Introduction
Lung transplantation (LT) is the mainstay of
therapeutic modalities for end-stage lung diseases, however, the
1-year survival rate following lung transplantation is only 80%,
with primary graft dysfunction (PGD) contributing to 30% of
mortalities (1).
Ischemia-reperfusion injury (I/R) has been reported to be one of
the main causes of PGD, therefore significant efforts have been
made to optimize the methods for lung preservation in order to
decrease the risk of lung injury during the period of ischemia
(2,3). Several studies have suggested that
prolonged durations of lung cold ischemia (CI), in combination with
other donor characteristics, has a negative effect on the outcome
following LT (1,4).
Autophagy is a cellular process in which
autophagosomes deliver cytoplasmic proteins and macromolecules to
lysosomes for degradation (5,6), and
has been implicated in a number of diseases (7,8).
Autophagy can lead to non-apoptotic programmed cell death, which is
termed autophagic cell death (9,10).
Increased autophagic activity and autophagic cell death have been
identified in the damaged tissues of various disease models
(11–14). A previous study demonstrated that
autophagy is also involved in warm I/R injury in the lung (15).
Autophagy is often rapidly upregulated during
starvation or cell stress (5,6).
Since CI preservation for LT magnifies cell stress and nutrient
deprivation, measuring the autophagic activity during CI would
yield significant results. In addition to apoptosis, autophagic
cell death has been hypothesized to be another important potential
mechanism of neural tissue damage, induced by ischemia (13,14).
However, whether autophagy is induced during CI of lung
preservation and whether autophagic cell death contributes to lung
tissue damage following CI remains to be elucidated. The present
study verified that autophagy is involved in CI of lung
preservation and autophagic cell death was observed in rat donor
lungs following prolonged CI.
Materials and methods
Ethics
Ethical approval for the present study was provided
by the Ethical Committee (no. KS1218) of the Shanghai Chest
Hospital, affiliated to Shanghai Jiaotong University (Shanghai,
China), on 10 July 2011.
CI preservation
The present study was performed in accordance with
the Guidelines for Animal Experiments of the Shanghai Jiaotong
University (Shanghai, China). Male Sprague-Dawley rats weighing
250–300 g were housed with free access to food and water under a
natural day/night cycle. All rats were acclimated for a week prior
to any experimental procedures. The rats were anesthetized by an
intraperitoneal injection of ketamine chloride (100 mg/kg; Jiangsu
Hengrui Medicine Co., Ltd., Lianyungang, China) and intubated
through a tracheotomy. Rats were mechanically ventilated with 100%
oxygen, at a tidal volume of 10 ml/kg and a respiratory rate of 70
breaths/min. Following heparinization (1000 U/kg intravenously), a
median sternotomy was performed. The pulmonary artery (PA) was
cannulated through a right ventriculotomy and the left atrium was
sheared directly. The lungs were flushed through the PA cannula
with 20 ml of cold low-potassium dextran solution (Perfadex,
Vitrolife, Gothenburg, Sweden) via gravity drainage of 25 cm
H2O. The PA, vein and trachea were ligated and
subsequently the heart-lung bloc was excised from the chest.
Following the excision, the inflated lung was placed into
low-potassium dextran solution and stored at 4°C for CI
preservation. A total of 30 rats were randomly divided into five
treatment groups and underwent en bloc heart-lung harvest as
described previously (16). These blocs were
subsequently followed by CI preservation for varying time periods
(0, 3, 6, 12 and 24 h, respectively). Following CI preservation,
the left lung tissues of each bloc were fixed in 4%
paraformaldehyde (Guangfu Fine Chemical Research Institute,
Tianjin, China) in 0.01 M phosphate-buffered saline (PBS; Basic
Medicine Faculty of Shanghai Jiaotong University, Shanghai, China)
pH 7.4 at 4°C for 24 h. Subsequently, the samples were
cryoprotected overnight in 30% sucrose in 0.01 M PBS at 4°C and
embedded in optimal cutting temperature (OCT) media prior to
immunofluorescence staining. The right lung tissues were frozen in
liquid nitrogen and stored at −80°C prior to western blot analysis
and reverse transcription quantitative polymerase chain reaction
(RT-qPCR) analysis.
