Introduction
In recent years, combination therapy with nivolumab,
a programmed death 1 (PD-1) immune checkpoint inhibitor antibody,
and ipilimumab, an anti-cytotoxic T-lymphocyte-associated antigen 4
(CTLA-4) antibody, have demonstrated clinical efficacy in the
treatment of metastatic RCC (mRCC) patients (1). These results led to the United State
Food and Drug Administration approving the combination of
ipilimumab and nivolumab in treatment-naïve patients with
intermediate- or poor-risk disease according to the International
Metastatic Renal Cell Carcinoma Database Consortium (IMDC) criteria
in April 2018 (2,3). In Japan, this combination therapy has
also been approved since August 2018. However, it is often
associated with a wide variety of immune-related adverse events
(irAEs) that can affect almost any organ site (1,4).
We herein report a patient with metastatic renal
cell carcinoma who developed the uncommon irAE of aseptic
meningitis as well as isolated ACTH deficiency and liver
dysfunction during ipilimumab and nivolumab therapy.
Case report
A 70-year-old Japanese woman was referred to our
institution for the evaluation of a right renal tumor that had been
detected by abdominal ultrasonography at a screening examination in
July 2018. She had a history of hypertension. She was diagnosed
with right renal cell carcinoma (cT1bN0M0) by computed tomography
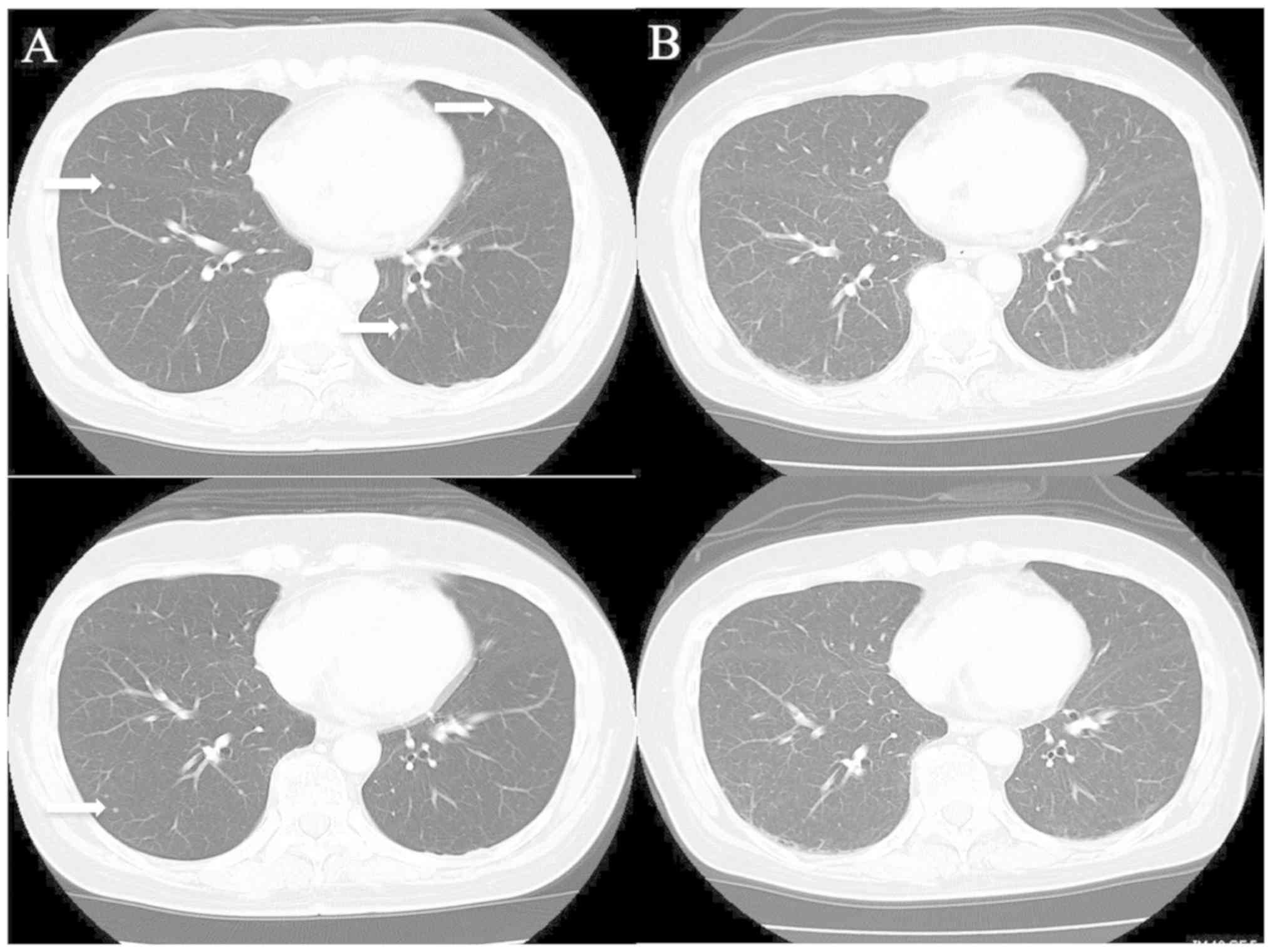
(CT) and underwent right nephrectomy in the same month. Two months
later, multiple lung metastases were observed by CT (Fig. 1A). Therefore, she was diagnosed as
‘intermediate risk’ according to the IMDC criteria [she had one
prognostic factor (<1 year since the diagnosis)].
