Introduction
Head and neck squamous cell carcinoma (HNSCC)
originates from the oral cavity, oropharynx, hypopharynx,
nasopharynx, and larynx and is one of the most fatal among cancers.
human papilloma virus (HPV) is believed to play role in the
pathogenesis of HNSCC, specifically in oropharyngeal cancer (OPC),
along with tobacco and alcohol. Despite HPV driven OPC increment in
western countries (1), HPV-positive
OPC responds well to chemoradiotherapy. In contrast, HPV-negative
patients are generally resistant to these treatment modalities.
Besides, advanced OPC requires multimodal approaches like surgery
with adjuvant irradiation or concurrent irradiation with salvage
surgery (2). As pharynx has
important role in basic functions such as speech, chewing, and
swallowing, complications and morbidity after treatment are the
additional consequences that patients suffer together with the main
problem of survival (3).
HPV-negative HNSCC patients are usually elder, the
lesions are larger and overall survival is less when compared to
HPV-positive HNSCC patients (4). It
is also suggested that HPV-positive and HPV-negative cases'
molecular background are different. According to Cancer Genome
Atlas Network data in HPV-negative cases, TP53 84%, CCND1 31%,
CDKN2A 58% and, FGFR1 10% have been altered. On the other hand,
TP53 and CCND1 have been altered only in 3% and CDKN2A and FGFR1
had no alteration in HPV-positive cases (5). Although there has been improvement in
understanding the background of HPV-negative cases, resistance to
chemo/radiotherapy is still the dead end indicating the need of
further studies. Cancer stem cell (CSC) model (hierarchic model) of
cancer suggests that only a subpopulation of cells in the tumor
bulk, CSC, have the potential to form the cancer cells that is
different than the stochastic model of cancer in which every cell
in the tumor bulk has the potential to form cancer cells. Besides,
clonal evolution of CSC puts forwards another difficulty in
revealing CSC mechanism and role in cancer because of subgroups and
genetic heterogeneity, which means different genetic backgrounds
and different phenotypes in CSC (6,7). Like
stem cells, cancer stem cells (CSCs) have the potential of
differentiation and self-renewal. First defined in leukemia
(8), later in other cancers like
breast (9), brain tumor (10), colon (11), and over (12), in 2007 CSC were defined in HNSCC
(13). CSCs have recently been a hot
spot in HNSCC research as they are postulated to play important
role in initiation, progression, invasion, metastasis, and as well
they are supposed to be resistant to chemo/radio therapy and
responsible for recurrence (14).
Their resistance to chemotherapy and radiation is through
mechanisms like dormancy, DNA repair, multidrug-resistance-type
membrane transporters, and escaping apoptosis (15). Although CSCs are very rare in the
tumor bulk, sometimes even less than 1%, they are considered to be
important to evaluate new therapeutic approaches (16). Not only by biological evidence but
also via mathematical modeling it is also shown that a successful
therapy should target CSCs as well (17). Additionally, CSC is an important
target in cancer that still needs to be clarified. There is the
necessity of understanding CSC better to elucidate their role in
carcinogenesis of HPV-negative OPC. Therefore, in this study we
focused on characterization of CSC in HPV-negative OPC cell line
UTSCC-60A to carry our understanding to a higher level for possible
treatment of OPC via CSC.
Materials and methods
Cell culture
UTSCC-60A (University of Turku- Squamous Carcinoma
Cell 60A) cell line, which was used for the experiments, is
HPV-negative oropharyngeal squamous cell carcinoma generated from
left tonsil cancer, kindly provided by Reidar Grenman, Department
of Otorhinolaryngology, Turku University, Finland (18–20).
UTSCC-60A was cultured in Dulbecco's modified Eagle's medium (DMEM,
Thermo Fisher Scientific, Inc.) containing 10% fetal bovine serum
(HyClone), 1% antibiotics (Thermo Fisher Scientific, Inc.) and, 1%
GlutaMax supplement (Thermo Fisher Scientific, Inc.) at 37°C in a
humidified atmosphere of 5% CO2 in air. Cells were
passaged at 4–5 days.
Isolation of CSC
CSCs were isolated through magnetic activated cell
sorting. Based on the cell number tyrpsinized (0.25% Trypsin-EDTA,
Thermo Fisher Scientific, Inc.), magnetic beads (goat anti-mouse
IgG magnetic beads, NEB) ratio was calculated. Trypsinized cells
were re-suspended in 1 ml of cold PBS and kept in 4°C until
combined with the magnetic beads. For 1×107 cells 0.25
µl of magnetic beads were washed with 1 ml of cold phosphate
buffered saline (PBS, Thermo Fisher Scientific, Inc.) three times.
This wash step included 2 min on the rotator followed by 2 min on
the magnetic rack, discarding the PBS without disturbing the
magnetic bead pellet every time. Then, magnetic beads were
incubated with the first antibody mouse anti-ALDH1A1 (ab105920;
Abcam) at 4°C for one and a half hour. Magnetic beads and antibody
ratio were 1:1. After antibody incubation, magnetic beads were
washed with cold PBS four times as same as mentioned above. Cells
that were trypsinized previously and kept at 4°C were combined with
magnetic beads and incubated at 4°C for half an hour. Cell and
magnetic bead suspension were carried to magnetic rack for
separation and kept on magnetic rack for 15 min. Without disturbing
the cell-magnetic bead pellet supernatant was carried to a clean
centrifuge tube representing nonCSC. Cell-magnetic bead pellet was
re-suspended in CSC medium displaying the CSC population.
Sphere formation assay
Isolated CSCs were plated to ultra-low attachment
surface 96U-well plate (Thermo Fisher Scientific, Inc.) in CSC
medium: DMEM, B27 2%, N2 1%, 10 ng/ml human epidermal growth factor
(EGF), 20 ng/ml human fibroblast growth factor (FGF), and
antibiotics 1%. Everyday cells were supplemented with fresh EGF and
FGF. Spheroids were evaluated under microscope.