Double immunofluorescence staining
Immunofluorescence staining was performed using
transverse sections to investigate alterations in the expression of
a specific autophagy marker, microtubule-associated protein 1 light
chain 3B (LC3B), at each time point following CI. To identify DNA
fragmentation (a marker of apoptosis) in the cells expressing LC3B,
double staining of LC3B and the terminal deoxynucleotidyl
transferase-mediated dUTP nick end labeling (TUNEL) were performed.
Tissue sections (10 μm thickness) were prepared from OCT
media-embedded tissue using a cryostat. The sections were washed in
0.01 M PBS and permeabilized in 0.2% Triton X-100 (Sigma-Aldrich,
St. Louis, MO, USA). For immunofluorescent labeling, sections were
pre-incubated in 20% goat serum (Beyotime Institute of
Biotechnology, Nantong, China) for 30 min and subsequently
incubated overnight at 4°C with the primary antibody, (LC3B, D11,
XP® rabbit monoclonal antibody used at 1:200; #3868s;
Cell Signaling Technology, Inc., Danvers, MA, USA) in 0.01 M PBS.
Following three washes in PBS, the sections were incubated for 2 h
with Alexa Fluor 488-conjugated anti-rabbit immunoglobulin G
antibody (1:500; A11008; Invitrogen Life Technologies, Carlsbad,
CA, USA) in 0.01 M PBS at room temperature in the dark. TUNEL
staining was applied using an in situ Cell Death Detection
kit, TMR red (Roche Diagnostics GmbH, Mannheim, Germany), according
to the manufacturer’s instructions. 4′,6-Diamidino-2-phenylindole
(Beyotime Institute of Biotechnology) was employed for nuclear
staining. Following rinsing in PBS, the sections were mounted with
antifade solution (Beyotime Institute of Biotechnology). The
immunoreactive signals were sequentially visualized in the same
section using an LSM 710 Meta confocal microscope (Zeiss, Jena,
Germany) with three distinct filters (405, 488 and 543 nm). The
signal intensities through each filter were matched at the time of
imaging. The images through each filter were individually optimized
for brightness and background prior to generating the final
composite images.
LC3B-positive cell counting
The LC3B-positive cells, which were defined as the
cells exhibiting punctuate LC3B fluorescent dots (14,17),
were counted in the transverse sections scanned previously. A total
of six serial sections were used for each sample. The LC3B-positive
cells were counted in five random microscopic fields
(magnification, ×40) of each section by an examiner who was blinded
to the experimental conditions.
Western blot analysis
Rat lung tissues were homogenized in cold T-PER™
lysis buffer (Pierce Biotechnology, Inc., Rockford, IL, USA) with a
protease inhibitor cocktail (Roche Diagnostics GmbH). Subsequently,
the lysates were quickly sonicated three times for 15 sec in an ice
bath, boiled for 5 min at 95°C and stored at −80°C prior to use.
Aliquots of proteins were separated by 10% sodium dodecyl sulfate
polyacrylamide gel, transferred onto a polyvinylidene difluoride
membrane and detected using antibodies against LC3B(D11)
XP® rabbit monoclonal antibody (1:1,000; #3868s; Cell
Signaling Technology, Inc.), Beclin-1 (H-300) rabbit polyclonal
antibody (1:1,000; sc-11427; Santa Cruz Biotechnology, Inc., Santa
Cruz, CA, USA) or caspase-3 rabbit polyclonal antibody (1:1,000;
#9662s; Cell Signaling Technology, Inc.), respectively. β-actin
(1:5,000; Sigma Aldrich, Shanghai, China) was used as a loading
control.
RT-qPCR analysis
RT-qPCR was performed to assess autophagy-related
gene 5 (Atg5), B-cell lymphoma 2 (Bcl-2) and Bcl-2-associated X
protein (Bax) gene expression in lung samples. Total RNA was
isolated using TRIzol (Invitrogen Life Technologies) according to
the manufacturer’s instructions. Reverse transcription was
completed using a PrimeScript 1st Strand cDNA Synthesis kit (Takara
Biotechnology Co., Dalian, China) according to the manufacturer’s
instructions. SYBR® Green qPCR was performed using an
Applied Biosystems 7500 real-time PCR System (Applied Biosystems,
Foster City, CA, USA) in a 20 μl reaction containing 2 μl of cDNA,
10 μl of 2X SYBR® Premix Ex Taq™ (DRR041A, Takara
Biotechnology Co.) and primers designed specifically for the genes
amplified (18). The primer
sequences are shown in Table I
(Sangon Biotech, Shanghai, China).
