Contents
Introduction
Background
Rationale
Methods for conducting information search
Government agenda
Cameroon cancer statistics
Quality of care to cancer patients in Cameroon
Government interventions
National cancer control
Community interventions
Current status of radiotherapy and chemotherapy
services in Africa and Cameroon
Limitations in resources: Anticancer drugs
Limitations of resources: Radiotherapy
Ethno-search for cancer therapy in Cameroon
Clinical cancer study efforts
Knowledge gaps
Conclusion
Introduction
Cancer is considered the leading cause of death in
developed countries and the second leading cause of death in
developing countries (1–5).The burden of cancer is notably heavier
in developing countries due to factors including age and lifestyle
choices such as smoking, physical inactivity, and consumption of
genetically modified foods that may lead to cancer (6). Approximately 12.7 million cancer
cases and 7.6 million cancer deaths are estimated to have occurred
in 2008 worldwide, with 56% of the cases and 64% of the deaths in
the economically developing world (7,8).
Deaths from cancer worldwide are projected to continue rising, with
an estimated 13.1 million deaths expected in 2030 (9,10).
In 2008, 715,000 new cases of cancer and 542,000 new
cancer deaths were recorded in Africa, rendering cancer an emerging
public health concern (12). These
numbers are likely to double within the next 20 years for the
reasons mentioned above (1).
Furthermore, an increase in the frequency of diagnosis of various
types of cancer such as lung, female breast and prostate cancers
has been observed due to lifestyle changes and detection practices
associated with urbanization and economic development (7,8). In
Cameroon, cancer accounts for 3% of deaths from all ages annually
(1–4) and the cancer risk for both males and
females prior to the age of 75 is 8.7% (Table I). Data concerning cancer
statistics in Cameroon are generally lacking at national and
institutional levels. Therefore, the aim of this review was to
assess some cases from the perspective of Cameroon as a developing
or low-income country.
 | Table ICancer prevalence and mortality in
Cameroon (73). |
Table I
Cancer prevalence and mortality in
Cameroon (73).
|
Characteristics | Male | Female | Both genders |
|---|
| Population
(thousands) | 9,538 | 9,549 | 19,088 |
| Number of new
cancer cases (thousands) | 5.4 | 6.3 | 11.7 |
| Age-standardized
rate (W) | 88.8 | 96.5 | 92.1 |
| Cancer risk prior
to age 75 (%) | 8.2 | 9.2 | 8.7 |
| Number of cancer
deaths (thousands) | 4.6 | 4.4 | 9.0 |
| Age-standardized
rate (W) | 76.8 | 70.5 | 73.1 |
Our knowledge regarding cancer prevention and
control has increased, yet the number of cancer cases is on the
increase. Should this trend continue, 16.5 million new cases of
cancer are expected to be diagnosed in 2020 (1–4) with
an approximate 10 million deaths expected, two-thirds of which are
likely to occur in developing nations (14). Although obtaining government
subsidies is crucial for the diagnosis and treatment of cancer
patients in Cameroon, cancer drugs remain both expensive and
scarce. Through the National Cancer Control Programs, the state of
Cameroon together with partners such as Sanofi Aventis is
attempting to ensure accessibility to drugs in a cost-effective
manner (15).
Cameroon has recently followed the global trend of
directing attention towards the search for alternative treatments
and the use of active herbal compounds for the treatment of cancer
and other diseases. In Cameroon, terpenoid plants such as
Hypericum lanceolatum(16)
have been identified as extremely potent anti-parasitic agents but
have demonstrated poor antimicrobial effects (17–19).
This review discusses the scope and potential impact of natural
products from Cameroon as anticancer remedy.
Background
Cameroon is a central African country whose natural
environment covers four bio-ecological zones from south to north:
the equatorial forest, the Guinea savannah, the Sahel savannah and
the encroaching desertification in the far north. Commonly referred
to as Africa in miniature, Cameroon has an estimated 250
ethno-linguistic groups from five regional-cultural groups spread
across the various ecological zones: the Semi-Bantus (western
highlanders) including the Bamileke, Bamoun and numerous smaller
entities in the North-West situated in the Guinea Savannah, who
constitute 38% of the population; the Bantus, coastal tropical
forest peoples, including the Bassa, Douala and numerous smaller
entities in the South-West, who constitute 12% of the population;
the southern tropical forest peoples, including the Ewondo, Bulu,
and Fang (all Beti subgroups), Maka and Pygmies (known as Bakas),
who constitute 18% of population; the predominantly Islamic peoples
of the northern regions (the Sahel) and central highlands,
including the Fulani, who constitute 18%; and the Hamites and
Semites peoples of the Sahel and central highlands, who constitute
14% of the population (20–22).
This ethnic and cultural diversity impacts on the perception,
treatment-seeking behavior and care for cancer and related
illnesses.
According to the 2008 statistics of the WHO, the
population of Cameroon is 19.088 million, and as with the majority
of African countries, has a low-income economy (1–4).
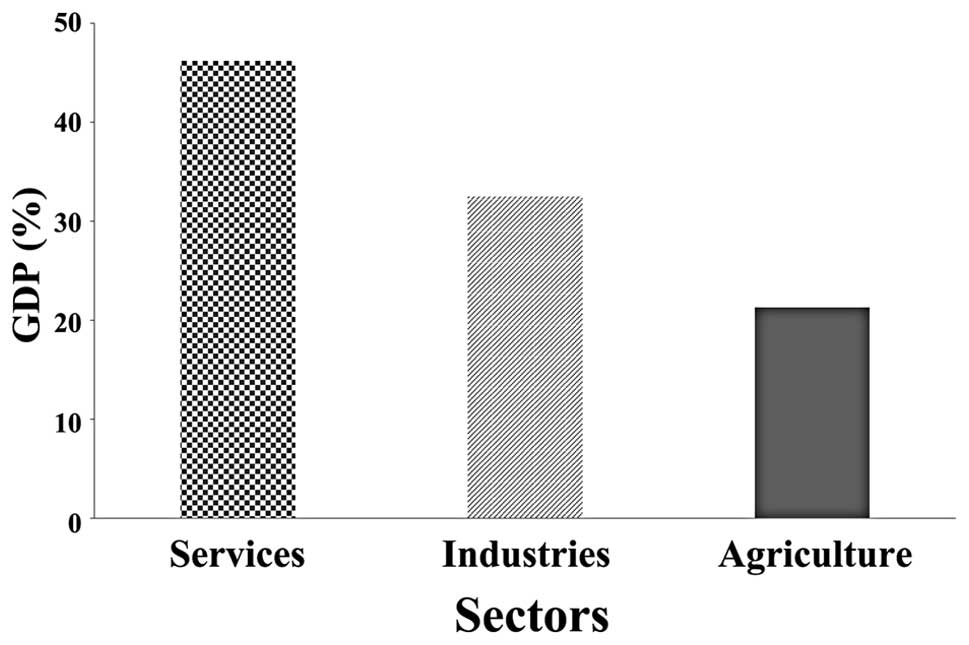
Over the past 5 years the average gross domestic product (GDP)
growth of the country has been 3.5%, below the originally estimated
5% and drawn mainly from three sectors (Fig. 1) (23). Recent figures have revealed that,
between 2000 and 2009 the country experienced economic growth at an
average annual rate of 3% (24).
An increase in the growth of trade with a valued import and export
of 56% has also been observed (24). As such, there are ongoing social
and economic changes resulting in increased urbanization with
potentially negative consequences that could affect health in the
short- or long-term.