Combination therapy (once every 3 weeks,
intravenously) of ipilimumab (1 mg/kg) and nivolumab (240 mg/body)
was administered as the first-line therapy in September 2018. On
the 14th day of the 2nd course, she complained of nonspecific
clinical symptoms, such as headaches, dizziness and nausea, and was
admitted to our hospital. However, she did not complain of or
develop any other specific clinical features pertaining to the
central nervous system. She also did not report any neck stiffness.
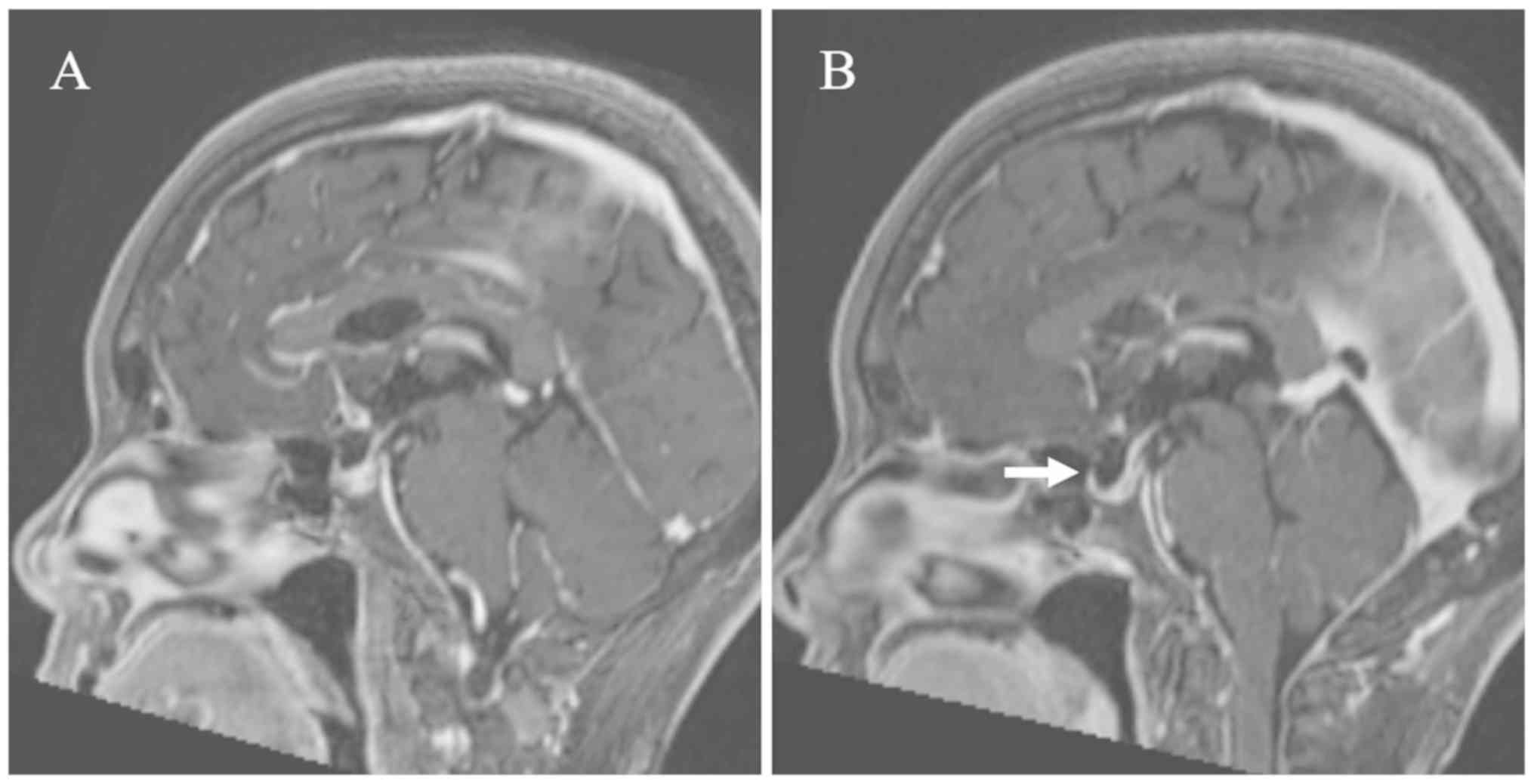
Brain magnetic resonance imaging (MRI) was preformed, but there
were no brain metastases or any findings suggestive of encephalitis
or meningitis (Fig. 2A). However,
meningitis could not be ruled out clinically, so a cerebrospinal
fluid (CSF) test was performed.