RT-qPCR
TriPure (Roche, Basel, Switzerland) was applied
directly to the isolated CSC and nonCSC followed by the
manufacturer's protocol. Before cDNA synthesis from CSC and nonCSC
samples, samples were treated with DNase (Thermo Fisher Scientific,
Inc.) following manufacturer's specifications. 100 ng of total RNA
for each sample was converted to first strand cDNA (RevertAid First
Strand cDNA Synthesis kit, Thermo Fisher Scientific, Inc.)
according to the manufacturer's protocol. All samples including
controls; reverse transcriptase negative, no template negative,
positive control; were amplified to confirm the cDNA synthesis
without DNA contamination. SyberGreen (Thermo Fisher Scientific,
Inc.) was used for RT-qPCR reaction on Applied Biosystems 7500 Real
Time PCR system. CSC markers OCT4, SOX2, BMI1, CD133, and KLF4 RNA
levels, quadruplicate samples for each marker were evaluated for 3
times. Gene specific amplification was normalized to β-actin
expression. Relative quantification results were calculated with
ΔΔCq method (21) through
manufacturer's Sequence Detection System (SDS) software
protocol.
Immunofluorescence staining
Isolated CSCs were cultured in CSC medium for 3 days
for immunofluorescence staining. Then spheres were carried to
chamber slides and incubated at 37°C in a humidified atmosphere of
5% CO2 in air, overnight. After spheres' attachment to
the surface of the chamber slide were confirmed under microscope
CSCs were fixed with 4% PFA/PBS and incubated at room temperature
for 20 min. After wash steps, blocking buffer was applied, which
was followed by first antibody, mouse monoclonal Anti-ALDH1A1
(abcam ab105920), 1:600 dilution application overnight at 4°C. Next
day slides were washed with PBS than incubated with 1:1,000
dilution second antibody (goat anti-mouse IgG; Abcam) 1 h in dark
at room temperature. Twice washed with PBS, nuclei staining (DAPI,
Thermo Fisher Scientific, Inc.) were performed. After last wash
step, chambers were removed from the slides and slides were
mounted. CSCs were examined under microscope (Nikon Eclipse, Ts2).
nonCSC immunofluorescence staining was performed as the same way as
mentioned above for CSC, except the sphere formation step.
Cell proliferation assay
Triplicate samples for each dosage of Cisplatin
(Sigma) for CSCs and nonCSCs plated to 96 well tissue culture