However, there is great disparity in the
distribution of wealth generated by economic growth, with 32.8% of
the Cameroonian population living below the poverty line
(<US$1/day) (1–4). Thus, the poverty-stricken primary
victims of cancer and other diseases have limited access to health
services, due to the high cost of diagnosis and treatment (∼2.1
million francs) (25,26). The cost of health services is
beyond the means of an average Cameroonian according to officials
of the National Cancer Control Committee (NCCC) (23,25,27).
As a consequence of the aforementioned socio-economic changes,
Cameroon may now be experiencing a double burden of infectious and
chronic non-communicable diseases (NCDs). The burden of infectious
diseases largely driven by malaria, HIV/AIDS and tuberculosis is
already weighing heavily on the economy. However, an increase in
the burden of NCDs, exhibiting elements of a health transition, in
which a combination of acute and chronic diseases coexist in the
same population and compete for limited resources has been a
critical issue (13,27).
Rationale
In their global statistic paper, Jemal et al
(7,8) concluded that a ‘significant
proportion of the worldwide burden of cancer could be prevented
through the application of existing cancer control knowledge, and
by implementing programs for tobacco control, vaccination (for
liver and cervical cancers) and early detection and treatment, as
well as public health campaigns promoting physical activity and
healthier dietary patterns’ and that ‘implementing and sustaining
such actions requires concerted efforts among private and
government public health agencies and the pharmaceutical industry,
as well as individual and government donors’. In this study, we
assess the efforts made by both the government and private sector
in the fight against cancer in Cameroon in the areas of research,
treatment and prevention. Emphasis is laid on research activities
in the field of cancer, particularly in the area of anticancer
research with regard to herbal sources and alternative treatments
(28–30). Key questions to be addressed
include: i) whether the cause of the increased incidence of cancers
can be identified; ii) which interventions are effective and which
interventions fail to improve the quality of care of the cancer
care receiver; iii) how to utilize the local and unique natural
resources to reduce the cost of cancer treatment. These questions
may be addressed by examining the literature available on the
prospect of cancer research in Cameroon with a focus on the impact
of natural resources and research on cancer treatment and
prevention.
Methods for conducting information
search
The literature was reviewed and a search was
conducted using keywords including cancer, Cameroon, epidemiology,
management, research, herbs, as well as a combination of these in
different permutations. A number of studies on cancer and
associated diseases in Cameroon were reviewed for this study
(1–4,15,18–20).
The review focused on published and gray literature on anticancer
activities of the government of Cameroon, Cameroonians and all
stakeholders involved in the domain of cancer. Cameroonian
investigators as well as research organizations on cancer were also
contacted for additional information and gray literature. The
search was also carried out in the TUTCM e-library. Search methods
were manual and electronic. Databases and search engines including
Google, Yahoo, Hinari and PubMed were searched to access other
relevant publications. International organizations such as WHO,
UNICEF, GTZ, IFORD and the UNDP were also contacted for possible
information through their websites. The keywords used in the search
were based on cancer and Cameroon. Several authorities were
consulted through personal communication to complement the review
of the literature. Any documents consulted were both in English and
French, the two official languages of Cameroon.
Government agenda
In its growth and strategy manuscript of 2010, the
government of Cameroon established specific aims constituting a
reference framework for: i) reducing poverty to a socially
acceptable level; ii) reaching middle-income country status; iii)
becoming a newly industrialized country; iv) consolidating the
democratic process and strengthening national unity (23). To attain this general vision, the
specific objectives of the strategy involved: i) increasing growth
to an annual average of 5.5% over the 2010–2020 period; ii)
reducing underemployment from 75.8 to below 50% in 2020, with the
creation of numerous formal jobs over this 10-year period; and iii)
reducing the monetary poverty rate from 39.9% in 2007 to 28.7% in
2020. To achieve these objectives, the government intends to
implement in a coherent and integrated manner: i) a growth
strategy, ii) an employment strategy, and iii) a strategy to
improve governance and the central government’s strategic
management (23).
To attain specific objectives, for example,
objective ii), the government launched a mass recruitment of 25,000
youths from all disciplines into the civil service in 2011. Actions
such as these are paramount in ensuring that chronic diseases such
as cancer, currently faced with expensive health care services,
receive more attention in economic terms.
Cameroon cancer statistics
GLOBOCAN statistics of Cameroon showed that the
age-standardized rate of cancer deaths is 73.1/100,000 persons/year
and the risk of succumbing to any type of cancer prior to the age
of 75 was 11% (7–10,31).
The most common cancer types are breast, uterine cervix, liver,
non-Hodgkin’s lymphoma and prostate cancer. Prostate cancer is the
most common malignancy in men, with an age-standardized incidence
rate of 19.2 and a mortality rate of 15.2/100,000 persons/year. In
women, breast and cervical cancers are the most prevalent tumors,
with breast cancer recording the age-standardized incidence rate of
27.9 and a mortality rate of 16.6/100,000 persons/year. For
cervical cancer, the age-standardized incidence rate is 24 and
mortality 19/100,000 persons/year (1–4,7,8).
Other less frequent female genital cancers in order of decreasing
frequency include ovarian, endometrial and vulva. These cancers,
often diagnosed at advanced stages, result in the belief that
cancer is incurable and therefore lethal. Efforts have been under
way to reverse these statistics in the area of early diagnosis,
treatment and prevention in recent years. Several studies support
the existence of screening programs for cervical, breast and
prostate cancers in Cameroon (32–34).
However, the impact of the activities of these programs on
prevalence, incidence and death rates have yet to be determined.
Therefore, whether these programs have contributed to reducing
cancer-related deaths over time is unclear. As the NCCC registry
does not extend to the national territory, there is no national
population-based cancer registry, although one is available for the
capital city, Yaoundé (35). Due
to the attitudes and beliefs of the population regarding cancer, a
national cancer screening program is organized periodically,
although only in the regions of Yaoundé and Douala. As such, the
rural population, which is most affected, is not included.