The examination of the CSF revealed normal glucose
levels but an elevated protein level at 195 mg/dl and a
significantly elevated white blood cell (WBC) count of
830/mm3 (lymphocytes 825/mm3, neutrophils
5/mm3; Table I). In
addition, CSF cytology showed no malignant cells, and the CSF
analysis was negative for bacteria and viruses (cytomegalovirus,
herpes simplex virus, varicella-zoster virus and human herpes virus
type 6). Based on these results, she was diagnosed with aseptic
meningitis induced by ipilimumab and nivolumab therapy, and
prednisolone (1 mg/kg/day) was started intravenously. After a few
days, her clinical symptoms improved rapidly, as did the CSF
analysis findings, so prednisolone was tapered gradually. On the
49th day of the 2nd course, she had no recurrence of clinical
symptoms on maintenance oral steroid treatment (prednisolone 10
mg/day), and a CSF analysis showed that the WBC count had dropped
to 44/mm3 (only lymphocytes; Table I). After delivering a sufficient
explanation of the risks and benefits to the patient, the 3rd
course of the combination therapy was readministered the next
day.
 | Table I.CSF analysis and blood glucose data of
the case study. |
Table I.
CSF analysis and blood glucose data of
the case study.
| CSF examination | Reference value | C2D14 | C2D23 | C2D49 | C3D10 | C3D25 |
|---|
| Glucose, mg/dl | 45-80 | 46 | 74 | 67 | 66 | 66 |
| Protein, mg/dl | <45 | 195 | 97 | 41 | 52 | 48 |
| WBC,
n/mm3 | <5 | 830 | 217 | 44 | 34 | 53 |
|
Lymphocyte,
n/mm3 | 0 | 825 | 215 | 44 | 34 | 53 |
|
Neutrophil,
n/mm3 | 0 | 5 | 2 | 0 | 0 | 0 |
| Blood glucose,
mg/dl | 73-109 | 106 | – | – | 148 | 141 |
| Blood to CSF glucose
ratio |
| 0.43 | – | – | 0.45 | 0.47 |
Two weeks later, she complained of nausea, anorexia
and fatigue. A relapse of meningitis was suspected, but the CSF
showed that the WBC count was not marked elevated compared to
before (Table I). Although CT was
performed to investigate the cause, no abnormal findings were
found. However, all multiple lung metastases had disappeared, and a
complete response was considered to have been achieved (Fig. 1B). The MRI of the brain showed mild
diffuse enlargement of the pituitary (Fig. 2B). Her laboratory data showed a low
sodium value (122 mmol/l). Based on the clinical symptoms,
examination values and MRI findings, adrenocorticotropic hormone
(ACTH) deficiency was suspected, and the administration of oral
hydrocortisone 20 mg/day (Cortril®; morning 15 mg,
evening 5 mg) was started after stopping prednisolone.
Two days later, her symptoms dramatically improved.
The results of the endocrine system tests revealed that her ACTH
(2.0 pg/ml) and cortisol (1.12 µg/dl) levels were lower than
normal. The levels of other anterior pituitary hormones (prolactin,
luteinizing hormone, follicle-stimulating hormone,
thyroid-stimulating hormone) were not low (Table II). Based on these findings, the
diagnosis was isolated ACTH deficiency induced by combination
therapy of ipilimumab and nivolumab.
| Table II.Patient laboratory data. |
Table II.
