Introduction
The thiopurine drugs, azathioprine (AZA) and
6-mercaptopurine (6-MP), are the most common drugs used to maintain
clinical remission in inflammatory bowel diseases (IBDs) such as
Crohn’s disease (CD) and ulcerative colitis (UC) (1–3).
However, in 15–30% of patients, these drugs have to be discontinued
due to adverse effects including bone marrow suppression,
hepatotoxicity, pancreatitis, fever, rash and gastrointestinal
intolerance (4–9). Furthermore, an AZA dosage of 2–3
mg/kg is recommended for the treatment of IBD patients in Western
countries (10), but lower doses
of AZA (0.6–1.2 mg/kg/day) are used in Japanese patients due to
their relatively heightened sensitivity (11).
Considerable interest has focused on the metabolism
of thiopurines as a means of individualizing therapy to minimize
any adverse effects and to maximize the clinical response. AZA and
6-MP are metabolized to 6-thioguanine nucleotide (6-TGN) (12,13).
The cytotoxic and immunosuppressive properties of AZA/6-MP are
mediated by 6-TGN, which incorporates into the DNA, thus leading to
DNA breakage and an inhibition of immune cell proliferation
(12). Susceptibility to bone
marrow toxicity upon AZA/6-MP therapy is genetically dependent on
inter-individual variations in thiopurine S-methyltransferase
(TPMT) enzyme activity, based on the genetic polymorphisms of
low-metabolizing alleles (12,13).
In the Japanese population, a single nucleotide polymorphism (SNP),
TPMT A719G, is the most prevalent allele (∼2%), and other
variants are very rare (7,14–16).
Genetic polymorphism of inosine triphosphate
pyrophosphatase (ITPase) has also been suspected as a factor
responsible for thiopurine intolerance (5,16–19).
ITPase catalyzes the breakdown of inosine triphosphate as part of a
futile cycle in the purine metabolic pathway (5). Genetic ITPase deficiency results in
the cellular accumulation of thioinosine triphosphate (TITP) and
causes thiopurine-associated toxicity (16,19).
Multidrug resistance protein 4 (MRP4/ABCC4) belongs
to the MRP family of drug transporters (20–23).
MRP4 is localized in the plasma membrane and shows an ATP-dependent
transport of a broad range of compounds including nucleoside
monophosphate analogs such as 6-MP and 6-TGN. Recently,
Krishnamurthy et al identified an SNP in the human
MRP4 gene (G2269A; rs3765534) that dramatically reduces MRP4
function by impairing its cell membrane localization, thus
resulting in myelosuppression (21). Database screens suggest a >18.7%
allelic frequency of MRP4 single nucleotide polymorphisms
(SNPs) in the Japanese population (21), while it is much less frequent in
other populations (21). Direct
sequence analyses in our laboratory indicated that the allelic
frequency of MRP4 G2269A was 14.7% in the Japanese
population (24). In IBD patients
treated with AZA/6-MP, the WBC count was significantly lower in
patients with the MRP4 G2269A SNP than in patients with a
wild allelotype (24). Thus,
MRP4 G2269A is a new genetic factor accounting for
thiopurine sensitivity in the Japanese population.
SNP genotyping is integrated together with therapy
for selecting treatments as well as for monitoring results. Rapid
and cost-effective methods must be developed for genotyping, and it
would be desirable to include this information in patient records
as a guide for physicians to individualize treatment. We previously
utilized polymerase-chain reaction-restriction fragment length
polymorphism (PCR-RFLP) analyses for the determination of the
TPMT and ITPase genotypes (24–26),
and used direct-sequencing analysis for MRP4 (24). However, these methods require
multiple steps and are time-consuming.
In this study, we investigated the usefulness of the
TaqMan® PCR assay for the rapid detection of SNPs of TPMT,
ITPase and MRP4. This may potentially lead to improved
safety and efficacy for thiopurine therapy in individual IBD
patients.
