Introduction
Breast cancer is the most frequent tumor and the
leading cause of cancer-related death among the female population
worldwide (1). Histopathological
factors such as the size of the primary tumor, differentiation
grade, the Ki-67 protein, the expression of estrogens (ER) and
progesterone (PgR) receptors or human epidermal growth factor
receptor 2 (HER2) and lymph node metastasis are associated with
tumor prognosis (2).
Identification of mechanisms underlying tumor cell invasion may
contribute to develop new therapies that can arrest local invasion
and metastatic spread of the disease.
Survivin, also called baculoviral inhibitor of
apoptosis repeat-containing 5 or BIRC5, is a 16.5-kDa protein which
in humans is encoded by the BIRC5 gene (3,4).
Survivin is a member of the inhibitor of apoptosis family that
serves to inhibit caspase activation therefore leading to negative
regulation of apoptosis or programmed cell death. Besides, it is
known that survivin localizes to the mitotic spindle by interaction
with tubulin during mitosis and may play an important role in
regulating mitosis (5). Survivin
is undetectable in terminally differentiated adult tissues, but
becomes notably expressed in the most common human tumors,
including stomach, colorectal, lung, breast, pancreatic and
prostate cancers (6,7).
Survivin expression can be deregulated in cancer by
several mechanisms, including amplification of the survivin locus
on chromosome 17q25, demethylation of survivin exons, increased
promoter activity and increased upstream signaling in the
phosphatidylinositol 3-kinase or mitogen-activated protein kinase
pathways. Additionally, the upregulation of survivin expression in
cancer cells seems to be independent of the cell cycle, suggesting
an increase in its antiapoptotic role compared with normal cells,
in which its mitotic regulation functions may be predominant
(8,9).
High survivin expression in the primary tumor, in
many cancer types, is almost invariably associated with a poor
prognosis for the patient. In breast cancer patients, however, the
association of survivin with prognosis is ambiguous, since previous
studies have reported it to be either irrelevant (10), or associated with poor (11) or good prognosis (12).
In this study, we tested the hypothesis that
survivin expression in patients with T4 breast cancer treated with
primary chemotherapy correlates with long-term outcomes. Moreover,
due to the conflicting data existing on the prognostic effect of
the tumor-suppressor protein p53 in breast cancer (13,14),
we also investigated the hypothesis of a possible association
between p53 and survivin as a factor further complicating patient
outcome.
Materials and methods
Patients
This retrospective study included 53 consecutive
breast cancer patients with clinical stage T4 as assessed by
physical examination and mammography, confirmed via core needle
biopsy. Patients were enrolled between 1992 and 2001. The median
follow-up was 125 months (range, 70–182 months). All 53 patients
received a multimodality treatment including primary chemotherapy,
surgery, radiation therapy (RT), adjuvant chemotherapy and hormone
therapy if indicated.
The median age of the patients was 50 years (range,
32–67 years). Regarding the pathological characteristics, 15
patients (28%) were diagnosed with inflammatory breast carcinoma
(T4d); 38 (72%) were non-inflammatory (T4abc). Twenty-eight
patients (53%) were ER-positive and 25 (47%) were ER-negative; 17
patients (32%) were PgR-positive and 36 (68%) PgR-negative; 24
patients (45%) were both ER- and PgR-negative and 16 (30%) both ER-
and PgR-positive; 12 patients (23%) were ER-positive PgR-negative;
10 patients (19%) were HER2-positive and 43 (81%) HER2-negative; 18
patients (34%) were HER2-, ER- and PgR-negative (triple negative;
TN), and 35 (66%) non-TN. Seventeen patients (32%) were
Ki-67-positive and 27 (51%) Ki-67-negative; Ki-67 was not
determined in 9 cases (17%). Baseline patient and tumor
characteristics are summarized in Table I.
 | Table I.Patient and tumor characteristics. |
Table I.