Patient laboratory data.
| Laboratory data | Reference value | C3D10 | C3D15 | C3D25 | C3D27 | C3D29 | C3D50 |
|---|
| WBC, n | 3,300-8,600/µl | 11,000 | 9,000 | 9,170 | 8,850 | 19,030 | 16,920 |
| Eosino (%) | 0.4–8.6 | 0.5 | 1.3 | 0.3 | 0.6 | 0.1 | 0.2 |
| AST, U/l | 13-30 | 35 | 50 | 131 | 155 | 69 | 20 |
| ALT, U/l | 10-42 | 41 | 57 | 204 | 244 | 176 | 44 |
| Na, mmol/l | 138-145 | 133 | 122 | 127 | 131 | 134 | – |
| CRP, mg/dl | 0-0.14 | 3.12 | 6.45 | 0.36 | 0.27 | <0.07 | – |
| ACTH, pg/ml | 7.2–63.3 | 15.7 | 2 | <1.5 | – | – | – |
| Cortisol, µg/dl | 6.24–18.0 | 3.18 | 1.12 | 38.1 | – | – | – |
| TSH, µIU/ml | 0.49–4.67 | – | 0.31 | 2.5 | – | – | – |
| F-T4, ng/ml | 0.71–1.85 | – | 0.91 | 0.89 | – | – | – |
| PRL, ng/ml | 4.29–13.69 | – | 60.5 | – | – | – | – |
| LH, mIU/ml | 0.79–5.72 | – | 8.08 | – | – | – | – |
| FSH, mIU/l | 2.00–8.30 | – | 30.54 | – | – | – | – |
On the 25th day of the 3rd course, she complained of
headache and anorexia. The CSF examination showed that the WBC
count had increased again (53/mm3, only lymphocytes),
and her laboratory data showed hepatic dysfunction and elevated
aspartate aminotransferase at 155 U/l and alanine aminotransferase
at 244 U/l (Tables I and II). She had no history of infection with
hepatitis B and C virus, and abdominal echography showed no
remarkable findings in her liver. She was diagnosed with liver
dysfunction and relapse of aseptic meningitis induced by
combination therapy of ipilimumab and nivolumab.
While continuing the administration of oral
hydrocortisone 20 mg/day, the administration of intravenous
prednisolone (total 1 mg/kg/day) was started additionally. The
liver dysfunction and aseptic meningitis gradually improved
(Table II). Three months later, CT
showed that the multiple lung metastases had not reappeared.
However, she had been taking oral hydrocortisone 20 mg/day for
isolated ACTH deficiency and prednisolone 2.5 mg/day for liver
dysfunction. Therefore, the immunotherapy was not restarted.
Discussion
Anti-CTLA-4 antibody and anti-PD-1 antibody have
different working points and mechanisms of activity, and their
combination brings about a synergetic effect on the tumor reduction
effect and overall survival (1,5).
However, the frequency and severity of irAEs is also
synergistically affected. Although the patient backgrounds differed
between these studies, grade 3 or 4 treatment-related AEs occurred
in 18.7% of patients treated with nivolumab alone for mRCC
(6), whereas such AEs occurred in
45.7% of patients treated with nivolumab plus ipilimumab for mRCC
(1). The most frequently reported
irAEs in the RCC population are skin events (59.6% of patients),
endocrine events (40.4% of patients), gastrointestinal events
(44.7% of patients), hepatic events (27.7%), renal events (12.8%)
and pulmonary events (10.6 %) (7).
Neurologic side-effects are rare but include cases of immune
polyneuropathies, Guillain Barré syndrome, myasthenia gravis,
posterior reversible encephalopathy syndrome, aseptic meningitis,
enteric neuropathy, transverse myelitis as well as immune
encephalitis (8). In a pooled
analysis of nearly 1,500 patients with melanoma treated with
ipilimumab, the incidence of neurologic irAEs was 0.1% (9,10).
