Introduction
Solid papillary carcinoma (SPC) is a relatively rare
but distinct clinicopathological feature of breast carcinomas with
frequent neuroendocrine differentiation, accounting for ~1% of all
breast carcinomas (1,2). Histopathologically, it is
characterised by solid and/or papillary growth patterns with
delicate fibrovascular stroma, and it may be classified as either
SPC in situ (absence of invasive lesions) or SPC invasive
(presence of invasive lesions) (1,2). It
has been established that SPCs frequently undergo neuroendocrine
differentiation detected by immunohistochemical analyses of
classical neuroendocrine markers, such as chromogranin A and
synaptophysin (1,2).
Lately, some novel neuroendocrine markers have been
used for routine histopathological diagnosis, and
insulinoma-associated protein 1 (INSM1) is one of the most notable
markers. Incidentally, INSM1 was originally identified from
a subtraction library of insulinoma. It encodes a transcription
factor with five zinc-finger motifs, essential for developing
neuroendocrine cells (3,4). The INSM1 is predominantly
expressed in the developing neuroendocrine tissues, and it is
activated by neurogenin 3, following NeuroD/β2 activation in
pancreatic endocrine cells (5).
Expression of INSM1 is suppressed by the Notch1-HES1 signalling
pathway, thereby repressing neuroendocrine differentiation
(6). Subsequently, its expression
has been reported in various neuroendocrine tumours, such as
pituitary adenoma (7), medullary
carcinoma of the thyroid (7,8),
carcinoid tumour, small and large cell neuroendocrine carcinoma of
the lung (9–11), neuroendocrine carcinoma of the
gastrointestinal tract (12), and
pancreatic neuroendocrine tumours (12,13).
Additionally, excellent sensitivity and specificity of INSM1 for
neuroendocrine differentiation in these tumours have also been
described (7–13). To date, the expression of INSM1 in
SPC has been analysed only in three reports (14–16),
with the largest case series comprising of 19 patients, which
showed that INSM1 is a useful neuroendocrine marker in SPC because
58% (11 of 19 patients) showed positive immunoreactivity (14).
The genes for α-thalassemia/mental retardation
syndrome X-linked protein (ATRX) and death domain-associated
protein (DAXX) play important roles in chromatin remodelling
at the telomeres and other genomic sites in normal tissues;
moreover, whole-exome analysis has revealed that inactivated
somatic mutations of these genes are frequently observed in
pancreatic neuroendocrine tumours (17). Subsequent studies have revealed
that loss of ATRX and DAXX is associated with chromosomal
instability and a shorter survival period in patients with
pancreatic neuroendocrine tumours (18,19).
However, the frequency of loss of ATRX and DAXX expression and its
prognostic significance in SPC patients has not yet been analysed.
Moreover, δ-like canonical Notch ligand 3 (DLL3), which plays an
important role in Notch signalling, is frequently expressed in
neuroendocrine-related tumours, such as neuroendocrine carcinomas
of the lungs (20). However, DLL-3
expression and its prognostic significance in SPC have not yet been
analysed. Therefore, the present study aimed to analyse the
immunohistochemical expression profiles of INSM1, ATRX, DAXX, and
DLL-3 in the largest series of patients with SPC of the breast
studied to date.
Materials and methods
Patient selection
We selected 39 patients with SPC, based on the
recent World Health Organization Classification of Breast Tumours
(1). The patients had
consecutively undergone surgical resections at the Department of
Surgery of the Kansai Medical University Hospital between January
2006 and December 2020.
This retrospective single-institution study was
conducted following the principles of the Declaration of Helsinki,
and the study protocol was approved by the Institutional Review
Board of the Kansai Medical University Hospital (approval
#2019059). All data are completely anonymised. The Institutional
Review Board waived the requirement for informed consent due to the
retrospective design of the study, using medical records and
archival samples without risk of identity exposure to the patients.
Moreover, the present study did not include any minors. All
information regarding this study, such as the inclusion criteria
and the opportunity to opt out, are provided through the
institutional website (https://www.kmu.ac.jp/hirakata/hospital/2671t800000136cd-att/a1642569623481.pdf).
Histopathological analysis
Surgically resected specimens were fixed with 10%
formalin at room temperature (24–48 h), sectioned (5–10 mm),
dehydrated by ethanol and xylene at room temperature, embedded in
paraffin (60°C), and stained with haematoxylin and eosin (5 min
each) at room temperature. More than two experienced pathologists
independently evaluated the histopathological features. We used the
TNM Classification of Malignant Tumours, Eighth Edition. The
histopathological grading of the invasive tumours was based on the
Nottingham histological grade (21). The Ki-67 labelling index (LI) of
invasive tumours was considered high when >20% of the neoplastic
cells were labelled because the median Ki-67 LI for invasive
carcinomas of no special type in our institute is 20%.
Immunohistochemistry
Immunohistochemical analyses of 4-micrometer
sections of whole tumour tissues containing in situ and/or
invasive regions were performed using autostainers (Ultra System,
Roche Diagnostics, or Autostainer link 48, DakoCytomation),
according to the manufacturer's instructions. Rabbit primary
polyclonal antibody against ATRX (HPA001906; Atlas Antibodies;
diluted 1:800; incubation time 20 min at room temperature), mouse
monoclonal antibody against chromogranin A (LK2H10; Cell Marque;
diluted 1:200; incubation time 20 min at room temperature), rabbit
polyclonal antibody against DAXX (HPA008736; Atlas Antibodies;
diluted 1:250; incubation time 20 min at room temperature), rabbit
monoclonal antibody against DLL3 (SP347; Roche Diagnostics;
prediluted; incubation time 20 min at room temperature), mouse
monoclonal antibody against INSM1 (A8; Santa Cruz Biotechnology;
diluted 1:50; incubation time 30 min at room temperature), and
mouse monoclonal antibody against synaptophysin (27G12; Nichirei
Bioscience; pre-diluted; incubation time 20 min at room
temperature) were used. Secondary antibody was pre-diluted (37°C)
[OptiView DAB Universal Kit (cat. no. 518-111427; Roche)]. At least
two researchers independently evaluated the immunohistochemical
staining of the tumours using the microscope (Olympus BX53). Any
tumour with >1% of neoplastic cells showing positive
immunoreactivity for chromogranin A, synaptophysin, INSM1, and DLL3
was recognised as a positive tumour. All tumour cells expressing
ATRX or DAXX were considered ATRX- or DAXX-retained, respectively,
and the ones without ATRX and/or DAXX were considered negative
cells, i.e., they had undergone loss of these markers.