Patient and tumor characteristics.
| Frequency (n) | % |
|---|
| Age | | |
| ≤50 | 23 | 43 |
| >50 | 30 | 57 |
| Tumor stage | | |
| T4abc | 38 | 72 |
| T4d | 15 | 28 |
| Axillary nodes | | |
| cLN0 | 3 | 6 |
|
cLN+ | 50 | 94 |
| Hormone receptor
status | | |
|
ER+/ER− | 28/25 | 53/47 |
|
PgR+/PgR− | 17/36 | 32/68 |
| HER2 status | | |
|
HER2+ | 10 | 19 |
|
HER2− | 43 | 81 |
| Proliferative
index | | |
|
Ki-67+ | 17 | 32 |
|
Ki-67− | 27 | 51 |
| Ki-67 unknown | 9 | 17 |
| Grading | | |
| G2 | 38 | 72 |
| G3 | 15 | 28 |
| Survivin
expression | | |
|
survivin+ | 21 | 40 |
|
survivin− | 32 | 60 |
| p53 expression | | |
|
p53+ | 13 | 24 |
|
p53− | 40 | 76 |
|
survivin+ and
p53+ | 11 | 21 |
|
survivin− and
p53− | 30 | 79 |
Pathological assessment
ER and PgR status was assessed by standard
immunohistochemical (IHC) analysis. Nuclear staining of ≥10% was
considered positive. Hormone receptor (HR)+ was
indicated as ER+ and PgR+, and HR−
was indicated as ER− and PgR−. HER2 status
was assessed by IHC or by fluorescence in situ hybridization
(FISH) in breast cancer tissue. HER2-positive tumors were defined
as 3+ on the IHC test. HER2-negative tumors were defined
as 0 or 1+ on the IHC test; IHC 2+ required
the FISH test.
Response assessment
The clinical measurement of the response to
neoadjuvant therapy was defined according to the International
Union Against Cancer (UICC) criteria (15) as: complete response (CR), a total
resolution of the breast tumor and axillary adenopathy based on
clinical and instrumental examinations; partial response (PR), a
≥50% reduction of the product of the two largest perpendicular
dimensions of the breast mass and axillary adenopathy; minor
response (MR), a <50% reduction of the product of the two
largest perpendicular dimensions of the breast mass and axillary
adenopathy; no change in clinical status (NC); and progressive
disease (PD).
Pathological complete response was defined as the
absence of residual invasive disease in both the breast and the
axilla. Gross invasive residual disease in breast tissue or the
presence of cancer-positive lymph nodes in the axilla were defined
as <pCR (2). Major pathological
response in breast tissue was defined as no more than 2 cm of
residual disease (pT0 plus pT1) (16).
Treatment plan
All patients were treated with primary chemotherapy
with anthracyline-containing regimens such as FEC (5-fluorouracil,
epirubicin, cyclophosphamide) or PEV (cisplatin, epirubicin,
vinorelbine).
After completing the neoadjuvant chemotherapy, 3–4
weeks after the last dose of treatment, patients underwent surgery
consisting of modified radical mastectomy or breastconserving
surgery. Postoperative adjuvant chemotherapy consisted of six
cycles of intravenous cyclophosphamide, methotrexate and
fluorouracil (CMF). The adjuvant treatment usually was initiated
3–4 weeks after surgery. Locoregional RT was performed during the
fourth course of CMF.
After completing the adjuvant chemotherapy, patients
with hormone receptor-positive tumors, if postmenopausal, received
tamoxifen for 5 years alone.
Clinical evaluations were performed every 3 months
for 2 years and every 6 months thereafter. Instrumental
examinations (e.g., mammography, liver ultrasound, chest X-ray,
bone scan and echocardiogram) were performed every 6 months for the
first 2 years and every 12 months thereafter for ≥5 years.
