Introduction
Mediopatellar plica (MP) in the knee is the synovial
structure of the knee joint cavity that is derived from embryonic
mesenchymal tissues without full absorption during embryonic
development. In arthroscopy and autopsy studies, the incidence rate
of MP was 19–70%, of which 1/8 to 1/10 had pathological MP with
pain in the patellofemoral joint (1).
Typical symptoms include painful locking within the joint and
chronic patellofemoral intermittent dull pain, which became severe
in up and downstairs movements and when sedentary. These symptoms
are not usually associated with knee effusions or swelling
(2–4).
The anatomic structure, and physiological and
pathological mechanisms in MP that may lead to pain remain to be
elucidated. The possible reasons for causes of patellofemoral pain
include: i) MP may have changed the normal biomechanic distribution
of the patellofemoral joint and physiological load of the
patellofemoral joint cartilage, leading to the stress increase of
partial articular cartilage and subchondral bone, which resulted in
localized cartilage damage and pain. The nociceptors that were
isolated from cartilage under the patella bone can provide a
theoretical basis for this hypothesis (5). ii) Patellofemoral pain may come from the
joint capsule, subchondral bone, patellar fat pad, retinaculum,
cartilage, the patellar tendon and synovial plica (5–8). Stimulated
by trauma and other chronic inflammatory factors, localized
hemorrhage may occur in the MP followed by fibrosis, thickening of
the synovial tissue, inflammation and long-term recurrent chronic
impact, which leads to patellofemoral pain (9). Substance-P (SP) is an undecapeptide that
functions as a neurotransmitter and a neuromodulator. This peptide
is widely distributed throughout the central and peripheral nervous
systems. There is substantial evidence that neuropeptide SP is
involved in neurogenic inflammation. Macrophages can be activated
by SP, provoking the release of inflammatory compounds. The release
of these chemical mediators is crucial for inflammatory response.
SP appears to have a major role in the development and maintenance
of pain and inflammation, and high levels of the neuropeptide are
associated with pain and persistent inflammation.
Therefore, we hypothesized that the increase of the
distribution of nerve fibers in symptomatic MP and its expression
of neuropeptide had a close correlation to the occurrence and
sustenance of pain. In the present study, immunohistochemistry was
used to investigate SP expression levels in MP. Semi-quantitative
analysis was utilized to compare the expression difference of SP in
asymptomatic plica and symptomatic plica with patellofemoral pain,
and the association between SP expression and patellofemoral pain
was discussed.
Materials and methods
Reagent
The rabbit anti-human SP polyclonal
antibody/fluorescein isothiocyanate labeled goat anti-rabbit
immunoglobulin G (ZsBio, Beijing, China) and
4,6-diamidino-2-phenylindole (DAPI) (Beyotime Co., Nantong, China)
were used.
Inclusion criteria and group
division
i) The blank control group included 20 patients (20
knees) who were diagnosed with only lateral discoid meniscus and MP
without patellofemoral joint pain; and ii) the positive control
group included 20 patients (20 knees) who were diagnosed with
synovial plica syndrome preoperatively, concomitant with
chondromalacia patella intraoperatively and femoral condyle
cartilage injuries. iii) The experimental group was the 20 patients
(20 knees) who were diagnosed with MP and no other concomitant
disorders in the joint.
Exclusion criteria
Patients with systemic diseases, such as diabetes,
systemic lupus erythematosus, rheumatoid arthritis and other
chronic inflammatory conditions, in the knee were excluded.
The study was approved by the Institutional Review
Board and Ethics Committee at The Center for Joint Surgery
(Southwest Hospital, The Third Military Medical University,
Chongqing, China). All the patients provided signed informed
consent.
Preoperative and postoperative pain
score evaluation
The visual analogue scale (VAS) was used to evaluate
the patients' patellofemoral joint pain preoperatively and
postoperatively. Patients were followed for 12±3.9 months (range,
6–19 months). The VAS 3-month postoperative results were obtained
to compare with the preoperative scores.