plates as 5×103 cells/well and incubated at 37°C in a
humidified atmosphere of 5% CO2 in air. After CSCs and
nonCSCs attachment to the wells confirmed under microscope, cells
were treated with Cisplatin for 24 h. Cisplatin dosage was used
between 40 µg/ml-0.3125 µg/ml. 50 µl of XTT (Roche Cell
Proliferation kit II; Roche) assay was added to the each well and
absorbance was read at 490–660 nm using microplate reader Corona
SH-9000Lab, following 4 h of incubation. Background was measured
through average of wells containing only medium. Cell proliferation
experiments were repeated twice with triplicate samples each time.
For statistical significance the Student's t-test was
determined.
Statistical analysis
Student's t-test was used to calculate the
significance of RT-qPCR and cell proliferation assay results
between CSC and nonCSC. P<0.05 was considered to indicate a
statistically significant difference. All experiments were repeated
at least twice with at least triplicate samples.
Results
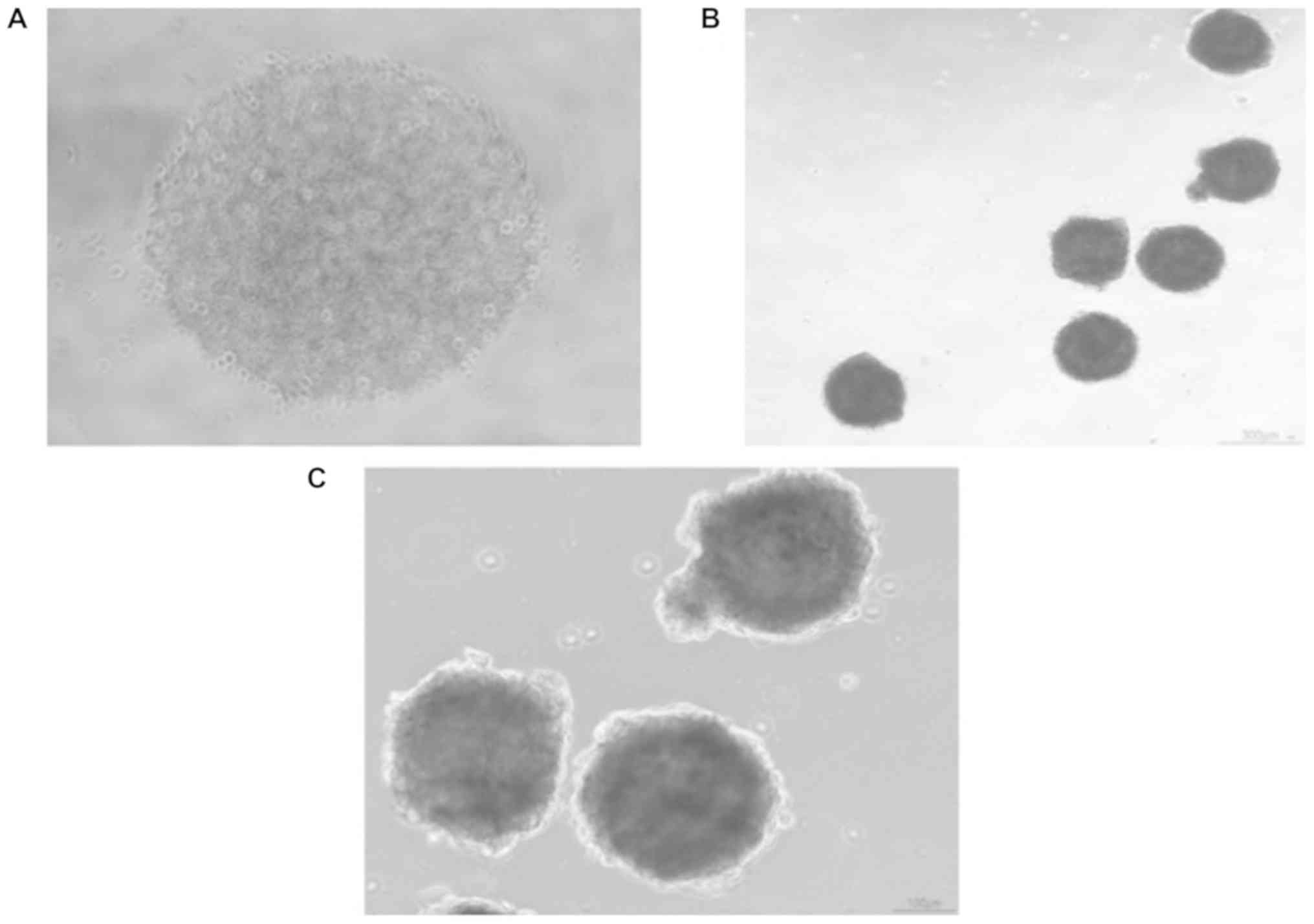
CSC spheres of UTSCC-60A cell
line
Before CSC isolation, cancer cells were counted
(Invitrogen) and after isolation CSCs were counted. In UTSCC-60A
cell-line there was only 0.6% of CSC which represented a small
population compared to nonCSC. Isolated CSCs were plated as
2×103 in each well of 96 well-plate U-bottom with CSC
medium. Spheres in each well could be observed under microscope
(Fig. 1A). At the 3rd-4th day CSC
spheres could be pictured after carrying to a flat-bottom well
plates (Fig. 1B and C).
Morphological images of spheres generated from UTSCC-60A were
highly dense and dark.
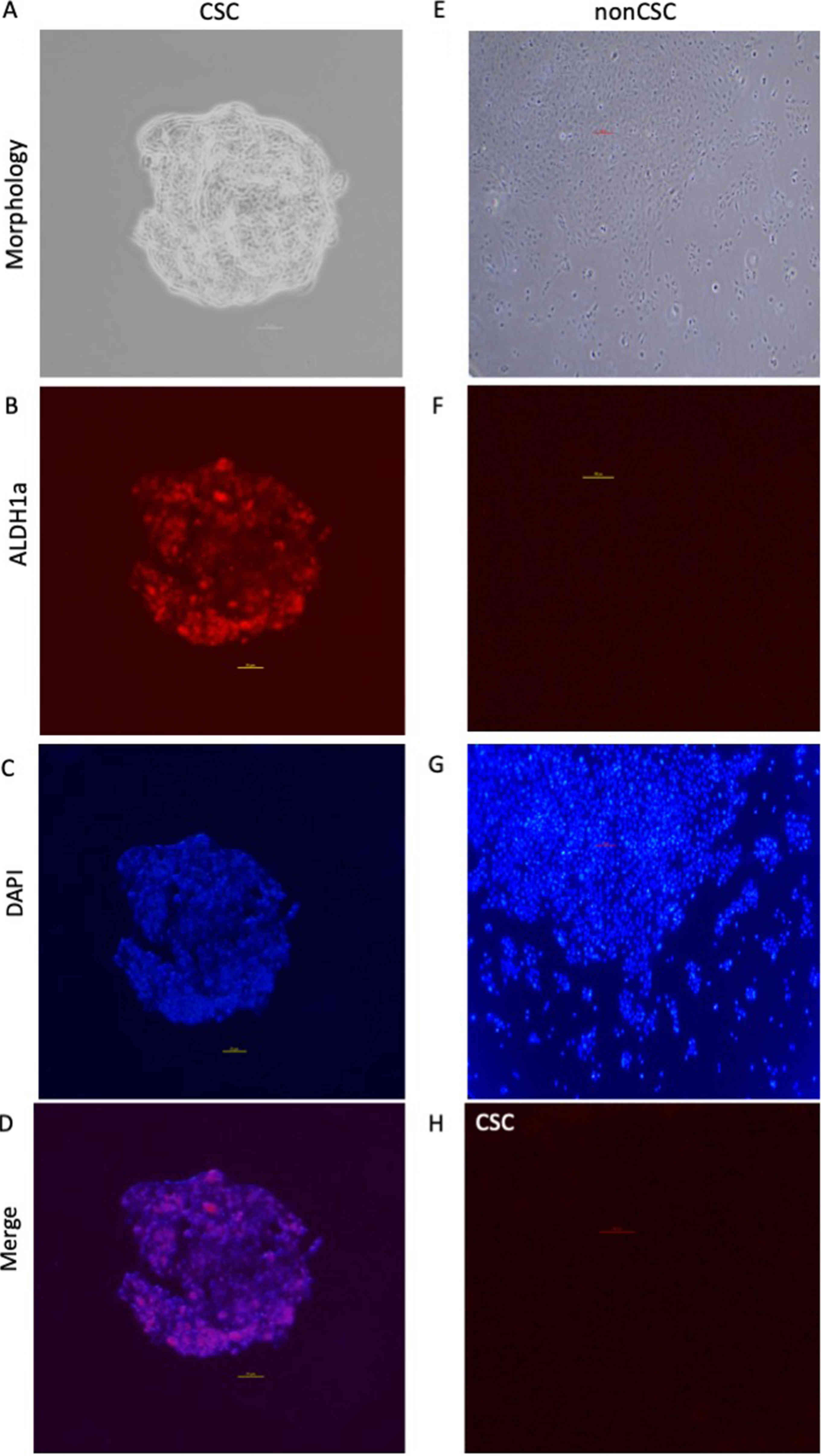
Immunofluorescence staining of
spheres
For both cell type mouse Anti-ALDH1A1 (ab105920;
Abcam) antibody was used for immunofluorescence staining. As
expected, while ALDH1a expression could be observed in CSC spheres,
there was no ALDH1a expression in nonCSC. This result confirmed the
successful isolation of CSCs. In CSC ALDH1a expression was specific
to spheroid formation. Negative control (no primary antibody)
didn't display any ALDH1a expression for both cell lines
representing clearance of undesired background staining. DAPI could
be detected for both cell type, displaying different patterns for
CSC and nonCSC (Fig. 2).