We herein report a 70-year-old woman with mRCC
receiving combination nivolumab and ipilimumab therapy who
developed aseptic meningitis, isolated ACTH deficiency and hepatic
dysfunction that were probably induced by an auto-immune related
mechanism. As meningitis and encephalitis were suspected based on
clinical symptoms, lumber puncture proved extremely helpful for
making a diagnosis because there were no findings on brain MRI. CSF
abnormalities with an elevated proteins level associated with
lymphocytic pleocytosis supported the presence of
inflammatory-mediated disease. General bacterial meningitis was
initially excluded because of the lymphocyte-dominated findings on
CSF. Tuberculous meningitis has also been reported to have
lymphocyte-dominated findings. However, in modern Japan,
tuberculosis infection itself is so rare that it was not considered
as a differential diagnosis. A CSF analysis was the most useful
examination for supporting the relationship between the aseptic
meningitis status and the response to steroid treatment. Aseptic
meningitis fortunately responded well to high-dose steroid therapy,
and her irAEs also improved to Grade 1 promptly. The early
improvement of the patient's symptoms and CSF analysis findings by
steroid treatment ruled out tuberculous meningitis. There were no
sequelae, and the prednisolone dose was able to be reduced to 10
mg/day within 1 month after the start of steroid therapy.
Whether or not to resume immune checkpoint inhibitor
treatment after neurological recovery is a matter of debate, and a
careful analysis of the risks and benefits should be done on a case
by case basis. The therapeutic effect was a complete response after
only 2 courses. However, the durability of the response to this
combination therapy for mRCC still remains unclear and this
combination immunotherapy is only allowed in the first-line setting
for mRCC in Japan. Steroid treatment therapy for this irAE
foutunately demonstrated a good response, so the combination
therapy was re-administered after both the risks and benefits were
sufficiently explained to the patient. However, isolated ACTH
deficiency occurred with the oral administration of steroids.
Furthermore, relapse of aseptic meningitis and liver dysfunction
also occurred. An autopsy analysis of the pituitary glands of
patients with cancer treated by CTLA-4 blockade described type II
and IV hypersensitivity reactions and a strong CTLA-4 expression in
the pituitary gland (11).
Therefore, this hypophysitis with pituitary enlargement
hypothetically could have been caused by type II hypersensitivity
reactions, such as complement activation and infiltration with
macrophages and phagocytosis, and type IV hypersensitivity
reactions, such as infiltration with autoreactive T lymphocytes.
Although the study was conducted in a melanoma population, it was
reported that approximately 40% of patients with advanced melanoma
who received nivolumab combined with ipilimumab in clinical trials
discontinued treatment because of AEs. However, the efficacy
outcomes seemed similar between patients who discontinued nivolumab
plus ipilimumab treatment because of AEs during the induction phase
and those who did not discontinue the treatment because of AEs
(12). In the present case,
re-administration of nivolumab and ipilimumab therapy occurred not
only other irAEs but also relapse of aseptic meningitis. Therefore,
we decided to resume immunotherapy when the disease progressed.
No standard treatment has yet been defined for
neurological irAEs. A commonly used protocol is oral prednisone at
roughly 1 mg/kg/day. A neurological irAE management algorithm has
been proposed (5,8). However, further studies are necessary
in order to establish the precise framework regarding the dose,
timing of tapering and administration period of steroid treatment.
In the present case, a longer tapering period for steroids might
have been needed in order to prevent recurrent irAEs. Indeed, it
was reported that neurological irAEs are not always reversible
(13), highlighting the importance
of optimizing treatment regimens.
With the increasing use of immune checkpoint
inhibitors in cancer treatment, practicing oncologists need to be
aware of the potential risks of neurologic irAEs and be able to
provide prompt treatment for this uncommon but potentially serious
class of AEs. Treatment algorithms for relatively frequent AEs have
been established, and there are many case reports of relatively
frequent AEs that can be referenced (14,15). The
present case of aseptic meningitis is a rare AE, and the diagnosis
and treatment of such events can be facilitated by the publication
of detailed clinical case reports. Proper testing based on the
careful observation of patients' clinical symptoms and intervention
with steroids will enable the effective treatment at an earlier
point in the clinical course.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
DT, NF and TN participated, conceived and designed
the present case report, analyzed and interpreted the data and
wrote the manuscript. DT, KI, TI and KT evaluated the patient and
participated in therapy. KI and MN evaluated radiological images.
TN and MN supervised the study and critically reviewed the
manuscript. All authors have read and approved the final version of
the manuscript.
Ethics approval and consent to
participate
The present case report was approved by the
Institutional Review Board of National Hospital Organization Kyushu
Cancer Center (approval no. 2014-99). Written informed consent was
obtained from the patient.
Patient consent for publication
The patient provided written informed consent for
the publication of any associated data and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Motzer RJ, Tannir NM, McDermott DF, Arén
Frontera O, Melichar B, Choueiri TK, Plimack ER, Barthélémy P,
Porta C, George S, et al: Nivolumab plus ipilimumab versus
sunitinib in advanced renal-cell carcinoma. N Engl J Med.
