Introduction
Cervical intraepithelial neoplasia (CIN), also known
as transformation and dysplasia of cervical intraepithelial cells,
is the precancerous lesion of squamous cell carcinoma. CIN is
usually detected through the Papanicolaou (Pap) cytological
screening or the high-risk human papillomavirus (HPV) DNA testing
(1). However, the Pap test or superior
colposcope multipoint sampling requires gynecological surgery. The
current inspection method takes time and may fail to collect the
most severe lesions. The diagnosis and staging of collected
specimens mainly depends on the pathological features.
The mechanisms involved in cell transformation and
dysplasia of CIN remain unclear. CXC chemokine receptor type 7
(CXCR7) has been suggested to play a role in tumor development.
However, studies on the function of CXCR7 in precancerous lesions
are limited. CXCR7 is a non-G protein-coupled receptor.
Heterodimerization of CXCR7 with other receptors, such as the
epidermal growth factor receptor or CXCR4, triggers intracellular
signaling events that are important for the regulation of cell
proliferation and apoptosis (2–4). Expression
of CXCR7 has been associated with a higher tumor grade and more
aggressive tumor growth in different types of cancer, such as
cervical cancer, prostate cancer, breast cancer, glioma and
hepatocellular carcinoma (5–8). CIN is usually associated with chronic
infection of the cervix mainly with the sexually transmitted HPV,
particularly the high-risk HPV 16 or HPV 18. The HPV encodes
several proteins, including E6 and E7, which lead to the
degradation of tumor-suppressor protein p53. In addition, smoking,
endogenous and exogenous immunodeficiency are also the risk factors
for CIN. CXCR7 was previously reported to play an important role in
regulating cell proliferation, apoptosis, tumor evasion,
trafficking of lymph node metastasis and metastasis in distinct
organs through auto/paracrine mechanisms (9). Additionally, high levels of CXCR7 have
been linked to poor disease-free or disease-specific survival rates
in cervical cancer patients (5).
Progression to invasive cancer occurs in ~1% of CIN I, 5% in CIN II
and ≥12% in CIN III. Treatment options for higher grade CIN include
conization of cervix, hysterectomy, cryocautery, electrocautery and
loop electrosurgical excision procedure, which differ from the
lower grade CIN.
The aim of the present study was to determine CXCR7
protein expression in various stages of CIN to understand the
potential contribution of CXCR7 in the development and progression
of CIN. Receiver operating characteristic (ROC) curves were
established to evaluate the prognostic value of CXCR7 in
differentiating different stages of CIN, which has not been
reported previously.
Materials and methods
Patient tissues
A total of 34 patients were recruited in the study.
Normal cervical tissues obtained from 7 patients with uterine
fibroid (with normal cervix) by hysterectomy were used as negative
controls. Ten patients with CIN I and 8 diagnosed with CIN II who
underwent loop electrosurgical excision procedure were included. A
total of 9 patients with CIN III under conization of cervix were
also enrolled. The study was approved by the Ethics Committee of
West China Hospital of Sichuan University (Sichuan, China). The
patient baseline characteristics were anonymously taken to document
the process. The Ethics Committees approved this consent
procedure.
The clinical stage was determined based on the
evaluation of the surgical specimens, which was performed by two
independent, experienced pathologists. Assessments were made
according to the International Federation of Gynecology and
Obstetrics 2009 system.
Immunohistochemistry (IHC)
CXCR7 expression in formalin-fixed,
paraffin-embedded specimens was assessed by IHC. Tissue blocks were
sectioned (5 µm) and deparaffinized with xylene. Antigen retrieval
with citrate antigen retrieval solution (pH 6.0) was performed in a
95°C water bath for 40 min. Sections were subsequently rinsed in
phosphate-buffered saline and incubated with 3%
H2O2 for 15 min to block endogenous
peroxidase activity.
