Introduction
Worldwide, ~1.25 million patients are diagnosed with
colorectal cancer (CRC) and >600,000 CRC-associated mortalities
are reported each year (1). The
likelihood of colorectal cancer diagnosis increases in patients
that are >40 years old; and increases progressively from the age
of 40 years, rising sharply in patients >50 years old. Most
(>90%) cases of colorectal cancer occur in people aged 50 years
or older (2). At least 50% of
patients develop metastases, and the majority of these patients
have unresectable tumors (3). CRC
survival is highly dependent upon the stage of disease at
diagnosis, and typically ranges from a 90% 5-year survival rate for
cancers detected at the localized stage; to a 70% rate for regional
types; to a 10% survival rate for those diagnosed with distant
metastatic cancer (4) In patients
with recurrences, the most frequent sites are the liver, lungs,
local and/or regional retroperitoneal, and peripheral lymph nodes.
However, metastases of colorectal cancer in the kidney are
considered to be extremely rare (5).
In the present study, the case of a 42-year-old male
patient with metastatic sigmoid colon cancer with progression to
the left kidney was reported. In addition, a review of the
literature was performed.
Case report
The study was approved by the ethics committee of
the National Cancer Institute (Vilnuis, Lithuania) and written
informed consent was obtained from the patient prior to publication
of the data. A 42-year-old male patient was admitted to the
National Cancer Institute in December 2009 with left lower quadrant
abdominal pain, obstipation, bloating and weight loss. Following
double-contrast X-ray of the large intestine, a sigmoid tumor
completely obstructing the bowel was diagnosed. The patient
underwent sigmoid resection and partial mesorectal excision of 10×8
cm in size. Sigmoid colorectal carcinoma pT3N0M0 (stage 2)
(6) penetrating the urinary bladder