378:1277–1290. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Heng DY, Xie W, Regan MM, Warren MA,
Golshayan AR, Sahi C, Eigl BJ, Ruether JD, Cheng T, North S, et al:
Prognostic factors for overall survival in patients with metastatic
renal cell carcinoma treated with vascular endothelial growth
factor-targeted agents: Results from a large, multicenter study. J
Clin Oncol. 27:5794–5799. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Heng DY, Xie W, Regan MM, Harshman LC,
Bjarnason GA, Vaishampayan UN, Mackenzie M, Wood L, Donskov F, Tan
MH, et al: External validation and comparison with other models of
the international metastatic renal-cell carcinoma database
consortium prognostic model: A population-based study. Lancet
Oncol. 14:141–148. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ardolino L and Joshua A: Immune checkpoint
inhibitors in malignancy. Aust Prescr. 42:62–67. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Postow MA, Chesney J, Pavlick AC, Robert
C, Grossmann K, McDermott D, Linette GP, Meyer N, Giguere JK,
Agarwala SS, et al: Nivolumab and ipilimumab versus ipilimumab in
untreated melanoma. N Engl J Med. 372:2006–2017. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Motzer RJ, Escudier B, McDermott DF,
George S, Hammers HJ, Srinivas S, Tykodi SS, Sosman JA, Procopio G,
Plimack ER, et al: Nivolumab versus everolimus in advanced
renal-cell carcinoma. N Engl J Med. 373:1803–1813. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hammers HJ, Plimack ER, Infante JR, Rini
BI, McDermott DF, Lewis LD, Voss MH, Sharma P, Pal SK, Razak ARA,
et al: Safety and efficacy of nivolumab in combination with
ipilimumab in metastatic renal cell carcinoma: The CheckMate 016
study. J Clin Oncol. 35:3851–3858. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hottinger AF: Neurologic complications of
immune checkpoint inhibitors. Curr Opin Neurol. 29:806–812. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tarhini A: Immune-mediated adverse events
associated with ipilimumab ctla-4 blockade therapy: The underlying
mechanisms and clinical management. Scientifica (Cairo).
2013:8575192013.PubMed/NCBI
|
|
10
|
Ibrahim RA, Berman DM, DePril V, Humphrey
RW, Chen T, Messina K M, Chin M, Liu HY, Bielefield M and Hoos A:
Ipilimumab safety profile: Summary of findings from completed
trials in advanced melanoma. J Clin Oncol. 29 (15 Suppl):S85832011.
View Article : Google Scholar
|
|
11
|
Caturegli P, Di Dalmazi G, Lombardi M,
Grosso F, Larman HB, Larman T, Taverna G, Cosottini M and Lupi I:
Hypophysitis secondary to cytotoxic T-lymphocyte-associated protein
4 blockade: Insights into pathogenesis from an autopsy series. Am J
Pathol. 186:3225–3235. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Schadendorf D, Wolchok JD, Hodi FS,
Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ, Cowey CL, Lao
CD, Chesney J, et al: Efficacy and safety outcomes in patients with
advanced melanoma who discontinued treatment with nivolumab and
ipilimumab because of adverse events: A pooled analysis of
randomized phase II and III trials. J Clin Oncol. 35:3807–3814.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Spain L, Walls G, Julve M, O'Meara K,
Schmid T, Kalaitzaki E, Turajlic S, Gore M, Rees J and Larkin J:
Neurotoxicity from immune-checkpoint inhibition in the treatment of
melanoma: A single centre experience and review of the literature.
Ann Oncol. 28:377–385. 2017.PubMed/NCBI
|
|
14
|
National Comprehensive Cancer Network, .
Guidelines on Management of Immune Checkpoint Inhibitor-Related
Toxicities Version 2, 2019. https://www.nccn.org/professionals/physician_gls/pdf/immunotherapy.pdf/Jun
3–2019
|
|
15
|
Brahmer JR, Lacchetti C, Schneider BJ,
Atkins MB, Brassil KJ, Caterino JM, Chau I, Ernstoff MS, Gardner
JM, Ginex P, et al: Management of immune-related adverse events in
patients treated with immune checkpoint inhibitor therapy: American
society of clinical oncology clinical practice guideline. J Clin
Oncol. 36:1714–1768. 2018. View Article : Google Scholar : PubMed/NCBI
|