Each section was incubated with the anti-CXCR7
antibody (1:100; MAB4227) from R&D Systems (Minneapolis, MN,
USA) for 45 min at 37°C, followed by labeling with secondary
antibody (GK500705; Envision™ Detection kit; Dako, Glostrup,
Denmark). Images of neoplasia and normal tissues were taken at
magnification, ×400.
Data analysis
Image-Pro Plus 6.0 software (Media Cybernetics,
Rockville, MD, USA) was used for analyzing IHC. For quantitative
analysis of the IHC results, area, diameter, density and integral
optical density (IOD) were chosen as the measurements. IOD
represents the IOD in the whole layer. The area stands for the
positive-stained area in the cervical intraepithelial layer.
Diameter is also for the positive-stained layer. Density or mean
density is equal to IOD SUM/area.
The ROC curves were established to evaluate the
prognostic value of CXCR7 in differentiating the stages of CIN. All
the statistical analyses were performed using the SPSS 20.0
software (IBM, Corp., Armonk, NY, USA). The statistical
significance of CXCR7 correlation in association with the
clinicopathological features was assessed using the
independent-sample t-test, one-way analysis of variance. P<0.05
was considered to indicate a statistically significant
difference.
Results
CIN samples
The samples were divided into 3 groups according to
the degree of atypical hyperplasia: CIN I, atypical cells are
confined to the inner 1/3 of the epithelial layer; CIN II, abnormal
cells are extended to the 2/3 of the epithelial layer; and CIN III,
atypical cells exceed the 2/3 of the epithelial layer, but do not
reach the whole layer.
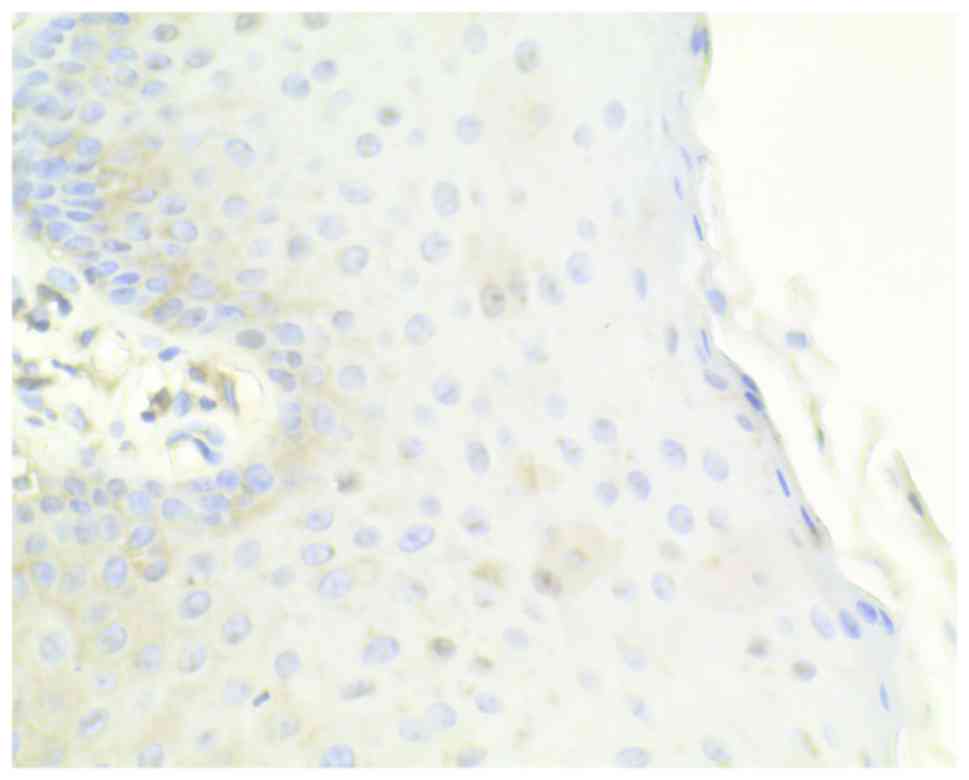
Normal cervical tissues from patients with uterine
fibroids were chosen as the negative controls, which showed a
limited immunohistochemical reaction (Fig.
