Introduction
Thyroid cancer is a common endocrine malignant
tumor, the prevalence of which continues to increase worldwide
(1). It has been reported that
~40,000 patients succumb to thyroid cancer per year, whereas
~300,000 new patients are diagnosed (1,2).
Papillary thyroid cancer (PTC) is the most common type of thyroid
cancer and is characterized by a differentiated neoplasia (3). BRAF mutations are highly prevalent in
thyroid carcinomas, especially B-Raf proto-oncogene
serine/threonine kinase (BRAF)V600E (4). Distinguishing PTC from a benign thyroid
nodule (BTN), including thyroid adenoma and classical nodular
goiter, is crucial for clinicians. Currently, the two most common
examination methods, ultrasound (US) and computed tomography, are
used to analyze suspect thyroid nodules (5). Furthermore, pre-operative US-guided
fine-needle aspiration cytology (FNAC) and intraoperative
pathological examination are performed to further explore patients
suspected of having PTC (5).
However, FNAC sampling is very invasive and therefore limited since
it requires multiple aspirations (6). Therefore, the identification of novel
non-invasive biomarkers that do not require any invasive procedure
is crucial for the early screening of PTC.
MicroRNAs (miRNAs/miRs) are small non-coding RNAs
that are key regulators in various physiological and pathological
processes, including cell proliferation, cell differentiation and
cell death (7–10). Recent studies have revealed that,
since circulating miRNAs are very stable in serum and plasma, and
present high sensitivity and specificity, they may be considered as
novel biomarkers (11,12). Xiong et al (13), demonstrated that miR-126-3p is a
tumor suppressor in the progression of thyroid cancer. In addition,
miR-375 has been reported to inhibit cell proliferation in thyroid
cancer cells by suppressing expression of erb-b2 receptor tyrosine
kinase 2 (10). Furthermore, miR-222
and miR-146b are positively correlated with the development of PTC
in patients with recurrent PTC (14).
The abnormal expression of miR-22 has been widely
reported in various types of cancer, including breast and
colorectal cancers (15,16). However, whether miR-22 is
dysregulated in PTC has not been investigated. The current study
aimed to evaluate the expression of miR-22 in patients with PTC and
to further elucidate whether it could be used as a potential
biomarker to differentiate patients with PTC from patients with BTN
and healthy controls.
Materials and methods
Patients
The present study was approved by the Research
Ethics Committee of the Hongqi Hospital Affiliated to Mudanjiang
Medical University (Mudanjiang, China) and all patients provided
written informed consent. A total of 150 patients with primary PTC,
100 patients with BTN, and 40 age- and sex-matched healthy controls
from the Hongqi Hospital Affiliated to Mudanjiang Medical
University were enrolled in this study between April 2016 and
November 2017. Written informed consent was obtained from all
participants. PTC or BTN tissues were extracted from patients, 10%
formalin-fixed at room temperature for 24 h and paraffin-embedded,
and further analyzed for histopathological diagnosis and miRNA
examination. The embedded samples were then immediately frozen for
total RNA extraction. In addition, blood samples (5 ml) were taken
from all subjects prior to surgery, and additional blood samples
were collected from six patients after tumor resection and
receiving appropriate treatment for 1 week. All blood samples were
directly placed into tubes containing sodium citrate. Then, blood
samples were centrifuged at 3,000 × g for 15 min at 4°C. Clinical
features of the patients included in this study are listed in
Table I.
 | Table I.Clinical features of patients with PTC
and healthy controls. |
Table I.
Clinical features of patients with PTC
and healthy controls.
| Variable | PTC patients | BTN patients | Healthy controls |
|---|
| Male/female | 73/77 | 52/48 | 19/21 |
| Age (year) | 55.3±11.3 | 49.5±16.2 | 53.8±7.9 |
| Tumor size (cm) |
|
|
|
| ≤1 | 77 | – | – |
|
>1 | 73 | – | – |
| Capsular
invasion |
|
|
|
|
Yes | 62 | – | – |
| No | 88 | – | – |
| Lymph node
metastasis |
|
|
|
|
Yes | 65 | – | – |
| No | 85 | – | – |
| No. of cancer
foci |
|
|
|
|
Single | 86 | – | – |
|
Multiple | 74 | – | – |
|
BRAFV600E gene |
|
|
|
|
Mutant | 98 | – | – |
| Wild
type | 52 | – | – |
US-guided FNAB
FNAB was performed to aspirate papillary thyroid
tissues by endocrinologists using a 25-gauge needle. After each
aspiration, the cytological material was immediately smeared onto
slides. The slides were prepared by both air-dried and
alcohol-fixed methods (70% alcohol once, 95% alcohol twice,
absolute alcohol three times, each time for 1 min at room
temperature). The air-dried smears were stained using the Diff-Quik
method (17) and immediately
evaluated by a cytopathologist, whereas the alcohol-fixed smears
were stained by the Papanicolaou method (18) in the cytology laboratory. The sample
slide obtained using the Diff-Quik method was then evaluated and
classified as ‘adequate (sufficient lymphocytes),’ ‘less than
optimal (some lymphocytes),’ or ‘inadequate (very few or no
lymphocytes)’. Another FNA pass was performed without smear, and
the sample was collected by rinsing the needle in a tube containing
1 ml Hank balanced salt solution without heparin. The specimens
were immediately transferred to the clinical laboratory and stored
at −20°C for 0 to 4 days prior to thyroglobulin (Tg) analysis. For
each patient, all passes were performed by the same
endocrinologist.