wall and upper rectum was identified. Subsequently, the patient
received 6 cycles of adjuvant chemotherapy with fluorouracil and
folinic acid (Mayo Clinic regimen) (7). The treatment did not produce any
side-effects. The patient remained without any signs of disease
relapse during follow-up, until February 2013, when he complained
of blood in the urine. A pelvic magnetic resonance imaging scan was
performed, which resulted in the diagnosis of a bladder tumor (a
4×5-cm mass was identified). However, chest and abdominal computed
tomography (CT) scans did not reveal any distant metastases. The
patient underwent transurethral resection of the bladder tumor and
8 cycles of adjuvant chemotherapy with capecitabine (1,250
mg/m2) twice daily, since he refused administration of
intravenous chemotherapy. Histological analysis of the resected
tissue demonstrated metastasis of the mucinous adenocarcinoma in
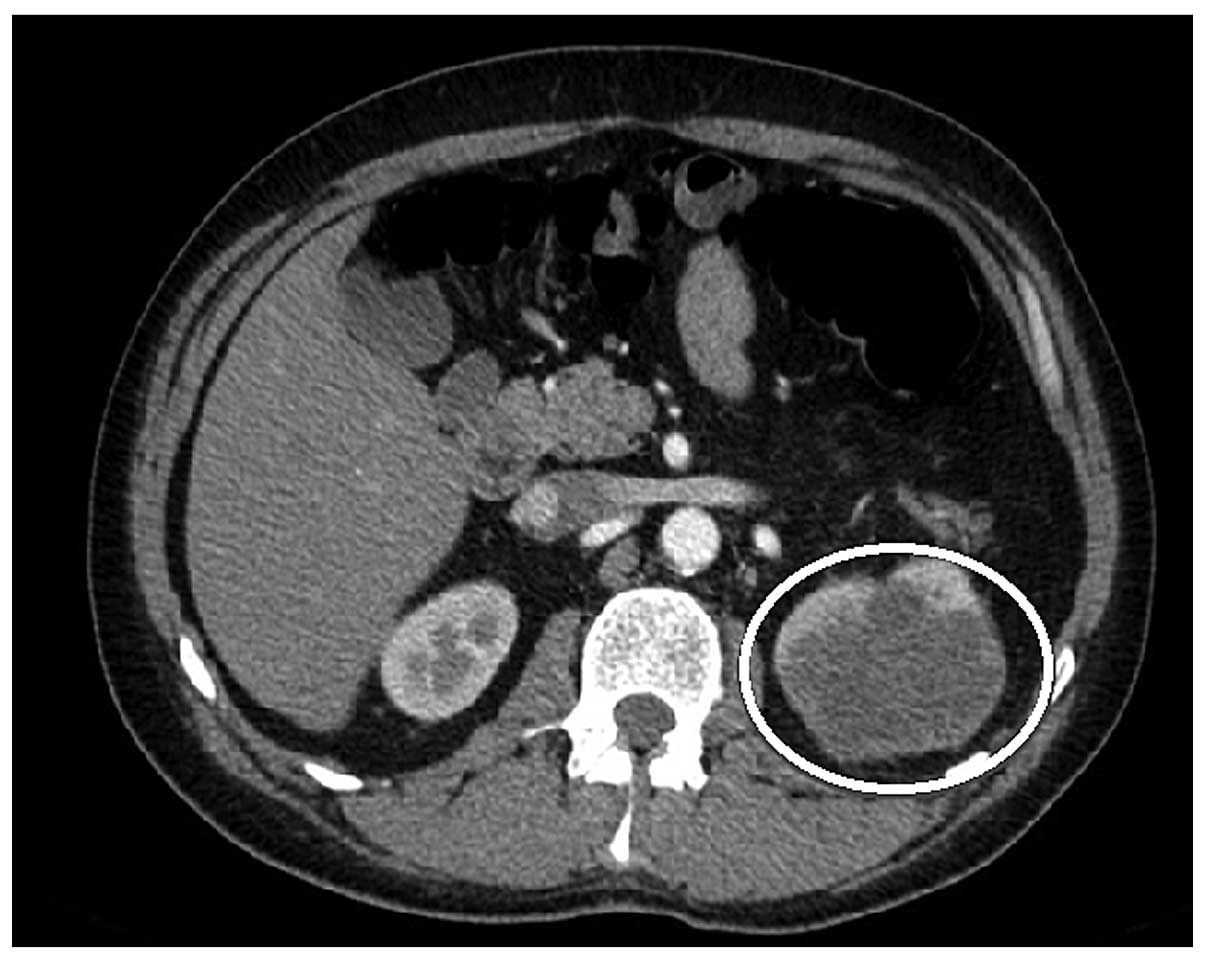
the urinary bladder wall. In October 2013, surveillance imaging
with a CT scan revealed the presence of an 81×66-mm tumor in the
upper pole of the left kidney (Fig.
1). At admission, the physical examination demonstrated no
abnormalities and the laboratory tests were unremarkable, while the
carcinoembryonic antigen (CEA) level was normal. Renal cellular
carcinoma was suspected and the patient underwent biopsy of the
kidney. Histological examination of the kidney biopsy tissue
established a diagnosis of adenocarcinoma, representing a sigmoid
cancer metastasis. During a laparotomy, left nephrectomy was
performed. The nephrectomy sample revealed tumor infiltration of
the perirenal and hilar fat of the renal capsule, with venous
spread. Histologically, a metastasis from the primary large-bowel
adenocarcinoma was diagnosed with KRAS gene mutation. The
patient refused adjuvant chemotherapy. The patient was alive and
remained disease-free 18 months subsequent to the surgery.
