Introduction
Schwannomas (neuroma, neurinoma or neurilemmoma) are
benign encapsulated peripheral nerve sheath neoplasms that arise
from Schwann cells, which produce myelin. Approximately 8% of head
and neck schwannomas involve the intracranial portion of a
peripheral nerve sheath (1,2). Primary intraorbital schwannomas account
for only 1–2% of all intracranial tumors (3). Intraocular schwannomas arise from
ciliary nerves in the uvea, mostly in the ciliary body or choroid
and occasionally in the iris (4–7).
Intraocular schwannomas are benign encapsulated tumors consisting
of a pure proliferation of Schwann cells and are not life
threatening; however, they can cause impairment and blindness via
tumor growth and serous retinal detachment, and appropriate
treatment is required to prevent vision loss and progressive
enlargement of the condition (8–10). Uveal
schwannoma is also termed a ‘pseudomelanoma’, as it simulates the
most common type of primary intraocular tumor, uveal melanoma; this
term reflects the difficulty in clinically distinguishing the
schwannoma from uveal malignant melanoma (11–13). In
certain previously reported cases, eyeball enucleation was
performed due to a diagnosis of malignant melanoma, and only after
subsequent histopathological examination of the surgical specimen
was a benign tumor revealed (14–18). In
the present study, the cases of 3 patients with intraocular
schwannoma who underwent surgical excision locally, retained the
eyeball or even achieved an improvement in visual acuity are
reviewed.
Case reports
Case 1
A 25-year-old man complained of vision loss that had
persisted for 1 month on January 19 2012 at Peking University
People's Hospital (Beijing, China). Poor eyesight of the right eye
with ametropia had been present since early age. Other past medical
and family histories were unremarkable. The best corrected visual
acuity was 20/640, with nystagmus, and the intraocular pressure
(IOP) was 9 mmHg in the right eye. Slit-lamp biomicroscopy showed a
normal anterior segment. Examination of the retina showed a
superotemporal, pre-equatorial, pigmentary choroidal tumor in the
right eye, which was associated with exudative retinal detachment
(Fig. 1). The left eye displayed
ametropia and nystagmus, and was otherwise normal. On
ultrasonography, the tumor measured 10.1 mm in width and 8.8 mm in
height, and the ciliary body was involved (Fig. 1).
Following a complete medical examination, the
patient was given a preliminary diagnosis of choroid and ciliary
body melanoma with exudative retinal detachment of the right eye.
Under general hypotension anesthesia, a trans-scleral local
resection was performed, with brachytherapy using a
106Ru ophthalmic applicator (model CCB) for 19 h. The
excised tumor was sent for histopathological examination. Specimens
was fixed with 4% neutral formalin at 25°C for 6 h and then
embedded in paraffin. Hematoxylin and eosin-stained sections (4 µm)
were obtained for light microscopy analysis. Sections (3 µm) were
cut and placed on silanized slides and pretreated at the
temperature of 25°C for 15 min in citrate buffer prior to
immunostaining in order to improve the staining pattern. Sections
were also pre-treated at 25°C for 10 min in 3% hydrogen peroxide
blocking reagent for blocking endogenous peroxidase activity.
Tissue sections were stained using the following monoclonal primary
antibodies (OriGene Technologies, Inc., Beijing, China): Mouse
anti-S-100 protein (cat. no. ZM-0224), rabbit anti-Desmin (cat. no.
ZA-0610), mouse anti-smooth muscle actin (cat. no. ZM-0003), mouse
anti-cluster of differentiation 34 (cat. no. ZM-0046) and rabbit
anti-vimentin (cat. no. ZA-0511). The incubation with these
antibodies was performed at 37°C for 1 h. The secondary antibody
used was horseradish peroxidase-labelled goat anti-mouse/rabbit IgG
polymer (cat. no. PV-8000; OriGene Technologies, Inc.). The
incubation was performed at 37°C for 30 min. The immunoreaction was
visualized by demonstration of conjugated peroxidase with
3,3′Diaminobenzidine (DAB; cat. no. ZLI-9019; dilution, 1:20;
OriGene Technologies, Inc.) as the substrate. The incubation was
performed for 5 min at 25°C. The slides were counterstained with
hematoxylin following staining with DAB in preparation for light
microscopy. The tissue sections were observed 40, 100 and ×200
magnification. HE staining revealed a tumor composed of spindle
cells that were arranged in bundle. Spindle cells were
well-differentiated and mild nuclear pleomorphism was present.