Tg-FNAB antibody assays
The Tg measurements in the needle washouts (Tg-FNAB)
were carried out using a commercial immunofluorometric assay
(TRA-1-81, Baiao Bolai Bio. Co, Beijing, China) with monoclonal
antibodies (DELFIA®; PerkinElmer, Inc., Waltham, MA,
USA) and a functional sensitivity of 1.0 ng/ml, according to the
manufacturer's protocol.
Sample acquisition and RNA
extraction
Total RNA from the serum and tissue samples was
isolated with RNAVzol LS (Vigorous Biotechnology Co, Beijing,
China, http://www.vigorousbiol.com/)
according to the manufacturer's protocol. The quality, quantity and
integrity of the RNA were monitored using a NanoDrop
spectrophotometer (ND-1000; NanoDrop Technologies; Thermo Fisher
Scientific, Inc., Wilmington, DE, USA).
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
The RNA was reverse transcribed into cDNA using the
Prime-Script one-step RT-qPCR kit referring to the M-MLV cDNA first
strand synthesis system (cat no. C28025-032, Invitrogen; Thermo
Fisher Scientific Inc., Waltham, MA, USA) according to the
manufacturer's protocol. qPCR was performed using SYBR Green
Supermix (Bio-Rad Laboratories, Inc., Hercules, CA, USA) in a
Bio-Rad iCycleriQ real-time PCR detection system. The qPCR
procedure was performed as follows: 95°C for 10 min, followed by 50
cycles of 95°C for 10 sec, 55°C for 10 sec, 72°C for 5 sec, 99°C
for 1 sec, 59°C for 15 sec and 95°C for 1 sec, after which, samples
were cooled to 40°C. U6 was used as an internal reference gene. The
relative expression levels were calculated using the
2−ΔΔCq method (19), and
the experiments were repeated in triplicate. The primers used in
the current study were as follows: miR-22-RT,
5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACTAAGC-3′; U6-RT,
5′-GTCGTATCCAGTGCAGGGTCCGAGGTATTCGCACTGGATACGACAAAATG-3′; miR-22,
forward, 5′-GCAGTTCTTCAGTGGCAAGC-3′; U6, forward,
5′-GCGCGTCGTGAAGCGTTC-3′; universal reverse primer,
5′-GTGCAGGGTCCGAGGT-3′. RT refers to the stem loop primer.
B-Raf proto-oncogene serine/threonine
kinase (BRAF)V600E gene testing
Determination of the BRAFV600E gene
mutation was carried out for all patients with PTC by PCR
techniques (20). DNA was isolated
from PTC tissues using a DNA Extraction kit (Promega Corporation,
Madison, WI, USA), and BRAF gene exon 15 was detected using a BRAF
mutant gene detection kit (Amoy Diagnostics Co., LTD, Fujian,
China) according to the manufacturer's protocol and the ABI7500
real-time PCR amplifier (Applied Biosystems; Thermo Fisher Inc.,
Waltham, MA, USA). The primers for amplification of exon 15 of BRAF
were designed as follows: Forward, 5′-TCATAATGCTTGCTCTGATAGGA-3′
and reverse, 5′-GGCCAAAAATTTAATCAGTGGA-3′). All procedures and
analyses were carried out in the biomolecular laboratory of the
Hongqi Hospital Affiliated to Mudanjiang Medical University.
Statistical analysis
Data are presented as the means ± standard deviation
(SD). Each experiment was repeated with three times. A two-tailed
unpaired Student's t-test was used for comparisons between two
groups. One-Way Analysis of Variance (SPSS 13.0; SPSS, Inc.,
Chicago, IL, USA) followed by a Tukey post hoc test was used to
compare more than two groups. Receiver operating characteristic
(ROC) curves were used to assess miR-22 as a biomarker, and the
area under the curve (AUC) was reported (SPSS version 20.0; IBM
Corp., Armonk, NY, USA). Spearman's correlation coefficient was
used to determine the correlation between serum miR-22 and tissue
miR-22, and serum miR-22 and Tg levels in the tissues of patients
with PTC. P<0.05 was considered to indicate a statistically
significant difference.
