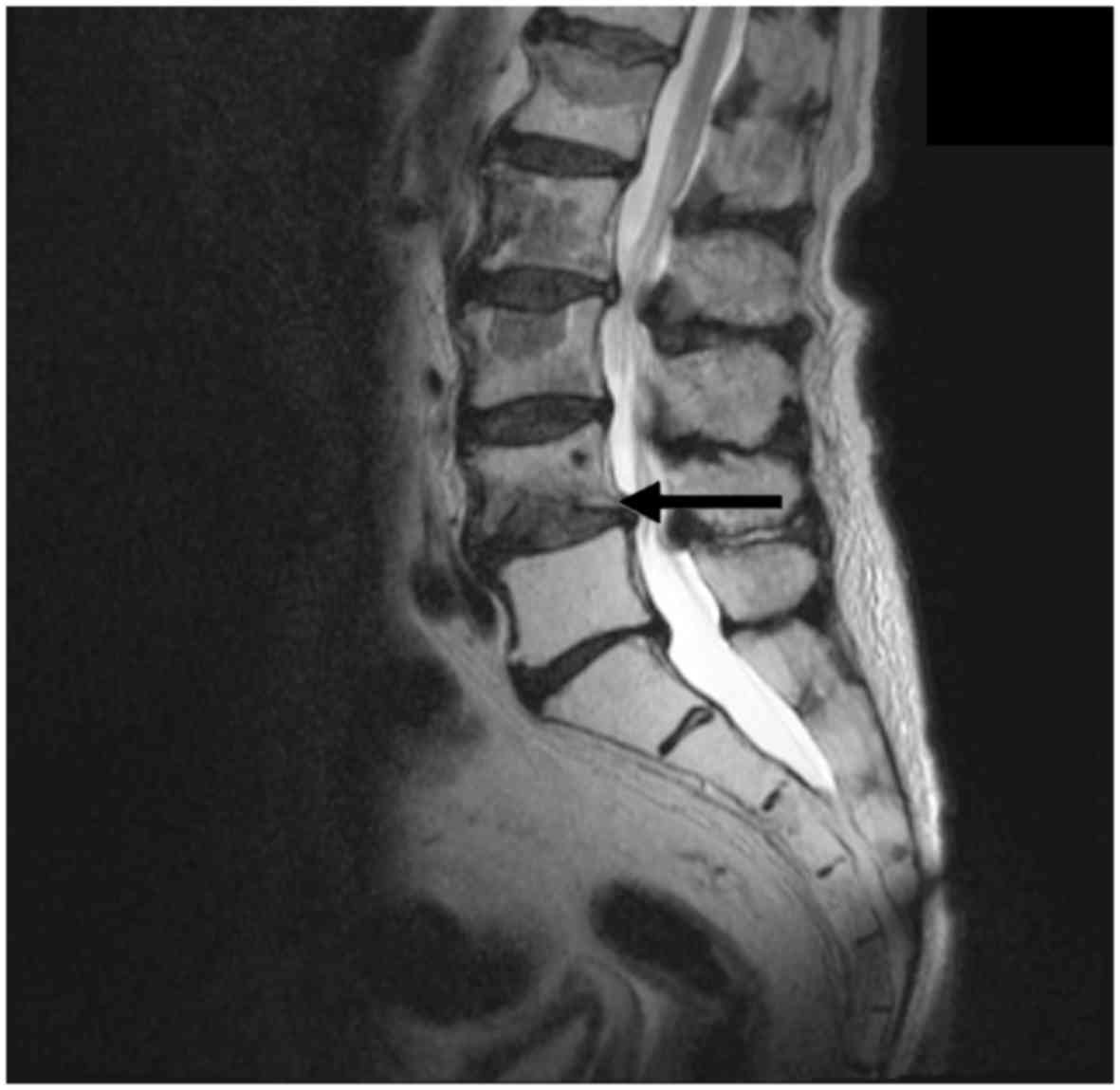
months after the end of treatment, the patient reported the onset
of acute lumbar sciatica (NRS=7/8) partially responsive to
pharmacological analgesic therapy. For this reason, on 14 July
2017, a magnetic resonance imaging (MRI) scan showed a vertebral
crushing on the L4-L5 level with spongiotic bone edema (Fig. 2). A subsequent prostate-specific
membrane antigen-positron emission tomography (PSMA-PET) scan
showed no pathologic tracer uptake on the same vertebral level
(Fig. 3). In August 2017, the
patient, after orthopedic consultation, underwent vertebroplasty on
L4-L5 with a vertebral biopsy that confirmed the absence of
neoplastic bone infiltration. After surgical intervention the
patient had a moderate decrease of the pain (NRS from 7/8 to
5).