Statistical analyses
All statistical analyses were performed using JMP
Start Statistics version 14.2 (Statistical Discovery Software; SAS
Institute). Associations between the two groups were evaluated
using Fisher's exact test for categorical variables and Wilcoxon's
rank test for continuous variables. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics and
immunohistochemical analyses
Table I summarises
the clinicopathological features of the study cohort. This study
comprised 39 female patients with SPC. At the initial diagnosis,
the median age was 72 years (age range: 39–87 years). The cohort
included 18 patients with SPC in situ (pathological stage 0)
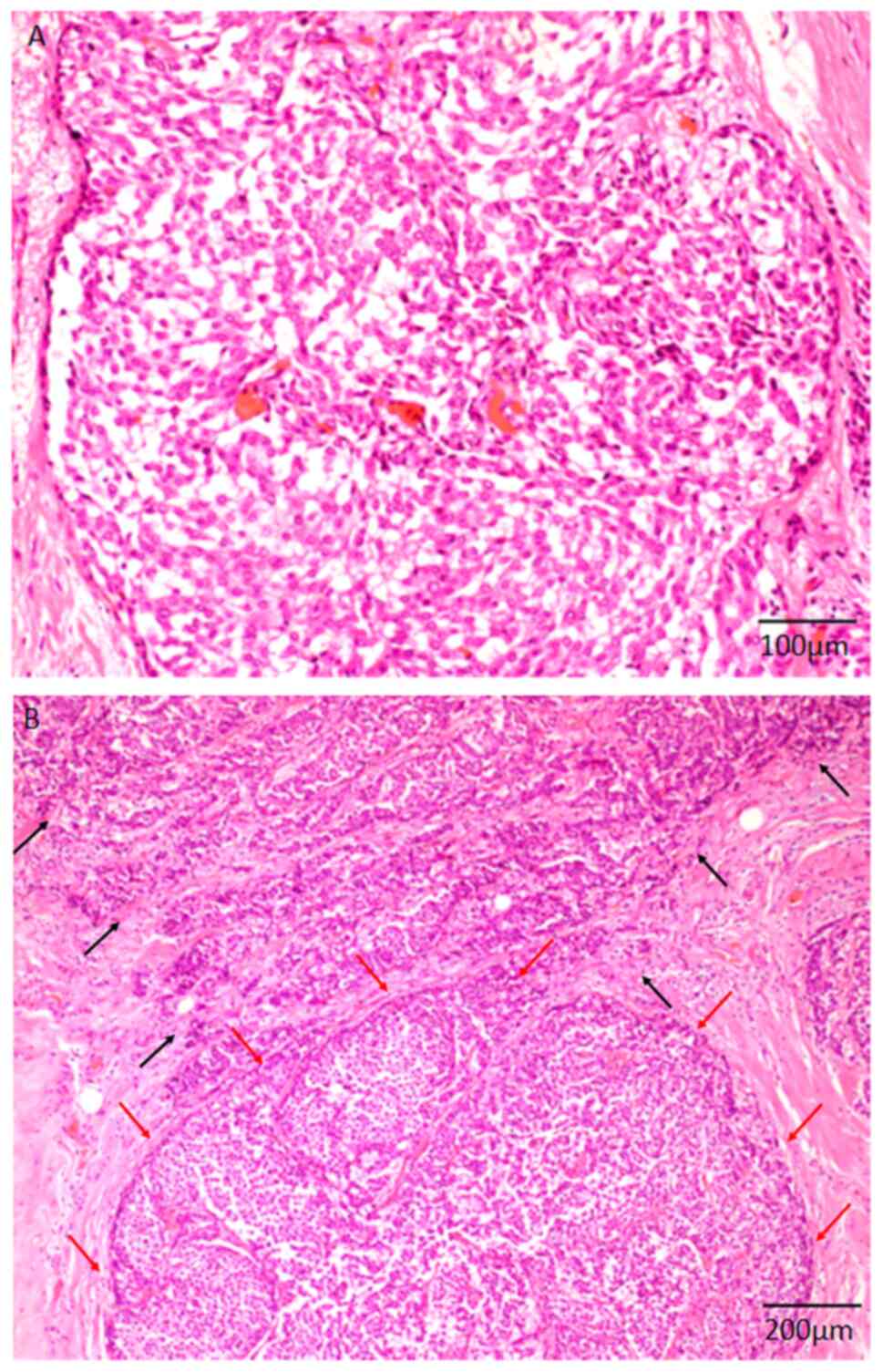
and 21 patients with SPC invasive. Typical histopathological
features of SPC in situ and SPC invasive are shown in
Fig. 1A and B, respectively. SPC
in situ composed of intraductal solid proliferation of the
neoplastic cells with slightly enlarged round nuclei and
eosinophilic cytoplasm (Fig. 1A).
Both infiltrative neoplastic growths forming irregular nests and
in situ lesions were noted in SPC invasive (Fig. 1B). Among the 18 patients with SPC
in situ, 15 had not undergone lymph node resection.
Moreover, the patients with SPC in situ were not tested for
human epidermal growth factor receptor 2 (HER2), because these
patients were not the possible candidate for anti-HER2 therapy.