Results
Serum miR-22 is increased in patients
with PTC
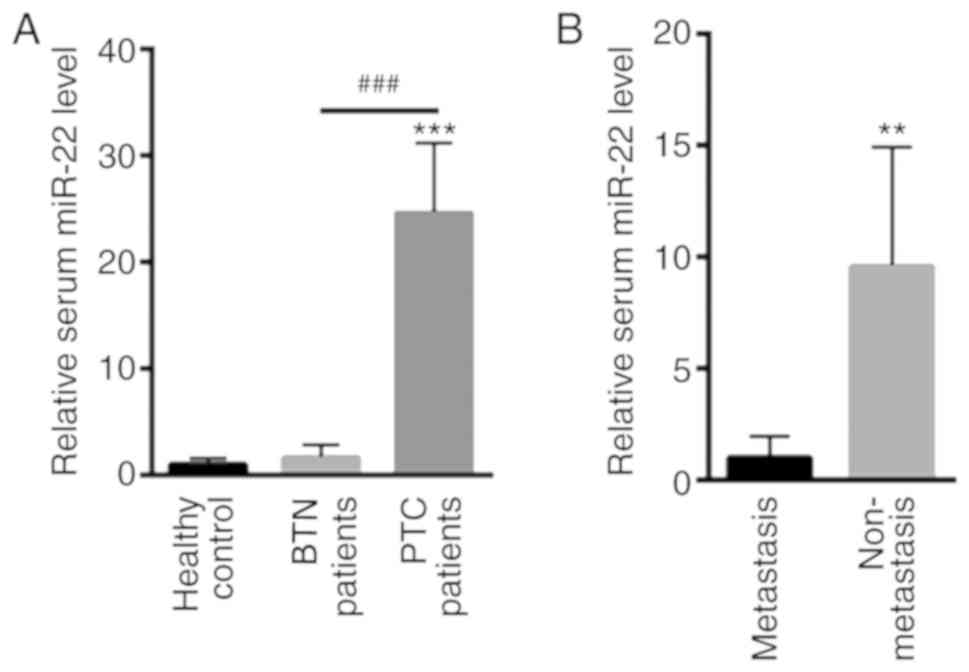
RT-qPCR was carried out to detect the levels of
miR-22 in the serum of patients with PTC, patients with BTN and
healthy controls. Serum miR-22 was slightly increased in patients
with BTN (1.67±1.18, P>0.05) whereas it was significantly
increased in patients with PTC (24.65±6.58) compared with the
healthy controls (1.00±0.58) (Fig.
1A). In addition, serum miR-22 was significantly increased in
patients with PTC and metastasis (9.57±5.35) compared with in
patients with PTC who have no metastasis (1.00±0.96) (P<0.01;
Fig. 1B).
Levels of miR-22 in thyroid tissue are
increased in patients with PTC
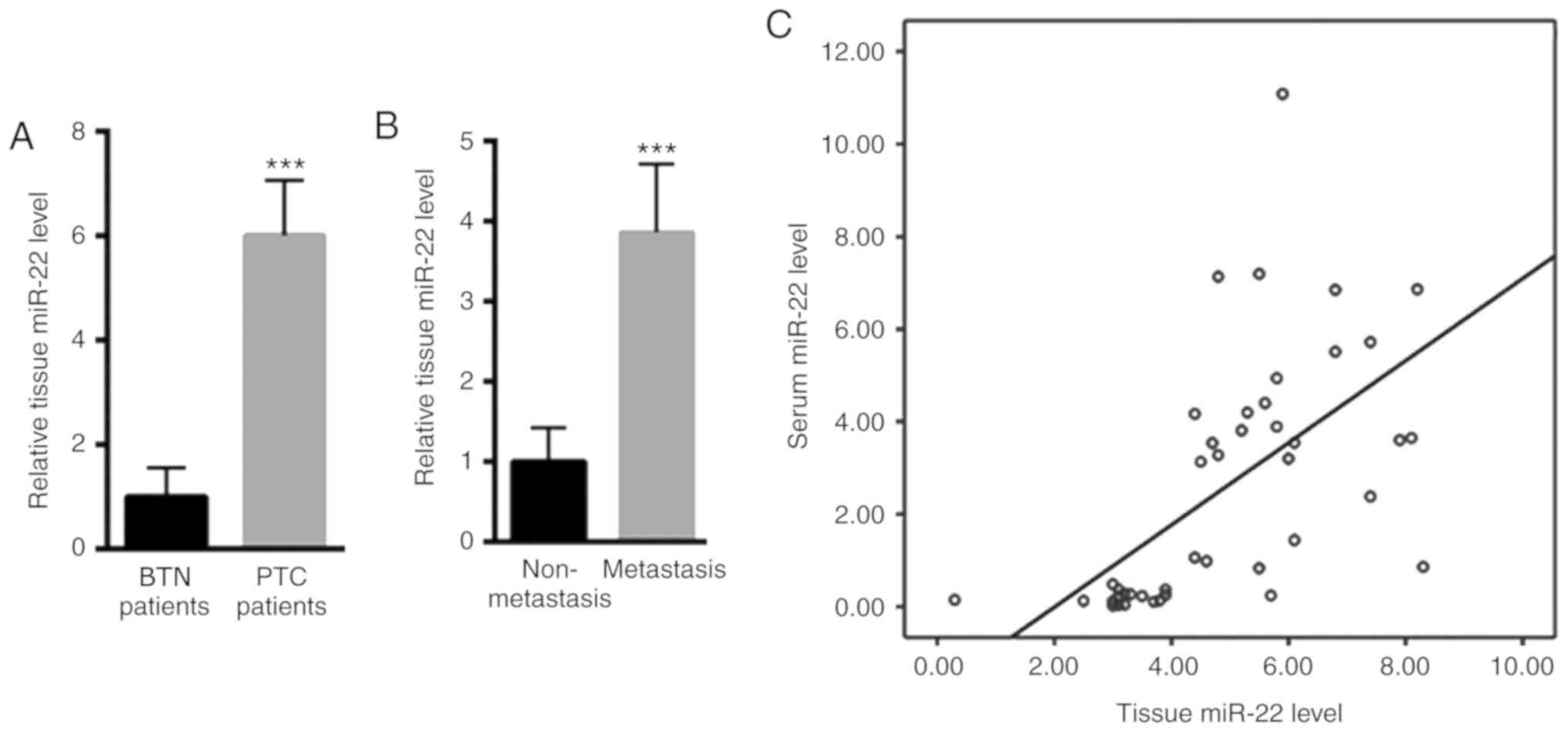
Furthermore, miR-22 expression levels were increased
in the thyroid tissue of patients with PTC (6.01±1.05) compared
with in patients with BTN (1.00±0.56) (Fig. 2A). In addition, miR-22 was increased
in patients with PTC and metastasis (3.86±0.85) compared with in
patients with PTC who have no metastasis (1.00±0.42) (Fig. 2B). The correlation between serum and
thyroid tissue levels of miR-22 was also investigated. Serum miR-22
levels were positively correlated with PTC tissue miR-22 levels
(r=0.592, P<0.001; Fig. 2C).