One year after the end of radium-223 treatment, the
patient had stable biochemical disease and there was slight uptake
decrease of the metastatic bone lesions at PET-PSMA scan. No other
oncology therapies have been administered.
Discussion
Patients with advanced prostate cancer with skeletal
localizations have an increased risk of developing bone fractures.
This risk is further increased if associated with osteoporosis
induced by prolonged androgen deprivation therapy and/or steroid
therapy (5).
The Alpharadin in Symptomatic Prostate Cancer
Patients (ALSYMPCA) study was a phase 3, randomized, double-blind,
multinational study that compared the efficacy and safety of
radium-223 with that of placebo in patients with CRPC and bone
metastases. The ALSYMPCA trial showed that the time to the first
SSE was significantly prolonged with radium-223 (median, 15.6
months vs. 9.8 months; HR=0.66; P<0.001) (3) and that concomitant bisphosphonate
therapy strongly predicted decreased risk of SSE, including bone
fractures (1). This effect may be as
a result of an additive effect of the two agents in reducing SSE
via independent different mechanisms, but may also be explained by
the bisphosphonate-related inhibition of osteoclasts leading to an
accumulation of inorganic bone matrix that could increase
radium-223 uptake (1,10).
All currently available bisphosphonates are
effective in improving bone mineral density (BMD) compared to
placebo in prostate cancer patients (11) although zoledronic acid has been shown
to be associated with a greater improvement in BMD at all bone
sites assessed (12). Furthermore,
beginning zoledronic acid therapy one month prior to the first
administration of radium-223 may increase the likelihood of pain
palliation and prevent pain flare (13). Parker et al reported an
increase in survival induced by radium-223 therapy in mCRPC, with a
median survival duration of 14.0 months compared with 11.2 months
with placebo (HR: 0.70; P=0.002) (3). The RANK-ligand-inhibitor, denosumab,
has also been shown to improve clinical outcome when administered
concomitantly with radium-223; in the international expanded access
program for radium-223, patients receiving combination treatment
denosumab plus radium-223 show longer survival (median not
available vs. 13 months with radium-223 alone), on the contrary
there wasn't a survival benefit with the bisphosphonates
combination (14). Currently, there
is emerging evidence from post hoc analyses of data from pivotal
phase 3 studies that bisphosphonate therapy in combination with
radium-223 may also increase survival, as well as contributing to
the prevention of SSE (15). For
this reason, it is important to consider beginning bone-targeted
therapies early in patients with multi-metastatic bone prostate
cancer on treatment with alpha-emitting therapy. Because there is
limited information about the prevention of osteoporosis (16–18),
supplementation with calcium and vitamin D in these patients is
also recommended, as in non-oncology patients with osteoporosis
(4,19). Furthermore, early recognition and
differentiation of osteoporotic processes from bone disease
progression becomes crucial in accurately assessing response to
radium-223 therapy and consequently for further therapeutic
decision making. In our case, the patient refused to start
zoledronic acid therapy despite the recommendation of a
maxillo-facial specialist, and two months after the end of
radium-223 therapy he showed a lumbar vertebral crushing that
mimicked bone progression disease at scintigraphy bone scan and
through the clinical manifestation of acute lumbar pain. However,
PSMA-PET and MRI scanning helped us to differentiate neoplastic
from osteoporotic disease (20–24).
This, in association with a stable PSA value and a decreased ALP
value, which was shown to have predictive value in the ALSYMPCA
trial (25,26), directed us to request an orthopedic
opinion which subsequently led to identifying the correct
therapeutic strategy to follow the radium-223 treatment.