Discussion
Isolated metastatic involvement of the kidney is
rare and sporadic, and usually occurs with concomitant
carcinomatosis (5). In the majority
of cases, solitary kidney metastases of CRC are asymptomatic and
detected on surveillance imaging or as a result of increased CEA
levels. Bracken et al performed an autopsy study of 11,328
patients and identified kidney metastases in only 2.7% of patients
with CRC; however, the incidence of solitary metastases has not
been previously reported (8). The
present study utilized a computerized literature search using
MEDLINE, PubMed and the Cochrane library and identified 14 cases of
CRC metastasis to the kidney (5,9–21). The current case is the 15th. In the
current patient, mucinous adenocarcinoma was diagnosed, which
occurs in ~10% of all cases of CRC (22). Pericolic and perirectal dissemination
and metastasis are more common than other types of metastasis, and
these tumors are more aggressive and atypical at presentation
(5).
The current patient initially underwent surgery due
to sigmoid cancer penetrating to the urinary bladder and upper
rectum. However, the patient later developed a metastasis in the
wall of the urinary bladder, and resection of the urinary bladder
was then performed. In October 2013, a metastasis to left kidney
was diagnosed on a CT scan. Therefore, retrograde spread of cancer
cells possibly occurred intraluminally from the urinary bladder to
the kidney in the present case, although no neoplastic infiltration
was observed in the ureter. Previous studies have also proposed
this type of dissemination (12). CRC
is known to metastasize locally or distantly via the lymphatic and
venous systems. In colon carcinoma, the lymphatic flow follows the
major arteries. Tumors located between more than one major vessel
may metastasize in any direction; however, the liver is by far the
most commonly-involved organ. The colon is drained by the portal
venous system, and thus metastases to the brain, spleen and kidney
occur by arterial dissemination (5).
Arterial dissemination is rare in colon cancer, with only 3% of all
colon cancer metastases caused by arterial dissemination (9). Another study stated that perirenal
tissues (Gerota's fascia and peritoneum) are very important in
direct tumor dissemination and the restoration of a normal
anatomical situation is essential (13).
The patient of the present study was asymptomatic
for 4 years after the procedure. Kidney metastasis was only
identified on a CT, without CEA level elevation. A biopsy was
performed to rule out a second primary renocellular cancer.
Systemic chemotherapy is the treatment of choice for CRC renal
metastases and, with the exception of rare emergencies or cases
with resectable disease, nephrectomy is not commonly used in the
management of CRC renal metastases (14,23). Other
relative indications for surgery are tumors with perirenal hematoma
and risk of rupture, as well as symptomatic patients (9). Another treatment option for symptomatic
patients is percutaneous kidney resection (16).
In conclusion, isolated renal metastases of CRC
without any other visceral metastases have rarely been reported in
the worldwide literature. The present study reported one such rare
case of CRC metastasis to the kidney.
References
|
1
|
Ferlay J, Soerjomataram I, Ervik M,
Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D and
Bray F: GLOBOCAN 2012: Estimated Cancer Incidence and Mortality
Worldwide: IARC CancerBase No. 11. Volume 1.0IARC; Lyon, France:
2012
|
|
2
|
National Cancer Institute, . SEER Cancer
Statistics Review, 1975–2005. http://seer.cancer.gov/archive/csr/1975_2005/results_merged/sect_06_colon_rectum.pdfAccessed.
May 10–2015
|
|
3
|
Grothey A, Van Cutsem E, Sobrero A, et al:
Regorafenib monotherapy for previously treated metastatic
colorectal cancer (CORRECT): an international, multicentre,
randomised, placebo-controlled, phase 3 trial. Lancet. 381:303–312.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jemal A, Clegg LX, Ward E, Ries LA, Wu X,
Jamison PM, Wingo PA, Howe HI, Anderson RN and Edwards BK: Annual
report to the nation on the status of cancer, 1975–2001, with a
special feature regarding survival. Cancer. 101:3–27. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Aksu G, Fayda M, Sakar B and Kapran Y:
Colon cancer with isolated metastasis to the kidney at the time of
initial diagnosis. Int J Gastrointest Cancer. 34:73–77. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Greene FL, Page DL, Fleming ID, Fritz AG,
Balch CM, Haller DG and Morrow M: Colon and rectumAJCC Cancer
Staging Manual. 6th. Springer-Verlag; New York, NY, USA:
|
|
7
|
Tomiak A, Vincent M, Kocha W, Taylor M,
Winquist E, Keith B, Sawyer M, Griffeth S, Whiston F and Stitt L:
Standard dose (Mayo regimen) 5-fluorouracil and low dose folinic
acid: prohibitive toxicity? Am J Clin Oncol. 23:94–98. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bracken RB, Chica G, Johnson DE and Luna
M: Secondary renal neoplasms: An autopsy study. South Med J.