Recurrence, particularly bone metastasis, was observed in only one
patient with invasive SPC. The median follow-up period was 33
months (range: 1–152 months). Table
I summarises the results of the immunohistochemical analyses of
the tumour specimens. All the tumour specimens tested positive for
oestrogen and progesterone receptors, except for one patient in the
SPC invasive group. Interestingly, HER2 was not overexpressed in
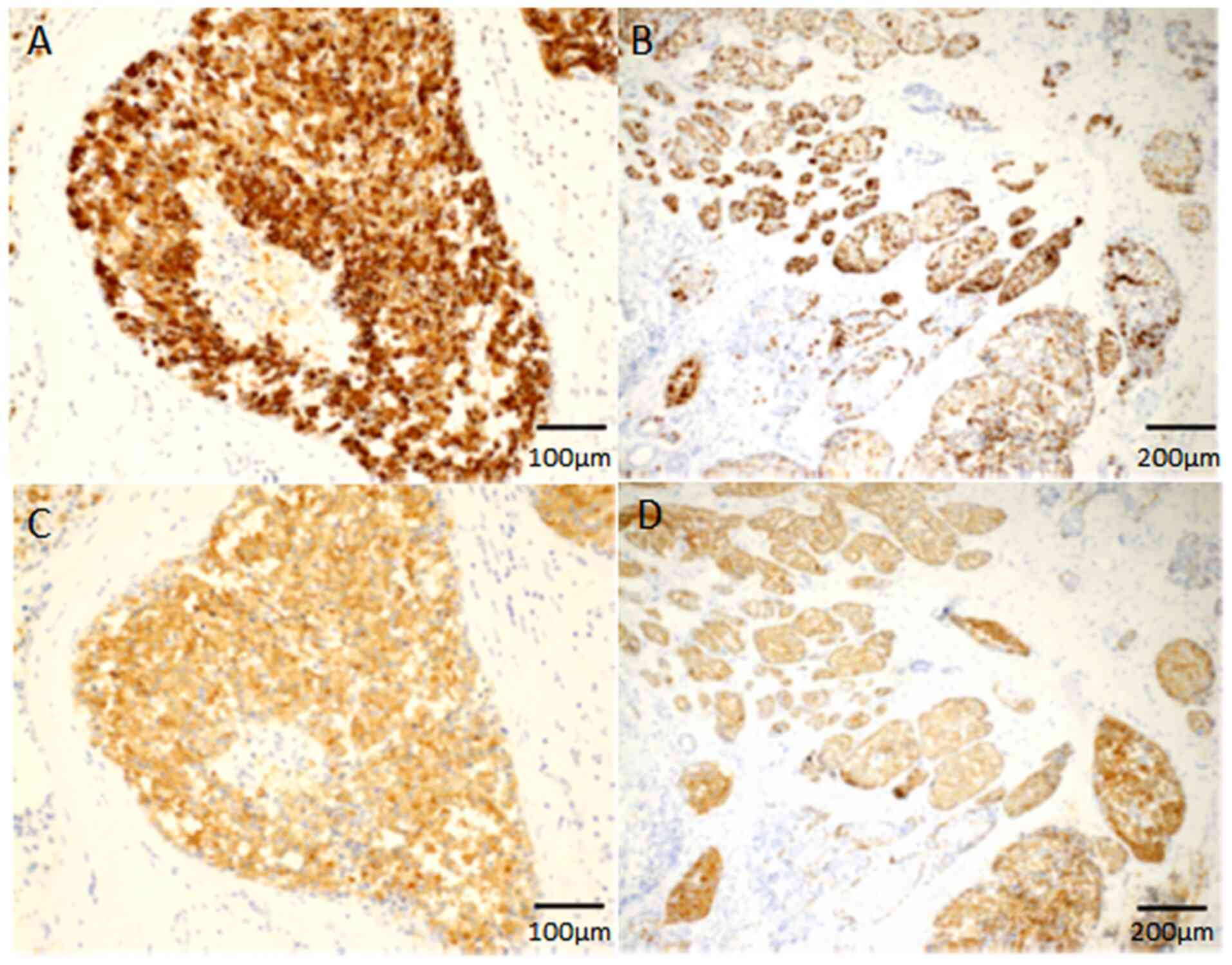
any of the samples from the SPC invasive group. Chromogranin A was
expressed in 64.1% (25 out of 39) of in situ and invasive
lesions (Fig. 2A and B), whereas
synaptophysin was expressed in all samples of in situ and
invasive lesions (Fig. 2C and D).
INSM1 expression was noted in 92.3% (36 out of 39) of in
situ and some of the invasive lesions (Fig. 3A and B). Each of ATRX and DAXX
expression was retained in 28.2% (11 out of 39) of in situ
lesions, and some invasive neoplastic cells showed loss of nuclear
immunoreactivity of ATRX or DAXX (Fig.
3C-F), whereas none of the patients showed positive
immunoreactivity for DLL3 (Fig.
3G).
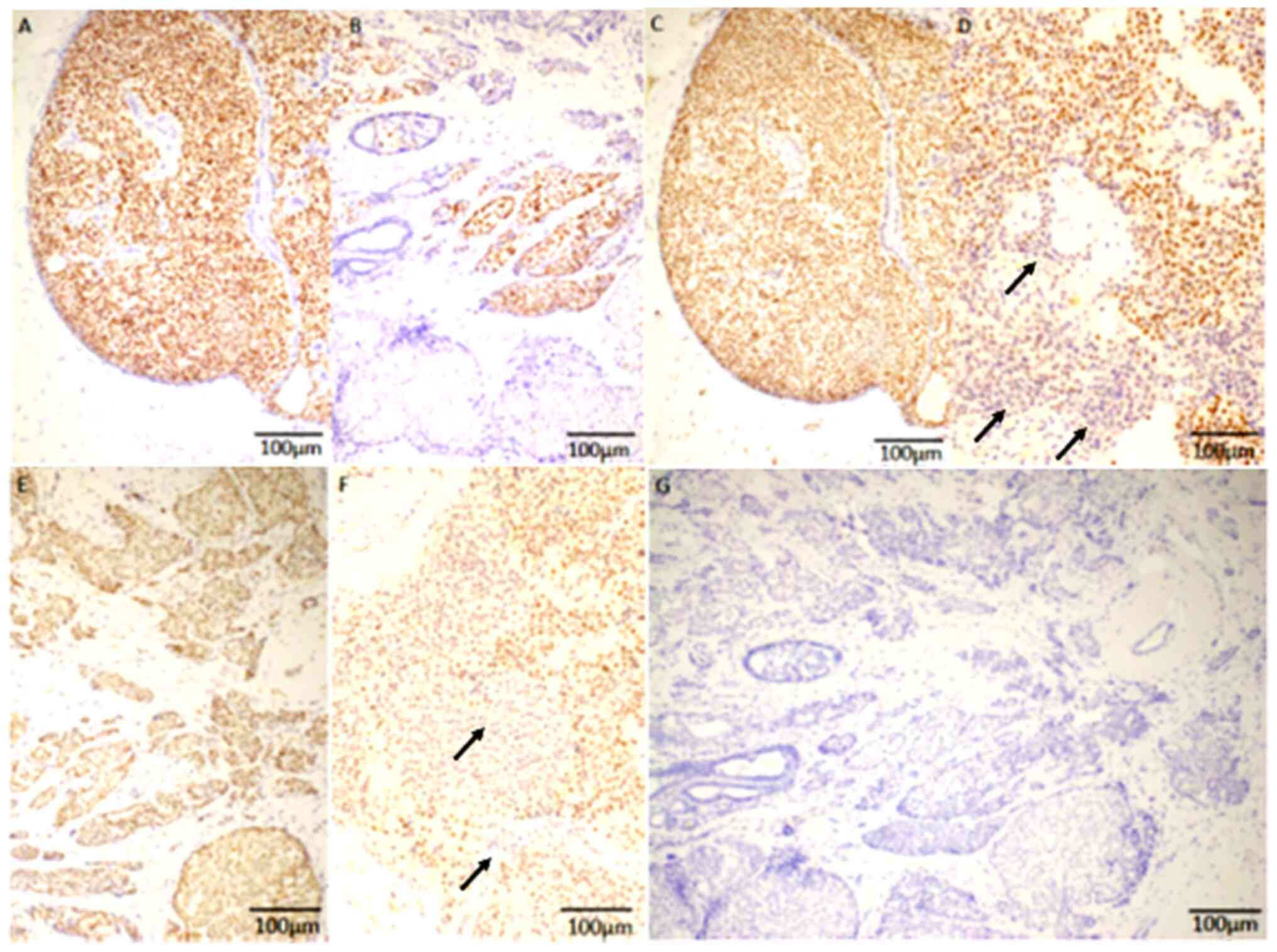 | Figure 3.INSM1, ATRX, DAXX and DLL3 expression
in SPC. (A) Diffuse nuclear expression of INSM1 is noted in SPC
in situ. (B) Some invasive neoplastic cells show positive
nuclear immunoreactivity (brown stain) for INSM1. (C) Retained
nuclear expression of ATRX is noted in the SPC in situ
group. (D) Some invasive neoplastic cells show loss of nuclear
immunoreactivity for ATRX (arrows). (E) Retained nuclear expression
of DAXX is noted in the SPC invasive group. (F) Some of the
invasive neoplastic cells show loss of nuclear immunoreactivity for
DAXX (arrows). (G) None of the samples suggested positive
expression for DLL3. Magnification, ×200; scale bars, 100 µm.
INSM1, Insulinoma-associated protein 1; DAXX, death domain
associated protein; ATRX, α-thalassemia/mental retardation syndrome
X-linked protein; SPC, solid papillary carcinoma; DLL3, δ-like
canonical notch ligand 3; SPC, solid papillary carcinoma. |
 | Table I.Clinicopathological characteristics of
patients with SPC. |
Table I.
Clinicopathological characteristics of
patients with SPC.
| Factors | n | % |
|---|
| Total number of