Immunohistochemical staining
This study was based on an analysis of
formalin-fixed, paraffin-embedded archival samples. Serial
microtome sections (6- to 7-μm thick) were treated for the
immunohistochemical staining of survivin and p53, using the
streptavidin-biotin alkaline phosphatase method. Water-bath,
heating-based antigen retrieval was performed by immersion in 10 mM
citrate buffer solution (pH 6.0) at 95°C for 40 min. After gradual
cooling for 20 min, the sections were treated for 45 min with 10%
normal goat or normal horse serum in PBS to block nonspecific
binding. Rabbit polyclonal antibody to recombinant human survivin
protein (1:2000; Novus Biologicals, Littleton, CO, USA), and mouse
monoclonal antibody to human p53 protein (1:50, clone DO-7; Dako,
Glostrup, Denmark) were used as primary antisera. Biotinylated
anti-rabbit and anti-mouse IgG were used as secondary antisera
(1:1000; Vector Laboratories, Burlingame, CA, USA). The sections
were further incubated in alkaline phosphatase-streptavidin
(1:1000; Vector Laboratories), and reacted with Fast Red Substrate
System (Dako).
In the experiment, all sections were thoroughly
rinsed in PBS between each step and were finally counterstained
with Mayer's hematoxylin and mounted in glycerol gelatin (Sigma,
St. Louis, MO, USA).
Sections of human cutaneous melanoma were used as
positive control tissues for survivin and p53 staining; negative
controls were obtained by omission of the primary antibody or by
replacing the primary antibody with an isotypematched antibody.
Positive and negative controls were run simultaneously.
Micrographs were captured by a digital camera Canon
PowerShot A620 (Canon Inc., Tokyo, Japan) on a microscope Zeiss
Axiophot (Carl Zeiss Inc., Oberkochen, Germany), and processed by
Adobe Photoshop software (version 7.0; Adobe Systems, Inc., San
Jose, CA, USA).
Evaluation of immunoreactivity
Results were independently evaluated by three
researchers (M.T.P., C.M. and P.D.) in a blinded fashion. Four to
six ×200 fields covering almost the whole of each of the four
sections per sample were examined with a 144-intersection point
square reticulum (0.78 mm2) inserted in the eyepiece and
scored for the percentage of immunoreactive cells.
The cutoff level for the immunohistochemical
analysis was set at 10%, meaning that those samples with >10% of
cells showing a moderate/strong intensity of nuclear and
cytoplasmic staining were considered to be positive.
Statistical analysis
Follow-up data were analyzed in September 2007.
Overall survival (OS) and disease-free survival (DFS) were
calculated based on the date of initial primary chemotherapy and
were analyzed using the Kaplan-Meier method. Statistical
comparisons between groups were performed using two-sided log-rank
tests. OS was defined as the time from study entry to the time of
death from any cause. DFS was defined as the time from study entry
to the time of local, regional or distant treatment failure,
occurrence of controlateral breast cancer or other second primary
cancer; or death without evidence of breast or a second primary
cancer. Multivariate analysis was performed using the Cox
regression model to assess additional prognostic values of the
different variables in relation to the expression of survivin.
Data were computed by the SPSS statistical software
package, version 15.0 (SPSS Inc., Chicago, IL, USA). All tests were
two-tailed, and a p-value of <0.05 was considered statistically
significant.
Results
All 53 patients were able to complete the
multimodality plan and therefore were evaluable for response to
primary chemotherapy. During neoadjuvant therapy, no case of
progressive disease was observed. The clinical response rate was
100% (95% CI, 65.2–89.5): complete clinical response (cCR) was
observed in 8 patients (15%) and partial clinical response (cPR) in
45 patients (85%). According to Sataloff's classification,
pathological complete response in the primary tumor (pCR) was
observed in 6 patients (11%), whereas pathological gross residual
tumor (pTR) was observed in 47 patients (89%). Major pathological
response in breast tissue was observed in 18 patients (34%). The
pathological lymph node (LN) assessment showed 12 patients with
pLN0 (23%) and 41 patients with pLN+ (77%). The expression of
survivin protein was positive in 21 patients (40%) and negative in
32 patients (60%); p53 immunostaining was detected in 13 cases
(25%) and 40 patients (75%) did not show any staining. Eleven
patients (21%) were both survivin- and p53-positive (Fig. 1).