In conclusion, patients with CRPC and bone
metastases who are enrolled for radium-223 therapy frequently have
concomitant osteoporotic disease due to prolonged hormone therapy
and/or steroid therapy. The osteoporotic process can increase the
risk of or accelerate the development of symptomatic skeletal
events which lead to considerable morbidity and deterioration in
the quality of life. Furthermore, complications of osteoporosis,
mimicking SSE due to bone progression disease, can interfere with
the response evaluation to alpha-emitting therapy and affect future
therapeutic decisions in patients with metastatic prostate cancer.
For this reason, to limit the osteoporotic process, it is important
to start with bone-targeted therapies such as bisphosphonates or
denosumab, along with adequate prophylactic calcium/vitamin D
supplementation, as soon as possible during radium-223 treatment.
This is particularly important for patients with multi-metastatic
disease and at low risk of mandibular osteonecrosis.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ELR (first author) analyzed clinical and imaging
data of the patient and wrote main part of the article, PG
contributed to analysis, in particular imaging evaluation. RC, CB,
AGM, FM and SF were involved in the clinical management of the
patients and contribute with imaging and other clinical data.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient.
Patient consent for publication
The patient provided written informed consent for
publication of the present study.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
mCRPC
|
metastatic castration-resistant
prostate cancer
|
|
BMD
|
bone mineral density
|
|
ALP
|
alkaline phosphatase
|
|
99mTc-BS
|
technetium-99m bone scintigraphy
|
|
PSMA-PET
|
prostate-specific membrane
antigen-positron emission tomography
|
|
MRI
|
magnetic resonance imaging
|
|
PSA
|
prostate-specific antigen
|
|
SSE
|
symptomatic skeletal event
|
|
NRS
|
Numeric Rating Scale
|
References
|
1
|
Sartor O, Coleman R, Nilsson S, Heinrich
D, Helle SI, O'Sullivan JM, Fosså SD, Chodacki A, Wiechno P, Logue
J, et al: Effect of radium-223 dichloride on symptomatic skeletal
events in patients with castration-resistant prostate cancer and
bone metastases: Results from a phase 3, double-blind, randomised
trial. Lancet Oncol. 15:738–746. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
European Medicines Agency: Zytiga
(abiraterone acetate) Summary of product characteristics.
https://www.ema.europa.eu/en/medicines/human/EPAR/zytigaSeptember
23–2011
|
|
3
|
Parker C, Nilsson S, Heinrich D, Helle SI,
O'Sullivan JM, Fosså SD, Chodacki A, Wiechno P, Logue J, Seke M, et
al: Alpha emitter radium-223 and survival in metastatic prostate
cancer. N Engl J Med. 369:213–223. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rosino-Sánchez A: Preventive management of
bone disease in advanced prostate cancer. Arch Esp Urol.
71:258–266. 2018.(In Spanish). PubMed/NCBI
|
|
5
|
Smith MR: Osteoporosis and other adverse
body composition changes during androgen deprivation therapy for
prostate cancer. Cancer Metastasis Rev. 21:159–166. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Smith MR: Diagnosis and management of
treatment-related osteoporosis in men with prostate carcinoma.
Cancer. 97:789–795. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tanvetyanon T: Physician practices of bone
density testing and drug prescribing to prevent or treat
osteoporosis during androgen deprivation therapy. Cancer.
103:237–241. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Diamond TH, Higano CS, Smith MR, Guise TA
and Singer FR: Osteoporosis in men with prostate carcinoma
receiving androgen-deprivation therapy: Recommendations for
diagnosis and therapies. Cancer. 100:892–899. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Coleman RE and McCloskey EV:
Bisphosphonates in oncology. Bone. 49:71–76. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cha TL, Wu TT, Vogelzang NJ, Huang CY,
Huang SP, Lin CC, Ou YC, Pang ST, Shen DH, Wu WJ and Chang WY:
Optimal usage of radium-223 in metastatic castration-resistant
prostate cancer. J Formos Med Assoc. 116:825–836. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Macherey S, Monsef I, Jahn F, Jordan K,
Yuen KK, Heidenreich A and Skoetz N: Bisphosphonates for advanced
prostate cancer. Cochrane Database Syst Rev.