Serum miR-22 is enhanced in BRAFV600E
mutant patients with PTC
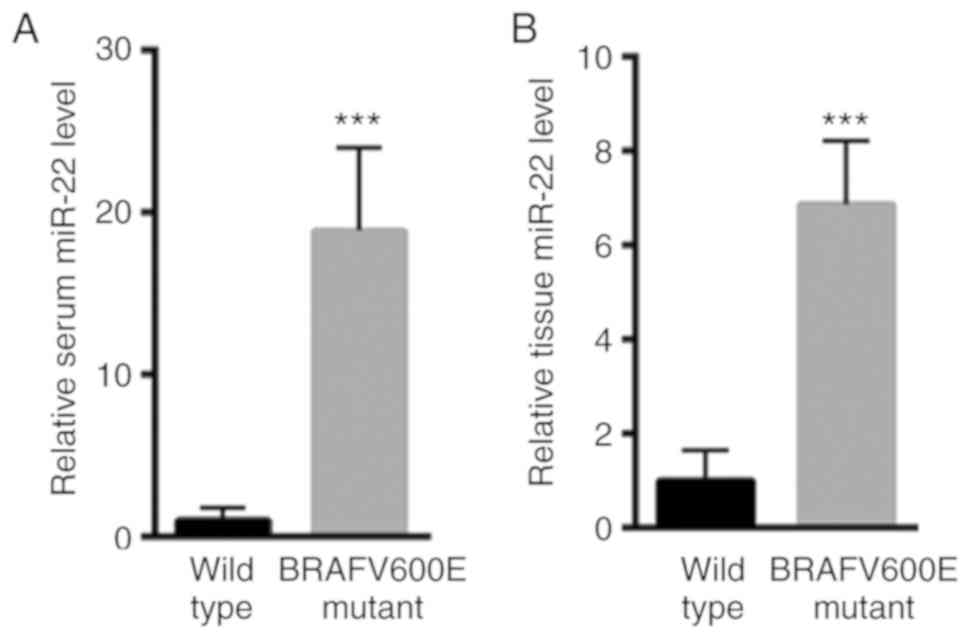
Patients with PTC were further divided according to
the presence of a BRAF gene mutation. As shown in Table I, 98 patients were identified as
BRAFV600E mutants and 52 patients were identified as wild type BRAF
patients. Furthermore, serum miR-22 levels were increased in the
BRAFV600E mutant patients with PTC (18.86±5.12) compared with in
the BRAFV600E wild type patients with PTC (1.00±0.79) (Fig. 3A). In addition, higher miR-22 levels
were identified in the thyroid tissues of BRAFV600E mutant patients
with PTC (6.87±1.35) compared with in the BRAFV600E wild
type patients with PTC (1.00±0.65) (Fig.
3B).
miR-22 is positively correlated with
Tg-FNAB levels
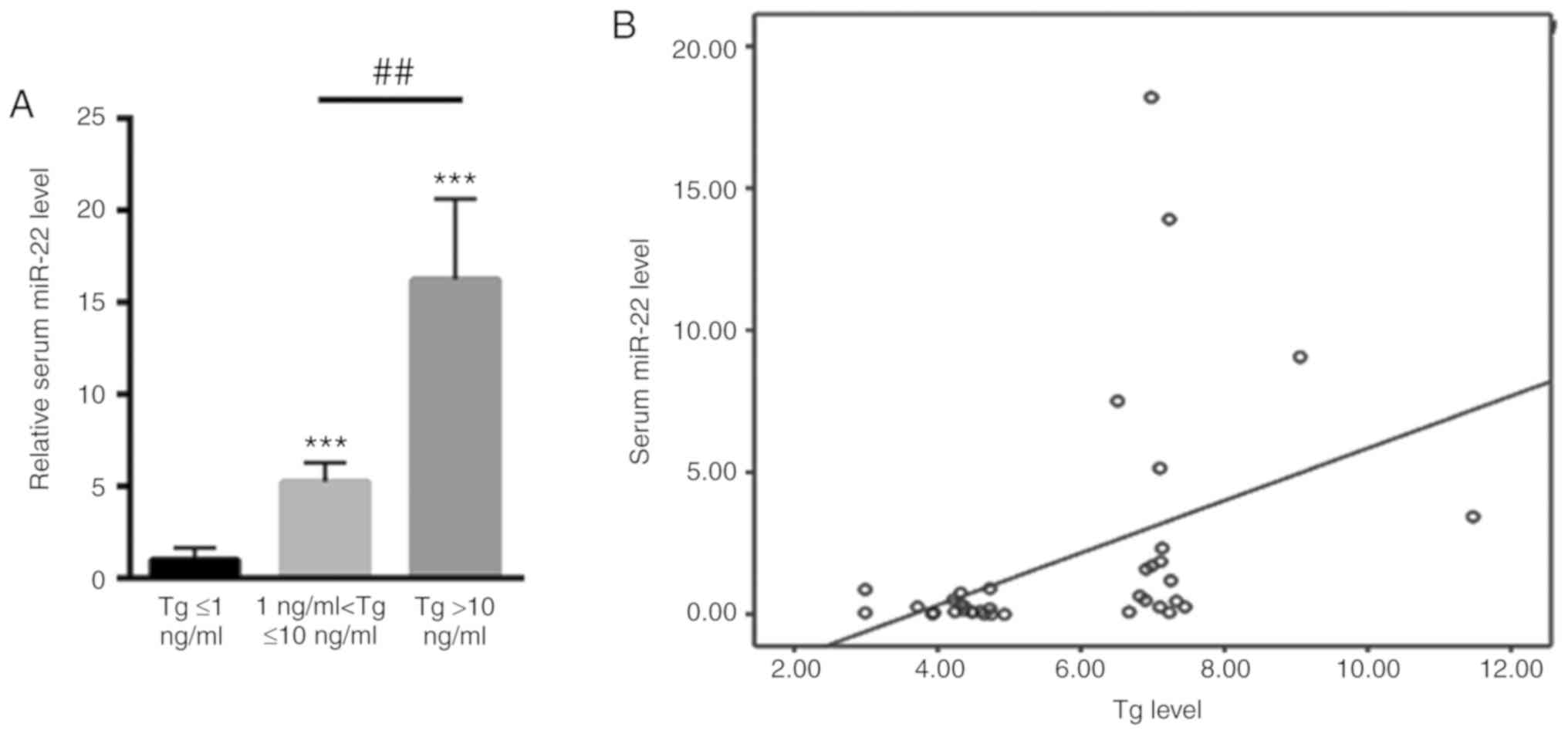
Tg determination in the needle washouts (Tg-FNAB) is
an important method to determine malignancy in the lymph nodes
(LNs). The serum expression levels of miR-22 were therefore
compared in the different Tg-FNAB groups. Briefly, 30 patients were