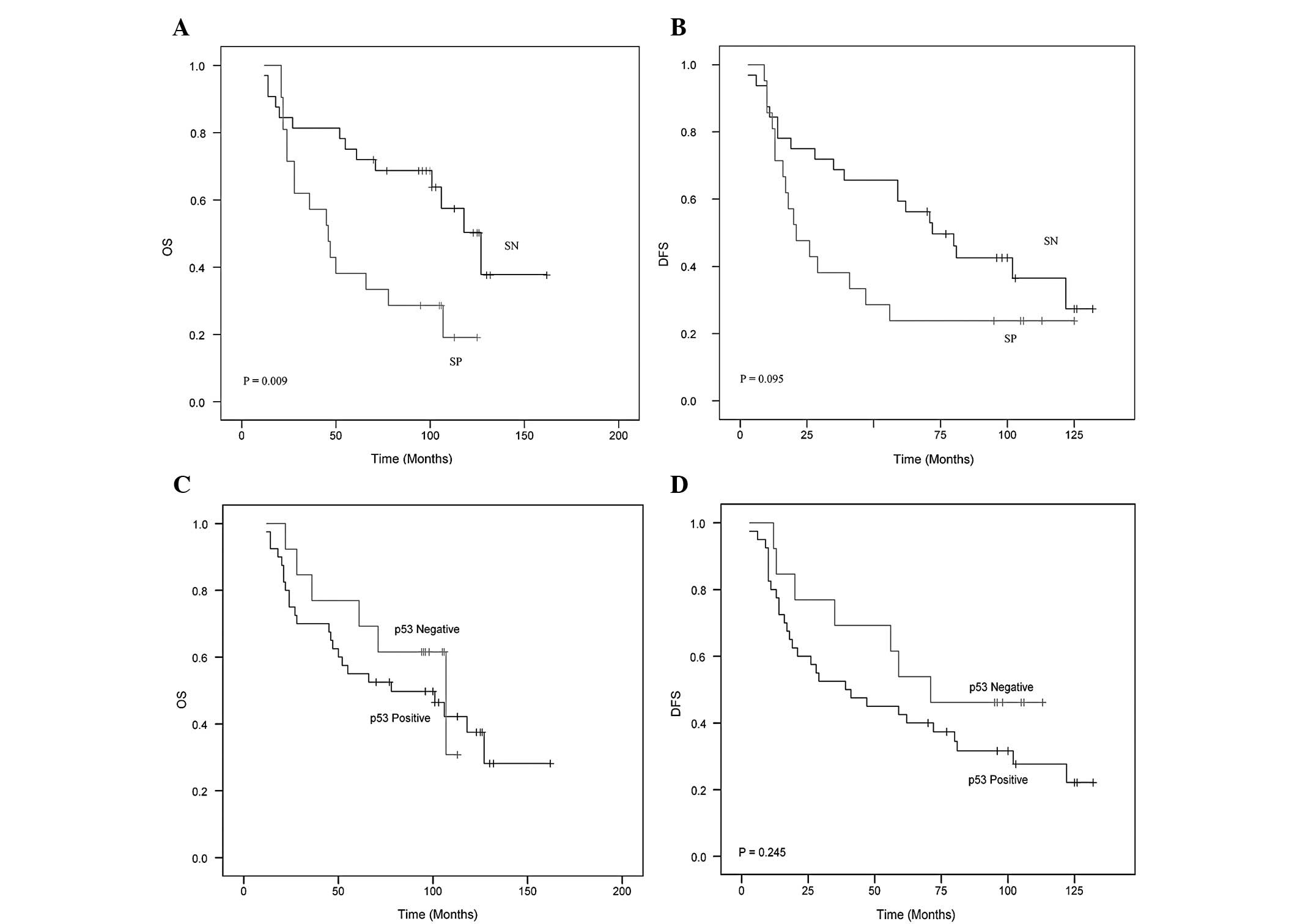
Global 5- and 10-year overall survival
and disease-free survival
In the entire group of 53 patients treated with
primary chemotherapy, the 5- and 10-year OS was 60.4 and 43.4%
respectively. The 5- and 10-year OS in the survivin-negative
patients was 75 and 56.3% respectively. The 5- and 10-year OS in
the survivin-positive patients was 38 and 23.8%, respectively
(p=0.009) (Fig. 2A).