Arthroscopy and specimen
preparation
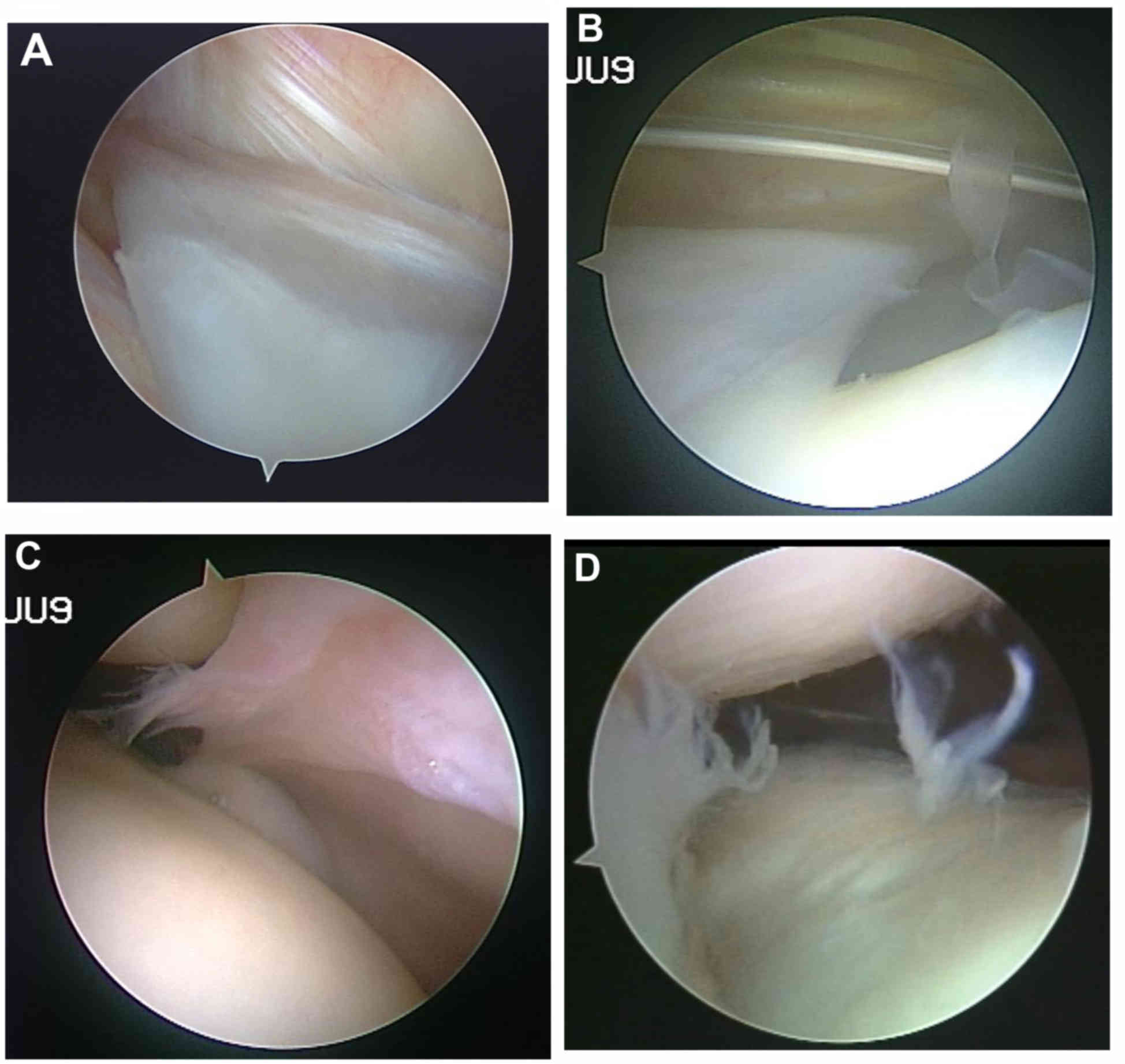
A total of 60 patients (60 knees) underwent
arthroscopy with an arthroscope that was equipped with a digital
colored three-chips endoscopic camera system inside (Smith &
Nephew, Andover, MA, USA). The procedure was completed by the same
arthroscopic surgeon. The diagnosis of symptomatic MP can be
confirmed by the presence of pathological disorders in the
arthroscope (Fig. 1) (10,11).
The specimens were obtained from the tissues in the
basilar section of the suprapatellaris plica and MP of each
patient.