Mitotic figures were rare. A palisading arrangement could be
observed (Fig. 1).
Immunohistochemistry results were as follows: S-100(+), Desmin(−),
smooth muscle actin(−), cluster of differentiation 34(−) and
Vimentin(+). The confirmed diagnosis of ciliochoroidal schwannoma
was therefore made in the right eye upon histopathological
examination following the trans-scleral incisional tumor
biopsy.
No complications occurred during the operative or
postoperative courses. On day 9 post-surgery, the patient's visual
acuity was 20/800, with an IOP of 9 mmHg. Examination of Fundus
demonstrated that the retina had been reattached. However, the
patient did not come back for a follow-up check following discharge
from hospital.
Case 2
A 48-year-old otherwise healthy woman presented
reporting observations of black shadow flies in the left eye for 5
years and vision loss that had persisted for 1 month on July 9 2014
at Peking University People's Hospital. Past medical and family
histories were unremarkable. Ophthalmic examination of the right
eye was normal. Visual acuity was 20/50 and the IOP was 13 mmHg in
the left eye. A slit-lamp biomicroscopic ophthalmic examination
revealed a large, prominent, pink, solid lesion that was rich in
blood vessels in the anterior chamber prior to the ciliary body
from the 6 to 9 o'clock positions, with iridodialysis and pupillary
deformation and shift (Fig. 2). The
fundus of the left eye showed multiple yellow mobile vitreous
particles that indicated asteroid hyalosis. Examination of the
retina showed a nasal choroidal tumor without hemorrhage and
exudation (Fig. 2).
Ultrasonography demonstrated asteroid hyalosis in
the vitreous humor and an inferior nasal lateral hypoechoic mass,
measuring 16.7 mm in cross-sectional basal diameters and 11.2 mm at
its greatest apical height (Fig. 2).
Ultrasound biomicroscopy demonstrated a giant mass on the inferior
nasal quadrant of the ciliary body. The acoustic reflectivity of
the anterior region was of low-to-middle grade (Fig. 2).
A trans-scleral local resection was performed, and
the tumor was completely removed and sent for histopathological
examination, which was performed according to the aforementioned
protocol. Histopathology examination revealed that the tumor was
composed of spindle cells, which were bland and well
differentiated. In addition, the majority of spindle cells were
arranged in bundles and some areas in a palisade pattern, which
confirmed the diagnosis of ciliochoroidal schwannoma. However, the
patient experienced suprachoroidal hemorrhage during surgery, and
was left with only the ability to perceive light. At the final
follow-up performed on the patient three months post-surgery, the
patient developed retinal detachment without light sensation, the
Ciliochoroidal schwannoma was totally removed and the eyeball was
preserved.