included in the ≤1 ng/ml Tg-FNAB group and 62 patients were
included in the 1–10 ng/ml Tg-FNAB group, whereas 58 patients were
included in >10 ng/ml Tg-FNAB group. As shown in Fig. 4A, serum miR-22 was much lower in
patients with PTC with ≤1 ng/ml Tg-FNAB (1.00±0.64). Conversely,
serum miR-22 was much higher in patients with PTC with 1–10 ng/ml
Tg-FNAB (5.23±1.03) and was highest in patients with PTC with
>10 ng/ml Tg-FNAB (16.24±4.36) (Fig.
4A). Furthermore, serum miR-22 was demonstrated to be
positively correlated with Tg levels in patients with PTC (r=0.423,
P<0.001; Fig. 4B).
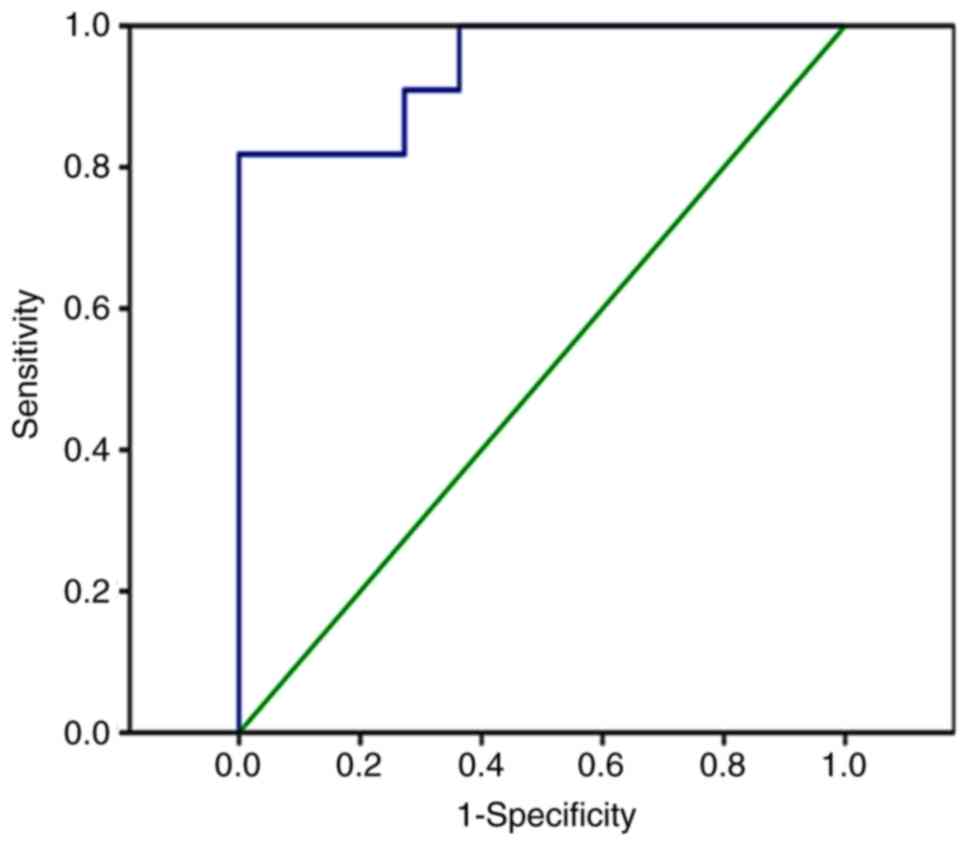
miR-22 differentiates patients with
PTC from healthy controls
Finally, a ROC analysis was carried out to evaluate
whether serum miR-22 expression could be used as a potential
biomarker to discern patients with PTC from healthy controls. Data
revealed that serum miR-22 could differentiate patients with PTC
from healthy controls, with an AUC of 0.942 (95% confidence
interval: 0.858–1.000; P<0.001; Fig.