Immunohistochemical study
The specimens were refrigerated at 4°C, frozen in
liquid nitrogen, embedded by a mixture of polyethylene glycol and
polyvinyl alcohol (optimal cutting temperature compound) and
sliced. The slices were 8 µm. Permeability was performed in
phosphate-buffered saline (PBS) with 0.1% (volume fraction, V/V)
Triton X-100 for 30 min and sealed for 15 min with 5% goat serum
(V/V). The slice was incubated in PBS and rabbit anti-human SP
(ZA-0235) 1:50 (V/V). The section was incubated overnight in a damp
environment at 4°C. Following this, it was rinsed with 0.01 mol/l
PBS three times, for 5 min each time. The fluorescent secondary
antibody was added to the procedure. The marker was fluorescein
isothiocyanate goat-anti-rabbit (ZF-3011) 1:50 (V/V) and the sample
was incubated at the constant temperature of 37°C. Following rising
with 0.01 mol/l PBS three times, 5 min each time, the sample was
dyed with DAPI for 1 min and 50% glycerine for mounting. Samples
were observed with a fluorescence microscope.
Semi-quantitative analysis
Image analysis software Olympus DP Controller and DP
Manager (Olympus Corp., Toyko, Japan) was used with 400-power
random observation for 50 visual fields. All the immunoreactive
fibers were numbered and the density of the nerve fibers was
calculated (fibers/cm2). The data collection was
completed by two pathological physicians in a double-blind
manner.
Statistical analysis
SAS JMP6.0 software (SAS Institute, Inc., Cary, NC,
USA) was used to analyze the statistical data, with the size of the
test set at α=0.05. Nerve density differences between the groups
were compared by the method of analysis of variance and
Student-Newman-Keuls test. Nerve density differences between the MP
and suprapatellar plica were compared by the paired t-test. The VAS
score differences of the experimental and positive control group
preoperative and 3 months postoperative were analyzed by the
Wilcoxon rank sum test. The association between the preoperative
VAS pain score and the SP fiber density of MP were analyzed by the
Spearman's correlation.
Results
Changes in structure between the
groups
The standard Sakakibara (12–14) taxonomy
was applied in MP arthroscopic classification criteria, as shown in
Fig. 2.
Pathological changes occurred between groups. The
plica structure widened significantly more compared to the blank
control (types C and D) in 31 cases, fibrous cord-like changes
occurred in 22 cases, ischemic pale hypertrophy in 11 cases, and
extrusion-forming flaps in 13 cases, respectively (Table I).
 | Table I.Sakakibara classification and
demography. |
Table I.
Sakakibara classification and
demography.
|
| Sakakibara