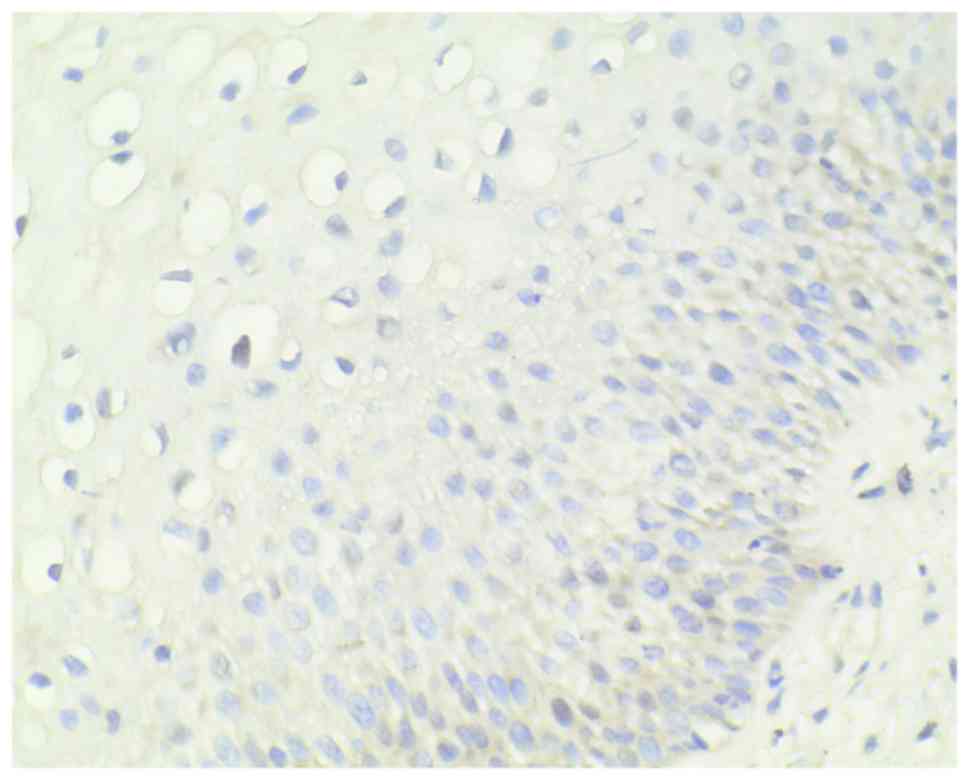
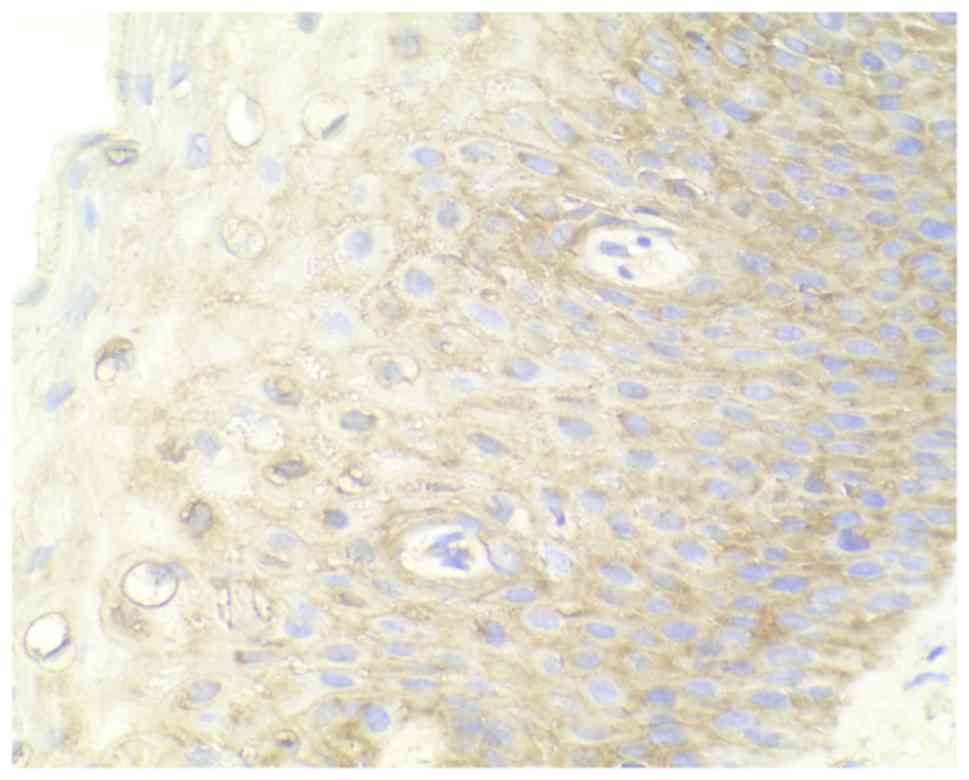
1). A relatively low level of CXCR7 expression in CIN I, medium
expression in CIN II and high expression in CIN III were observed
(Figs. 2–4). Immunohistochemical staining of CIN
samples showed that cytoplasm was positively stained in the
atypical or dysplastic proliferative cells, particularly in the
abnormally arranged cells with abnormal nucleus (Figs. 2–4). In
the absence of the primary antibody, no immunoreactivity was
detected, indicating the specificity of the antibody used in the
study.
Analysis of the CXCR7 expression
Area analysis demonstrated a significantly increased
expression of CXCR7 in CIN tissues (151.77±4.76) compared to normal
cervical tissues (102.52±32.63) (P<0.01). A significant
difference was also observed in IOD analysis between CIN tissues
(23,313.60±5,052.56) and the negative control (16,266.36±5,695.51)
(P<0.01).
As shown in Table I,
the positive area was significantly increased in CIN I, CIN II and