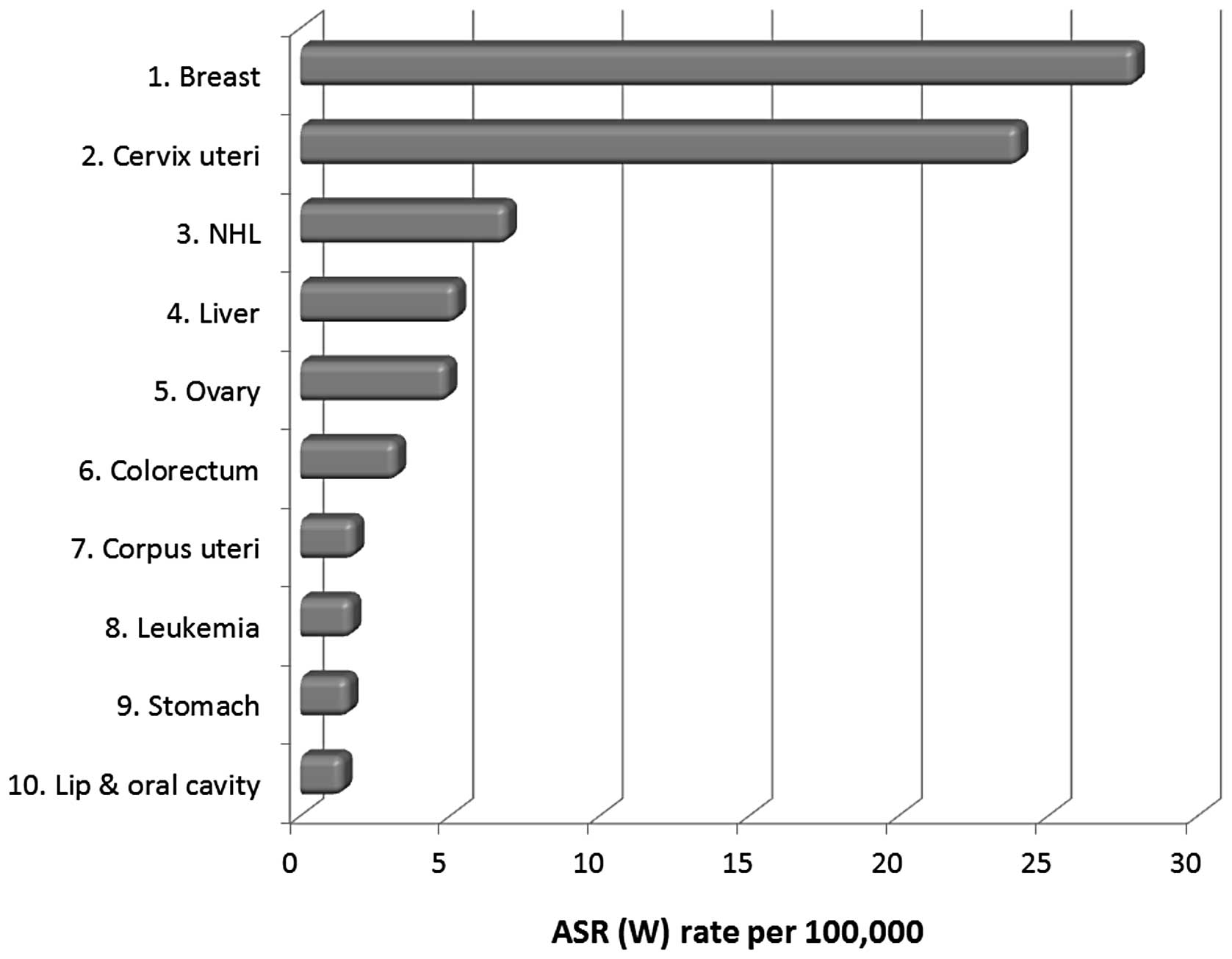
The international agency for research on cancer
(IARC) in 2008, estimated the top 10 population-based
age-standardized incidences of cancers for both men and women in
Cameroon (Figs. 2–5). These data indicate that the rate of
cancer prevalence and related deaths is critical. Prostate cancer
is the most common cancer among men in Cameroon (Fig. 2), followed by liver cancer,
non-Hodgkin’s lymphoma (NHL), Kaposi sarcoma, colorectal cancer,
leukemia, stomach and lung cancer. In women, breast cancer is the
most common type of cancer (Fig.
3), followed by cervical cancer, non-Hodgkin’s lymphoma (NHL),
liver, ovarian, colorectal and uterine cancer, leukemia, and
stomach cancer. The leading cause of cancer-related deaths among
women in Cameroon is cervical cancer (Fig. 4), followed by breast cancer,
non-Hodgkin’s lymphoma (NHL), liver, ovarian and colorectal cancer,
leukemia, and stomach cancer, whereas in men, it is prostate cancer
followed by other cancer types (Fig.
5).
 | Figure 2Ten most common cancers among men in
Cameroon, including prostate cancer, liver cancer, non-Hodgkin’s
lymphoma (NHL), Kaposi sarcoma, colorectal cancer, leukemia,
stomach cancer, lung cancer, other pharynx and lip and oral cavity.
Age-standardized rate (ASR) is the potential rate of a population
if a standard age structure was available. This rate is the number
of new cancer cases/100,000 populations/year (10,14). |
Of note is evidence of male breast cancer in
Cameroon. In a study conducted by Ndom et al (15) a male-to-female breast cancer ratio
of 3.7% was noted. Therefore, male breast cancer should be
considered in the fight against cancer.
Quality of care to cancer patients in
Cameroon
Cancer surveillance in Cameroon is scarce and where
it occurs, it is usually not well-organized, while the records for
cancer-related deaths are inaccurate as the majority of
cancer-related deaths are not reported or recorded due to limited
services available in most areas, with the exception of Yaoundé and
Douala (36,37). Patients usually present at hospital
with an advanced stage of the disease (15,32,35)
due to various factors including ignorance, local beliefs and
poverty, although the reasons for delayed diagnosis and treatment
remain to be elucidated in qualitative and quantitative
investigations. Delay in hospital visitations has also been
compounded by traditional healers, medical and paramedical staff,
who for financial or other reasons, treat cancer patients without
appropriate skills. This is exacerbated by the fact that cancer
treatment centers are centralized in Yaoundé and Douala only,
allowing patients to seek alternative treatement and care. This
situation can be improved by identification and training of
traditional healers whose use of herbs has provided evidence of
tumor regression. The anti-proliferative activities of their
decoctions should be tested and better guided in their practice
(32).
Inadequacy of equipment limits the practice of
cancer case management and treatment in most African countries
(12,38). In Cameroon, oncology is not a
popular medical specialty among young medical officers and nurses,
which aggravates the shortage of care providers to these patients.
Additionally, despite the National Committee’s successful efforts
to secure drugs at a reduced cost, drugs used for chemotherapy are
expensive. Cancer control in national health development programs
has been promoted, however, adequate funding to achieve these goals
is critical.
Government interventions
The government of Cameroon has ratified the WHO’s
Framework Convention on Tobacco Control (FCTC), but it remains
largely non-compliant to any existing FCTC measures (39). A number of tobacco control measures
exist in Cameroon, including some limited smoke-free legislations,
which, however, are frequently not implemented. Drope refers to
this lack of implementation as ‘the politics of smoke-free policy’
(40). Additionally, the national
tobacco control program keeps no data regarding the trends in
tobacco consumption and consumer behaviors in public places, and
the progress of this program is hardly evaluated (41).
Health warnings on cigarette packs, such as
‘cigarette smoking is dangerous to your health’, and advertisements
against smoking are recent events in Cameroon as the national
tobacco control and taxation bill did not include all aspects of
the FCTC. Thus, there is a need for more effective tobacco control
programs, as well as to enforce the legislation that prohibits
smoking in all public places, address the issue of free advertising
by the tobacco industry, increase public awareness of the health
hazards associated with cigarette smoking and other tobacco
products, as well as restrict the access of young persons to
cigarettes (39).
This campaign has faced great setbacks partly due to
cigarette smoking being a lifestyle choice for most uniformed
services in Cameroon, particularly the military and gendarmerie.
Cameroon has only recently attempted to actively implement
smoke-free regulations and directives, such as the banning of
smoking in public buildings by the ministry of Public Health.
Recent studies have reported an informal ban on smoking on public
transportation services (6). In
late 2009, a team of tobacco control advocates, funded by the ATSA
initiative, initiated a program to implement smoke-free policies in
Mfoundi beyond just government buildings to include other public
(e.g., hospitals, educational institutions, healthcare facilities
and tourist establishments) and private environments (e.g.,
workplaces) (42,43). In this ongoing effort, the advocacy
team continues to engage civil society organizations, enforcement
officials and the local authorities as key partners.