Classification |
|
|
|---|
|
|
|
|
|
|---|
| Group | A | B | C | D | Age, mean ± standard
deviation (range) | Male/female |
|---|
| Blank control | 7 | 9 | 4 | 0 | 34.8±12.0
(14–58) | 8/12 |
| Positive control | 0 | 7 | 9 | 4 | 33.8±8.8 (17–52) | 10/10 |
| Experimental | 1 | 5 | 11 | 3 | 28.9±7.1 (17–39) | 9/11 |
| Total | 8 | 21 | 24 | 7 | 32.5±9.8 (14–58) | 27/33 |
No significant statistical difference was observed
in gender (P=0.817) and age (P=0.135) among the blank control,
experimental and the positive control groups. Type C/D in the
experimental group was higher compared to the blank control group
(P=0.001), and there was no significant difference between the
experimental and positive control groups (P=0.736).
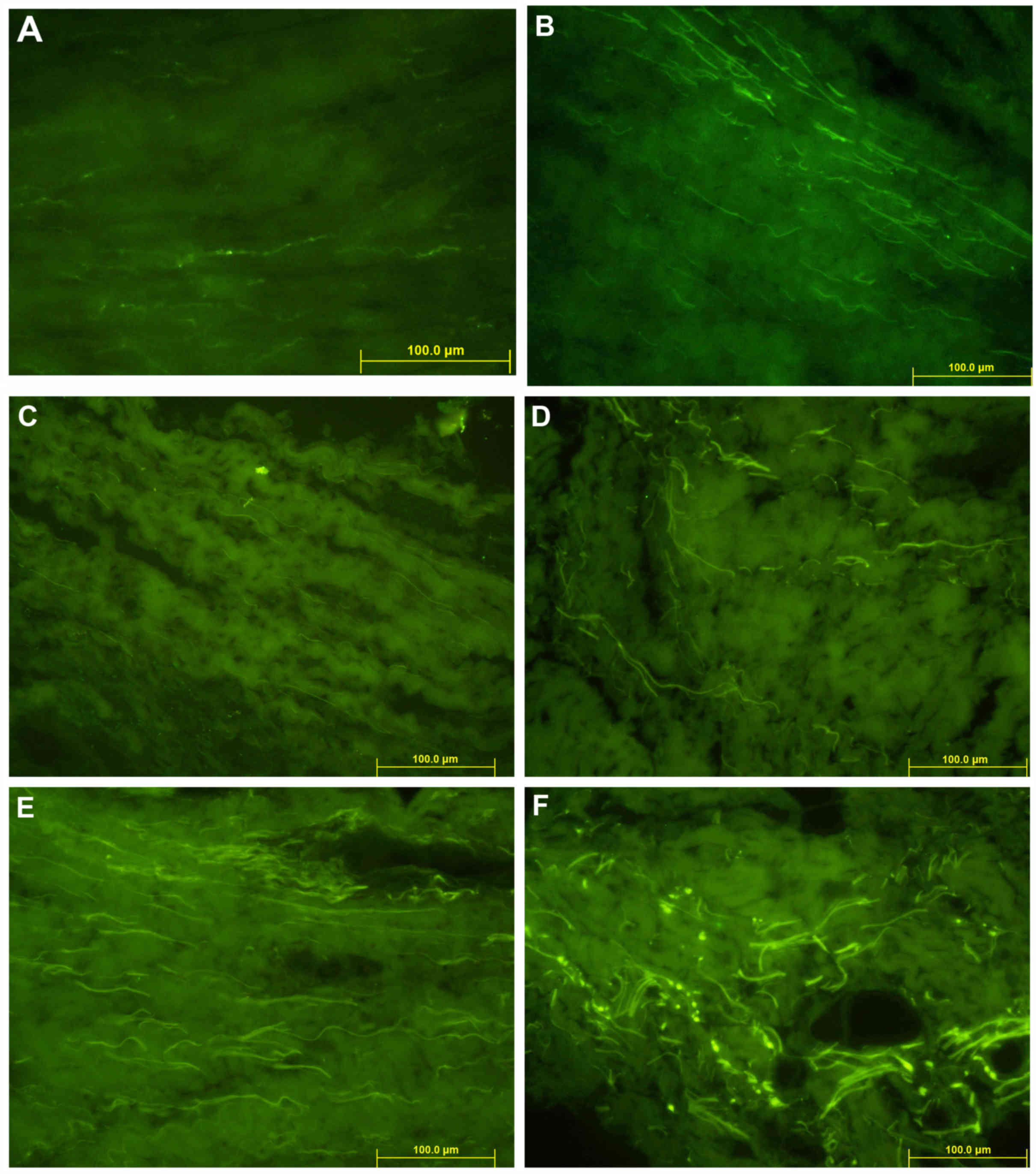
Distribution of SP fibers
Immunohistochemical staining revealed a positive
performance of SP in MP (magnification, ×400) as shown in Fig. 3.
Semi-quantitative data analysis of SP staining is
shown in Table II. Staining SP nerve
fiber density in suprapatellar plica revealed that the positive
control group was higher when compared to the experimental and
blank control groups, P<0.001; however, there was no difference
between the experimental and blank control groups.
| Table II.Staining SP nerve fiber density of
suprapatellar plica and MP. |
Table II.
Staining SP nerve fiber density of
suprapatellar plica and MP.
| Group | Case, n | Suprapatellar
plica | MP | Statistic |
|---|
| Blank control | 20 |
24.60±26.17 |
23.23±18.41 | t=0.14 |
| Positive control | 20 | 117.36±73.62 | 268.00±71.60 | P=0.8884 |
|
|
|
|
| t=10.51 |
| Experimental | 20 | 59.06±44.06 | 255.44±87.91 | P=0.0056 |
|
|
|
|
| t=13.13 |
| Statistics |
| F=11.27 | F=47.70 | P=0.0013 |
|
|
| P<0.001 | P<0.001 |
|
VAS pain evaluation
The VAS pain evaluation results are shown in
Table III. No significant difference
was observed in the preoperative pain score of the experimental and
the positive control groups. Postoperative pain scores were
significantly lower.
| Table III.VAS pain evaluation results. |
Table III.
VAS pain evaluation results.
| Group | Case, n | Preoperative | 3-month
postoperative | Statistics |
|---|
| Experimental
group | 20 | 61.35±22.36 | 11.78±3.77 | W=210, P=0.0027 |
| Positive control
group | 20 | 68.45±16.39 | 12.96±5.31 | W=213, P=0.0095 |
| Statistics |
| W=373, P=0.371 | W=384, P=0.481 |
|
Association of VAS pain evaluation and
density of SP fibers of MP
The correlation between VAS pain score and
innervation density of SP in 40 patients in the experimental and
positive control groups was analyzed. The results showed a positive
correlation between SP positive nerve density and pain scores
(r=0.4612, P=0.0027).