CSC marker expression by RT-qPCR
CSC markers OCT4, SOX2, KLF4 and BMI1were expressed
significantly higher in CSC when compared to nonCSC. OCT4, SOX2,
KLF4 and BMI1 were respectively 2.33, 2.53, 2.68, and 1.34 folds
higher in CSC. For OCT4, SOX2 and KLF4 were all P<0.01,
respectively P=0.0009, P=0.0001, P=0.0043, P=0.0013. CD133
expression was almost at the same level in both cell type (Fig. 3). CD133 gene expression was only
1.03-fold higher and P=0.91.
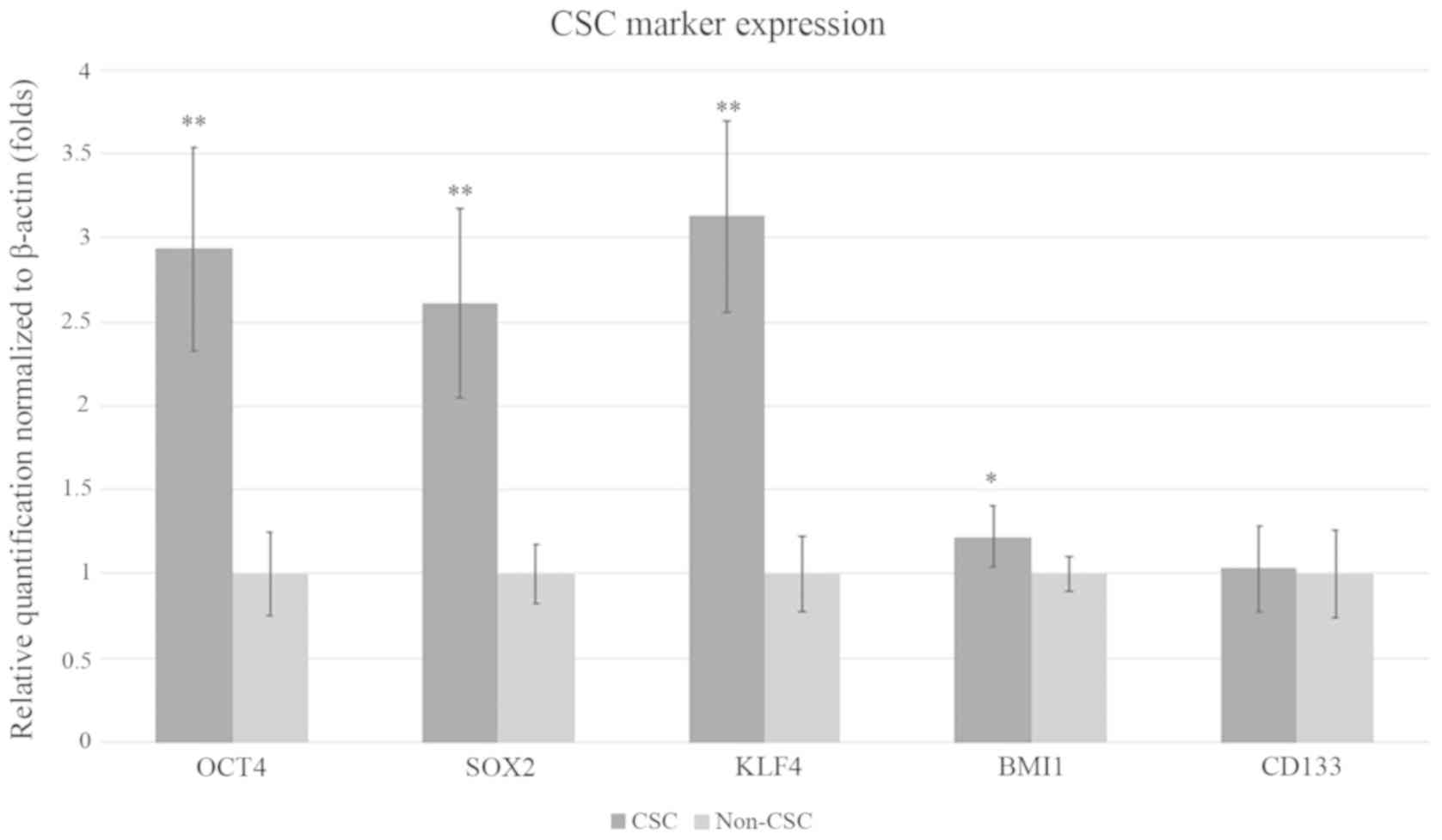 | Figure 3.Reverse transcription-quantitative
PCR results of CSC marker expression normalized to β-actin
expression. Relative expression of CSC and non-CSC for markers
CD133, OCT4, SOX2, KLF4 and BMI1 are presented as fold changes. CSC
expression levels for markers CD133, OCT4, SOX2, KLF4 and BMI1 were
compared to non-CSC expression levels of the same genes. Error bars
represent the mean ± SD of at least quadruplicate samples of three
independent experiments. *P<0.05 and **P<0.01 vs. non-CSC.