Case 3
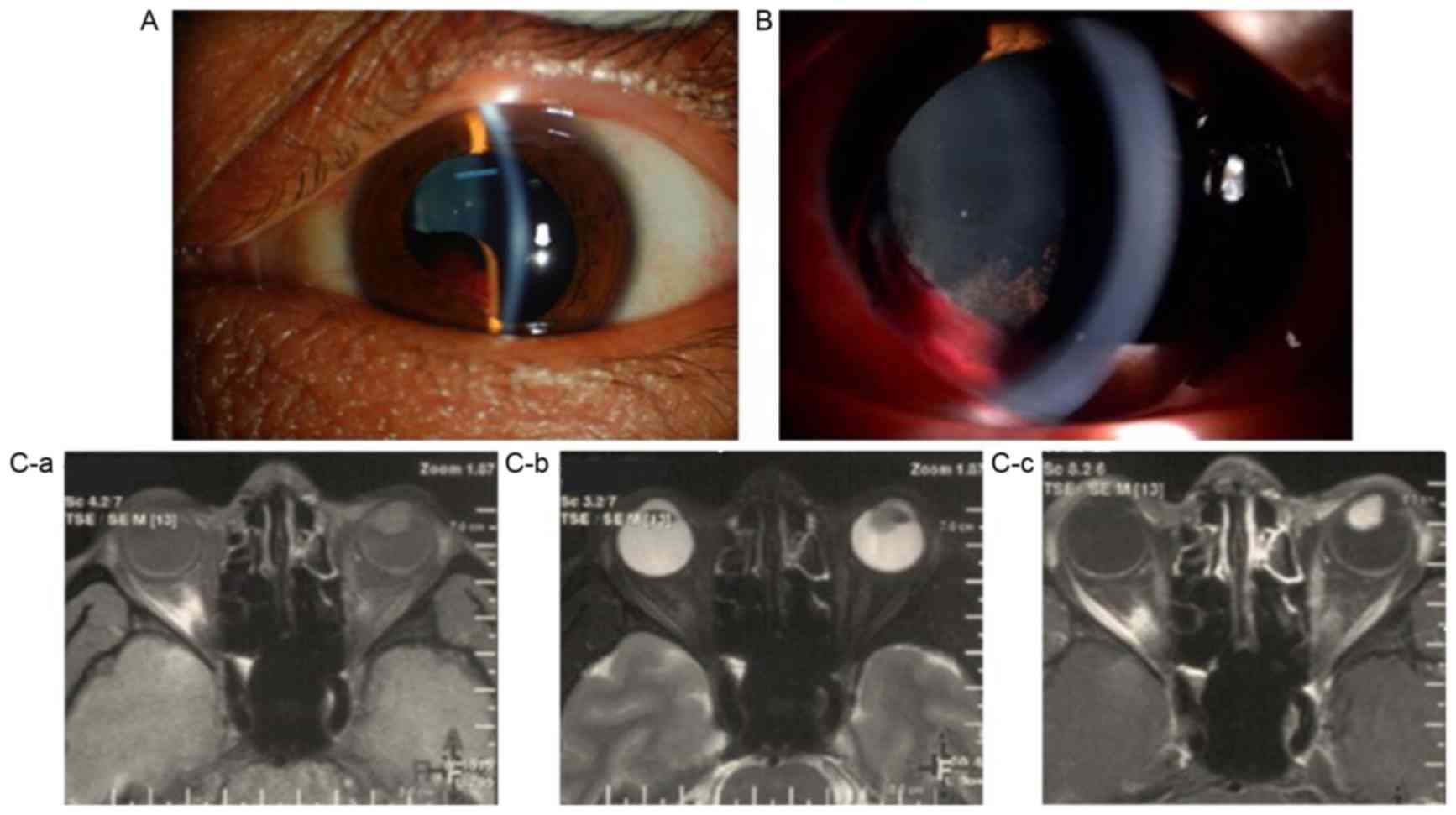
A 30-year-old otherwise healthy man reported loss of
visual acuity in the left eye following a injury following a fit 3
months previously on April 26 2013 at Peking University People's
Hospital. Past medical and family histories were unremarkable. The
ophthalmic examination of the right eye was normal. The patient's
best corrected visual acuity (BCVA) was 20/200 and the IOP was 11
mmHg in the left eye. A dilated ophthalmic examination revealed a
highly prominent brown, avascular, solid, homogenous lesion in the
ciliary body from the 6 to 9 o'clock position, with subluxation of
the lens temporally and superiorly (Fig.
3). Examination of the optic disk and retina indicated normal
results.
Ultrasound biomicroscopy demonstrated a giant mass
behind the inferior nasal quadrant of the iris. The acoustic
reflectivity of the anterior region was of medium-to-high grade,
with posterior attenuation. A computed tomography scan revealed an
area with slightly high density in the antero-inferior vitreous.