subjects | 39 |
|
| Median age, years
(range) | 72.0 (39–87) |
|
| Menopausal
status |
|
|
|
Premenopausal | 4 | 10.3 |
|
Postmenopausal | 34 | 87.2 |
|
Unknown | 1 | 2.6 |
| Median body mass
index, kg/m2 (range) | 23.8 (16.4-34.9) |
|
| Median tumor size of
the invasive component, mm (range) | 1 (0–45) |
|
| Pathological
stage |
|
|
| 0 | 18 | 46.2 |
| I | 15 | 38.5 |
|
IIA | 4 | 10.3 |
|
IIB | 2 | 5.1 |
|
IIIA | 0 | 0.0 |
|
IIIB | 0 | 0.0 |
|
IIIC | 0 | 0.0 |
| Lymph node
status |
|
|
|
Positive | 3 | 7.7 |
|
Negative | 21 | 53.8 |
| Not
tested | 15 | 38.5 |
| Lymphatic
invasion |
|
|
|
Positive | 6 | 15.4 |
|
Negative | 33 | 84.6 |
| Venous
invasion |
|
|
|
Positive | 3 | 7.7 |
|
Negative | 36 | 92.3 |
| Nottingham
histological grade (SPC invasive) |
|
|
| 1 | 5 | 12.8 |
| 2 | 12 | 30.8 |
| 3 | 4 | 10.3 |
| Ki-67 labeling
index (SPC invasive) |
|
|
|
>20% | 7 | 17.9 |
|
≤20% | 14 | 35.9 |
| Estrogen
receptor |
|
|
|
Positive | 38 | 97.4 |
|
Negative | 1 | 2.6 |
| Progesterone
receptor |
|
|
|
Positive | 38 | 97.4 |
|
Negative | 1 | 2.6 |
| Human epidermal
growth factor receptor 2 |
|
|
|
Positive | 0 | 0.0 |
|
Negative | 21 | 53.8 |
| Synaptophysin |
|
|
|
Positive | 39 | 100.0 |
|
Negative | 0 | 0.0 |
| Chromogranin A |
|
|
|
Positive | 25 | 64.1 |
|
Negative | 14 | 35.9 |
|
Insulinoma-associated protein 1 |
|
|
|
Positive | 36 | 92.3 |
|
Negative | 3 | 7.7 |
|
Α-thalassemia/mental retardation syndrome
X-linked protein |
|
|
|
Retained | 11 | 28.2 |
|
Lost | 28 | 71.8 |
| Death domain
associated protein |
|
|
|
Retained | 11 | 28.2 |
|
Lost | 28 | 71.8 |
| Δ-like canonical
Notch ligand 3 |
|
|
|
Positive | 0 | 0.0 |
|
Negative | 39 | 100.0 |
| Recurrence |
|
|
| No
recurrence | 38 | 97.4 |
|
Recurred | 1 | 2.6 |
Association between
clinicopathological factors and the expression of chromogranin A,
synaptophysin, and INSM1
Table II
summarises the associations between the clinicopathological factors
observed in patients with SPC and the expression of chromogranin A,
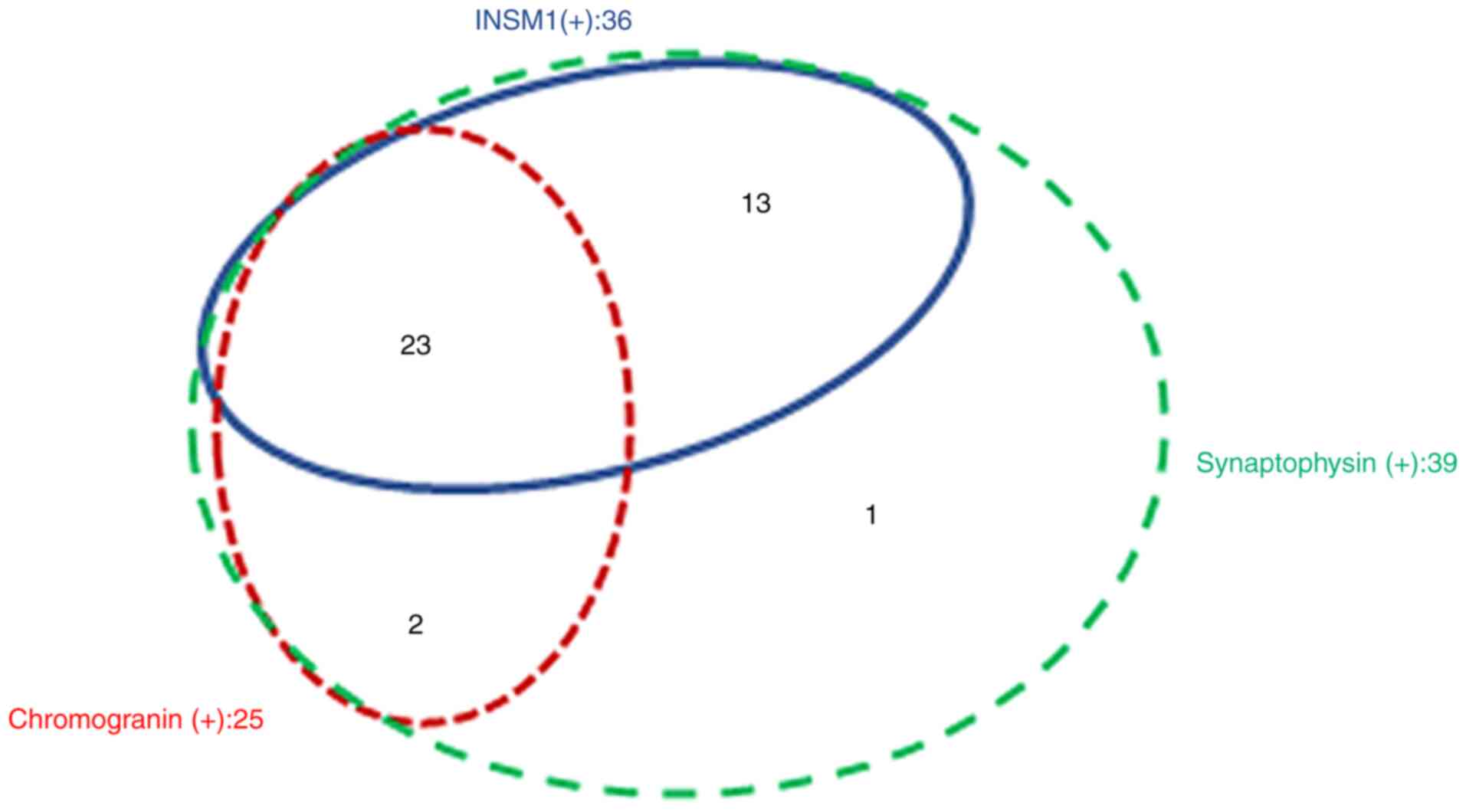
synaptophysin, and INSM1. The distribution of these three markers
is shown in Fig. 4. Among the 39
patients, 23 showed positive immunoreactivity for all three
markers, while the remaining 16 lacked expression of more than one