 | Table IPolymerase chain reaction
primers. |
Table I
Polymerase chain reaction
primers.
| Genes | Forward 5′-3′ | Reverse 5′-3′ |
|---|
| Atg5 |
AGTGGAGGCAACAGAACC |
GACACGAACTGGCACATT |
| Bcl-2 |
GGATGACTTCTCTCGTCGCTAC |
TGCAGATGCCGGTTCAG |
| Bax |
GCAGGGAGGATGGCTGGGGAGA |
TCCAGACAAGCAGCCGCTCACG |
| β-actin |
GTCAGGTCATCACTATCGGCAAT |
AGAGGTCTTTACGGATGTCAACGT |
Statistical analysis
Data are expressed as the mean ± standard deviation.
The statistical significance was estimated by one-way analysis of
variance followed by the Student-Newman-Keuls test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Autophagy is induced following CI
To assess autophagic activity in lung tissues
following CI, the protein expression of LC3B-I and LC3B-II
(autophagosome marker proteins) was examined using western blot
analysis. A significant increase in the ratio of LC3B-II/I was
observed after 3 h of CI, peaked at 6 h and subsequently decreased
to the basal level after 12 h (Fig. 1A
and B). This result suggested that autophagic activity was
induced in lung tissues following CI. Consistently, changes in the
level of the protein Beclin-1, another key autophagic protein,
exhibited a similar trend (Fig. 1C and
D).
Immunofluorescence staining of
LC3B-positive cells
In order to confirm these findings, the
LC3B-positive cells were detected by immunofluorescence staining. A
marked increase in the number of LC3B puncta was observed in lung
tissue within the prolonged CI time, which is consistent with the
trend observed in western blot analysis. The marked increase in
LC3B-positive cells was initiated at 3 h, peaked at 6 h following