At present, no national food policy exists in
Cameroon. A few legislations guiding the registration of food
products in Cameroon are applicable with a mandate on food products
to demarcate the following information: food labeling, nutritional
value of foods, microbial content and additives clearly evident on
packaging (44). However, 32% of
the Cameroonian population is illiterate (3,4) and
a great proportion of the general population is illiterate and not
likely to read the packaging information on these products.
National cancer control
In a telephone interview to an undisclosed source,
Dr Anderson Doh of the Faculty of Medicine and Biomedical Sciences
of Yaoundé addressed key questions pertaining to cancer control in
Cameroon. From his responses, a national committee for the control
of cancer was set up on October 24, 1990 whose activities were
limited and only consisted of periodic screening campaigns (2 or 3
times/year) for cancers of the cervix, breast and prostate.
Occasional screening campaigns were also organized by a few
specialists. These activities were, however, not coordinated.
The NCCC was reorganized by ministerial decision
N°0153/MSP/CAB of 13 January 2002, and charged with six general
objectives and nine specific objectives. Priority objectives
involved the prevention of cancer, diagnosis and treatment of
cancer cases, collection of data, undertaking of research and
mobilization of resources. In 2004, it published a comprehensive
plan including all the main components. This plan cannot be fully
implemented, however, due to lack of funds. After implementing its
2006/2020 strategic plan, the NCCC was revised.
Anti-mitotic drugs are provided at <40% the cost
in private pharmacies with funding from the Ministry of Health,
especially funds from the ‘Heavily Indebted Poor Countries (HIPC)
Initiative’ (25). Individuals
take care of their patients. Since 80% of cancer patients present
at a late stage of the disease, palliative care is a significant
component of the NCCC. On 6th April 2006, the Ministry of Health
signed a partnership agreement with the International Network for
Cancer Treatment and Research (INCTR) with the objective of
initiating a palliative care program. As from 2006, analgesics used
for pain treatment were subsidized by the ministry of health. A
national vaccination for hepatitis B as a preventive measure was
initiated in 2005 to help limit the development of liver cirrhosis
and viral-induced liver cancer in Cameroonians.
The overall objective of the NCCC is to reduce
cancer-related morbidity and mortality in Cameroon and to create a
cancer registry, albeit the data currently available for this
registry are drawn from the district, regional and referral
hospitals only. Information from the rural areas is therefore
lacking, particularly as the effect of the NCCC is evident only in
Yaoundé and Douala at major hospitals.
Notably, in 2004, the government signed a convention
with the pharmaceutical company Sanofi Aventis, which resulted in
the reduction of cost of the company’s most effective cancer drug
(taxotere) to ∼70%. The drug according to company officials had
been previously sold at 480,000 Francs, while following the
convention the cost was set at 170,000 Francs. As part of
activities to mark the national cancer prevention week in Cameroon
a series of surgical operations were carried out by a team of
American and Cameroonian specialists. Specialized cancer treatment
centers are available where early stages of cancer can be diagnosed
and treated. These centers also provide palliative and
psychological care to cancer patients. Considering that some cancer
diagnoses are extremely expensive, the NCCC has developed more
cost-effective but highly efficient procedures to diagnose certain
types of cancer. The NCCC has produced and distributed numerous
detailed documents on cancer and trained a large number of health
personnel on cancer-related issues. Well-equipped mobile diagnosis
and treatment teams proceed from Yaoundé to towns and villages
around the country to carry out awareness campaigns, as well as
screening and treatment of cancer cases on a volunteer basis.
Community interventions
Nationwide campaigns to promote physical activity,
good nutrition, and tobacco control do not exist. Instead, sporadic
activities are often organized around particular events such as the
national cancer week that are usually ceremonial and limited to
health administrative regions such as Yaoundé and Douala. These
health promotion activities used both conventional (mass media,
health facilities and distribution of health education materials)
and non-conventional (meetings in market places, in
churches/mosques and health education activities in schools)
methods to promote good health. The Cameroon Baptist Convention
Health Board runs a cervical prevention and Women’s Health
Programme (WHP) in the private confessional sector. Evaluation
studies on the impact of these interventions on health outcome are
lacking as do cost effectiveness analyses of these interventions.
Therefore, which intervention is most effective remains to be
determined.
Current status of radiotherapy and
chemotherapy services in Africa and Cameroon
Resources for the treatment of Cancer in Cameroon as
with many developing countries are very limited. Among develo ping
countries, the five-year cancer survival is lower in African
nations compared to developing countries in Asia and South America
(45). Poor cancer survival is a
strong indication that additional investment is needed to improve
the quality and accessibility of health services, disease
awareness, and studies into cancer prevention, early detection, and
treatment (45,46). The INCTR reported the global
anticancer drug sales (Fig.
6).
Limitations in resources: Anticancer
drugs
Fig. 6 shows the
percentage of anticancer drug sales (grey bars) and the percentage
of cancer burden (white bars). The USA accounts for 61% of the
anticancer drug sales in the world, but only has 18% of the world’s
cancer burden. By contrast, the group, the ‘rest of the world’,
which largely comprises low- and middle-income countries, indicates
clear global inequity in cancer care (10,14).
These countries account for 61% of the world’s burden of cancer
(47), but only 5% of anticancer
drug sales. In Cameroon, a 20-year descriptive retrospective study
carried out between March, 1989 and March, 2009, based on the
registry and medical records of patients attending the Radiation
Therapy Unit of the Yaoundé General Hospital by Kemfang et
al (36), revealed that 57.55%
of patients received neoadjuvant chemotherapy and 27.32% adjuvant
chemotherapy, a total of 84.87% of patients receiving chemotherapy.
They also observed that the benefit from endocrine therapy was
substantial, in that study, in the absence of hormone receptor
status: tamoxifen was proposed to all patients, with the exception
of lymphoma cases, and was used by 84.11% of patients (36,38).
However, 15.89% of patients were not able to afford tamoxifen.
Aromatase inhibitors or activators (anastrozole, letrozole, and
exemestane) that have demonstrated better efficacy than tamoxifen,
could also not be utilized due to their lack of availability or
high cost (36).
Although the results appear promising, it is crucial
to note that these were data derived from only the radiation unit
of a single hospital of breast cancer patients over 20 years from a
population with annual cases of cancer of >11,700 patients
(1–4).
When compared with developed and middle-income
countries, it is evident that there is a need to intensify search
for anticancer lead compounds from local Cameroonian herbs and the
development of alternative therapy for cancer case management in
Cameroon. Based on the evidence above, the search for hormonal
therapy from natural sources would be a possible relief for the
Cameroonian cancer patient and care giver. For example, whether the
potential use of phytoestrogens derived from the Cameroonian
natural flora offers a cheaper alternative to the current synthetic
and expensive hormonal therapies should be investigated. In
Cameroon, traditional medicine is important in health care, with
80% of people being treated for diseases such as malaria.
Traditional medicine is widespread in rural areas where people do
not always depend on ‘Western’ medicine (48). Thus, it is necessary to determine
which interventions of the Cameroonian traditional medical systems
require strengthening to be of benefit in cancer treatment.
Limitations of resources: Radiotherapy
By 2004, there were ∼2,500 radiotherapy centers and
3,700 machines available for cancer treatment in the developing
world. Additionally, although there was a pressing need for
radiotherapy for ∼3 million patients in the developing world, the
number of centers and machines available in those countries were
sufficient for only 1.85 million patients. By contrast, countries
including Cameroon had only one machine available for over
19,000,000 patients in contrast to one machine for 250,000 patients
in high-income countries (11,46,49).