CIN III as compared to the negative control (P=0.013, 0.001 and
0.008, respectively). In IOD analysis, a significant difference was
observed between the CIN II or CIN III group and the negative
control group (P=0.02 and 0.01, respectively).
 | Table I.Quantitative analysis of the
immunohistochemical results. |
Table I.
Quantitative analysis of the
immunohistochemical results.
| Dependent
variables | Mean difference from
negative control ± standard error | P-value | 95% confidence
interval |
|---|
| Area |
|
|
|
| CIN
I | −42.69±12.96 |
0.01a | (−77.92 to
−7.46) |
| CIN
II | −60.80±13.61 |
<0.001a | (−97.80
to −23.80) |
| CIN
III | −46.27±13.25 |
0.01a | (−82.30
to −10.24) |
| Density |
|
|
|
| CIN
I |
7.71±5.49 | 0.51 | (−7.22 to 22.63) |
| CIN
II | −5.77±5.77 | 0.75 | (−21.45 to 9.91) |
| CIN
III | −8.06±5.61 | 0.49 | (−23.33 to 7.21) |
| Diameter |
|
|
|
| CIN
I | −0.69±0.50 | 0.52 | (−2.06 to 0.67) |
| CIN
II | −1.40±0.53 | 0.06 | (−2.83 to 0.04) |
| CIN