CI and thereafter decreased to the basal level after 12 h of CI
preservation (Fig. 2). In order to
further confirm autophagy induction in lung tissues following CI,
the mRNA level of another important autophagy marker, Atg5,
was assessed via qPCR analysis. In a similar manner to that of LC3B
induction, a significant increase in Atg5 expression was
detected in the 6 h group compared with the 0 h group following CI
(Fig. 3).
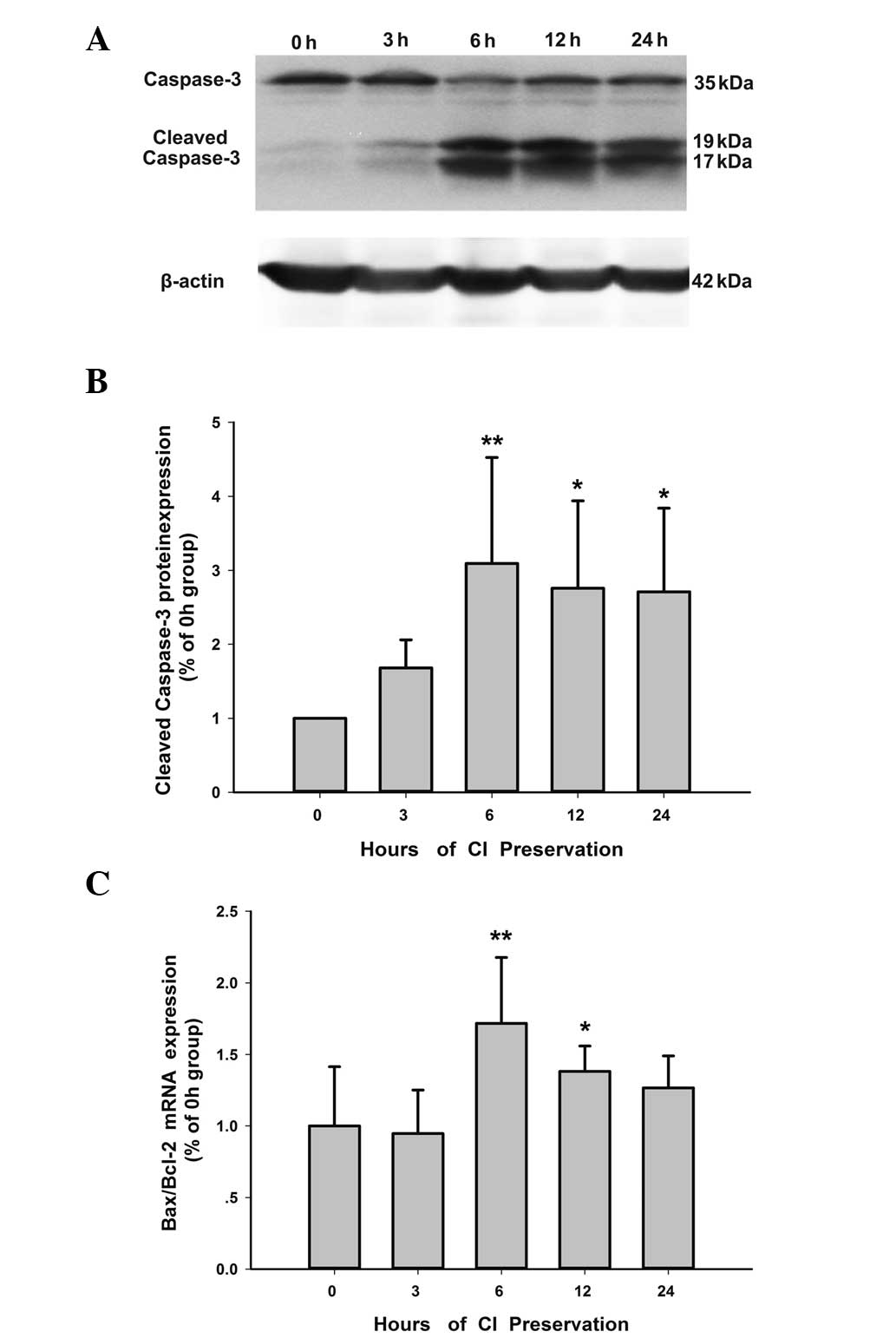
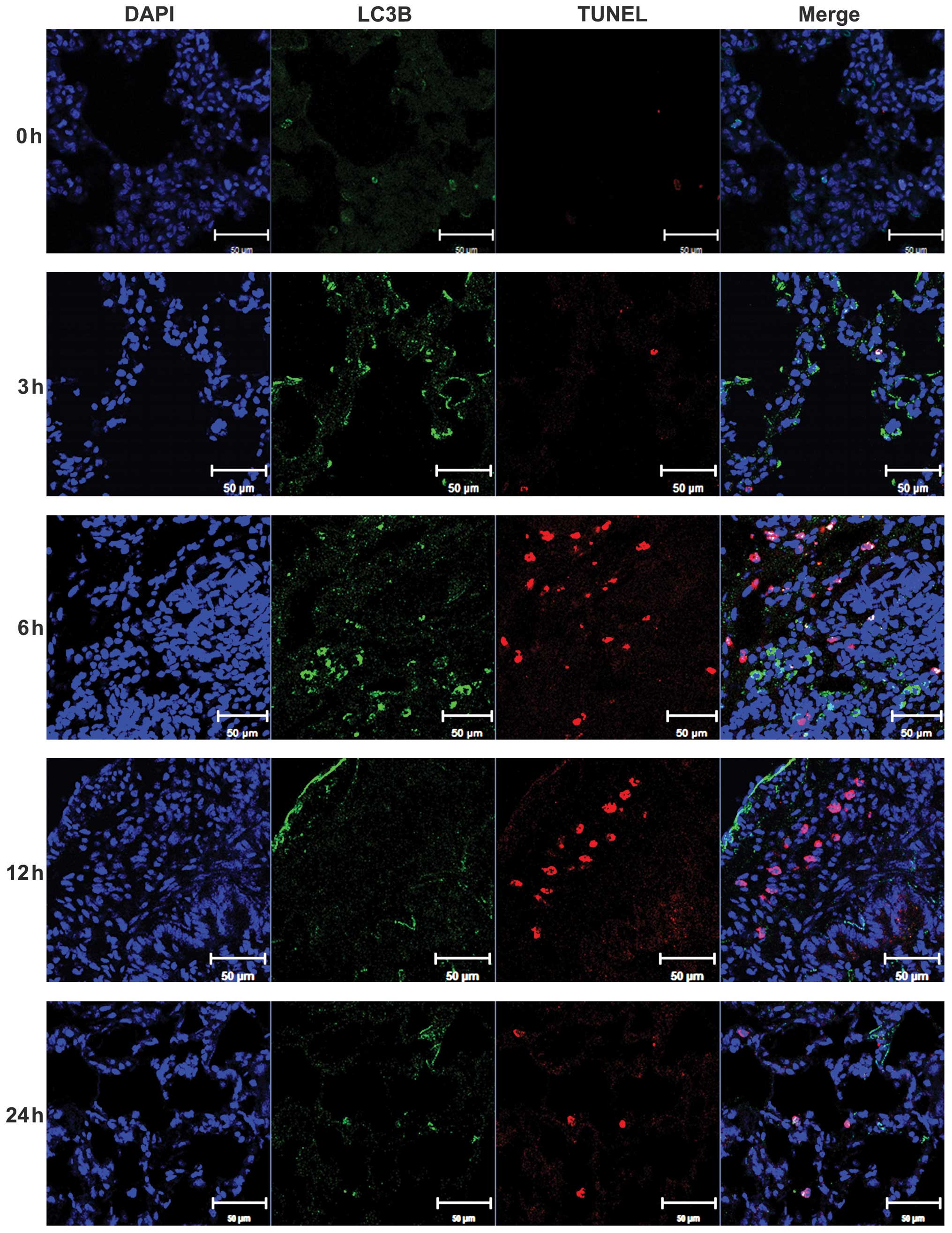
Autophagic cell death and apoptosis in
lung tissues following CI
Autophagic cell death and apoptosis in lung tissues
following CI was also determined. Apoptosis in lung tissues
following CI was initially verified through analyzing the changes
in the expression level of an apoptosis marker enzyme, caspase-3,
in each group. The level of cleaved caspase-3, the active form,
markedly increased between 6 and 24 h post-CI compared with the
basal level at 0 h (Fig. 4A and
B). In addition, the ratio of mRNA of the pro-/anti-apoptotic
genes Bax/Bcl-2 significantly increased between 6–12 h of CI
preservation (Fig. 4C). The
present results verified marked apoptosis in the lung CI model. To
identify autophagic cell death and apoptosis in lung tissues
following CI, double-immunofluorescence analysis of LC3B and TUNEL
(an apoptosis-specific staining assay) was performed. The results
clearly demonstrated that the levels of TUNEL-positive cells and
the LC3B-positive cells increased at 6 h after CI, compared with
the 0 h group (Fig. 5). The
LC3B-positive signals only partially colocalized with the TUNEL