The overall 5- and 10-year DFS was 45 and 32.1%,
respectively. The 5- and 10-year DFS in the 32 survivin-negative
patients was 59.4 and 37.5%, respectively. The 5- and 10-year DFS
in the 21 survivin-positive patients was 23.8% (p=0.095) (Fig. 2B).
Among the patients with p53-positive or -negative
expression, no statistically significant differences were observed
in terms of the 5- and 10-year DFS and OS (Fig. 2C and D).
Effect of independent predictors of
long-term overall survival in relation to the expression of
survivin
The statistical analysis performed using the
Cox-regression model on the patients with survivin-positivity
showed a hazard ratio (HR) of 2.6 (95% CI, 1.2–5.5; p=0.012). When
survivin-positivity was associated with several prognostic
variables (age, ER, PR, G2/3, Ki-67, stage T4d and HER2), the HR
ranged between 2.3 and 2.6. When survivin-positivity was associated
with the variable p53, the HR was 3.27 (95% CI, 1.5–7.2) (Table II).
| Table II.Effect of predictors on the 10-year
OS in relation to the expression of survivin in a multivariate
analysis performed using the Cox-regression model. |
Table II.
Effect of predictors on the 10-year
OS in relation to the expression of survivin in a multivariate
analysis performed using the Cox-regression model.
| Predictors | | HR | 95% CI | p-value |
|---|
|
Survivin-positivea | | 2.615 | 1.240–5.515 | 0.012 |
| Ageb | SP | 2.609 | 1.236–5.504 | 0.012 |
| ERb | SP | 2.343 | 1.083–5.070 | 0.031 |
| PgRb | SP | 2.265 | 1.030–4.982 | 0.042 |
| G2/3b | SP | 2.650 | 1.258–5.581 | 0.010 |
| HER2 statusb | SP | 2.612 | 1.238–5.509 | 0.012 |
|
p53-positiveb | SP | 3.279 | 1.491–7.213 | 0.003 |
| T4db | SP | 2.565 | 1.204–5.464 | 0.015 |
| Triple
negativeb | SP | 2.450 | 1.305–5.657 | 0.022 |
| Ki-67b | SP | 2.473 | 1.162–5.265 | 0.019 |
Discussion
The primary objective of our study was to
investigate the correlation between the expression of survivin
protein with long-term survival in a homogeneous group of stage T4
breast cancer patients treated with a multimodality treatment.
Survivin was detected in the nucleus and cytoplasm.
In these cases, the nuclear reaction was prominent with a low
cytoplasmic reaction. Other cases exhibited staining confined
exclusively to the cytoplasm. Mitotic figures were stained, and
survivin was also localized to mitotic spindles.
It is known that there are different survivin splice
variants with unique subcellular localizations and functions
(17). Among these, nuclear
variants appears to play a key role in cell division, whereas
cytoplasmic varients seem essential for the inhibition of apoptosis
(18).
It is not yet possible to quantify and study the
survivin proteins individually due to the lack of specific
antibodies (19). Thus, our
immunohistochemical localization in both the nuclei and cytoplasm,
obtained by an antibody recognizing all of the survivin proteins,
represented the combined expression of all variants.