Patients and methods
Patients
We enrolled 44 healthy volunteers (female/male:
23/21) and 235 IBD patients (UC, n=157; CD, n=78) attending the
Gastroenterology Outpatient Clinic at the Hospital of the Shiga
University of Medical Science. All subjects were Japanese. The
protocol of this study was approved by the Ethics Committee of the
Shiga University of Medical Science.
TaqMan® PCR assay (Applied
Biosystems, Foster City, CA)
Genotyping for TPMT A719G (rs1142345),
ITPase C94A (rs1127354) and MRP4 G2269A (rs3765534)
was performed using Custom TaqMan SNP genotyping assays in which a
fluorogenic probe, consisting of an oligonucleotide labeled with
both a fluorescent reporter dye (FAM or VIC) and a quencher dye, is
included in a typical PCR. Amplification of the probe-specific
product causes cleavage of the probe, generating an increase in
reporter fluorescence (27,28).
Each primer and probe set was used in the TaqMan SNP genotyping
assays (ID: C_19567_20, C_27465000_10 and C_27478235_20; Applied
Biosystems) in accordance with the information on the Applied
Biosystems website (http://www.appliedbiosystems.com).
The PCR was performed according to the
manufacturer’s instructions provided by Applied Biosystems. The PCR
thermal cycling was as follows: initial denaturing at 95°C for 30
sec; 40 cycles of 92°C for 5 sec and 60°C for 20 sec. Thermal
cycling was performed using a LightCycler 480 system (Roche
Diagnostics, Switzerland). Each 96-well plate contained 80 samples
of an unknown genotype and 4 reaction mixtures containing the
reagents, but no DNA (no-template control). The no-DNA control
samples were necessary for the Sequence Detection System (SDS) 7700
signal processing, as outlined in the TaqMan Allelic Discrimination
Guide. The genotypes were determined visually based on the dye
component fluorescent emission data depicted in the X-Y
scatter-plot of the SDS software.
Genotyping of MRP4 G2269A by direct
sequencing
Mononuclear cells were isolated from heparinized
blood using a Ficoll density gradient. The genomic DNA was isolated
using a DNA extraction kit purchased from Qiagen (Valencia, CA).
MRP4 exon 18 encompassing 2269 SNPs was amplified from
genomic DNA by the use of forward 5′-TCCAGTGGCTGATTTTCTGA-3′ and
reverse 5′-GAGTGTAAACTGCGGTGGT-3′ primers (21) under the following conditions: 95°C
for 5 min, followed by 32 cycles of 95°C for 30 sec, 59°C for 40
sec and 72°C for 40 sec. The sequencing was carried out on an ABI
PRISM 3130 Automated Sequencer (Applied Biosystems, Carlsbad,
CA).
Genotyping of TPMT and ITPase
The TPMT and ITPase genotypes were
determined by polymerase-chain reaction-restriction fragment length
polymorphism (PCR-RFLP) analyses. The PCR primers and PCR protocol
were designed according to a previously described method (25,26).