Magnetic resonance imaging (MRI) demonstrated a lesion as an
isointense area on T1-weighted imaging (T1WI), which showed
homogenous contrast enhancement, and as an isointense area or an
area with slightly high intensity on T2WI (Fig. 3). No other clinically evident tumors
were present.
Following a complete medical examination, the
patient was given a preliminary diagnosis of a ciliary body tumor
with a secondary subluxated lens of the left eye. Under general
hypotension anesthesia, the tumor was carefully dissected free and
completely removed under a lamellar scleral flap, combined with
brachytherapy using the 106Ru ophthalmic applicator
(model CCA) for 24 h. Specimens were sent for histopathological
examination, which was performed according to the aforementioned
protocol. Histopathology examination revealed that the tumor was
composed of spindle cells, which were bland and well
differentiated. In addition, the majority of spindle cells were
arranged in bundles and some areas in a palisade pattern, which
confirmed the diagnosis of schwannoma. Thus, the pathological
diagnosis was a schwannoma of the ciliary body in the left eye.
No complications were noted during the operative or
postoperative courses. Slit-lamp images captured on postoperative
day 5 showed that the giant iridociliary mass had been completely
resolved (Fig. 3). The patient's BCVA
was 20/40, with an IOP of 10 mmHg. The patient was followed up for
16 months and was disease-free until the last follow-up
examination, with a BCVA of 20/20.
Discussion
Intraocular schwannoma is an extremely rare benign
neoplasm that arises from Schwann cells. To date, there has been no
report of malignant intraocular schwannoma (5,16,18). A confirmed diagnosis depends on the
immunohistochemical analysis of biopsy results, which can
distinguish schwannoma from other spindle-cell tumors. Intraocular
schwannoma often disguises itself as an amelanotic choroidal
melanoma in the clinic. In a previous report, 44% of eyes with
schwannoma were reported to have been enucleated, since the
clinical assessment tended to be that of a malignant mass (13). Local lesion resection can successfully
preserve a viable globe. Complete lesion resection results in
visual acuity being preserved and a normal IOP. In the present case
series, the schwannomas were isolated tumors with no association
with multisystem disorders, and all the three cases underwent local
resection and retained the eyeball.
Case 1 is typical in that the patient was
preliminarily diagnosed with choroid and ciliary body melanoma upon
medical examination and only confirmed with a ciliochoroidal
schwannoma on histopathological examination. Case 2 showed a
prominent, pink, solid lesion that was rich in blood vessels, with
a pathological diagnosis of schwannoma. The lack of tumor
pigmentation is not diagnostic; for example, leiomyoma, melanoma
and other tumors can be amelanotic, while schwannoma can be deeply
pigmented. Histopathological examination is required for a
definitive diagnosis. Case 3 is the only case in which the ciliary
body was involved, and following a local excision, the BCVA was
significantly improved.
In conclusion, choroidal schwannoma has a variety of
clinical manifestations. The most common symptom is decreasing
vision without pain, but others include proptosis of the eye, the
limitation of ocular movement, leukocoria and occasional pain, as
described in previously reported cases (5). However, all the clinical features are
attributable to the expansile growth of the tumor and the
oppression of the surrounding structures. Although clinical
features and findings on ultrasonography, indocyanine green
choroidal angiography, fundus fluorescein angiography, MRI and
computed tomography in a schwannoma can provide assistance in
differentiating these tumors from others, a definite
differentiation is often not possible prior to histopathological
examination (19). In certain
previous cases, eyeball enucleation has been performed due to a
malignant melanoma diagnosis or due to the rapid progression of
symptoms, which was considered malignant, and only subsequent
histopathological examination of the surgical specimen has revealed
a benign tumor. As cytologically benign tumors, intraocular
schwannomas only require treatment to prevent the visual loss that
results from their enlargement. In cases where the clinical
features are not typical of melanoma, such as the presence of
cystic components or amelanotic lesions, we recommend performing a
surgical excision followed by immunohistological analysis to
confirm the features of the neoplasm, whether benign or malignant,
prior to considering enucleation. Thus, the present study indicates
that pathological biopsy is required for diagnosis and the optimal
therapy for intraocular schwannoma is local resection. A reliable
non-invasive examination is now required to obtain a diagnosis and
guide the subsequent treatment, in order to reduce the final
enucleation rate.