12:CD0062502017.PubMed/NCBI
|
|
12
|
Poon Y, Pechlivanoglou P, Alibhai SMH,
Naimark D, Hoch JS, Papadimitropoulos E, Hogan ME and Krahn M:
Systematic review and network meta-analysis on the relative
efficacy of osteoporotic medications: Men with prostate cancer on
continuous androgen-deprivation therapy to reduce risk of fragility
fractures. BJU Int. 121:17–28. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yap KKL, Wong W, Ji L, Groshen SG, Quinn
DI, Pinski JK, Bryce AH and Dorff TB: Impact of timing of
administration of bone supportive therapy on pain palliation from
radium-223. J Clin Oncol. 35 (Suppl 15):S50232017. View Article : Google Scholar
|
|
14
|
Saad F, Carles J, Gillessen S, Heidenreich
A, Heinrich D, Gratt J, Lévy J, Miller K, Nilsson S, Petrenciuc O,
et al: Radium-223 and concomitant therapies in patients with
metastatic castration-resistant prostate cancer: An international,
early access, open-label, single-arm phase 3b trial. Lancet Oncol.
17:1306–1316. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Saad F, Sternberg CN, Mulders PFA, Niepel
D and Tombal BF: The role of bisphosphonates or denosumab in light
of the availability of new therapies for prostate cancer. Cancer
Treat Rev. 68:25–37. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Heidenreich A, Bastian PJ, Bellmunt J,
Bolla M, Joniau S, van der Kwast T, Mason M, Matveev V, Wiegel T,
Zattoni F, et al: EAU guidelines on prostate cancer. Part II:
Treatment of advanced, relapsing, and castration-resistant prostate
cancer. Eur Urol. 65:467–479. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Saylor PJ: Bone targeted therapies for the
prevention of skeletal morbidity in men with prostate cancer. Asian
J Androl. 16:341–347. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Morgans AK and Smith MR: Bone-targeted
agents: Preventing skeletal complications in prostate cancer. Uro
Clin North Am. 39:533–546. 2012. View Article : Google Scholar
|
|
19
|
Bilezikian JP: Osteoporosis in men. J Clin
Endocrinol Metab. 84:3431–3434. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Udovicich C, Perera M, Hofman MS, Siva S,
Del Rio A, Murphy DG and Lawrentschuk N:
68Ga-prostate-specific membrane antigen-positron
emission tomography/computed tomography in advanced prostate
cancer: Current state and future trends. Prostate Int. 5:125–129.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
von Eyben FE, Picchio M, von Eyben R, Rhee
H and Bauman G: 68Ga-labeled prostate-specific membrane
antigen ligand positron emission tomography/computed tomography for
prostate cancer: A systematic review and meta-analysis. Eur Urol
Focus. 4:686–693. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Osman OM, Fahmy YR, El-Oraby AM, El-Basmy
AA and Amin YE: Role of diffusion WIs and T2 * GRE pulse sequences
in dubious vertebral marrow pathological lesions. J Egypt Natl Canc
Inst. 19:254–262. 2007.PubMed/NCBI
|
|
23
|
Cicala D, Briganti F, Casale L, Rossi C,
Cagini L, Cesarano E, Brunese L and Giganti M: Atraumatic vertebral
compression fractures: Differential diagnosis between benign
osteoporotic and malignant fractures by MRI. Musculoskelet Surg. 97
(Suppl 2):S169–S179. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Brodowicz T, Hadji P, Niepel D and Diel I:
Early identification and intervention matters: A comprehensive
review of current evidence and recommendations for the monitoring
of bone health in patients with cancer. Cancer Treat Rev. 61:23–34.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sartor O, Coleman RE, Nilsson S, Heinrich
D, Helle SI, O'Sullivan JM, Vogelzang NJ, Bruland Ø, Kobina S,
Wilhelm S, et al: An exploratory analysis of alkaline phosphatase,
lactate dehydrogenase, and prostate-specific antigen dynamics in
the phase 3 ALSYMPCA trial with radium-223. Ann Oncol.
28:1090–1097. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nguyen NC, Shah M, Appleman LJ, Parikh R
and Mountz JM: Radium-223 therapy for patients with metastatic
castrate-resistant prostate cancer: An update on literature with
case presentation. Int J Mol Imaging. 2016:25680312016. View Article : Google Scholar : PubMed/NCBI
|