signal when merged. Notably, the nuclei of the TUNEL-positive,
LC3B-negative cells were shrunken or fragmented, indicating the
presence of typical apoptotic nuclei. By contrast, the nuclei of
TUNEL- and LC3B- double positive cells were round, as usually
observed in autophagic cell death (19) (Fig.
6).
Discussion
Although significant progress has been made in the
study of the function of autophagy in a number of ischemic
conditions in vitro and in vivo, little is known with
regard to autophagy in lung tissues following CI preservation. The
present study revealed that autophagy is involved in lung CI
preservation and autophagic cell death in rat donor lungs that
undergo prolonged CI. This process may be involved in CI-induced
lung injury. These hypotheses are supported by the following
experimental evidence: i) In a lung CI model, autophagy was induced
and found to reach a peak at 6 h after CI compared with the basal
level at 0 h; ii) following 12 h of CI, the autophagic markers
decreased to the basal level. In addition to apoptosis, autophagic
cell death was also induced by lung CI preservation, which was
identified by double-immunofluorescence analysis of LC3B and
TUNEL.
Autophagy is a tightly regulated and highly
conserved physiological process involving the recycling of
cytoplasmic proteins and molecules within autophagolysosomes
(20,21). Starvation, hypoxemia and energy
depletion are potent stimulators of autophagy, in vitro and
in vivo (21). Under these
conditions, autophagy is hypothesized to enable cell survival by
recycling essential amino acids and cell metabolites (5,6,22).