CSC, cancer stem cell; KLF4, Kruppel-like factor; BMI1, BMI1
proto-oncogene, polycomb ring finger. |
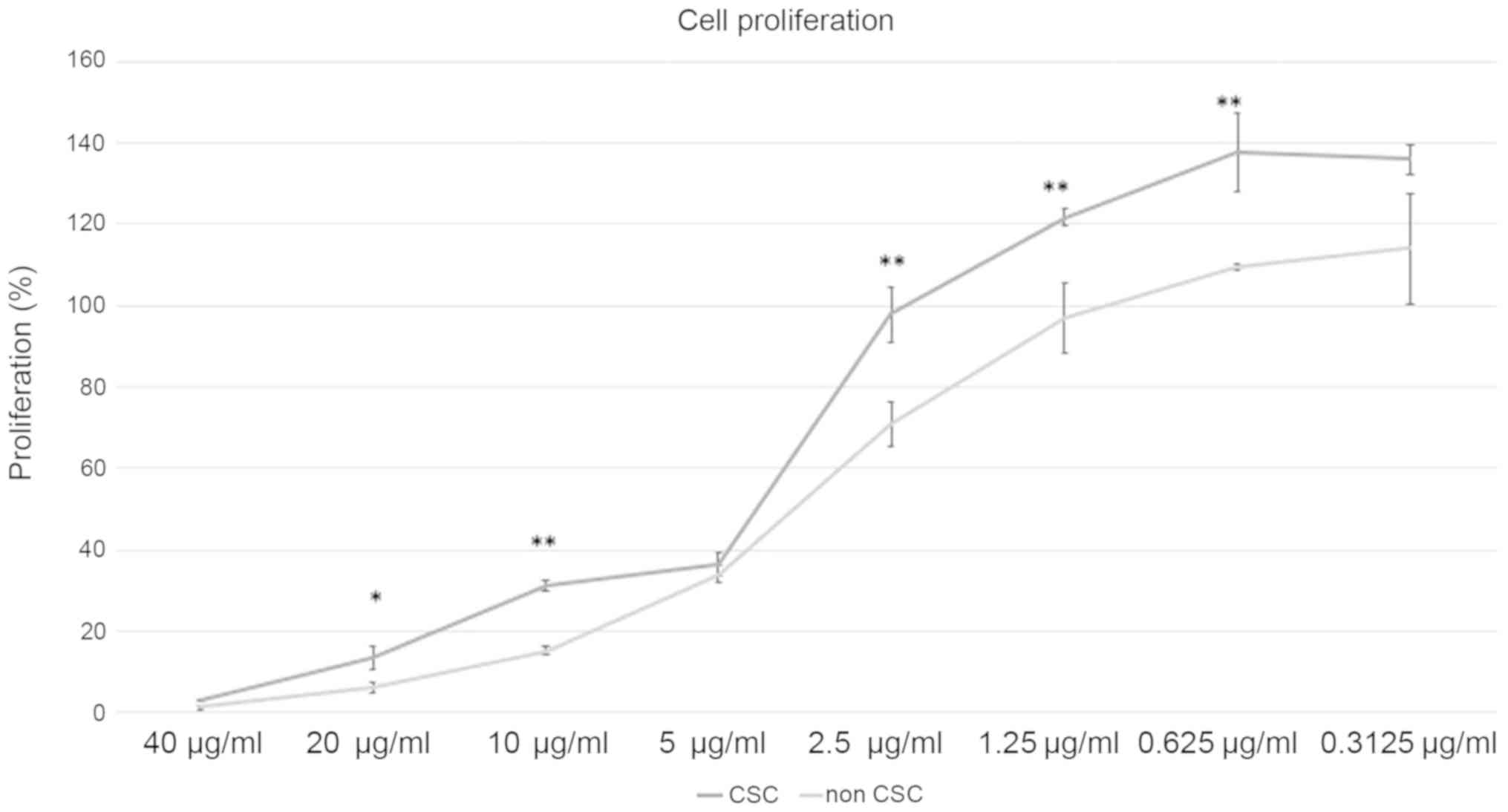
Effect of Cisplatin treatment to CSC
and nonCSC
As CSC are thought to be resistant to
chemotherapeutics we confirmed their proliferation compared to
nonCSC after cisplatin treatment. We applied different doses of
cisplatin between 40 to 0.3125 µg/ml. Our results displayed CSC to
be more resistant to cisplatin (Fig.
4). For 20, 10, 2.5, 1.25, 0.625 µg/ml cisplatin treatment,
cell proliferation percentages were significantly higher in CSC.
P-values for these dosages were respectively P=0.017, P=0.0006,
P=0.006, P=0.008, P=0073. For dosages of 5 and 0.3125 µg/ml cell
proliferation rates weren't significant, P=0.32 and P=0.06
respectively.
Discussion
HPV-negative cases still remain problem for the
treatment of OPC. It is known that they have different genetic
background but their resistance to chemoradiation needs to be
elucidated. Recent literature supports CSCs might be the reason of
resistance to therapy in various kinds of cancers including HNSCC
(22–25). As current anticancer therapies don't
target CSCs specifically, instead of eradicating them they may even
be expanding resistant CSC clones (16). Ionizing radiation itself can induce
CSC properties (26–28). Cisplatin as well, is thought to be
whether a chemotherapeutic that CSCs are resistant to or induces
CSC properties in various types of cancer (29–32).CSC
proportion in HPV- negative and HPV-positive HNSCC is challenging.
Based on the data of their study Tang et al (33) stated that HPV status does not
correlate with the CSC proportion of HNSCC and concluded that CSCs
are more resistant to cisplatin than nonCSCs, which is irrelevant
to HPV status. In another study investigating the effect of
irradiation on CSC subject to HPV status, it was demonstrated that
HPV-negative HNSCC cell line UM-SCC-1 had lower CSC proportion than
the HPV-positive HNSCC cell line UM-SCC-47 and after irradiation
both cell lines had elevated CSC proportion varied in course of
time, but only HPV-positive cell line displayed significant
plasticity in repopulating CSC phenotype in depleted cultures
(34). Additionally, Zhang et
al (35) demonstrated that
HPV-positive HNSCC has higher CSC population than HPV-negative
HNSCC and proposed that rather than absolute CSC number CSC
phenotype might be more important for disease aggressiveness.