marker (Fig. 4). The advanced
pathological stages and body mass index were significantly
correlated with the lack of expression of either INSM1 or
chromogranin A (P=0.033 and 0.049, respectively). By contrast,
other clinicopathological factors, including the presence of
invasive tumours, were not significantly correlated with the lack
of expression of INSM1 or chromogranin A. Moreover, the sample from
only patient who showed recurrence tested negative for chromogranin
A and INSM1.
| Table II.Associations between
clinicopathological factors and the expressions of chromogranin A,
synaptophysin and INSM1. |
Table II.
Associations between
clinicopathological factors and the expressions of chromogranin A,
synaptophysin and INSM1.
| Factors | Chromogranin A,
synaptophysin, and INSM1-positive (n=23) | Chromogranin A,
synaptophysin, or INSM1-negative (n=16) | P-value |
|---|
| Median age, years ±
SD | 70.0±13.7 | 72.0±9.1 | 0.764 |
| Menopausal
status |
|
| 0.124 |
|
Premenopausal | 4 | 0 |
|
|
Postmenopausal | 18 | 16 |
|
|
Unknown | 1 | 0 |
|
| Median body mass
index, kg/m2±SD | 24.3±4.1 | 23.1±2.9 | 0.049 |
| SPC in situ
or invasive |
|
| 0.516 |
| SPC
invasive | 11 | 10 |
|
| SPC
in situ | 12 | 6 |
|
| Pathological
stage |
|
| 0.033 |
|
0+I | 22 | 11 |
|
| II | 1 | 5 |
|
| Lymph node
status |
|
| >0.999 |
|
Positive | 1 | 2 |
|
|
Negative | 11 | 10 |
|
| Not
tested | 11 | 4 |
|
| Estrogen
receptor |
|
| >0.999 |
|
Positive | 22 | 16 |
|
|
Negative | 1 | 0 |
|
| Progesterone
receptor |
|
| >0.999 |
|
Positive | 22 | 16 |
|
|
Negative | 1 | 0 |
|
Table III
summarises the associations between the clinicopathological factors
of the patients in the SPC invasive group and the expression of
chromogranin A, synaptophysin, and INSM1. Incidentally, the lack of
chromogranin A or INSM1 expression in the invasive component was
significantly associated with a higher pathological stage (P=0.012)
and a tendency for advanced histological grade and high Ki-67 LI,
but the difference was not significant (P=0.090 and 0.064,
respectively).
| Table III.Associations between the
clinicopathological factors of patients in the solid papillary
carcinoma invasive group and expression of chromogranin A,
synaptophysin, and INSM1. |
Table III.