III |
0.39±0.51 | 0.87 | (−1.01 to 1.78) |
| IOD |
|
|
|
| CIN
I |
−4,604.65±2,485.56 | 0.27 | (−11,363.15 to
−2,153.86) |
| CIN
II |
−8,311.75±2,610.36 |
0.02a | (−15,409.60 to
−1,213.90) |
| CIN
III |
−8,637.23±2,541.78 |
0.01a | (−15,548.61 to
−1,725.85) |
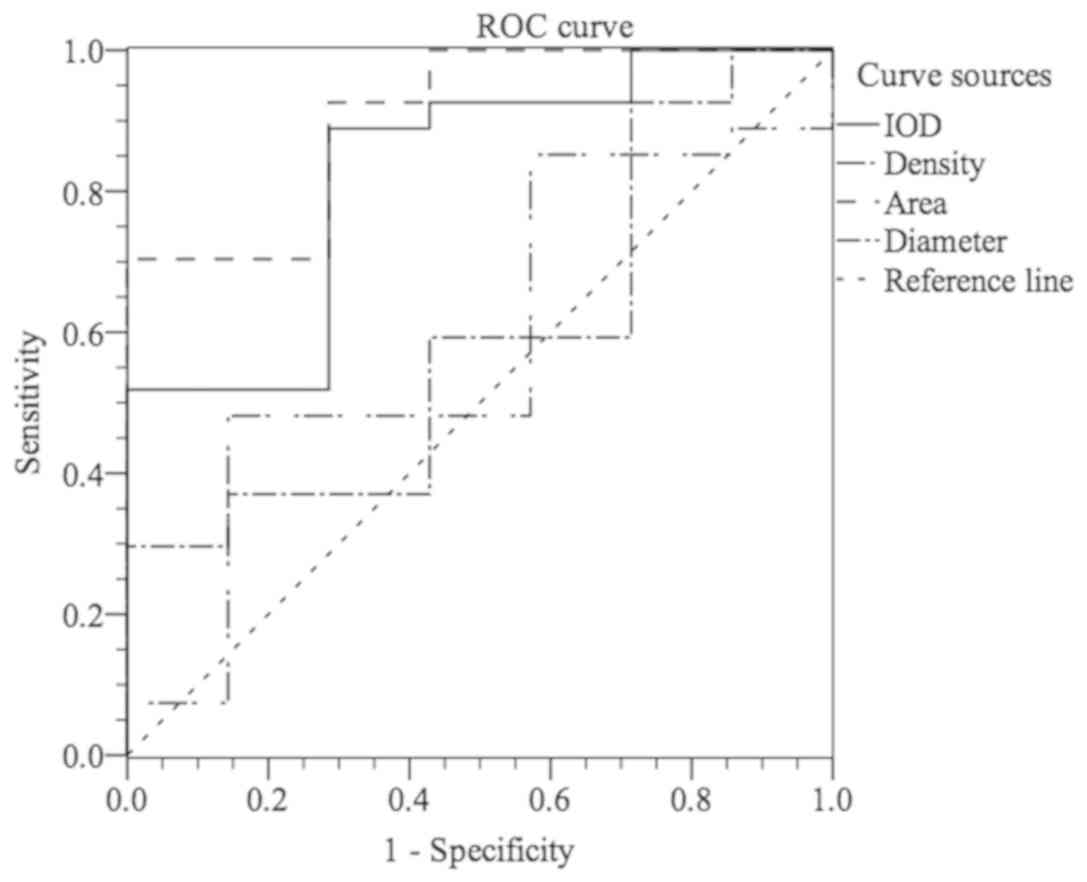
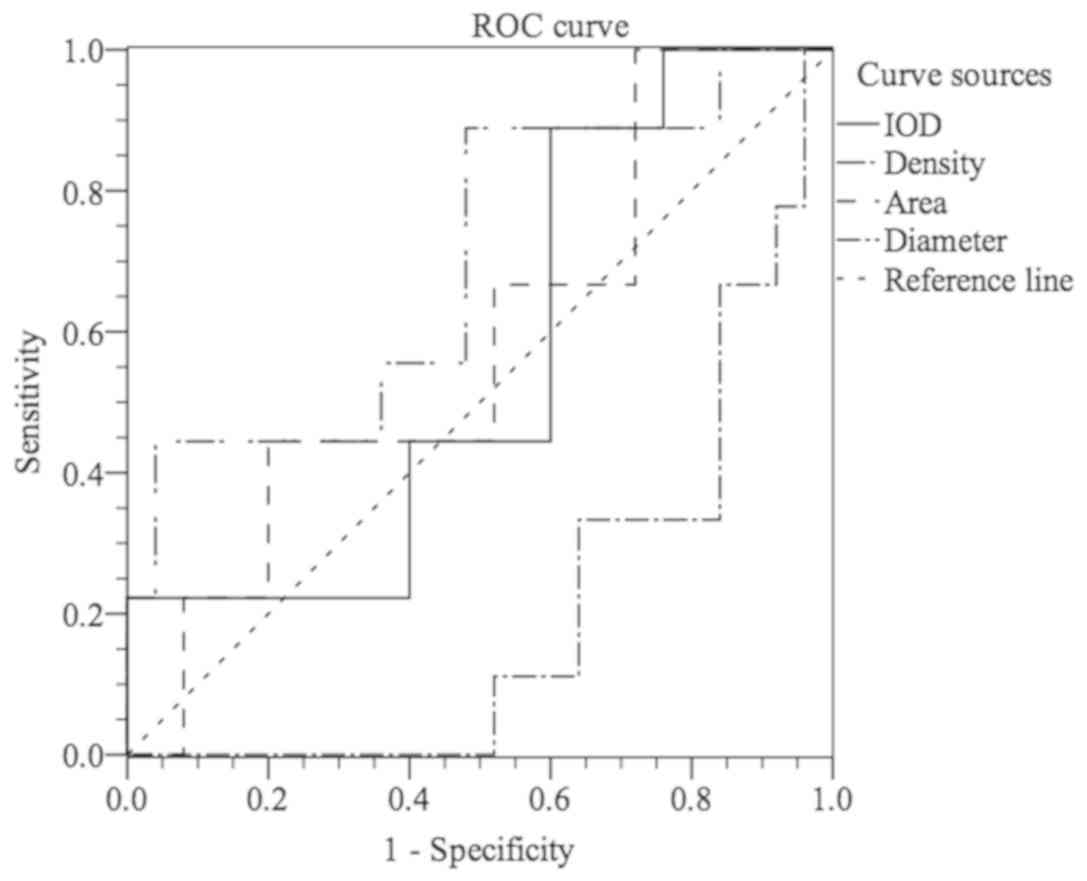
To further assess the ability of CXCR7 to
distinguish CIN stages, ROC curve analysis was used, which was not
reported previously. As shown in Fig.
5, stages I–III of CIN could be differentiated from normal
cervical epithelium by CXCR7 staining with an area under the curve
(AUC) of 0.825 (IOD) [95% confidence interval (CI), 0.655 to 0.996]
and 0.905 (area) (95% CI, 0.789 to 1.000). For IOD, at the cut-off
value of 18,833.945, the sensitivity and the specificity were 88.9
and 71.4%, respectively, in discriminating CIN I–III from normal
tissue (Fig. 5). For area, Fig. 5 showed that, with an AUC of 0.905 (95%
CI, 0.789 to 1.000), CIN I–III could be differentiated from normal
cervical epithelium at the cut-off value of 137.515 with
sensitivity (70.4%) and specificity (100.0%). Similarly, Fig. 6 showed that CXCR7 could differentiate
stages II–III from stage I or negative control with an AUC of 0.663
(IOD) (95% CI, 0.478 to 0.847) or 0.666 (area) (95% CI, 0.476 to
0.856). At the cut-off value of 19,731.52, the sensitivity and
specificity were 92.7 and 50.0% in discriminating CIN II–III from
negative to CIN I (Fig. 6). However,
CIN III could not be easily distinguished from normal tissue or CIN
I–II with an AUC of 0.698 (density) (95% CI, 0.488 to 0.907,
Fig. 7). With the cut-off value of
165.755, CIN III could be discriminated from normal tissue to CIN
I–II at the sensitivity of 50.0% and the specificity of 90.0% (AUC
of 0.666) (Fig. 7). However, the
cut-off value is 19,731.52 (IOD) with sensitivity (88.9%) and
specificity (40%) in discriminating stage III from stages I–II and
normal tissue, which was not satisfactory (Fig. 7).