Contradictorily, Vlashi et al (36) supported that HPV-negative cell lines
have a higher proportion of CSC and radiation induced
dedifferentiation of head and neck cancer cells into CSC depending
on the HPV status. In the present study we detected coherent data
of low CSC proportion in HPV-negative OPC cell line. Together with
the low proportion of CSC our data displayed significantly high
expression of CSC markers OCT4, SOX2, KLF4 and BIM1 compared to
nonCSC indicating CSC phenotype.
Recently it is known that CSC may also originate
from differentiated cells and nonCSC, and there are different
phenotypes of CSC, displaying genetic heterogeneity (37,38).
Almeida et al (39) defined
holospheres, merospheres and paraspheres in HNSCC cell lines and
suggested that CSCs with enhanced stemness and invasive potential
are a specific population that exist in holospheres. Our
morphological data also displayed highly dark and dense holospheres
of CSCs.
Aldehyde dehydrogenase 1 (ALDH1) is an informative
marker of CSC of HNSCC (40–43). In a systematic review of HNSCC, CSC
markers used in many of the studies are defined as ALDH1, CD44 and
BMI1, and in which ALDH1 is correlated tumor aggressiveness, tumor
size, presence of lymph node metastasis and tumor staging (44). Likewise, a meta-analysis declared
that ALDH1 positive patients had worse prognosis associated with
common clinicopathological features and poor prognostic factors
(45). Also, Yata et al
showed that increased ALDH1 activity HNSCC cells represent CSC
(46). We have displayed the
expression of ALDH1a expression in tumor spheres of UTSCC-60A cell
line while confirming CSC isolation.
CSC is a promising target for cancer treatment.
Macha et al (47) targeted
CSC via afitinib, a pan-EGFR-TKI, in HNSCC cell lines and showed
that afitinib inhibited formation and growth of tumor spheres which
also demonstrated significant radio-sensitization. Setúbal Destro
Rodrigues et al (48)
examined effects of Cetuximab and Erlotinib on the cell
sub-populations in HNSCC cell lines and showed that EGFR blocking
reduced cell proliferation, reduced motility of EMT-CSCs and
increased sensitivity of Epi-CSCs to chemoradiation by inducing
their differentiation. Also, the decrease of CSC marker expression,
downregulation of migration and invasion, and quiescence of
epithelial to mesenchymal transition was shown by targeting CSC in
HNSCC through novel C-terminal Hsp90 inhibitors (KU711 and KU757)
(49). Our data displayed that CSC
were more resistant to cisplatin treatment than nonCSC (Fig. 4) and for all doses except 5 and
0.3125 µg/ml cell proliferation rate was significantly higher for
CSC.
CSC studies shoulder great importance on
understanding CSC mechanism in carcinogenesis and how will this
information be translated to therapy. Even though this is a
comprehend step because of the underlying complex mechanisms and
genetic heterogeneity, recent improvements in CSC information is
promising. Eventually it can be proposed that not only targeting
cancer cells but also targeting CSC in cancer specifically is
probably an important advancement in cancer treatment.
In this study, CSC of HPV-negative OPC cell line is
characterized. It's been shown that CSC proportion is low but CSC
markers are highly expressed and CSCs are more resistant to
cisplatin treatment than nonCSC. The present study suggests that
even the proportion of CSC may be low in HPV-negative OPC, CSC
properties may be an important factor in resistance to cisplatin,
which needs further investigation to define the underlying
mechanisms.
Acknowledgements
The authors would like to thank Professor Reidar
Grenman (Department of Otorhinolaryngology-Head and Neck Surgery,
Turku University and Turku University Hospital, Turku, Finland) for
providing the UTSCC-60A cell line.
Funding
The present study was supported by a grant to MG
from the Ministry of Education, Culture, Sports, Science and
Technology of Japan (grant no. 17K11401).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
MG designed the study, acquired the data, analyzed
the data and prepared the manuscript. EG acquired the data,
analyzed the data, performed the statistical analysis and prepared
the manuscript. ST designed the study and edited the manuscript. KE
performed the statistical analysis and edited the manuscript. MH
designed the study, controlled the quality of the data and reviewed
the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Božinović K, Sabol I, Dediol E, Milutin
Gašperov N, Manojlović S, Vojtechova Z, Tachezy R and Grce M:
Genome-wide miRNA profiling reinforces the importance of miR-9 in
human papillomavirus associated oral and oropharyngeal head and
neck cancer. Sci Rep. 9:23062019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cohan DM, Popat S, Kaplan SE, Rigual N,
Loree T and Hicks WL Jr: Oropharyngeal cancer: Current
understanding and management. Curr Opin Otolaryngol Head Neck Surg.
17:88–94. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Preuss SF, Quante G, Semrau R, Mueller RP,
Klussmann JP and Guntinas-Lichius O: An analysis of surgical
complications, morbidity, and cost calculation in patients
undergoing multimodal treatment for operable oropharyngeal
carcinoma. Laryngoscope. 117:101–105. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Biktasova A, Hajek M, Sewell A, Gary C,
Bellinger G, Deshpande HA, Bhatia A, Burtness B, Judson B, Mehra S,
et al: Demethylation therapy as a targeted treatment for human
papillomavirus-associated head and neck cancer. Clin Cancer Res.
23:7276–7287. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cancer Genome Atlas Network, .