Associations between the
clinicopathological factors of patients in the solid papillary
carcinoma invasive group and expression of chromogranin A,
synaptophysin, and INSM1.
| Factors | Chromogranin A,
synaptophysin, and INSM1-positive (n=10) | Chromogranin A,
synaptophysin, or INSM1-negative (n=11) | P-value |
|---|
| Pathological
stage |
|
| 0.012 |
| I | 10 | 5 |
|
| II | 0 | 6 |
|
| Lymphatic
invasion |
|
| 0.149 |
|
Positive | 1 | 5 |
|
|
Negative | 9 | 6 |
|
| Venous
invasion |
|
| >0.999 |
|
Positive | 1 | 2 |
|
|
Negative | 9 | 9 |
|
| Nottingham
histological grade |
|
| 0.090 |
|
1+2 | 10 | 7 |
|
| 3 | 0 | 4 |
|
| Ki-67 labelling
index (%) |
|
| 0.064 |
| High
(>20) | 1 | 6 |
|
| Low
(≤20) | 9 | 5 |
|
Association between
clinicopathological factors and the expression of ATRX and
DAXX
Table IV
summarises the association between the clinicopathological factors
of the patients with SPC and the expression of ATRX and DAXX. Among
the 39 patients, samples from eight had retained both ATRX and DAXX
expression, while those of the remaining 31 showed loss of ATRX
and/or DAXX expression. Although the median age of the patients
with loss of ATRX and/or DAXX was significantly higher than that of
the patients who had retained the expression of ATRX and DAXX,
there were no significant differences between the groups, even for
the presence of invasive tumours. Moreover, the only patient to
show recurrence exhibited loss of ATRX and/or DAXX.
| Table IV.Association between
clinicopathological factors and the expressions of ATRX and
DAXX. |
Table IV.
Association between
clinicopathological factors and the expressions of ATRX and
DAXX.
| Factors | ATRX- and
DAXX-retained (n=8) | ATRX- and/or
DAXX-loss (n=31) | P-value |
|---|
| Median age, years ±
SD | 62.5±13.9 | 72.0±10.3 | 0.016 |
| Menopausal
status |
|
| 0.189 |
|
Premenopausal | 2 | 2 |
|
|
Postmenopausal | 6 | 28 |
|
|
Unknown | 0 | 1 |
|
| Median body mass
index, kg/m2±SD | 24.0±3.8 | 23.8±3.9 | 0.702 |
| SPC in situ
or invasive |
|
| 0.702 |
| SPC
invasive | 5 | 16 |
|
| SPC
in situ | 3 | 15 |
|
| Pathological
stage |
|
| >0.999 |
|
0+I | 7 | 26 |
|
| II | 1 | 5 |
|
| Lymph node
status |
|
| >0.999 |
|
Positive | 1 | 2 |
|
|
Negative | 5 | 16 |
|
| Not
tested | 2 | 13 |
|
| Estrogen
receptor |
|
| 0.205 |
|
Positive | 7 | 31 |
|
|
Negative | 1 | 0 |
|
| Progesterone
receptor |
|
| 0.205 |
|
Positive | 7 | 31 |
|
|
Negative | 1 | 0 |
|
Table V summarises
the association between the clinicopathological factors of the
patients in the SPC invasive group and ATRX and DAXX expression.
Among the 21 patients, nine had retained both ATRX and DAXX
expression in the invasive component, while the remaining 12 showed
loss of ATRX and/or DAXX expression in the invasive component. The
presence of lymphatic invasion was significantly correlated with
the loss of ATRX and/or DAXX expression (P=0.019). However, the
Nottingham histological grade and Ki-67 LI were not significantly
different between the two groups.
| Table V.Association between
clinicopathological factors of patients in the SPC invasive group
and the expression of ATRX and DAXX. |
Table V.
Association between
clinicopathological factors of patients in the SPC invasive group
and the expression of ATRX and DAXX.
| Factors | ATRX- and
DAXX-retained (n=9) | ATRX- and/or
DAXX-loss (n=12) | P-value |
|---|
| Lymphatic
invasion |
|
| 0.019 |
|
Positive | 0 | 6 |
|
|
Negative | 9 | 6 |
|
| Venous
invasion |
|
|
|
|
Positive | 1 | 2 | >0.999 |
|
Negative | 8 | 10 |
|
| Nottingham
histological grade |
|
|
|
|
1+2 | 9 | 8 | 0.104 |
| 3 | 0 | 4 |
|
| Ki-67 labeling
index (%) |
|
|
|
| High
(>20) | 2 | 5 | 0.642 |
| Low
(≤20) | 7 | 7 |
|
Discussion
In the present study, we demonstrated that INSM1 is
a useful neuroendocrine marker for diagnosing breast SPC, and it
might even be superior to chromogranin A (positive rates were 92.3
and 64.1% for INSM1 and chromogranin A, respectively).
Additionally, the lack of INSM1 or chromogranin A expression was
significantly correlated with an advanced pathological stage in
patients with SPC, and in patients with invasive SPC, it showed a
significant association of a higher pathological stage and a
tendency to be associated with high Ki-67 LI and advanced
histological grade. Moreover, the loss of ATRX or DAXX expression
was significantly correlated with the presence of lymphatic
invasion.
Incidentally, INSM1 has been recognised as a useful
and specific neuroendocrine marker because it is an essential
transcription factor for developing normal neuroendocrine cells
wherein its expression is highly restricted (3–5).
Previously several reports have concluded that INSM1 expression is
specific to various neuroendocrine tumours (7–13).