5).
Discussion
The identification of novel biomarkers for patients
with PTC is crucial (21,22). It has been reported that a BRAF
mutation, assessed after FNA, is an important biomarker for
aggressive PTC (23). Furthermore,
p27, p21, cyclin D1, osteopontin and E-cadherin have also been
suggested as potential biomarkers for the diagnosis of PTC
(24,25). However, these biomarkers are limited
due to their poor clinical applications.
Due to their stability and abundance in the
circulatory system, circulating miRNAs have been revealed as
important biomarkers for various types of cancer (11,12). To
the best of our knowledge, the present study is the first to
demonstrate increased miR-22 levels in the serum of patients with
PTC compared with in patients with BTN and healthy controls.
Similarly, the levels of miR-22 were increased in thyroid tissues
of patients with PTC compared with in patients with BTN. These
observations indicated that miR-22 may have an oncogenic role in
the development of PTC. In addition, cancer metastasis is still a
major cause of mortality for patients (26). Identifying a novel diagnostic tool or
therapeutic intervention that would serve a key role in the
prevention of PTC is therefore crucial (27). In the present study, serum and tissue
miR-22 levels were significantly increased in patients with PTC and
metastasis compared with in patients with PTC who had no
metastasis.
The T1799A nucleotide mutation in the BRAF gene is a
key oncogenic mutation in patients with PTC (28,29). It
has been estimated that 45% of patients with PTC have this
mutation, which corresponds to a valine-to-glutamic acid exchange
in codon 600 of the BRAF protein (BRAFV600E). This mutation
increases serine/threonine protein kinase activities and
constitutively activates the mitogen-activated protein kinase
signaling pathway (30,31). Therefore, BRAFV600E represents an
important prognostic marker for patients with PTC (30,31). The
expression levels of miR-22 in serum and tissue samples from
patients with PTC and the BRAFV600E mutation were also analyzed and
compared with the wild type patients. Results demonstrated that
serum and tissue miR-22 levels were increased in patients with PTC
with the BRAFV600E mutation, thus indicating that the upregulation
of miR-22 may be positively associated with the risk of PTC.
Furthermore, Tg-FNAB is another important method for
determining LN metastases (32,33).
However, 5–10% of FNABs have been demonstrated to have
non-diagnostic value and 6–8% to be false negatives (34). The present study revealed that serum
miR-22 expression was significantly augmented in patients with PTC
with 1–10 ng/ml Tg-FNAB and >10 ng/ml Tg-FNAB, thus suggesting
that serum miR-22 may be used as an auxiliary non-invasive
diagnostic method in line with Tg-FNAB levels. The ROC analysis
also demonstrated that serum miR-22 expression was able to directly
differentiate patients with PTC from healthy controls.
A previous study proposed that circulating miR-22 is
associated with the etiology of liver injury in patients with human
immunodeficiency virus (HIV), which suggests that miR-22
circulating levels may be an independent predictor of liver injury
in patients with HIV (35).
Furthermore, serum miR-22-5p is correlated with acute myocardial
infarction (AMI), which suggests that miR-22 could also be a
promising biomarker for the diagnosis of AMI (36). In comparison with these studies, the
present study attempted to determine whether serum miR-22
expression could be a potential biomarker for patients with PTC.
Other conditions may also cause an increase in serum miR-22
(1,2). The present study mainly focused on
miR-22 expression in patients with PTC; a detailed analysis of
miR-22 expression in serum and tissues was conducted from patients
previously categorized into different groups. miR-22 levels were
assessed in 150 patients with PTC, 100 patients with BTN and 40
normal subjects. The results revealed a significant increase in
miR-22 expression in the serum and thyroid tissues of patients with
PTC, which was associated with the presence of metastasis and the
BRAFV600E mutation. ROC analysis also demonstrated that serum
miR-22 may be used as a biomarker for screening patients with PTC.
These novel findings are interesting and may be of significant
clinical importance.
In conclusion, to the best of our knowledge, the
present study was the first to reveal that miR-22 serum levels may
represent a novel biomarker for patients with PTC that does not
involve any invasive procedure. However, a larger number of samples
should be included in a future study. In addition, detailed
analysis of the potential relationship between serum levels of
miR-22 and the clinicopathological features of patients should be
considered.
Acknowledgements
Not applicable.
Funding
The present study was supported by a grant from the
PhD startup fund of Mudanjiang Medical University (grant no.
MMU-20170615).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author upon reasonable
request.
Authors' contributions
DW performed the experiments and analyzed the data.
CG, TK, GM, and JL performed the RT-qPCR experiments. YS designed
the experiments, analyzed the data and gave final approval of the
published version. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Research
Ethics Committee of Hongqi Hospital Affiliated to Mudanjiang
Medical University, Mudanjiang City (HQH-2016014, Mudanjiang City,
China), and all the patients have provided written informed consent
for this study.