The preservation of donor organs involves the rapid cooling of
ex vivo organs to 4°C (23). Although hypothermia is essential
for the preservation of donor lungs and significantly extends organ
viability, it is associated with inactivation of the sodium pump,
oxidative stress and the release of proinflammatory mediators
(1,24). Additionally, donor organs are
subjected to nutrient deprivation and energy depletion. These
events are effective triggers for autophagy, as has been
demonstrated in the liver (25–28),
kidney (29–31) and heart (32–35).
The results in the present study demonstrated that the protein or
mRNA levels of three autophagic markers (LC3B, Beclin-1 and
Atg5) in rat lung tissues significantly increased after 3–6
h of CI preservation, indicating that autophagy was significantly
induced in the rat lung tissues during CI preservation.
By contrast, autophagy has also been hypothesized to
be involved in cell death (32,36–40).
At present, at least three different types of cell death (necrosis,
apoptosis and autophagic cell death) are considered to be involved
in a number of ischemic events. Previous studies, however, have
only focused on necrosis and apoptosis, but not autophagic cell
death, as potential mechanisms of lung damage following CI
preservation (41,42). Autophagic cell death can be
morphologically differentiated from apoptotic cell death. The
nucleus is shrunken and fragmented in apoptosis, while it remains
round in autophagic cell death (14,19,43).
In the present study, immunostaining results demonstrated a partial
colocalization of LC3B and TUNEL signal in rat lung tissues
following CI preservation. The nuclei of TUNEL-positive and
LC3B-negative cells were shrunken or fragmented, which were typical
apoptotic nuclei; however the nuclei of the cells positive for
TUNEL and LC3B were observed to be round, which was consistent with
the nuclear morphology of autophagic cell death. These results
suggest that autophagic cell death may be involved in rat lung
injury following CI preservation.
There remains a number of limitations to the present
study. For example, to what extent the final pulmonary function may
be affected by autophagy and autophagic cell death during prolonged
CI preservation remains to be elucidated. Further investigations
are required to elucidate whether the function of autophagy is
protective or detrimental for donor lung tissue during CI and by
which molecular mechanism autophagy was induced in CI preservation.
In addition, the association between autophagy and apoptosis during
CI preservation also requires detailed investigation.
In conclusion, to the best of our knowledge this is
the first study demonstrating the activation of autophagy and
induction of autophagic cell death in lung tissue following CI
preservation. The present results suggest that CI preservation may
induce cell death in rat lung tissues through apoptosis, as well as
through autophagic cell death simultaneously, which may be
considered an important factor in future therapeutic approaches to
organ preservation for lung transplantation.
Acknowledgements
The authors would like to thank Dr Qiang Tan, Dr
Hui-fang Sha, Dr Xiao-hua Yang and Dr Xin Niu for their advice and
helpful suggestions. This study was supported by the Foundation of
Shanghai Municipal Health Bureau (grant no. 20124331) Young
Scientist Research Project of Shanghai Municipal Health Bureau
(grant no. 20134y074), Shanghai Natural Science Foundation (grant
no. 12ZR1428700) and Scientific Development Foundation of Shanghai
Chest Hospital (grant no. YZ13-33), ‘1050’ Foundation of Shanghai
Chest Hospital (grant no. 11-5).
References
|
1
|
de Perrot M, Liu M, Waddell TK and
Keshavjee S: Ischemia-reperfusion-induced lung injury. Am J Respir
Crit Care Med. 167:490–511. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Novick RJ, Menkis AH and McKenzie FN: New
trends in lung preservation: a collective review. J Heart Lung
Transplant. 11:377–392. 1992.PubMed/NCBI
|
|
3
|
de Perrot M and Keshavjee S: Lung
preservation. Semin Thorac Cardiovasc Surg. 16:300–308. 2004.
View Article : Google Scholar
|
|
4
|
Thabut G, Mal H, Cerrina J, et al: Graft
ischemic time and outcome of lung transplantation: a multicenter
analysis. Am J Respir Crit Care Med. 171:786–791. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee J, Giordano S and Zhang J: Autophagy,
mitochondria and oxidative stress: cross-talk and redox signalling.
Biochem J. 441:523–540. 2012. View Article : Google Scholar :
|
|
6
|
Mizushima N and Komatsu M: Autophagy:
renovation of cells and tissues. Cell. 147:728–741. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ogier-Denis E and Codogno P: Autophagy: a
barrier or an adaptive response to cancer. Biochim Biophys Acta.