Results
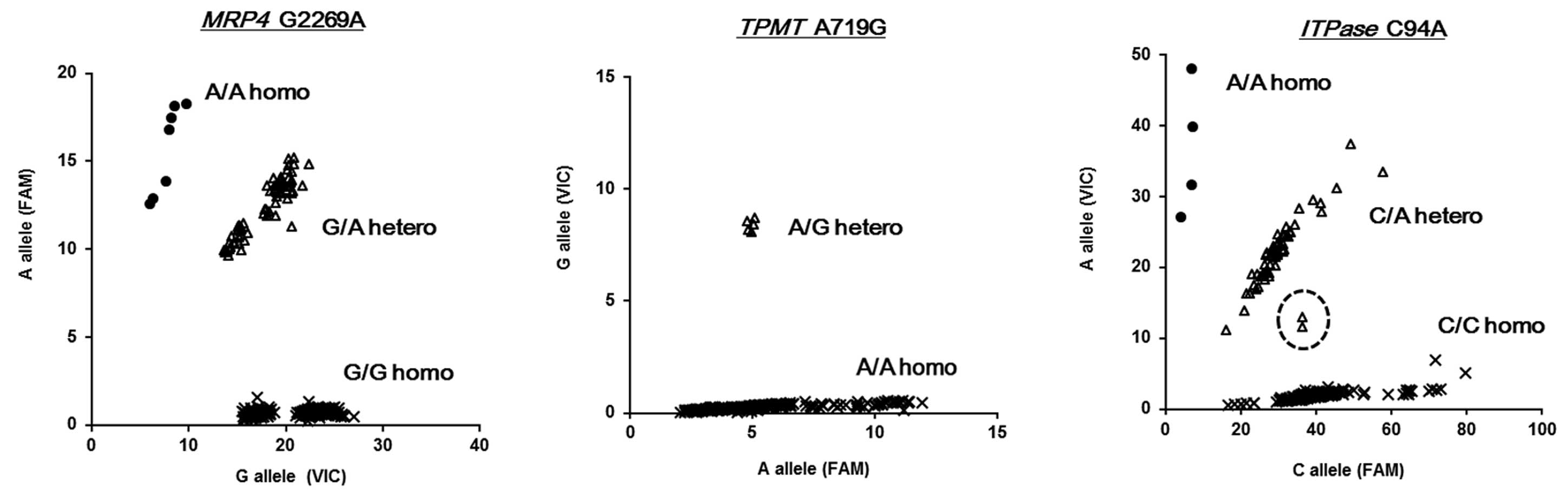
We first genotyped the MRP4 G2269A
(rs3765534) SNP in 279 DNA samples using the TaqMan assay,
achieving a success rate of 100% (279/279) (Fig. 1 and Table I). The allelogram showed a clear
separation of the MRP4 G2269A SNPs (Fig. 1). These results were compared with
our previous data obtained by the direct-sequencing assay (G/G 204,
G/A 68 and A/A 7) (24) (Table I), which we routinely use for
MRP4 G2269A SNP typing. A comparison of the two methods
yielded one discordant result (TaqMan was G/G, and sequencing
result was G/A). This was re-sequenced and the TaqMan assay was
correct. Thus, we calculated the overall accuracy of the TaqMan
assay for MRP4 G2269A (rs3765534) at 100% (279/279). The
allele distribution in IBD patients is shown in Table II. The allele frequency of
MRP4 G2269A was 0.145.
 | Table I.Comparison of the results of the
allele distribution determined by the TaqMan assay and direct
sequence and PCR-RFLP methods. |
Table I.
Comparison of the results of the
allele distribution determined by the TaqMan assay and direct
sequence and PCR-RFLP methods.
| Genotype allele | Methods
|
|---|
| TaqMan | Direct sequence | PCR-RFLP |
|---|
| MRP4
G2289A | | | |
| G/G
(wild-type) | 205 | 204 | |
| G/A | 67 | 68 | |
| A/A | 7 | 7 | |
| Allele
frequency | 0.145 | | |
| TPMT
A719G | | | |
| A/A
(wild-type) | 274 | | 274 |
| G/G | 5 | | 5 |
| Allele
frequency | 0.009 | | |
| ITPase
C94A | | | |
| C/C
(wild-type) | 215 | | 212 |
| C/A | 60 | | 61 |
| A/A | 4 | | 6 |
| Allele
frequency | 0.121 | | |
| Table II.Allele distribution determined by the
TaqMan assay in IBD patients. |
Table II.
Allele distribution determined by the
TaqMan assay in IBD patients.
| Genotype
allele | UC | CD | Healthy |
|---|
| MRP4
G2289A | | | |
| G/G
(wild-type) | 117 | 56 | 32 |
| G/A | 36 | 21 | 10 |
| A/A | 4 | 1 | 2 |
| TPMT
A719G | | | |
| A/A
(wild-type) | 155 | 76 | 43 |
| G/G | 2 | 2 | 1 |
| ITPase
C94A | | | |
| C/C
(wild-type) | 124 | 60 | 31 |
| C/A | 30 | 17 | 13 |
| A/A | 3 | 1 | 0 |
Next, we genotyped TPMT A719G (rs1142345)
using the TaqMan assay, achieving a success rate of 100% (Fig. 1). The results of TPMT A719G
were also clearly separated in allelograms, and were identical with
the results for PCR-RFLP (Table
I). The allele distribution in IBD patients is shown in
Table II, and the allele frequency
of TPMT A719G was 0.009.