Comprehensive genomic characterization of head and neck squamous
cell carcinomas. Nature. 517:576–582. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Beck B and Blanpain C: Unravelling cancer
stem cell potential. Nat Rev Cancer. 13:727–738. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Xie X, Teknos TN and Pan Q: Are all cancer
stem cells created equal? Stem Cells Transl Med. 3:1111–1115. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bonnet D and Dick JE: Human acute myeloid
leukemia is organized as a hierarchy that originates from a
primitive hematopoietic cell. Nat Med. 3:730–737. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Al-Hajj M, Wicha MS, Benito-Hernandez A,
Morrison SJ and Clarke MF: Prospective identification of
tumorigenic breast cancer cells. Proc Natl Acad Sci USA.
100:3983–3988. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Singh SK, Hawkins C, Clarke ID, Squire JA,
Bayani J, Hide T, Henkelman RM, Cusimano MD and Dirks PB:
Identificationof human brain tumour initiating cells. Nature.
432:396–401. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ricci-Vitiani L, Pagliuca A, Palio E,
Zeuner A and De Maria R: Colon cancer stem cells. Gut. 57:538–548.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Szotek PP, Pieretti-Vanmarcke R, Masiakos
PT, Dinulescu DM, Connolly D, Foster R, Dombkowski D, Preffer F,
Maclaughlin DT and Donahoe PK: Ovarian cancer side population
defines cells with stem cell-like characteristics and Mullerian
Inhibiting Substance responsiveness. Proc Natl Acad Sci USA.
103:11154–11159. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Prince ME, Sivanandan R, Kaczorowski A,
Wolf GT, Kaplan MJ, Dalerba P, Weissman IL, Clarke MF and Ailles
LE: Identification of a subpopulation of cells with cancer stem
cell properties in head and neck squamous cell carcinoma. Proc Natl
Acad Sci USA. 104:973–978. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Albers AE, Chen C, Köberle B, Qian X,
Klussmann JP, Wollenberg B and Kaufmann AM: Stem cells in squamous
head and neck cancer. Crit Rev Oncol Hematol. 81:224–240. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Morrison R, Schleicher SM, Sun Y, Niermann
KJ, Kim S, Spratt DE, Chung CH and Lu B: Targeting the mechanisms
of resistance to chemotherapy and radiotherapy with the cancer stem
cell hypothesis. J Oncol. 12011:9418762011.
|
|
16
|
Klonisch T, Wiechec E, Hombach-Klonisch S,
Ande SR, Wesselborg S, Schulze-Osthoff K and Los M: Cancer stem
cell markers in common cancers-therapeutic implications. Trends Mol
Med. 14:450–460. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dingli D and Michor F: Successful therapy
must eradicate cancer stem cells. Stem Cells. 24:2603–2610. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Laban S, Steinmeister L, Gleißner L, Grob
TJ, Grénman R, Petersen C, Gal A, Knecht R, Dikomey E and Kriegs M:
Sorafenib sensitizes head and neck squamous cell carcinoma cells to
ionizing radiation. Radiother Oncol. 109:286–292. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Maushagen R, Reers S, Pfannerstill AC,
Hahlbrock A, Stauber R, Rahmanzadeh R, Rades D, Pries R and
Wollenberg B: Effects of paclitaxel on permanent head and neck
squamous cell carcinoma cell lines and identification of
anti-apoptotic caspase 9b. J Cancer Res Clin Oncol. 142:1261–1271.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tamagawa S, Beder LB, Hotomi M, Gunduz M,
Yata K, Grenman R and Yamanaka N: Role of miR-200c/miR-141 in the
regulation of epithelial-mesenchymal transition and migration in
head and neck squamous cell carcinoma. Int J Mol Med. 33:879–886.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Livak KJS and chmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Diehn M, Cho RW, Lobo NA, Kalisky T, Dorie
MJ, Kulp AN, Qian D, Lam JS, Ailles LE, Wong M, et al: Association
of reactive oxygen species levels and radioresistance in cancer
stem cells. Nature. 458:780–783. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
McDermott SC, Rodriguez-Ramirez C,
McDermott SP, Wicha MS and Nör JE: FGFR signaling regulates
resistance of head and neck cancer stem cells to cisplatin.
Oncotarget. 9:25148–25165. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Phi LTH, Sari IN, Yang YG, Lee SH, Jun N,
Kim KS, Lee YK and Kwon HY: Cancer stem cells (CSCs) in drug
resistance and their therapeutic implications in cancer treatment.
Stem Cells Int. 2018:54169232018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Prieto-Vila M, Takahashi RU, Usuba W,
Kohama I and Ochiya T: Drug resistance driven by cancer stem cells
and their niche. Int J Mol Sci. 18(pii): E25742017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ghisolfi L, Keates AC, Hu X, Lee DK and Li
CJ: Ionizing radiation induces stemness in cancer cells. PLoS One.
7:e436282012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gomez-Casal R, Bhattacharya C, Ganesh N,
Bailey L, Basse P, Gibson M, Epperly M and Levina V: Non-small cell
lung cancer cells survived ionizing radiation treatment display
cancer stem cell and epithelial-mesenchymal transition phenotypes.
Mol Cancer. 12:942013. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lee Y, Kim KH, Kim DG, Cho HJ, Kim Y,
Rheey J, Shin K, Seo YJ, Choi YS, Lee JI, Lee J, Joo KM and Nam DH:
FoxM1 promotes stemness and radio-resistance of glioblastoma by
regulating the master stem cell regulator sox2. PLoS One.