Discussion
In previous studies, including those by Broom and
Fulkerson (15), Jackson et al
(16) and Shahriaree and Nottage
(17), the contact between
mediopatellar and femoral condyle was reported to not cause pain
directly, however, types A and B, with smaller morphological plica,
can cause patellofemoral pain. There is no direct correlation
between the occurrence of the patellofemoral pain and plica
morphology. However, the basic research with regards to its
clinical causes remains to be elucidated.
Currently, an increasing number of studies have
focused on the study of neurophysiological changes of soft tissues
in the knee joint to explain a variety of pathological changes and
functional abnormalities (5,18,19). Certain
studies have reported that the level of neuropeptide nerve fibers
in patients with anterior knee pain rose significantly in the
tissues of retinaculum and fat pads (7). In the previous studies it has been
confirmed that SP is an important neurotransmitter of pain, and the
material basis for the conduction of pain, whose level is the
indicator of the pain degree experienced by the patient in the knee
joint and soft tissue (20–23).
An objective pain assessment was affected by patient
attributes, including psychological factors and individual
differences, so therefore, the experiments were designed by taking
the specimens from the same patient, which can reduce the influence
on the experimental data caused by individual differences for the
feelings of pain. In the present study, the SP expression levels in
patients with MP and suprapatellar plica were compared within the
same group. The study found that in the blank control group, there
was no significant difference in the SP fibers distribution. There
was also no pain symptom in MP and in suprapatellar plica. In the
experimental and positive control groups, the SP expression levels
in MP were significantly higher compared to the levels of
suprapatellar plica. There was no suprapatellar bursa effusion,
inflammation or pain in the selected specimens. A high degree of
consistency existed between the increase of density of SP fibers in
MP and the aggravated patellofemoral pain.
Arthroscopic resection of symptomatic MP can
significantly alleviate and eliminate the symptoms of
patellofemoral pain, which has been confirmed by a number of
previous studies (2–4). The preoperative patellofemoral pain
scores and 3-month postoperative scores were compared between the
experimental and positive control groups, and found that pain was
significantly relieved following the resection of the symptomatic
MP.
The distribution of SP nerve fiber density in MP and
the pain scores of patients with patellofemoral pain were analyzed.
The same conclusion could be drawn from contrastive analysis based
on each group on nerve fiber density and pain scores: SP expression
nerve fibers increased significantly in the patients with
symptomatic MP, and its abnormal structure was closely associated
with the patients who reported an aggravation of patellofemoral
pain.
Considering that the patients with symptomatic MP
had cartilage injuries in patellofemoral joint in the majority of
cases, the patients were divided into two groups so that the
influence of cartilage injuries could be avoided. No significant
difference in preoperative pain score was observed between the two
groups. With regards to the number of nerve distribution between
the two groups, the positive control group was higher compared to
that of the experimental group. This may be attributed to the
presence of the patellofemoral joint cartilage injury, with loss of
cartilage debris entering the patellar medial synovial tissue,
synovial cells breaking the metabolic balance of local materials,
causing local inflammation in the synovial tissue (24), and affecting the local neural
structures. Wu et al (25) in
2000 confirmed that the nerve fiber density increased in the ankle
osteoarthritis inflammatory synovial tissues, and only a small
amount of nerve distribution existed in the healthy synovial
tissue.
The present study has two limitations. Firstly, the
blank control group was the patients with lateral discoid meniscus.
The tear of lateral meniscus and the debris of cartilage may deduce
the inflammation in the synovial membrane. The density of the SP
fibers in MP may be higher compared to that of normal people. By
contrast, semi-quantitative analysis of innervation for SP fibers
was variable, possibly implying the trend of SP fibers
distribution, however, it was not precise enough to evaluate the
number of SP fibers innervated in the plica. Quantitative analysis
of the density may improve this.
In conclusion, an increase of SP expression in
symptomatic MP may be the important pathophysiological basis that
causes pain. The density of SP expression nerve fibers and the
level of pain are closely associated. Expression of SP has an
important role in the pathogenic mechanisms of symptomatic MP.
Glossary
Abbreviations
Abbreviations:
|
MP
|
mediopatellar plica
|
|
SP
|
substance-P
|
References
|
1
|
Dupont JY: Synovial plicae of the knee.