Discussion
In the present study, the CXCR7 protein was strongly
positive in neoplasia. Previously, it was reported that CXCR7
expression was higher in cervical cancer compared to CIN and normal
cervical mucosa, particularly in those with an advanced stage of
cancer and lymph node metastasis (10). However, the difference in CXCR7 protein
expression among different stages of CIN has not been previously
investigated and the ROC curve analysis has not been performed. To
the best of our knowledge, this is the first study to report that
the CXCR7 protein expression level gradually increases from normal
cervical intraepithelium to CIN.
It was previously shown with in situ
hybridization and IHC that CXCR7 expression is induced in various
types of cancer and increased with malignancy (7,8,11,12). The
results in the present study that CXCR7 is overexpressed in CIN
samples compared with normal tissues support the idea that CXCR7
may serve as a prognostic marker (5,13).
Alternatively, the upregulated expression of CXCR7 may favor
precancerosis. CXCR7 is expressed in numerous malignant cells,
including breast, lung, pancreatic and prostate cancer cells
(6,13–15). CXCR7
is expressed in 43% of cervical cancer specimens and is associated
with tumor size and lymph node metastasis together with
disease-free survival (5). The
significant difference in CXCR7 protein expression level was
observed between CIN I, CIN II, CIN III and the negative control in
the present study. It is possible that CXCR7 promotes further
cancerous activity. CXCR7 is induced under the classic tumor
microenvironment (hypoxic and acidic conditions) in human
microvascular endothelial cells (8).
It is also upregulated in the tumor-associated vasculature
(6,12,16).
However, the upregulation was not observed in the vasculature of
corresponding healthy tissues (12),
indicating that angiogenesis is influenced by CXCR7.
Hepatocarcinoma cells treated with vascular endothelial growth
factor results in a positive feedback for CXCR7 expression
(17), further supporting the notion
that CXCR7 impacts on vascular growth, therefore favoring
precancerosis and subsequently cancerous lesions.
Current evidence suggests that CXCR7 may function in
intraepithelial neoplasia dysplasia or cervical interstitial
neoplasia. Further investigation is required to understand the
accurate mechanism of CXCR7 in regulating precancerosis and to
assess the possible value of the CXCR7 expression level detection
in the blood samples of patients as a non-invasive, prognostic and
diagnostic marker.
Acknowledgements
The present study was supported by the National
Innovative Experimental Projects of Sichuan University, 2012 (grant
no. 201210610114). The authors would like to thank Mr. Zengliang
Xia and Mr. Faqiang Zhang from the West China Laboratory of
Molecular Genetics for their great technical assistance.
References
|
1
|
Origoni M, Salvatore S, Perino A,
Cucinella G and Candiani M: Cervical Intraepithelial Neoplasia
(CIN) in pregnancy: The state of the art. Eur Rev Med Pharmacol
Sci. 18:851–860. 2014.PubMed/NCBI
|
|
2
|
Hartmann TN, Grabovsky V, Pasvolsky R,
Shulman Z, Buss EC, Spiegel A, Nagler A, Lapidot T, Thelen M and
Alon R: A crosstalk between intracellular CXCR7 and CXCR4 involved
in rapid CXCL12-triggered integrin activation but not in
chemokine-triggered motility of human T lymphocytes and CD34+
cells. J Leukoc Biol. 84:1130–1140. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Décaillot FM, Kazmi MA, Lin Y, Ray-Saha S,
Sakmar TP and Sachdev P: CXCR7/CXCR4 heterodimer constitutively
recruits beta-arrestin to enhance cell migration. J Biol Chem.