10:e01377032015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Barr MP, Gray SG, Hoffmann AC, Hilger RA,
Thomale J, O'Flaherty JD, Fennell DA, Richard D, O'Leary JJ and
O'Byrne KJ: Generation and characterization of cisplatin-resistant
non-small cell lung cancer cell lines displaying a stem-like
signature. PLoS One. 8:e541932013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ghosh RD, Ghuwalewala S, Das P, Mandloi S,
Alam SK, Chakraborty J, Sarkar S, Chakrabarti S, Panda CK and
Roychoudhury S: MicroRNA profiling of cisplatin-resistant oral
squamous cell carcinoma cell lines enriched with
cancer-stem-cell-like and epithelial-mesenchymal transition-type
features. Sci Rep. 6:239322016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Miyazaki H, Takahashi RU, Prieto-Vila M,
Kawamura Y, Kondo S, Shirota T and Ochiya T: CD44 exerts a
functional role during EMT induction in cisplatin-resistant head
and neck cancer cells. Oncotarget. 9:10029–10041. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Jiang P, Xu C, Zhou M, Zhou H, Dong W, Wu
X, Chen A and Feng Q: RXRα-enriched cancer stem cell-like
properties triggered by CDDP in head and neck squamous cell
carcinoma (HNSCC). Carcinogenesis. 39:252–262. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tang AL, Owen JH, Hauff SJ, Park JJ,
Papagerakis S, Bradford CR, Carey TE and Prince ME: Head and neck
cancer stem cells: The effect of HPV-an in vitro and mouse study.
Otolaryngol Head Neck Surg. 149:252–60. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Reid P, Wilson P, Li Y, Marcu LG,
Staudacher AH, Brown MP and Bezak E: In vitro investigation of head
and neck cancer stem cell proportions and their changes following
X-ray irradiation as a function of HPV status. PLoS One.
12:e01861862017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhang M, Kumar B, Piao L, Xie X, Schmitt
A, Arradaza N, Cippola M, Old M, Agrawal A, Ozer E, et al: Elevated
intrinsic cancer stem cell population in human
papillomavirus-associated head and neck squamous cell carcinoma.
Cancer. 120:992–1001. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Vlashi E, Chen AM, Boyrie S, Yu G, Nguyen
A, Brower PA, Hess CB and Pajonk F: Radiation-induced
dedifferentiation of head and neck cancer cells into cancer stem
cells depends on human papillomavirus status. Int J Radiat Oncol
Biol Phys. 94:1198–1206. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Chaffer CL, Brueckmann I, Scheel C,
Kaestli AJ, Wiggins PA, Rodrigues LO, Brooks M, Reinhardt F, Su Y,
Polyak K, et al: Normal and neoplastic nonstem cells can
spontaneously convert to a stem-like state. Proc Natl Acad Sci USA.
108:7950–7955. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Biddle A, Liang X, Gammon L, Fazil B,
Harper LJ, Emich H, Costea DE and Mackenzie IC: Cancer stem cells
in squamous cell carcinoma switch between two distinct phenotypes
that are preferentially migratory or proliferative. Cancer Res.
71:5317–5326. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Almeida LO, Guimarães DM, Squarize CH and
Castilho RM: Profiling the behavior of distinct populations of head
and neck cancer stem cells. Cancers (Basel). 8(pii): E72016.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chen YC, Chen YW, Hsu HS, Tseng LM, Huang
PI, Lu KH, Chen DT, Tai LK, Yung MC, Chang SC, et al: Aldehyde
dehydrogenase 1 is a putative marker for cancer stem cells in head
and neck squamous cancer. Biochem Biophy Res Commun. 385:307–313.
2009. View Article : Google Scholar
|
|
41
|
Sayed SI, Dwivedi RC, Katna R, Garg A,
Pathak KA, Nutting CM, Rhys-Evans P, Harrington KJ and Kazi R:
Implications of understanding cancer stem cell (CSC) biology in
head and neck squamous cell cancer. Oral Oncol. 47:237–243. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Marcato P, Dean CA, Giacomantonio CA and
Lee PW: Aldehyde dehydrogenase: Its role as a cancer stem cell
marker comes down to the specific isoform. Cell Cycle.
10:1378–1384. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Qian X, Wagner S, Ma C, Coordes A, Gekeler
J, Klussmann JP, Hummel M, Kaufmann AM and Albers AE: Prognostic
significance of ALDH1A1-positive cancer stem cells in patients with
locally advanced, metastasized head and neck squamous cell
carcinoma. J Cancer Res Clin Oncol. 140:1151–1158. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Curtarelli RB, Gonçalves JM, Dos Santos
LGP, Savi MG, Nör JE, Mezzomo LAM and Rodríguez Cordeiro MM:
Expression of cancer stem cell biomarkers in human head and neck
carcinomas: A systematic review. Stem Cell Rev. 14:769–784. 2018.
View Article : Google Scholar
|
|
45
|
Zhou C and Sun B: The prognostic role of
the cancer stem cell marker aldehyde dehydrogenase 1 in head and
neck squamous cell carcinomas: A meta-analysis. Oral Oncol.
50:1144–1148. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yata K, Beder LB, Tamagawa S, Hotomi M,
Hirohashi Y, Grenman R and Yamanaka N: MicroRNA expression profiles
of cancer stem cells in head and neck squamous cell carcinoma. Int
J Oncol. 47:1249–1256. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Macha MA, Rachagani S, Qazi AK, Jahan R,
Gupta S, Patel A, Seshacharyulu P, Lin C, Li S, Wang S, et al:
Afatinib radiosensitizes head and neck squamous cell carcinoma
cells by targeting cancer stem cells. Oncotarget. 8:20961–20973.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Setúbal Destro Rodrigues MF, Gammon L,
Rahman MM, Biddle A, Nunes FD and Mackenzie IC: Effects of
cetuximab and erlotinib on the behaviour of cancer stem cells in
head and neck squamous cell carcinoma. Oncotarget. 9:13488–13500.
2018.PubMed/NCBI
|
|
49
|
Subramanian C, Kovatch KJ, Sim MW, Wang G,
Prince ME, Carey TE, Davis R, Blagg BSJ and Cohen MS: Novel
c-terminal Heat shock protein 90 inhibitors (KU711 and Ku757) are
effective in targeting head and neck squamous cell carcinoma cancer
stem cells. Neoplasia. 19:1003–1011. 2017. View Article : Google Scholar : PubMed/NCBI
|