Over 20 countries, mostly in sub-Saharan Africa had no radiotherapy
machines according to the International Atomic Energy Agency
standards. To compound the problem, many existing machines were not
being used due to a lack of maintenance of the equipment, expired
sources of cobalt, or a lack of radiotherapists or physicists
(26). Little change has been
noted in this situation in the last 8 years for many African
countries.
In a comparison between high-income countries (HIC)
and low- and middle-income countries (LMICs), it was observed that
between 50 and 60% of patients in HIC diagnosed with cancer were
administered radiotherapy at some point during their treatment,
while for patients living in LMICs, radiotherapy remains an
unattainable treatment option, with only 25% of radiotherapy
patients in LMICs having access to the radiotherapy treatment.
There is therefore a need to increase the survival rate (11). While in some HIC, external
radiotherapy only accounts for 5% of the total cost of cancer care,
for many LMICs the infrastructure for and capital costs of
initiating radiotherapy are extremely high, sometimes reaching
>$4 million/U (26,11). When auxiliary costs such as
training and maintenance are added, the total price is vastly
increased (26).
Between 1998 and 2002, Cameroon had only two
mega-voltage machines available for the estimated 14.5 million
people, while 12,949 cases of cancer were reported (26). Between 1989 and 2009, the
radiotherapy unit of Yaoundé General Hospital noted a gradual
increase in the number of patients receiving radiotherapy from 3
patients in 1989 to 73 patients in 2009, suggesting a mean number
of 25 patients/year out of the 531 registered cases (36). In their study, Kemfang et al
(36) reported that 98.80% of
patients were treated with radiotherapy delivered by the cobalt
unit following surgery. This study reveals the great demand for
these services, however, it is beyond the means of the average
Cameroonian due to the high costs involved.
Ethno-search for cancer therapy in
Cameroon
The screening of medicinal plants used as anticancer
drugs has provided modern medicine with effective cytotoxic
pharmaceuticals (50). The US for
example gets most of its anticancer drugs from natural sources such
as herbs (51,29). In the last decades, scientists have
been exploiting the biodiversity of pathways exhibited by the flora
world to unveil lead compounds that are of great value to drug
development and the field of anticancer drug research is likely to
benefit from these advancements in herbal medicines. Voss et
al (52) had earlier reported
the development of anticancer drugs vinblastine and vincristine
from Catharanthus roseus. Hostettman et al (30) were able to show that a large number
of plant extracts from plant families including Guittiferae,
Rubiaceae, Apocynaceae, Euphorbiaceae and Solanaceae demonstrated
great potential for anticancer activities both in vitro and
in vivo(30,53). These plants are located in an
exceptionally rich biodiversity, and few scientific studies have
been carried out in Africa in general and Cameroon in particular,
on the anti-proliferative or pro-apoptotic effects of medicinal
plants. However, some studies based on Cameroonian plants are
presented in the subsequent paragraphs.
In the search for anticancer drugs from herbal
extracts, a few of the studies available from Cameroonian
investigators are cancer-based. For example, in 2011, Kuete et
al (54) found that the
compounds xanthone V1 and 2-acetylfuro-1,4-naphthoquinone of
Cameroon herbal origin showed 65.8 and 59.6%, respectively,
inhibition of the growth of blood capillaries on the
chorioallantoic membrane of quail eggs in an anti-angiogenic assay.
Following treatment with 2-fold IC50 and after 72 h, the
two compounds induced cell cycle arrest in the S phase, and
significant apoptosis in CCRF-CEM leukemia cells. Caspase-3/7 was
activated by xanthone V1. The overall results of that study
provided evidence for the cytotoxicity of compounds xanthone V1 and
2-acetylfuro-1,4-naphthoqui-none, supporting their potential use in
cancer therapy (54,55).
Kuete and Efferth (55) recently screened 5 Cameroonian
medicinal plants widely used in cancer treatment, (Sida acuta,
Sida cordifolia,Sida rhombilifolia, Urena lobata and Viscum
album), for their cytoxicity against Hep G2 hepatocarcinoma
cells. The results showed that these plants exhibited relatively
moderate anti-proliferative effects (56). However, pronounced tumor-reducing
effects were observed when extracts from the roots and leaves of
Bersama engleriana were used on Crown Gall tumor formation
(18). An IC50 of 27.16
μg/ml was reported for Antiaris Africana in DU-145
prostate cancer cells, while even better activity (IC50
of 13.84 μg/ml) was recorded in Hep G2 hepatocarcinoma cells
(19). One of the most active
compounds isolated from Antiaris Africana,
3,39-dimethoxy-49-O-β-d-xylopyronosylellagic acid
exhibited considerable anti-proliferative activities towards Hep G2
(IC50 of 3.84 μg/ml) and DU-145 (IC50
of 6.24 μg/ml) cells (19).
Newbouldia laevis (Bignoniaceae) the main constituent of a
Cameroonian medicinal plant was found to be extremely active
against DU-145 cells with an IC50 of 64.59 nM (57). Wighteone and alpinumisoflavone
isolated from Erythrina indica (Leguminosae) were reported
to be cytotoxic (effective doses of 0.78 and 4.13 μg/ml,
respectively) when tested against KB nasopharyngeal cancer cells
(58). Globulixanthones A and B
isolated for the first time in the Cameroonian medicinal plant,
Symphonia globulifera L. f. (Clusiaceae), showed good
anti-proliferative activities against human KB cells, with
IC50 values of 2.15 and 1.78 μg/ml, respectively
(59). Compound values of 2.0 and
6.6 μg/ml, respectively, for dihydrochelerythrine and
6-acetonyldihydrochelerythrine against L. donovani were
noted (60).
The south-west regional pharmacopoeia developed by
Jiofack et al (61,62) from a full-length ethno-botanical
survey of 289 plant species belonging to 89 families, did not
indicate anticancer components. This is mainly due to the fact that
scientific methods of phytochemical extraction, isolation and
characterization were not employed, nor were the subsequent
scientific models for anticancer activities of the herbs tested.
This would be a misrepresentation of the medicinal potential of
Cameroonian herbs from the South-West and littoral regions
ecological zone. Studies of this nature would present more useful
data if scientific proof of the claims of the therapeutic
indications of the herbalist were tested and standardized. However,
despite the skills offered, lack of resources would not allow the
Cameroonian ethno-scientist to explore his potential nor that of
the rich ecological flora.
A similar study was conducted in the Lebialem
division by Focho et al (63), however, results pertaining to the
use of anticancer herbs in that region were not recorded. Reasons
for the lack of research data involve, not only policy problems,
but also the research methodology for evaluating traditional
medicine likely due to lack of equipment and funds. Literature and
data on the studies of traditional medicine in various
ethno-research laboratories in Cameroon are available. However,
their validity remains to be confirmed as most literature is based
on the findings of traditional practitioners and are not
scientifically viable (64). Thus,
there is a need for validation and standardization of
phytomedicines and traditional medical practices in order that this
sector be incorporated within the health care system of Cameroon
(65). As the characteristics and
applications of traditional medicine differ from those of western
medicine, the manner in which traditional medicine is evaluated as
well as the type of academic research approaches and methods that
may be used to evaluate the safety and efficacy of traditional
medicine are new challenges that have emerged in recent years
(65,67). Together with an increased interest
in medicine is an increased interest in the safety aspects of the
practice of herbal medicine (64,65,67).