Furthermore, SPC is a distinct clinicopathological feature of
breast carcinoma that frequently shows neuroendocrine
differentiation; SPC shows frequent positive immunoreactivity for
chromogranin A and synaptophysin (1,2).
However, to the best of our knowledge, only three studies have
addressed the expression of INSM1 in SPCs (14–16).
According to a previous report, INSM1 expression was noted in 11
out of 19 patients with SPC (2 of 3 SPC in situ, and nine of
16 SPC invasive). Among these 19 patients with SPC, 11 tested
positive for synaptophysin and/or chromogranin A, while the
remaining eight were synaptophysin- and chromogranin A-negative.
Positive INSM1 expression was noted in nine of the 11
above-mentioned neuroendocrine marker-positive patients and two of
the eight neuroendocrine marker-negative patients (14). Additionally, another report showed
that eight out of eight (including one patient without
synaptophysin and chromogranin A expression) patients showed
positive INSM1 expression (15)
(INSM1 expression rate in SPC was not available in the remaining
report (16)). The current study
includes the analysis of the largest series of SPCs for INSM1
expression, and it shows that 92.3% (36 of 39) of the patients
tested positive for INSM1 expression. According to these results,
it may be suggested that although INSM1 is a useful neuroendocrine
marker, neuroendocrine differentiation in SPCs might not be defined
by only INSM1 (14). Therefore, a
combination of classical neuroendocrine markers and INSM1 might be
useful for detecting neuroendocrine differentiation in SPCs because
INSM1 may be expressed in patients with luminal B breast cancer,
even if samples test negative for chromogranin A and synaptophysin
(22). Moreover, this study
demonstrated for the first time that the lack of INSM1 or
chromogranin A expression is significantly correlated with an
advanced pathological stage in patients with SPC, and it is
associated with a significant higher pathological stage and a
tendency toward high Ki-67 LI and advanced histological grade in
patients with invasive SPC. Hence, examining INSM1, chromogranin A,
and synaptophysin expression might be useful for analysing the
characteristics of tumour cells in SPCs. A previous study
demonstrated that NOTCH 1 expression was absent in SPC (14), which corresponded to the fact that
INSM1 is essential for neuroendocrine differentiation, and Notch 1
negatively regulates neuroendocrine differentiation (6,14).
Moreover, DLL3 plays an important role and is considered an
autonomous inhibitor of Notch signalling, and SPCs show positive
immunoreactivity for Notch 2 and Notch 3 (14,20).
DLL3 expression was not detected in all patients with SPC in the
present cohort, consistent with the results of a previous study
(23). Although the detailed
mechanism regarding the relationship among DLL3, Notch 2, and Notch
3 expression is unknown, lack of DLL3 expression in SPC might be
related to the expression of Notch 2 and Notch 3.
If the expression of ATRX and DAXX is retained, then
the prognosis of patients with pancreatic neuroendocrine tumours is
improved (18,19). This study is the first to address
the expression of these two markers in patients with SPC. However,
in the present cohort, we observed that the loss of ATRX or DAXX
expression is significantly correlated with the presence of
lymphatic invasion, but not with an advanced histological grade or
a high Ki-67 LI. Loss of ATRX or DAXX expression is associated with
chromosomal instability and poor survival in patients with
pancreatic neuroendocrine tumours (18). Therefore, a significant presence of
lymphatic invasion in the present cohort might be related to poor
survival in pancreatic neuroendocrine tumours (18). However, the present study did not
analyse the prognosis of patients.
There are several limitations to the present study.
First, this study was a retrospective single-centre analysis, which
could have led to a selection bias; however, this is the largest
series of patients with SPC studied to date. Second, this study
included only one patient with recurrence, even though SPC is
recognised as an indolent breast cancer and metastasis and/or
recurrence is relatively rare (1).
Therefore, the prognostic significance of INSM1, ATRX, and DAXX
expression is difficult to determine. Third, synaptophysin was
expressed in all patients with SPC in the present cohort. However,
synaptophysin expression may sometimes be lost (2,14),
and the rate of INSM1 expression is different between
synaptophysin- and/or chromogranin A-positive and synaptophysin-
and chromogranin A-negative SPC patients (14). Hence, the expression of ATRX and
DAXX might be different between these two groups. Accordingly,
additional studies must be performed with larger series of patients
with SPC than the present study, who may/may not show metastasis
and may test positive or negative for chromogranin A and/or
synaptophysin. This will help analyse the clinical significance of
the expression of these markers.
In conclusion, we studied the largest series of SPCs
to date and demonstrated that INSM1 is a useful neuroendocrine
marker for SPCs of the breast, and it might even be superior to
chromogranin A. Furthermore, the lack of INSM1 or chromogranin A
expression is significantly correlated with advanced pathological
stages in patients with SPC. There is a significant association
between a higher pathological stage and a tendency toward high
Ki-67 LI and an advanced stage histological grade in patients with
invasive SPC. However, loss of ATRX or DAXX expression, both of
which are useful prognostic markers for patients with pancreatic
neuroendocrine tumours, is significantly correlated with the
presence of lymphatic invasion. Additional studies with larger
cohorts are needed to determine the clinical significance of the
expression of these markers.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated and analysed in the present study
are included in this published article.
Authors' contributions
HY and MI conceived and designed the study and
performed the immunohistochemical analyses. HY, MI, KY, KT, MS and
TS acquired and analysed the data. HY and MI confirmed the
authenticity of all the raw data. HY and MI drafted the manuscript,
tables and figures. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
This retrospective single-institution study was
conducted in accordance with the principles of the Declaration of
Helsinki, and the study protocol was approved by the Institutional
Review Board of the Kansai Medical University Hospital (approval
no. 2019059; Hirakata, Japan). All data are completely anonymized.
The Institutional Review Board waived the requirement of informed
consent due to the retrospective design of the study, using medical
records and archival samples with no risk of identity exposure for
the patients. Moreover, the present study did not include any
minors.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ATRX
|
α-thalassemia/mental retardation
syndrome X-linked protein
|
|
DAXX
|
death domain-associated protein
|
|
DLL3
|
δ-like canonical notch ligand 3
|
|
INSM1
|
insulinoma-associated protein 1
|
|
LI
|
labelling index
|
|
SPC
|
solid papillary carcinoma
|
References
|
1
|
Mac Grogan G, Collins LC, Lerwill M, Rakha
EA and Tan BY: Solid papillary carcinoma (in situ and invasive).