The TaqMan assay for ITPase C94A also
achieved a success rate of 100%. The allelogram showed the two
outliers that could not be easily assigned genotypes (dotted circle
in ITPase C94A allelogram; Fig.
1). These were directly sequenced and assigned to C/A
heterozygotes. A comparison between TaqMan assay and PCR-RFLP
analyses yielded 12 discordant results for ITPase C94A
(Table I and III), and direct sequencing indicated that
the results of the TaqMan assay were correct. The allele
distribution in IBD patients is shown in Table II. The allele frequency of
ITPase C94A was 0.121.
| Table III.Discordant results for ITPase
C94A determined by PCR-RFLP and TaqMan assay. |
Table III.
Discordant results for ITPase
C94A determined by PCR-RFLP and TaqMan assay.
| PCR-RFLP | TaqMan | n |
|---|
| C/A | C/C | 6 |
| C/A | A/A | 1 |
| C/C | C/A | 3 |
| A/A | C/A | 2 |
| Total | | 12 |
Discussion
Thiopurines are effective immunosuppressants for IBD
patients, but the intracellular accumulation of 6-TGNs causes
dose-limiting hematopoietic toxicity. In particular, Japanese
populations are sensitive to thiopurines, and relatively lower
doses of AZA (0.6–1.2 mg/kg/day) are recommended for the treatment
of Japanese IBD patients (11).
Similar to TPMT A719G and ITPase C94A, we recently
showed that MRP4 G2269A is a new factor accounting for
heightened thiopurine sensitivity in Japanese patients with IBD
(24). Although the SNPs
accounting for thiopurine sensitivity have been reported as
important factors for individualizing therapy to minimize adverse
effects and to maximize clinical response, a rapid and clinically
applicable method for the SNP genotyping of these genes has not yet
been established.
TaqMan® assays are a reliable method for
SNP genotyping (27,29). Good genotyping data can usually be
obtained in a short time using a small amount of genomic DNA, and
many samples can be processed simultaneously. In the present study,
we used the TaqMan assay for the typing of SNPs responsible for
thiopurine sensitivity, and accurately genotyped targeted SNPs. In
the assays for ITPase C94A, we detected two outliers which
were confirmed to be C/A heterozygotes by direct sequencing. The
precise reasons for this phenomenon remain unclear, but incomplete
digestion of the fluorescent-probe by the 5′-nuclease activity of
TaqDNA-polymerase was suspected (30). The TaqMan assays for MRP4
G2269A and TPMT A719G showed no outliers, and clearly
separated the genotypes in allelograms.
We routinely use direct sequencing for MRP4
and PCR-RFLP for TPMT and ITPase SNP genotyping.
There was one discordant result between the TaqMan assays and
previously performed sequencing data for MRP4 G2269A.
Re-sequencing indicated that the TaqMan assay was correct.
Discordant results for ITPase C94A between the TaqMan assays
and PCR-RFLPs were detected in 12 samples. Direct-sequencing data
supported the accuracy of the results of the TaqMan assays, and
incomplete digestion or unclear visualization of the restriction
fragments may have caused genotyping errors in the PCR-RFLP
assays.
The advantages of the present genotyping method are
its accuracy, ease of use and the short processing time. The
disadvantage of the present method is the requirement of special
PCR machines. The accurate SNP typing of an individual patient
among a population with different sensitivities to drugs is
critically important for the determination of therapeutic
strategies. When 96-well plates are used, the TaqMan assay enables
a simultaneous analysis of at least 20 samples for the detection of
3 SNPs. Furthermore, one analysis requires approximately 2 h. Thus,
TaqMan assays for SNP genotyping responsible for thiopurine
sensitivity may provide a great advantage for the management of IBD
patients with thiopurine drug treatment.