The private sector, which is involved in the business of herbal
drugs, should take responsibility and ensure the safety and
efficacy of these herbal drugs. Stringent government policies
regulating the promotion of herbal medicines and products in
Cameroon via advertising should be implemented, while traditional
practitioners should act in a responsible manner (64).
Clinical cancer study efforts
In a descriptive retrospective study based on the
registry and medical records of patients in the Gynecology and
Obstetrics unit, Yaoundé General Hospital, Kemfang et al
(36) reinforced the position
occupied by late presentation and advanced stage of diagnosis of
breast cancer profile in developing countries. During the study
period, 531 breast cancer patients were recorded of which 0.75%
were male. A total of 66.1% of the patients were <50 years old
and 31.9% <40. Additioanlly, 95.34% of patients detected their
cancers themselves and delayed seeking treatment at hospital for
∼1,035 months. Up to 54.94% of patients had used traditional
medicine prior to medical evaluation. In another study, Ndom et
al (15) looked into male
breast cancer showing a male-to-female breast cancer ratio of 3.7%.
They likewise confirmed the fact that the majority of patients (17
patients, 80%) had advanced stage at diagnosis before consulting a
doctor (15).
An important knowledge gap was identified by McCarey
et al (68) among health
workers in Cameroon. Cervical cancer and prevention by screening
showed several gaps and important misconceptions regarding
screening methods. Most participants were aware that cervical
cancer is a major public health concern (86%), were able to
identify the most important etiological factors (58%) and believed
that screening may prevent cervical cancer (90%) and may be
performed by Pap test (84%). However, less than half were
considered for VIA or HPV screening tests (38 and 47%,
respectively). Thus, knowledge pertaining to cancer etiology and
screening was lowest among nurses/midwives (68). However, more data are required for
this finding. It would therefore be profitable if an emphasis on
cancer (cervical, breast and uterine) is placed on nurse training
programs as part of reproductive health. Angwafo et al
(69) have also reported the
results of prostatic biopsies from an ongoing national prostate
cancer survey in Cameroon. A total of 111 men in Dibombari, aged
≥40 years, were recruited for a medical interview, PSA assay and
digital rectal examination (DRE). Biopsies were performed on 24
subjects who had either suspicious prostates on DRE and/or PSA ≥4
ng/ml. Six men (5.4%) were shown to have cancer, another 6 had
low-grade prostatic intraepithelial neoplasia (PIN), and another 2
(1.8%) had high-grade PIN. Sow et al (70) reported on urogenital malignancies
in the Yaoundé Central Hospital between 1987 and 2005, identifying
a total of 520 cases of prostate cancer out of 2,371 benign and
malignant tumors (including over 1,000 cases of BPH). Those results
indicate that prostate cancer is the most dominant malignant
urogenital tumor observed in Cameroonian males.
Knowledge gaps
Gaps in knowledge of how traditional knowledge
systems of health function in Cameroon, as well as their
limitations and prospects following the WHO traditional medicines
strategies remain (70).
Successful experiences and approaches on conservation and
sustainable use of medicinal plants are rare. With regard to
research aspects pertaining to medicinal plants, traditional
medicine and local communities, a number of questions remain to be
addressed, including which traditional decoctions are effective and
by what mechanism; which of the decoctions have been tested in its
natural composition and how; how traditional medicinal knowledge,
practices and preparations should be validated at the community
levels where its use is optimal, as well as by what scientific
methods and facilities; the standardization of Cameroonian
traditional medicines at local and traditional healer levels in the
community, and what methods and facilities should be utilized;
determining the best functional conditions for indigenous medical
practices; identifying the traditional medicine care receivers in
Cameroon and the conditions under which they seek alternative
treatments; the extent of acceptance of traditional medicines by
the population in general; and the point of integration between
western and traditional medicines in Cameroon.
Identification, classification and documentation of
all major medicinal plants is also a concern as well as how to
identify what has been lost from untransferred knowledge,
particularly at the periphery. Additional concerns that should be
addressed include whether traditional knowledge systems relating to
sustainable use and conservation of medicinal plants are clearly
understood; whether gender issues have been adequately considered;
whether traditional methods can be incorporated into research
strategies; how local and traditional knowledge may contribute to
the propagation and sustainable use and conservation of medicinal
plants; the limitations and potentials of spiritual beliefs
relating to traditional healing systems; the cultural practices and
beliefs that are supportive of the conservation and sustainable
utilization of medicinal plants; as well as the benefits derived. A
coherent research agenda for the Cameroon ethno-scientist should
focus on: i) safety and efficacy of traditional remedies; ii)
designation of appropriate research procedures and standardization
of herbal medicines that are illegally inundating the market; iii)
provide reasons for the utilization of traditional medicines
extrapolating results to the area of medical, social, demographics
and economics sciences; iv) defining the consumers of traditional
medicines and stating conditions under which traditional medicines
are most appropriate; v) conducting ethno-botanical surveys such as
those of Jiofack et al (61,62)
and the Red Data Book regarding the status of Cameroonian medicinal
plants; vi) initiation of studies of indigenous conservation with a
focus on the rapid disappearance of the natural flora used as
medicinal plants; vii) effective agro-ecological methods that
enhance the propagation and cultivation of specific medicinal
plants with a particular focus on the encroaching
desertification.
Conclusion
Cancer in particular and research in general is
given very little attention in Cameroon. Attention is usually paid
to infectious- and poverty-related diseases either due to their
volatile and extremely sensitive nature or due to the lack of
funding. Consequently, victims of cancer and other chronic diseases
generate their own interventions to cope with their conditions, a
‘coping mechanism’. In most developing countries cancer has not
been a priority for health ministries as nutritional, parasitic and
infectious diseases have presented a greater and more immediate
challenge. The level of interest in and development of cancer
statistics may reflect the low priority that has been given to
malignant disease in the past. There is the need in Cameroon for
the continuous promotion of health research in cancer management
and development of new chemical entities from the plethora of
natural medicinal flora. Thus, cancer study awareness could be
elevated to priority status (72,73).
Acknowledgements
This study was supported by funding
from the Doctoral Fund of Ministry of Education of China (RFDP,
20111210110007) and the Chinese Scholarship for International
Students. The authors would like to thank Dr Joseph Forbi and Dr
Teresia M.F.R Dias for reading the manuscript and Professor W.F.
Mbacham for all the comments and support.
References
|
1.
|
World Health Organization (WHO): Cancer
prevention and control; report to the secretariat by the 58th World
Health Assembly. http://www.who.int/mediacentre/news/releases/2005/pr_wha05/en/index.html.
Accessed January 23, 2012.
|
|
2.
|
WHO: The global burden of disease: 2004
update. Geneva: pp. 1–150. 2008
|
|
3.
|
WHO world health statistics 2009:
Cause-specific mortality and morbidity. http://www.who.int/whosis/whostat/EN_WHS09_Table2.pdf.
Accessed January 23, 2012.
|
|
4.
|
WHO world health statistics: Cameroon
factsheets of health statistics 2010 and Non Communicable Disease
Country Profiles, 2011. http://www.afro.who.int/.