Controversies and review. Clin Sports Med. 16:87–122. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kerimoğlu S, Citlak A, Cavuşoğlu S and
Turhan AU: Bucket-handle tear of medial plica. Knee. 12:239–241.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Madhusudhan TR, Kumar TM, Bastawrous SS
and Sinha A: Clinical examination, MRI and arthroscopy in meniscal
and ligamentous knee Injuries - a prospective study. J Orthop Surg.
3:192008. View Article : Google Scholar
|
|
4
|
Boyd CR, Eakin C and Matheson GO:
Infrapatellar plica as a cause of anterior knee pain. Clin J Sport
Med. 15:98–103. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wojtys EM, Beaman DN, Glover RA and Janda
D: Innervation of the human knee joint by substance-P fibers.
Arthroscopy. 6:254–263. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Inami S, Shiga T, Tsujino A, Yabuki T,
Okado N and Ochiai N: Immunohistochemical demonstration of nerve
fibers in the synovial fold of the human cervical facet joint. J
Orthop Res. 19:593–596. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Witoński D and Wagrowska-Danielewicz M:
Distribution of substance-P nerve fibers in the knee joint in
patients with anterior knee pain syndrome. A preliminary report.
Knee Surg Sports Traumatol Arthrosc. 7:177–183. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ferretti A: Epidemiology of jumper's knee.
Sports Med. 3:289–295. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hardaker WT, Whipple TL and Bassett FH:
Diagnosis and treatment of the plica syndrome of the knee. J Bone
Joint Surg Am. 62:221–225. 1980.PubMed/NCBI
|
|
10
|
Calpur OU, Copuroglu C and Ozcan M: United
unresorbed medial and lateral plicae as anterior mesenchymal
synovial septal remnant. Knee Surg Sports Traumatol Arthrosc.
10:378–380. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Farcas C, Hargital Z, Gaspar L, Kuki A,
Csernatony Z and Szepesi K: Histological changes in the symptomatic
mediopatellar plica. Knee. 11:103–108. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Koshino T and Okamoto R: Resection of
painful shelf (plica synovialis mediopatellaris) under arthroscopy.
Arthroscopy. 1:136–141. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sakakibara J: Arthroscopic study on lino's
band (plicasynovia is mediopatellaris). J Jpn Orthop Assoc.
50:513–522. 1976.
|
|
14
|
Munzinger U, Ruckstuhl J, Scherrer H and
Gschwend N: Internal derangement of the knee joint due to
pathologic synovial folds: The mediopatellar plica syndrome. Clin
Orthop Relat Res. 155:59–64. 1981.PubMed/NCBI
|
|
15
|
Broom MJ and Fulkerson JP: The plica
syndrome: A new perspective. Orthop Clin North Am. 17:279–281.
1986.PubMed/NCBI
|
|
16
|
Jackson RW, Marshall DJ and Fujisawa Y:
The pathologic medical shelf. Orthop Clin North Am. 13:307–312.
1982.PubMed/NCBI
|
|
17
|
Shahriaree H and Nottage WM: Synovial
folds and plicae. O'Connor Textbook of Arthroscopic Surgery (2nd).
Shahriaree H: (Philadelphia). JB Lippincott. 535–541. 1992.
|
|
18
|
Biedert RM and Sanchis-Alfonso V: Sources
of anterior knee pain. Clin Sports Med. 21:335–347. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sanchis-Alfonso V and Roselló-Sastre E:
Anterior knee pain in the young patient - what causes the pain?
‘Neural model.’. Acta Orthop Scand. 74:697–703. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dragoo JL, Johnson C and McConnell J:
Evaluation and treatment of disorders of the infrapatellar fat pad.
Sports Med. 42:51–67. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sanchis-Alfonso V: Patellofemoral pain.
Orthopade. 37835–836. (838): 840. 2008.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ordeberg G: Characterization of joint pain
in human OA. Novartis Found Symp. 260:105–115; discussion 115–121,
277–279. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Seidel MF and Lane NE: Control of
arthritis pain with anti-nerve-growth factor: Risk and benefit.
Curr Rheumatol Rep. 14:583–588. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lyu SR, Tzeng JE, Kuo CY, Jian AR and Liu
DS: Mechanical strength of mediopatellar plica - the influence of
its fiber content. Clin Biomech (Bristol, Avon). 21:860–863. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wu Z, Nagata K and Iijima T:
Immunohistochemical study of NGF and its receptors in the synovial
membrane of the ankle joint of adjuvant-induced arthritic rats.
Histochem Cell Biol. 114:453–459. 2000.PubMed/NCBI
|