In regards to potential prognostic factors, nuclear
or cytoplasmic survivin has been demonstrated to be an unfavorable
prognostic marker in several types of tumors, while other studies
have described nuclear or cytoplasmic survivin as a favorable
prognostic marker (20–24).
In our study, the statistical analysis showed that
the patients whose tumors did not express survivin had a better
outcome compared to survivin-positive tumors in terms of either DFS
or OS. These findings are not surprising in view of other works
showing that survivin expression is associated with a worse outcome
in several tumor types. Regarding breast cancer, as we previously
mentioned, there is still controversy on the exact value of
survivin as a prognostic factor.
In this regard, Kennedy et al (21) found a negative correlation between
survivin expression and survival, while the results of Tanaka et
al (12) appeared consistent
with our findings since survivin positivity was associated with a
worse outcome in a non-homogeneous series of patients with stage
I–III breast cancer. Similar results were also reported by Hinnis
et al (11) who found that
survivin positivity was significant associated with poor survival
in a series of breast cancer patients treated with chemotherapy or
hormone therapy.
In our study, which differed from others because of
a longer median follow-up period (125 months), we demonstrated, in
a homogeneous series of T4 breast cancer patients, that the
expression of survivin is associated with a significantly shorter
duration of overall survival [HR=2.6 (95% CI, 1.2–5.5)] (p=0.012)
even long-term.
Moreover, additional prognostic factors were
analyzed to evaluate their influence when associated, one by one,
with survivin positivity. In more detail, none of the prognostic
factors considered in this study except the variable p53 modified
the HR. Notably, p53 (HR=3.2) seemed to negatively enhance the
effect of survivin on survival. When we analyzed the outcome of
patients whose tumors were both p53- and survivin-positive, a
significant less favorable prognosis was observed. This finding may
be explained taking into consideration the tight relationship
between wild-type p53 and survivin which act in an opposite manner
(25). In fact, p53 negatively
regulates the expression of survivin. Conversely, the presence of
mutant p53 would translate with increased expression of survivin,
leading to the speculation that the combination of these two
molecular factors might have a synergistic negative effect on
survival.
In conclusion, our study demonstrated that survivin
expression in T4 breast cancer patients is a possible independent
prognostic factor which is maintained long-term. In the future,
additional large prospective studies are needed to validate the
expression of survivin as a potential novel biomarker for breast
cancer patients.
Acknowledgements
Particular thanks are due to Mrs Maria
Itala Mosso and Mr Massimo Annis for their expert technical
assistance.
References
|
1.
|
Ferlay J, Bray F, Pisani P and Parkin DM;
GLOBOCAN 2002: Cancer Incidence, Mortality and Prevalence
Worldwide. IARC Press. Lyon: 2004.
|
|
2.
|
Dowsett M and Dunbier AK: Emerging
biomarkers and new understanding of traditional markers in
personalized therapy for breast cancer. Clin Cancer Res.
14:8019–8026. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3.
|
Altieri DC: Molecular cloning of effector
cell protease receptor-1, a novel cell surface receptor for the
protease factor Xa. J Biol Chem. 269:3139–3142. 1994.PubMed/NCBI
|
|
4.
|
Altieri DC: Splicing of effector cell
protease receptor-1 mRNA is modulated by an unusual retained
intron. Biochemistry. 33:13848–13855. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Mita AC, Mita MM, Nawrocki ST and Giles
FJ: Survivin: key regulator of mitosis and apoptosis and novel
target for cancer therapeutics. Clin Cancer Res. 14:5000–5005.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Ambrosini G, Adida C and Altieri DC: A
novel antiapoptosis gene, survivin expressed in cancer and
lymphoma. Nat Med. 3:917–921. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Adida C, Crotty PL, McGrath J, et al:
Developmentary regulated expression of the novel cancer
antiapoptosis gene survivin in human and mouse differentiation. Am
J Pathol. 152:43–49. 1998.PubMed/NCBI
|
|
8.
|
Olie RA, Simões-Wüst AP, Baumann B, et al:
A novel antisense oligonucleotide targeting survivin expression
induces apoptosis and sensitizes lung cancer cells to chemotherapy.