Accessed January 23, 2012.
|
|
5.
|
Bray F, Ren JS, Masuyer E and Ferlay J:
Global estimates of cancer prevalence for 27 sites in the adult
population in 2008. Int J Cancer. July 3–2012.(Epub ahead of
print).
|
|
6.
|
Njoumemi Z, Sibetcheu D, Ekoe T and Gbedji
E: Tobacco in Cameroon from farming to control in Africa tobacco
situational analysis. https://www.atsa.org. Accessed January
18, 2012.
|
|
7.
|
Jemal A, Bray F, Forman D, O’Brien M,
Ferlay J, Center M and Parkin DM: Cancer burden in Africa and
opportunities for prevention. Cancer. 118:4372–4384. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Jemal A, Bray F, Ferlay J, Ward E and
Forman D: Global cancer statistics. CA Cancer J Clin. 61:69–90.
2011. View Article : Google Scholar
|
|
9.
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers CD and Parkin DM: GLOBOCAN 2008: Cancer Incidence,
Mortality and Prevalence Worldwide in 2008. http://globocan.iarc.fr.
Accessed June 17, 2012.
|
|
11.
|
Parkin DM: The global health burden of
infection-associated cancers in the year 2002. Int J Cancer.
118:3030–3044. 2006.PubMed/NCBI
|
|
12.
|
Parkin DM, Sitas F, Phil D, Chirenje M,
Stein L, Abratt R and Wabinga H: Part I: Cancer in indigenous
Africans - burden, distribution, and trends. Lancet Oncol.
9:683–692. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Frenk J, Bobadilla J, Sepùlveda J and
Cervantes ML: Health transition in middle-income countries: new
challenges for health care. Health Policy Plan. 4:29–39. 1989.
View Article : Google Scholar
|
|
14.
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers CD and Parkin D: GLOBOCAN 2008: Cancer Incidence and
Mortality Worldwide. IARC CancerBase No. 10. Lyon, France: IARC;
2010, http://globocan.iarc.fr.
2010. Accessed June 17, 2012.
|
|
15.
|
Ndom P, Germaine U, Bell EMD, Eloundou A,
Hossain N and Huo D: Characterization of male breast cancer in
Yaoundé, Cameroon and a meta-analysis of literature in Africa.
1–15. 2007.
|
|
16.
|
Hippolyte KW, Kowa TK, Lonfouo AN, Tchinda
AT, Tane P, Kikuchi H, Frédérich M and Oshima Y: Phenolic compounds
and terpenoids from hypericum lanceolatum. Rec Nat Prod. 6:94–100.
2012.
|
|
17.
|
Lenta BN, Tantangmo F, Devkota KP, Wansi
JD, Chouna JR, Soh RC, Neumann B, Stammler HG, Tsamo E and Sewald
N: Bioactive constituents of the stem bark of beilschmiedia
zenkeri. J Nat Prod. 72:2130–2134. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Kuete V, Mbaveng AT, Tsaffack M, Beng VP,
Etoa FX, Nkengfack AE, Meyer MJJ and Lall N: Antitumor, antioxidant
and antimicrobial activities of Bersama
engleriana(melianthaceae). J Ethnopharmacol. 115:494–501. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Kuete V, Vouffo B, Mbaveng AT, Vouffo EY,
Siagat RM and Dongo E: Evaluation of Antiaris africana
methanol extract and compounds for antioxidant and antitumor
activities. Pharm Biol. 47:1042–1049. 2009.
|
|
20.
|
Enow-Orock GE, Ndom P, Essame-Oyono JL and
Doh AS: Cancer incidence in Yaounde 2004–2008: Yaoundé cancer
registry technical report. Yaoundé: National Cancer Control
Program, Cameroon; pp. 26–27. 2009
|
|
21.
|
United state development service (USDS):
2010, http://www.hhs.gov/secretary/about/priorities/strategicplan2010-2015.pdf
and http://www.cdc.gov/nchs/data/hus/hus10.pdf.
Accessed September 5, 2012.
|
|
22.
|
UK border and immigration service’s 2008:
Country of origin information report. http://supportkurds.org/reports/new-home-officeuk-borders-agency-country-of-origin-information-report.
Accessed August 26, 2012.
|
|
23.
|
African development bank country strategy
papers 2010–2014: Cameroon regional departments center: 2–8,
2009.
|
|
24.
|
World development indicators.
International Bank for Reconstruction and Development/The World
Bank; Washington, DC: 2009
|
|
25.
|
Cameroon - ministry of economy and
finance. Memorandum No. 07/788, 2010.
|
|
26.
|
Barton MB, Frommer M and Shafiq J: Role of
radiotherapy in cancer control in low-income and middle-income
countries. Lancet Oncol. 7:586–595. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Fezeu L, Fointama E, Ngufor G, Mbeh G and
Mbanya JC: Diabetes awareness in general population in Cameroon.
Diabetes Res Clin Pract. 90:312–318. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28.
|
Mbeh GN, Edwards R, Ngufor G, Assah F,
Fezeu L and Mbanya JC: Traditional healers and diabetes: results
from a pilot project to train traditional healers to provide health
education and appropriate health care practices for diabetes
patients in Cameroon. Glob Health Promot. 17(Suppl 2): 17–26. 2010.
View Article : Google Scholar
|
|
29.
|
Newman DJ and Cragg GM: Natural products
as sources of new drugs over the last 25 years. J Nat Prod.
70:461–477. 2007.PubMed/NCBI
|
|
30.
|
Hostettmann K, Marston A, Ndjoko K and
Wolfender JL: The potential of African plants as source of drugs.
Curr Org Chem. 4:973–1010. 2000.
|
|
31.
|
Mbakop A, Oyono EJL, Ngbangako MC and
Abondo A: Current epidemiology of cancers in cameroon (Central
Africa). Bull Cancer. 79:1101–1104. 1992.(In French).
|
|
32.
|
Doh AS, Nkele NN, Achu P, Essimbi F,
Essame O and Nkegoum B: Visual inspection with acetic acid and
cytology as screening methods for cervical lesions in Cameroon. Int
J Gynaecol Obstet. 89:167–173. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33.
|
Suba EJ and Raab SS: Population-based Pap
screening in Cameroon. Acta Cytol. 47:948–949. 2003.PubMed/NCBI
|
|
34.
|
Robyr R, Nazeer S, Vassilakos P, Matute
JC, Sando Z, Halle G, Mbakop A and Campana A: Feasibility of
cytology-based cervical cancer screening in rural Cameroon. Acta
Cytol. 46:1110–1116. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
35.
|
Enow-Orock G, Mbu R, Ngowe NM, Tabung FK,
Mboudou E, Ndom P, Nkele N, Takang W, Essame-Oyono JL and Doh A:
Gynecological cancer profile in the Yaounde population, Cameroon.
Clin Mother Child Health. 3:437–444. 2006.
|
|
36.
|
Kemfang JDN, Yomi J, Kasia JM, Mawamba Y,
Ekortarh AC and Vlastos G: Breast cancer profile in a group of
patients followed up at the Radiation Therapy Unit of the Yaounde
General Hospital, cameroon. Int J Gynaecol Obstet.
2011:1435062011.PubMed/NCBI
|
|
37.
|
Tebeu PM, Petignat P and Mhawech-Fauceglia
P: Gynecological malignancies in Maroua, Cameroon. Int J Gynaecol
Obstet. 104:148–149. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38.
|
Eniu A, Carlson RW, Aziz Z, Bines J,
Hortobágyi GN, Bese NS, Love RR, Vikram B, Kurkure A and Anderson
BO: Breast cancer in limited resource countries; treatment and
allocation of resources. Breast J. 12(Suppl 1): S38–S53.