Patient consent for publication
All patients provided consent for publication of
their data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Haugen BR, Sawka AM, Alexander EK, Bible
KC, Caturegli P, Doherty GM, Mandel SJ, Morris JC, Nassar A, Pacini
F, et al: American thyroid association guidelines on the management
of thyroid nodules and differentiated thyroid cancer task force
review and recommendation on the proposed renaming of encapsulated
follicular variant papillary thyroid carcinoma without invasion to
noninvasive follicular thyroid neoplasm with papillary-like nuclear
features. Thyroid. 27:481–483. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hao Y, Pan C, Chen W, Zhu WZ and Qi JP:
Differentiation between malignant and benign thyroid nodules and
stratification of papillary thyroid cancer with aggressive
histological features: Whole-lesion diffusion-weighted imaging
histogram analysis. J Magn Reson Imaging. 44:1546–1555. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fusco A, Chiappetta G, Hui P, Rostan GG,
Golden L, Kinder BK, Dillon DA, Giuliano A, Cirafici AM, Santoro M,
Rosai J, et al: Assessment of RET/PTC oncogene activation and
clonality in thyroid nodules with incomplete morphological evidence
of papillary carcinoma: A search for the early precursors of
papillary cancer. Am J Pathol. 160:2157–2167. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jolly LA, Novitskiy S, Owens P, Massoll N,
Cheng N, Fang W, Moses HL and Franco AT: Fibroblast-mediated
collagen remodeling within the tumor microenvironment facilitates
progression of thyroid cancers driven by BrafV600E and Pten loss.
Cancer Res. 76:1804–1813. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Brace MD, Wang J, Petten M, Bullock MJ,
Makki F, Trites J, Taylor SM and Hart RD: Differential expression
of transforming growth factor-beta in benign vs. papillary thyroid
cancer nodules; a potential diagnostic tool? J Otolaryngol Head
Neck Surg. 43:222014.
|
|
6
|
Hwang S, Shin DY, Kim EK, Yang WI, Byun
JW, Lee SJ, Kim G, Im SJ and Lee EJ: Focal lymphocytic thyroiditis
nodules share the features of papillary thyroid cancer on
ultrasound. Yonsei Med J. 56:1338–1344. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Baldini E, Tuccilli C, Prinzi N, Sorrenti
S, Falvo L, Vito CD, Catania A, Tartaglia F, Mocini R, Coccaro C,
et al: Deregulated expression of Aurora kinases is not a prognostic
biomarker in papillary thyroid cancer patients. PLoS One.
10:e01215142015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Komatsu S, Ichikawa D, Takeshita H,
Morimura R, Hirajima S, Tsujiura M, Kawaguchi T, Miyamae M, Nagata
H, Hirotaka K, et al: Circulating miR-18a: A sensitive cancer
screening biomarker in human cancer. In Vivo. 28:293–297.
2014.PubMed/NCBI
|
|
9
|
Kurashige J, Mima K, Sawada G, Takahashi
Y, Eguchi H, Sugimachi K, Mori M, Yanagihara K, Yashiro M, Hirakawa
K, et al: Epigenetic modulation and repression of miR-200b by
cancer-associated fibroblasts contribute to cancer invasion and
peritoneal dissemination in gastric cancer. Carcinogenesis.
36:133–141. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang XZ, Hang YK, Liu JB, Hou YQ, Wang N
and Wang MJ: Over-expression of microRNA-375 inhibits papillary
thyroid carcinoma cell proliferation and induces cell apoptosis by
targeting ERBB2. J Pharmacol Sci. 130:78–84. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chou CK, Liu RT and Kang HY:
MicroRNA-146b: A novel biomarker and therapeutic target for human
papillary thyroid cancer. Int J Mol Sci. 18:2017. View Article : Google Scholar
|
|
12
|
Dai L, Wang Y, Chen L, Zheng J, Li J and
Wu X: MiR-221, a potential prognostic biomarker for recurrence in
papillary thyroid cancer. World J Surg Oncol. 15:112017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xiong Y, Kotian S, Zeiger MA, Zhang L and
Kebebew E: miR-126-3p inhibits thyroid cancer cell growth and
metastasis, and is associated with aggressive thyroid cancer. PLoS
One. 10:e01304962015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lee JC, Zhao JT, Clifton-Bligh RJ, Gill A,
Gundara JS, Ip JC, Glover A, Sywak MS, Delbridge LW, Robinson BG
and Sidhu SB: MicroRNA-222 and microRNA-146b are tissue and
circulating biomarkers of recurrent papillary thyroid cancer.
Cancer. 119:4358–4365. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu H, Huang X and Ye T: MiR-22
down-regulates the proto-oncogene ATP citrate lyase to inhibit the
growth and metastasis of breast cancer. Am J Transl Res.
10:659–669. 2018.PubMed/NCBI
|
|
16
|
Chen Z, Shen A, Liu L, Chen Y, Chu J, Cai
Q, Qi F, Sferra TJ and Peng J: Pien Tze Huang induces apoptosis and
inhibits proliferation of 5-fluorouracil-resistant colorectal
carcinoma cells via increasing miR-22 expression. Exp Ther Med.