Cancer Res. 60:2805–2809. 2000.
|
|
9.
|
Sah NK, Khan Z, Khan GJ and Bisen PS:
Structural, functional and therapeutic biology of survivin. Cancer
Lett. 244:164–171. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
O'Driscoll L, Linehan R, Kennedy MS, et
al: Lack of prognostic significance of survivin, survivin-ΔEx3,
survivin-2B, galectin-3, bag-1, bax-α and MRP-1 mRNAs in breast
cancer. Cancer Lett. 201:225–236. 2003.
|
|
11.
|
Hinnis AR, Luckett JCA and Walker RA:
Survivin is an independent predictor of short-term survival in poor
prognostic breast cancer patients. Br J Cancer. 96:639–645. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Tanaka K, Iwamoto S, Gon G, et al:
Expression of survivin and its relationship to loss of apoptosis in
breast carcinomas. Clin Cancer Res. 6:127–134. 2000.PubMed/NCBI
|
|
13.
|
Bertheau P, Espié M, Turpin E, et al: TP53
status and response to chemotherapy in breast cancer. Pathobiology.
75:132–139. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Brennan DJ, Rexhepaj E, O'Brien SL, et al:
Altered cytoplasmic-to-nuclear ratio of survivin is a prognostic
indicator in breast cancer. Clin Cancer Res. 14:2681–2689. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Hayward JL, Carbone PP, Heusen JC, et al:
Assessment of response to therapy in advanced breast cancer. Br J
Cancer. 35:292–298. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Sataloff DM, Mason BA, Prestipino AJ, et
al: Pathologic response to induction chemotherapy in locally
advanced carcinoma of the breast: a determinant of outcome. J Am
Coll Surg. 180:297–306. 1995.PubMed/NCBI
|
|
17.
|
Li F and Ling X: Survivin study: an update
of ‘what is the next wave’? J Cell Physiol. 208:476–486. 2006.
|
|
18.
|
Dohi T, Beltrami E, Wall NR, Plescia J and
Altieri DC: Mitochondrial survivin inhibits apoptosis and promotes
tumorigenesis. J Clin Invest. 114:1117–1127. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Li XN, Shu Q, Su JM, et al: Differential
expression of survivin splice isoforms in medulloblastomas.
Neuropathol Appl Neurobiol. 33:67–76. 2007.PubMed/NCBI
|
|
20.
|
Altieri DC and Marchisio PC: Survivin
apoptosis: an interloper between cell death and cell proliferation
in cancer. Lab Invest. 79:1327–1333. 1999.PubMed/NCBI
|
|
21.
|
Kennedy SM, O'Driscoll L, Purcell R, et
al: Prognostic importance of survivin in breast cancer. Br J
Cancer. 88:1077–1083. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Ponnelle T, Chapusot C, Martin L, et al:
Cellular localisation of survivin: impact on the prognosis in
colorectal cancer. J Cancer Res Clin Oncol. 131:504–510. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Xie D, Zeng YX, Wang HJ, et al: Expression
of cytoplasmic and nuclear survivin in primary and secondary human
glioblastoma. Br J Cancer. 94:108–114. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Piras F, Murtas D, Minerba L, et al:
Nuclear survivin is associated with disease recurrence and poor
survival in patients with cutaneous malignant melanoma.
Histopathology. 50:835–842. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Mirza A, McGuirk M, Hockenberry TN, et al:
Human survivin is negatively regulated by wild-type p53 and
participates in p53-dependent apoptotic pathway. Oncogene.
21:2613–2622. 2002. View Article : Google Scholar : PubMed/NCBI
|