2006.PubMed/NCBI
|
|
39.
|
Simpson D: Cameroon-disappearing ads mark
good start. Tob Control. 16:295–296. 2007.
|
|
40.
|
Drope J: The politics of smoke-free
policies in developing countries: Lessons from Africa. CVD Prev
Control. 5:65–73. 2010. View Article : Google Scholar
|
|
41.
|
Ezzati M, Henley SJ, Lopez AD and Thun MJ:
Role of smoking in global and regional cancer epidemiology- current
patterns and data needs. Int J Cancer. 116:963–971. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
42.
|
Mfoundi department, Cameroon: Memorandum
No. 1913. 2007
|
|
43.
|
Africa tobacco situational analyses (ATSA)
project 105799. https://www.idrc.ca/en/ev-155993-201_105799-1-IDRC_ADM_INFO.html.
Accessed July 11, 2012.
|
|
44.
|
Law framework on consumer protection in
cameroon. http://www.legicam.org/index.php.
Accessed July 11, 2012.
|
|
45.
|
Sankaranarayanan R, Swaminathan R, Brenner
H, et al: Cancer survival in Africa, Asia, and Central America: a
population-based study. Lancet Oncol. 11:165–173. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
46.
|
Levin V and Tatsuzaki H: Radiotherapy
services in countries in transition-gross national income per
capita as a significant factor. Radiother Oncol. 63:147–150. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
47.
|
John R and Ross H: The global economic
cost of cancer, American cancer society, september, 2010.
http://www.cancer.org/AboutUs/GlobalHealth/global-economic-cost-of-cancer-report.
Accessed July 23, 2012.
|
|
48.
|
Djoyum B: journal Le jour. Cameroun.
12:2007.
|
|
49.
|
Ahmad K: Millions in developing world
deprived of radiotherapy. Lancet Oncol. 4:4562003. View Article : Google Scholar : PubMed/NCBI
|
|
50.
|
Boik J: Natural Compounds in Cancer
Therapy. Oregon Medical Press; Princeton, MN, USA: 2001
|
|
51.
|
Stévigny C, Bailly C and Quetin-Leclercq
J: Cytotoxic and antitumor potentialities of aporphinoid alkaloids.
Curr Med Chem Anticancer Agents. 5:173–182. 2005.PubMed/NCBI
|
|
52.
|
Voss C, Eyol E and Berger MR:
Identification of potent anti-cancer activity in Ximenia
americana aqueous extracts used by African traditional
medicine. Toxicol Appl Pharmacol. 211:177–187. 2006.
|
|
53.
|
Whelan LC and Ryan MF: Ethanolic extracts
of Euphorbia and other ethnobotanical species as inhibitors
of human tumour cell growth. Phytomedicine. 10:53–58. 2003.
|
|
54.
|
Kuete V, Wabo HK, Eyong KO, Feussi MT,
Wiench B, Krusche BB, Tane P, Folefoc GN and Efferth T: Anticancer
activities of six selected natural compounds of some Cameroonian
medicinal plants. PLoS ONE. 6:e217622011. View Article : Google Scholar : PubMed/NCBI
|
|
55.
|
Kuete V and Efferth T: Cameroonian
medicinal plants: pharmacology and derived natural products. Front
Pharmacol. 1:1232010. View Article : Google Scholar : PubMed/NCBI
|
|
56.
|
Pieme CA, Penlap VN, Ngogang J and
Costache M: In vitro cytotoxicity and antioxidant activities of
five medicinal plants of Malvaceae family from Cameroon. Environ
Toxicol Pharmacol. 29:223–228. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
57.
|
Eyong KO, Kumar PS, Kuete V, Folefoc GN,
Nkengfack AE and Baskaran S: Semisynthesis and antitumoral activity
of 2-acetylfuranonaphthoquinone and other naphthoquinone
derivatives from lapachol. Bioorg Med Chem Lett. 18:5387–5390.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
58.
|
Nkengfack A, Azebaze AG, Waffo AK, Fomum
ZT, Meyer M and Heerden VF: Cytotoxic isoflavones from Erythrina
indica. Phytochemistry. 58:1113–1120. 2001. View Article : Google Scholar
|
|
59.
|
Nkengfack AE, Mkounga P, Fomum ZT, Meyer M
and Bodo B: Globulixanthones A and B, two new cytotoxic xanthones
with isoprenoid groups from the root bark of Symphonia
globulifera. J Nat Prod. 65:734–736. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
60.
|
Fotie J, Bohle DS, Olivier M, Gomez MA and
Nzimiro S: Trypanocidal and antileishmanial dihydrochelerythrine
derivatives from Garcinia lucida. J Nat Prod. 70:1650–1653.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
61.
|
Jiofack T, Fokunang C, Kemeuze V,
Fongnzossie E, Tsabang N, Nkuinkeu R, Mapongmetsem PM and
Nkongmeneck BA: Ethnobotany and phytopharmacopoea of the South-West
ethnoecological region of Cameroon. J Med Plants Res. 2:197–206.
2008.
|
|
62.
|
Jiofack T, Fokunang C, Guedje N, Kemeuze
V, Fongnzossie E, Nkongmeneck BA, Mapongmetsem PM and Tsabang N:
Ethnobotanical uses of medicinal plants of two ethnoecological
regions of cameroon. Int J Med Med Sci. 2:60–79. 2010.
|
|
63.
|
Focho DA, Ndam WT and Fonge BA: Medicinal
plants of Aguambu-Bamumbu in the Lebialem highlands, southwest
province of Cameroon. Afr J Pharm Pharacol. 3:1–13. 2009.
|
|
64.
|
Bodeker G: Traditional health knowledge
and public policy. Nature and Resource. 30:5–16. 1994.
|
|
65.
|
UNESCO: Traditional knowledge in tropical
environment. Nature and Resource. 30:1994.
|
|
66.
|
Posey DA and Dutfield G: Beyond
Intellectual Property -Towards Traditional Resource Rights for
Indigenous Peoples and Local Communities. Ottawa, Canada:
International Development Research Center; 1996
|
|
67.
|
Wambebe C: Development and production of
standardised phytomedicines. National Institute for Pharmaceutical;
Abuja, Nigeria: 1998
|
|
68.
|
McCarey C, Pirek D, Tebeu PM, Boulvain M,
Doh AS and Petignat P: Awareness of HPV and cervical cancer
prevention among Cameroonian healthcare workers. BCM Womens Health.
11:452011. View Article : Google Scholar : PubMed/NCBI
|
|
69.
|
Angwafo FF III, Zaher A, Befidi-Mengue R,
Wonkam A, Takougang I, Powell I and Murphy G: High-grade
intra-epithelial neoplasia and prostate cancer in dibombari,
Cameroon. Prostate Cancer Prostatic Dis. 6:34–38. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
70.
|
Sow M, Nkégoum B, Oyono JL, Garoua and
Nzokou A: Epidemiological and histological features of urogenital
tumours in Cameroon. Prog Urol. 16:36–39. 2006.(In French).
|
|
71.
|
WHO technical report series 863. Annex 11
guidelines for the assessment of herbal medicines. pp. 178–183.
1996
|
|
72.
|
The international network for cancer
treatment and research (INCTR): http://www.inctr.org/.
Accessed June 23, 2012.
|
|
73.
|
International agency for research on
cancer (IARC) world health organization: Globocam 2008 section of
cancer information. https://www.iarc.fr. Accessed May 10,
2012.
|