286:32188–32197. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Singh RK and Lokeshwar BL: The
IL-8-regulated chemokine receptor CXCR7 stimulates EGFR signaling
to promote prostate cancer growth. Cancer Res. 71:3268–3277. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schrevel M, Karim R, ter Haar NT, van der
Burg SH, Trimbos JB, Fleuren GJ, Gorter A and Jordanova ES: CXCR7
expression is associated with disease-free and disease-specific
survival in cervical cancer patients. Br J Cancer. 106:1520–1525.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miao Z, Luker KE, Summers BC, Berahovich
R, Bhojani MS, Rehemtulla A, Kleer CG, Essner JJ, Nasevicius A,
Luker GD, et al: CXCR7 (RDC1) promotes breast and lung tumor growth
in vivo and is expressed on tumor-associated vasculature. Proc Natl
Acad Sci USA. 104:15735–15740. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hattermann K, Held-Feindt J, Lucius R,
Müerköster SS, Penfold ME, Schall TJ and Mentlein R: The chemokine
receptor CXCR7 is highly expressed in human glioma cells and
mediates antiapoptotic effects. Cancer Res. 70:3299–3308. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Monnier J, Boissan M, L'Helgoualc'h A,
Lacombe ML, Turlin B, Zucman-Rossi J, Théret N, Piquet-Pellorce C
and Samson M: CXCR7 is up-regulated in human and murine
hepatocellular carcinoma and is specifically expressed by
endothelial cells. Eur J Cancer. 48:138–148. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hattermann K and Mentlein R: An infernal
trio: The chemokine CXCL12 and its receptors CXCR4 and CXCR7 in
tumor biology. Ann Anat. 195:103–110. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kurban S, Tursun M, Kurban G and Hasim A:
Role of CXCR7 and effects on CXCL12 in SiHa cells and upregulation
in cervical squamous cell carcinomas in Uighur women. Asian Pac J
Cancer Prev. 15:9211–9216. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shimizu S, Brown M, Sengupta R, Penfold ME
and Meucci O: CXCR7 protein expression in human adult brain and
differentiated neurons. PLoS One. 6:e206802011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Madden SL, Cook BP, Nacht M, Weber WD,
Callahan MR, Jiang Y, Dufault MR, Zhang X, Zhang W, Walter-Yohrling
J, et al: Vascular gene expression in nonneoplastic and malignant
brain. Am J Pathol. 165:601–608. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gebauer F, Tachezy M, Effenberger K, von
Loga K, Zander H, Marx A, Kaifi JT, Sauter G, Izbicki JR and
Bockhorn M: Prognostic impact of CXCR4 and CXCR7 expression in
pancreatic adenocarcinoma. J Surg Oncol. 104:140–145. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Burns JM, Summers BC, Wang Y, Melikian A,
Berahovich R, Miao Z, Penfold ME, Sunshine MJ, Littman DR, Kuo CJ,
et al: A novel chemokine receptor for SDF-1 and I-TAC involved in
cell survival, cell adhesion, and tumor development. J Exp Med.
203:2201–2213. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang J, Shiozawa Y, Wang J, Wang Y, Jung
Y, Pienta KJ, Mehra R, Loberg R and Taichman RS: The role of
CXCR7/RDC1 as a chemokine receptor for CXCL12/SDF-1 in prostate
cancer. J Biol Chem. 283:4283–4294. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sánchez-Martín L, Estecha A, Samaniego R,
Sánchez-Ramón S, Vega MÁ and Sánchez-Mateos P: The chemokine CXCL12
regulates monocyte-macrophage differentiation and RUNX3 expression.
Blood. 117:88–97. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zheng K, Li HY, Su XL, Wang XY, Tian T, Li
F and Ren GS: Chemokine receptor CXCR7 regulates the invasion,
angiogenesis and tumor growth of human hepatocellular carcinoma
cells. J Exp Clin Cancer Res. 29:312010. View Article : Google Scholar : PubMed/NCBI
|