72:806–807. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Klaasse Zn, Prabhakar R, Madi R,
Shingleton WB and Terris MK: Bilateral metachronous colon cancer
metastasis to kidneys: a rare case with a treatment dilemma. Uro
Today Int J. 6:1–5. 2012.
|
|
10
|
Wolff JM, Boeckmann W and Jakse G:
Spontaneous kidney rupture due to a metastatic renal tumour. Case
report. Scand J Urol Nephrol. 28:415–417. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Waleczek H, Wente MN and Kozianka J:
Complex pattern of colon cancer recurrence including a kidney
metastasis: A case report. World J Gastroenterol. 11:5571–5572.
2005.PubMed/NCBI
|
|
12
|
Kibar Y, Deveci S, Sümer F and Seçkin B:
Renal papillae metastasis of sigmoid colon adenocarcinoma. Int J
Urol. 12:93–95. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nelson J, Rinard K, Haynes A, Filleur S
and Nelius T: Extraluminal colonic carcinoma invading into kidney:
A case report and review of the literature. ISRN Urol.
2011:7071542011.PubMed/NCBI
|
|
14
|
Dagnoni C, Granero LCS and Rovere RK:
Sigmoid adenocarcinoma with renal metastasis. Clin Pract.
1:e882011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Komeya M, Nakaigawa N, Sano F, Kagota M,
Murakami T, Makiyama K, Miyoshi Y, Ogawa T, Uemura H, Yao M, et al:
A case of upper urinary tract metastases from sigmoid colon cancer.
Hinyokika Kiyo. 55:339–343. 2009.(In Japanese). PubMed/NCBI
|
|
16
|
Milbank AJ, Savage SJ, Angermeier KW, Ng
CS and Streem SB: Metastatic cancer to the renal pelvis: A novel
approach to management. Urology. 64:807–809. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Brambilla E, Heck AA, Cao JG, Toniazzo GT
and Petteffi L: Isolated renal metastasis after colon cancer. Can J
Urol. 14:3649–3650. 2007.PubMed/NCBI
|
|
18
|
Lowe LH, Zagoria RJ, Chen MY and Dyer RB:
Intraluminal renal metastasis from colon cancer simulating a fungus
ball. Urol Radiol. 13:226–227. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shiraishi T, Hasegawa Y, Itoh H and
Nakakuki K: Implantation of colon cancer cells onto renal pelvic
mucosa. A case report. APMIS. 97:181–184. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ho L, Wassef H, Henderson R and Seto J:
Renal metastasis from primary colon cancer on FDG PET-CT. Clin Nucl
Med. 34:596–597. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Julianov A, Stoyanov H and Karashmalakov
A: Late renal metastasis from sigmoid adenocarcinoma. Lancet Oncol.
5:7262004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Numata M, Shiozawa M, Watanabe T, Tamagawa
H, Yamamoto N, Morinaga S, Watanabe K, Godai T, Oshima T, Fujii S,
et al: The clinicopathological features of colorectal mucinous
adenocarcinoma and a therapeutic strategy for the disease. World J
Surg Oncol. 10:1092012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Melichar B, Morávek P, Ferko A and Podhola
M: Metastatic colorectal carcinoma and kidney tumors: A report of
four cases. Tumori. 96:483–486. 2010.PubMed/NCBI
|