In conclusion, we successfully genotyped the SNPs
responsible for thiopurine sensitivity using TaqMan® SNP
assays. This method was very accurate and convenient. We believe
that this technique is useful for the treatment of IBD patients to
avoid the adverse events of thiopurine drugs.
References
|
1.
|
Adler DJ and Korelitz BI: The therapeutic
efficacy of 6-mercaptopurine in refractory ulcerative colitis. Am J
Gastroenterol. 85:717–722. 1990.PubMed/NCBI
|
|
2.
|
Sandborn W, Sutherland L, Pearson D, May
G, Modigliani R and Prantera C: Azathioprine or 6-mercaptopurine
for inducing remission of Crohn’s disease. Cochrane Database Syst
Rev. 6:CD0005452000.
|
|
3.
|
Hibi T and Ogata H: Novel
pathophysiological concepts of inflammatory bowel disease. J
Gastroenterol. 41:10–16. 2006. View Article : Google Scholar
|
|
4.
|
Gearry RB, Barclay ML, Burt MJ, Collett JA
and Chapman BA: Thiopurine drug adverse effects in a population of
New Zealand patients with inflammatory bowel disease.
Pharmacoepidemiol Drug Saf. 13:563–567. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Van Dieren JM, Hansen BE, Kuipers EJ,
Nieuwenhuis EE and Van der Woude CJ: Meta-analysis: inosine
triphosphate pyrophosphatase polymorphisms and thiopurine toxicity
in the treatment of inflammatory bowel disease. Aliment Pharmacol
Ther. 26:643–652. 2007.
|
|
6.
|
Gisbert JP and Gomollon F:
Thiopurine-induced myelotoxicity in patients with inflammatory
bowel disease: a review. Am J Gastroenterol. 103:1783–1800. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Takatsu N, Matsui T, Murakami Y, et al:
Adverse reactions to azathioprine cannot be predicted by thiopurine
S-methyltransferase genotype in Japanese patients with inflammatory
bowel disease. J Gastroenterol Hepatol. 24:1258–1264. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Lees CW, Maan AK, Hansoti B, Satsangi J
and Arnott ID: Tolerability and safety of mercaptopurine in
azathioprine-intolerant patients with inflammatory bowel disease.
Aliment Pharmacol Ther. 27:220–227. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Winter JW, Gaffney D, Shapiro D, et al:
Assessment of thiopurine methyltransferase enzyme activity is
superior to genotype in predicting myelosuppression following
azathioprine therapy in patients with inflammatory bowel disease.
Aliment Pharmacol Ther. 25:1069–1077. 2007. View Article : Google Scholar
|
|
10.
|
Lichtenstein GR, Sbreu MT, Cohen R and
Tremaine W: American Gastroenterological Association Institute
technical review on corticosteroids, immunomodulators, and
infliximab in inflammatory bowel disease. Rev Gastroenterol Mex.
71:351–401. 2006.(In Spanish).
|
|
11.
|
Hibi T, Naganuma M, Kitahora T, Kinjyo F
and Shimoyama T: Low-dose azathioprine is effective and safe for
maintenance of remission in patients with ulcerative colitis. J
Gastroenterol. 38:740–746. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Derijks LJ, Gilissen LP, Engels LG, et al:
Pharmacokinetics of 6-thioguanine in patients with inflammatory
bowel disease. Ther Drug Monit. 28:45–50. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Haglund S, Taipalensuu J, Peterson C and
Almer S: IMPDH activity in thiopurine-treated patients with
inflammatory bowel disease – relation to TPMT activity and
metabolite concentrations. Br J Clin Pharmacol. 65:69–77.