14:3533–3540. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Domper Arnal MJ and Ferrandez Arenas Á:
and Lanas Arbeloa Á: Esophageal cancer: Risk factors, screening and
endoscopic treatment in Western and Eastern countries. World J
Gastroenterol. 21:7933–7943. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Benjamin H, Schnitzer-Perlman T, Shtabsky
A, VandenBussche CJ, Ali SZ, Kolar Z and Pagni F;: Rosetta Genomics
Group, Bar D and Meiri E: Analytical validity of a microRNA-based
assay for diagnosing indeterminate thyroid FNA smears from
routinely prepared cytology slides. Cancer Cytopathol. 124:711–721.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Qu K, Pan Q, Zhang X, Rodriguez L, Zhang
K, Li H, Ho A, Sanders H, Sferruzza A, Cheng SM, et al: Detection
of BRAF V600 mutations in metastatic melanoma: Comparison of the
Cobas 4800 and Sanger sequencing assays. J Mol Diagn. 15:790–795.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yoon JH, Lee HS, Kim EK, Moon HJ and Kwak
JY: Thyroid nodules: Nondiagnostic cytologic results according to
thyroid imaging reporting and data system before and after
application of the bethesda system. Radiology. 276:579–587. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Moon HJ, Kim EK, Yoon JH and Kwak JY:
Malignancy risk stratification in thyroid nodules with
nondiagnostic results at cytologic examination: Combination of
thyroid imaging reporting and data system and the Bethesda System.
Radiology. 274:287–295. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang J, Liu BJ, Xu HX, Xu JM, Zhang YF,
Liu C, Wu J, Sun LP, Guo LH, Liu LN, et al: Prospective validation
of an ultrasound-based thyroid imaging reporting and data system
(TI-RADS) on 3980 thyroid nodules. Int J Clin Exp Med. 8:5911–5917.
2015.PubMed/NCBI
|
|
24
|
Rodolico V, Cabibi D, Pizzolanti G,
Richiusa P, Gebbia N, Martorana A, Russo A, Amato MC, Galluzzo A
and Giordano C: BRAF V600E mutation and p27 kip1 expression in
papillary carcinomas of the thyroid <or=1 cm and their paired
lymph node metastases. Cancer. 110:1218–1226. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pesutic-Pisac V, Punda A, Gluncic I and
Bedeković V: Kragić AP and Kunac N: Cyclin D1 and p27 expression as
prognostic factor in papillary carcinoma of thyroid: Association
with clinicopathological parameters. Croat Med J. 49:643–649. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nguyen QT, Lee EJ, Huang MG, Park YI,
Khullar A and Plodkowski RA: Diagnosis and treatment of patients
with thyroid cancer. Am Health Drug Benefits. 8:30–40.
2015.PubMed/NCBI
|
|
27
|
Baldini E, Sorrenti S, Tuccilli C, Prinzi
N, Coccaro C, Catania A, Filippini A, Bononi M, Antoni ED,
D'Armiento M and Ulisse S: Emerging molecular markers for the
prognosis of differentiated thyroid cancer patients. Int J Surg. 12
(Suppl):S52–S56. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cohen Y, Xing M, Mambo E, Guo Z, Wu G,
Trink B, Beller U, Westra WH, Ladenson PW and Sidransky D: BRAF
mutation in papillary thyroid carcinoma. J Natl Cancer Inst.
95:625–627. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kimura ET, Nikiforova MN, Zhu Z, Knauf JA,
Nikiforov YE and Fagin JA: High prevalence of BRAF mutations in
thyroid cancer: Genetic evidence for constitutive activation of the
RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma.
Cancer Res. 63:1454–1457. 2003.PubMed/NCBI
|
|
30
|
Davies H, Bignell GR, Cox C, Stephens P,
Edkins S, Clegg S, Teague J, Woffendin H, Garnett MJ, Bottomley W,
et al: Mutations of the BRAF gene in human cancer. Nature.
417:949–954. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Millington GWM. Mutations of the BRAF gene
in human cancer. Davies, et al: (Nature 2002; 417 949 54). Clin Exp
Dermatol. 38:222–223. 2013.PubMed/NCBI
|
|
32
|
Li QK, Nugent SL, Straseski J, Cooper D,
Riedel S, Askin FB and Sokoll LJ: Thyroglobulin measurements in
fine-needle aspiration cytology of lymph nodes for the detection of
metastatic papillary thyroid carcinoma. Cancer Cytopathol.
121:440–448. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hanna AN, Michael CW and Jing X: Mixed
medullary-follicular carcinoma of the thyroid: Diagnostic dilemmas
in fine-needle aspiration cytology. Diagn Cytopathol. 39:862–865.
2011. View
Article : Google Scholar : PubMed/NCBI
|
|
34
|
Frasoldati A and Valcavi R: Challenges in
neck ultrasonography: Lymphadenopathy and parathyroid glands.
Endocr Pract. 10:261–268. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Anadol E, Schierwagen R, Elfimova N, Tack
K, Schwarze-Zander C, Eischeid H, Noetel A, Boesecke C, Jansen C,
Dold L, et al: Circulating microRNAs as a marker for liver injury
in human immunodeficiency virus patients. Hepatology. 61:46–55.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Maciejak A, Kiliszek M, Opolski G, Segiet
A, Matlak K, Dobrzycki S, Tulacz D, Sygitowicz G, Burzynska B and
Gora M: miR-22-5p revealed as a potential biomarker involved in the
acute phase of myocardial infarction via profiling of circulating
microRNAs. Mol Med Rep. 14:2867–2875. 2016. View Article : Google Scholar : PubMed/NCBI
|