WHO Classification of Tumours. 5th edition. Breast Tumours IARC;
Lyon: pp. 63–65. 2019
|
|
2
|
Otsuki Y, Yamada M, Shimizu S, Suwa K,
Yoshida M, Tanioka F, Ogawa H, Nasuno H, Serizawa A and Kobayashi
H: Solid-papillary carcinoma of the breast: Clinicopathological
study of 20 cases. Pathol Int. 57:421–429. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Goto Y, De Silva MG, Toscani A, Prabhakar
BS, Notkins AL and Lan MS: A novel human insulinoma-associated
cDNA, IA-1, encodes a protein with ‘zinc-finger’ DNA-binding
motifs. J Biol Chem. 267:15252–15257. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gierl MS, Karoulias N, Wende H, Strehle M
and Birchmeier C: The zinc-finger factor Insm1 (IA-1) is essential
for the development of pancreatic beta cells and intestinal
endocrine cells. Genes Dev. 20:2465–2478. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lan MS and Breslin MB: Structure,
expression, and biological function of INSM1 transcription factor
in neuroendocrine differentiation. FASEB J. 23:2024–2033. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jia S, Wildner H and Birchmeier C: Insm1
controls the differentiation of pulmonary neuroendocrine cells by
repressing Hes1. Dev Biol. 408:90–98. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rooper LM, Bishop JA and Westra WH: INSM1
is a sensitive and specific marker of neuroendocrine
differentiation in head and neck tumors. Am J Surg Pathol.
42:665–671. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Seok JY, Kang M, De Peralta-Venturina M
and Fan X: Diagnostic utility of INSM1 in medullary thyroid
carcinoma. Int J Surg Pathol. 29:615–626. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dermawan JK and Mukhopadhyay S:
Insulinoma-associated protein 1 (INSM1) differentiates carcinoid
tumourlets of the lung from pulmonary meningothelial-like nodules.
Histopathology. 72:1067–1069. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sakakibara R, Kobayashi M, Takahashi N,
Inamura K, Ninomiya H, Wakejima R, Kitazono S, Yanagitani N,
Horiike A, Ichinose J, et al: Insulinoma-associated Protein 1
(INSM1) is a better marker for the diagnosis and prognosis
estimation of small cell lung carcinoma than neuroendocrine
phenotype markers such as chromogranin A, synaptophysin, and CD56.
Am J Surg Pathol. 44:757–764. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mukhopadhyay S, Dermawan JK, Lanigan CP
and Farver CF: Insulinoma-associated protein 1 (INSM1) is a
sensitive and highly specific marker of neuroendocrine
differentiation in primary lung neoplasms: An immunohistochemical
study of 345 cases, including 292 whole-tissue sections. Mod
Pathol. 32:100–109. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
González I, Lu HC, Sninsky J, Yang C,
Bishnupuri K, Dieckgraefe B, Cao D and Chatterjee D:
Insulinoma-associated protein 1 expression in primary and
metastatic neuroendocrine neoplasms of the gastrointestinal and
pancreaticobiliary tracts. Histopathology. 75:568–577. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tanigawa M, Nakayama M, Taira T, Hattori
S, Mihara Y, Kondo R, Kusano H, Nakamura K, Abe Y, Ishida Y, et al:
Insulinoma-associated protein 1 (INSM1) is a useful marker for
pancreatic neuroendocrine tumor. Med Mol Morphol. 51:32–40. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kudo N, Takano J, Kudoh S, Arima N and Ito
T: INSM1 immunostaining in solid papillary carcinoma of the breast.
Pathol Int. 71:51–59. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Seijnhaeve E, Galant C and Van Bockstal
MR: Nuclear insulinoma-associated Protein 1 expression as a marker
of neuroendocrine differentiation in neoplasms of the breast. Int J
Surg Pathol. 29:496–502. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Metovic J, Castellano I, Marinelli E,
Osella-Abate S, Sapino A, Cassoni P and Papotti M: INSM1 expression
in breast neoplasms with neuroedocrine features. Endocr Pathol.
32:452–460. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Jiao Y, Shi C, Edil BH, de Wilde RF,
Klimstra DS, Maitra A, Schulick RD, Tang LH, Wolfgang CL, Choti MA,
et al: DAXX/ATRX, MEN1, and mTOR pathway genes are frequently
altered in pancreatic neuroendocrine tumors. Science.
331:1199–1203. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Marinoni I, Kurrer AS, Vassella E, Dettmer
M, Rudolph T, Banz V, Hunger F, Pasquinelli S, Speel EJ and Perren
A: Loss of DAXX and ATRX are associated with chromosome instability
and reduced survival of patients with pancreatic neuroendocrine
tumors. Gastroenterology. 146:453–460. e52014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang F, Xu X, Ye Z, Qin Y, Yu X and Ji S:
Prognostic significance of altered ATRX/DAXX gene in pancreatic
neuroendocrine tumors: A meta-analysis. Front Endocrinol
(Lausanne). 12:6915572021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Matsuo K, Taniguchi K, Hamamoto H, Inomata
Y, Komura K, Tanaka T, Lee SW and Uchiyama K: Delta-like canonical
Notch ligand 3 as a potential therapeutic target in malignancies: A
brief overview. Cancer Sci. 112:2984–2992. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I. The value of histological
grade in breast cancer: Experience from a large study with
long-term follow-up. C.W. Elston & I O Ellis Histopathology
1991; 19.403-410. Histopathology. 41((3A)): 151–152; discussion
152–3. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Razvi H, Tsang JY, Poon IK, Chan SK,
Cheung SY, Shea KH and Tse GM: INSM1 is a novel prognostic
neuroendocrine marker for luminal B breast cancer. Pathology.
53:170–178. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vranic S, Palazzo J, Sanati S, Florento E,
Contreras E, Xiu J, Swensen J and Gatalica Z: Potential novel
therapy targets in neuroendocrine carcinomas of the breast. Clin
Breast Cancer. 19:131–136. 2019. View Article : Google Scholar : PubMed/NCBI
|