2007.PubMed/NCBI
|
|
14.
|
Ban H, Andoh A, Tanaka A, et al: Analysis
of thiopurine S-methyltransferase genotypes in Japanese patients
with inflammatory bowel disease. Intern Med. 47:1645–1648. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Hiratsuka M, Inoue T, Omori F, Agatsuma Y
and Mizugaki M: Genetic analysis of thiopurine methyltransferase
polymorphism in a Japanese population. Mutat Res. 448:91–95. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16.
|
Uchiyama K, Nakamura M, Kubota T, Yamane
T, Fujise K and Tajiri H: Thiopurine S-methyltransferase and
inosine triphosphate pyrophosphohydrolase genes in Japanese
patients with inflammatory bowel disease in whom adverse drug
reactions were induced by azathioprine/6-mercaptopurine treatment.
J Gastroenterol. 44:197–203. 2009. View Article : Google Scholar
|
|
17.
|
Kurzawski M, Dziewanowski K, Lener A and
Drozdzik M: TPMT but not ITPA gene polymorphism influences the risk
of azathioprine intolerance in renal transplant recipients. Eur J
Clin Pharmacol. 65:533–540. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Allorge D, Hamdan R, Broly F, Libersa C
and Colombel JF: ITPA genotyping test does not improve detection of
Crohn’s disease patients at risk of azathioprine/6-mercaptopurine
induced myelosuppression. Gut. 54:5652005.
|
|
19.
|
Zelinkova Z, Derijks LJ, Stokkers PC, et
al: Inosine triphosphate pyrophosphatase and thiopurine
s-methyltransferase genotypes relationship to azathioprine-induced
myelosuppression. Clin Gastroenterol Hepatol. 4:44–49. 2006.
View Article : Google Scholar
|
|
20.
|
Wielinga PR, Reid G, Challa EE, et al:
Thiopurine metabolism and identification of the thiopurine
metabolites transported by MRP4 and MRP5 overexpressed in human
embryonic kidney cells. Mol Pharmacol. 62:1321–1331. 2002.
View Article : Google Scholar
|
|
21.
|
Krishnamurthy P, Schwab M, Takenaka K, et
al: Transporter-mediated protection against thiopurine-induced
hematopoietic toxicity. Cancer Res. 68:4983–4989. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Peng XX, Shi Z, Damaraju VL, et al:
Up-regulation of MRP4 and down-regulation of influx transporters in
human leukemic cells with acquired resistance to 6-mercaptopurine.
Leuk Res. 32:799–809. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Borst P, Evers R, Kool M and Wijnholds J:
A family of drug transporters: the multidrug resistance-associated
proteins. J Natl Cancer Inst. 92:1295–1302. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Ban H, Andoh A, Imaeda H, et al: The
multidrug-resistance protein 4 polymorphism is a new factor
accounting for thiopurine sensitivity in Japanese patients with
inflammatory bowel disease. J Gastroenterol. 45:1014–1021. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Yates CR, Krynetski EY, Loennechen T, et
al: Molecular diagnosis of thiopurine S-methyltransferase
deficiency: genetic basis for azathioprine and mercaptopurine
intolerance. Ann Intern Med. 126:608–614. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Marinaki AM, Ansari A, Duley JA, et al:
Adverse drug reactions to azathioprine therapy are associated with
polymorphism in the gene encoding inosine triphosphate
pyrophosphatase (ITPase). Pharmacogenetics. 14:181–187. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Hui L, DelMonte T and Ranade K: Genotyping
using the TaqMan assay. Current Protocols Human Genetics. Haines
JL: John Wiley; New York: 2008, View Article : Google Scholar
|
|
28.
|
Mitani Y, Lezhava A, Sakurai A, et al:
Rapid and cost-effective SNP detection method: application of
SmartAmp2 to pharmaco-genomics research. Pharmacogenomics.
10:1187–1197. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29.
|
Morita A, Nakayama T, Doba N, Hinohara S,
Mizutani T and Soma M: Genotyping of triallelic SNPs using TaqMan
PCR. Mol Cell Probes. 21:171–176. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30.
|
Livak KJ: Allelic discrimination using
fluorogenic probes and the 5′ nuclease assay. Genet Anal.
14:143–149. 1999.
|