Acknowledgements
The authors would like to thank Dr. QingYu Meng
(Department of Ophthalmology, Peking University People's Hospital,
Beijing, China) for their cooperation in the modification of the
image format.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JL contributed to the conception and constructive
discussion of the case series. YY, YC and KW contributed to
analysis of the data, and the preparation and writing of the
manuscript. YY contributed to the search for computerized databases
and patient medical records. KS and DS contributed to the
pathological diagnosis and description.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from all
patients.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Tung H, Chen T and Weiss MH: Sixth nerve
schwannomas. Report of two cases. J Neurosurg. 75:638–641. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kurtkaya-Yapicier O, Scheithauer B and
Woodruff JM: The pathobiologic spectrum of Schwannomas. Histol
Histopathol. 18:925–934. 2003.PubMed/NCBI
|
|
3
|
Butt ZA and McNab AA: Orbital
neurilemmoma: Report of seven cases. J Clin Neurosci. 5:390–393.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Shields JA, Sanborn GE, Kurz GH and
Augsburger JJ: Benign peripheral nerve tumor of the choroid: A
clinicopathologic correlation and review of the literature.
Ophthalmology. 88:1322–1329. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee SH, Hong JS, Choi JH and Chung WS:
Choroidal schwannoma. Acta Ophthalmol Scand. 83:754–756. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim IT and Chang SD: Ciliary body
schwannoma. Acta Ophthalmol Scand. 77:462–466. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mawas J: Schwannomas of the iris (gliomas
of the terminal ciliary nerves). Bull Soc Ophtalmol Fr. 62:31–41.
1962.(In French). PubMed/NCBI
|
|
8
|
Tsuzuki N, Katoh H, Ohnuki A, Ishihara S,
Miyazawa T, Nawashiro H and Shima K: Cystic schwannoma of the
orbit: Case report. Surg Neurol. 54:385–387. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Subramanian N, Rambhatia S, Mahesh L,
Menon SV, Krishnakumar S, Biswas J and Noronha OV: Cystic
schwannoma of the orbit-a case series. Orbit. 24:125–129. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lam DS, Ng JS, To KF, Abdulah V, Liew CT
and Tso MO: Cystic schwannoma of the orbit. Eye. 11:798–800. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Augsburger JJ, Shields JA, Folberg R, Lang
W, O'Hara BJ and Claricci JD: Fine needle aspiration biopsy in the
diagnosis of intraocular cancer. Cytologic-histologic correlations.
Ophthalmology. 92:39–49. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Scheie HG and Yanoff M: Pseudomelanoma of
the ciliary body. Report of a patient. Arch Ophthalmol. 77:81–83.
1967. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
You JY, Finger PT, Iacob C, McCormick SA
and Milman T: Intraocular schwannoma. Surv Ophthalmol. 58:77–85.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Matsuo T and Notohara K: Choroidal
schwannoma: Immunohistochemical and electron-microscopic study.
Ophthalmologica. 214:156–160. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen JJ, Kamberos NL, O'Dorisio MS, Syed
NA and Boldt C: Choroidal schwannoma in a 6-month-old girl. J
AAPOS. 18:197–199. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mortuza S, Esmaeli B and Bell D: Primary
intraocular ancient schwannoma: A case report and review of the
literature. Head Neck. 36:E36–E38. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Thaller VT and Perinti A and Perinti A:
Benign schwannoma simulating a ciliary body melanoma. Eye.
12:158–159. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Damato B, Damato EM, Konstantinidis L,
Heimann H and Coupland SE: Choroidal schwannoma: A case series of
five patients. Br J Ophthalmol. 98:1096–1100. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fan JT, Campbell RJ and Robertson DM: A
survey of intraocular schwannoma with a case report. Can J
Ophthalmol. 30:37–41. 1995.PubMed/NCBI
|