1603:113–128. 2003.PubMed/NCBI
|
|
8
|
Shintani T and Klionsky DJ: Autophagy in
health and disease: a double-edged sword. Science. 306:990–995.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bursch W, Karwan A, Mayer M, et al: Cell
death and autophagy: cytokines, drugs and nutritional factors.
Toxicology. 254:147–157. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Clarke PG: Developmental cell death:
morphological diversity and multiple mechanisms. Anat Embryol
(Berl). 181:195–213. 1990. View Article : Google Scholar
|
|
11
|
Suzuki C, Isaka Y, Takabatake Y, et al:
Participation of autophagy in renal ischemia/reperfusion injury.
Biochem Biophys Res Commun. 368:100–106. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Matsui Y, Takagi H, Qu X, et al: Distinct
roles of autophagy in the heart during ischemia and reperfusion:
roles of AMP-activated protein kinase and Beclin 1 in mediating
autophagy. Circ Res. 100:914–922. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kanno H, Ozawa H, Sekiguchi A, Yamaya S
and Itoi E: Induction of autophagy and autophagic cell death in
damaged neural tissue after acute spinal cord injury in mice. Spine
(Phila Pa. 1976.36:E1427–E1434. 2011. View Article : Google Scholar
|
|
14
|
Rami A, Langhagen A and Steiger S: Focal
cerebral ischemia induces upregulation of Beclin 1 and
autophagy-like cell death. Neurobiol Dis. 29:132–141. 2008.
View Article : Google Scholar
|
|
15
|
Zhang J, Wang JS, Zheng ZK, et al:
Participation of autophagy in lung ischemia-reperfusion injury in
vivo. J Surg Res. 182:e79–e87. 2012. View Article : Google Scholar
|
|
16
|
Wu J, Wei J, You X, et al: Inhibition of
hydrogen sulfide generation contributes to lung injury after
experimental orthotopic lung transplantation. J Surg Res.
182:e25–e33. 2013. View Article : Google Scholar
|
|
17
|
Kabeya Y, Mizushima N, Ueno T, et al: LC3,
a mammalian homologue of yeast Apg8p, is localized in autophagosome
membranes after processing. EMBO J. 19:5720–5728. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ray SK, Matzelle DC, Wilford GG, Hogan EL
and Banik NL: E-64-d prevents both calpain upregulation and
apoptosis in the lesion and penumbra following spinal cord injury
in rats. Brain Res. 867:80–89. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chen Y, Azad MB and Gibson SB: Methods for
detecting autophagy and determining autophagy-induced cell death.
Can J Physiol Pharmacol. 88:285–295. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yang Z and Klionsky DJ: Mammalian
autophagy: core molecular machinery and signaling regulation. Curr
Opin Cell Biol. 22:124–131. 2010. View Article : Google Scholar :
|
|
21
|
Mizushima N, Yoshimori T and Levine B:
Methods in mammalian autophagy research. Cell. 140:313–326. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yang Z and Klionsky DJ: Eaten alive: a
history of macroautophagy. Nat Cell Biol. 12:814–822. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Okada Y and Kondo T: Preservation solution
for lung transplantation. Gen Thorac Cardiovasc Surg. 57:635–639.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zaouali MA, Ben Abdennebi H,
Padrissa-Altés S, Mahfoudh-Boussaid A and Roselló-Catafau J:
Pharmacological strategies against cold ischemia reperfusion
injury. Expert Opin Pharmacother. 11:537–555. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lu Z, Dono K, Gotoh K, et al:
Participation of autophagy in the degeneration process of rat
hepatocytes after transplantation following prolonged cold
preservation. Arch Histol Cytol. 68:71–80. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Gotoh K, Lu Z, Morita M, et al:
Participation of autophagy in the initiation of graft dysfunction
after rat liver transplantation. Autophagy. 5:351–360. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Minor T, Stegemann J, Hirner A and
Koetting M: Impaired autophagic clearance after cold preservation
of fatty livers correlates with tissue necrosis upon reperfusion
and is reversed by hypothermic reconditioning. Liver Transpl.
15:798–805. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Padrissa-Altés S, Zaouali MA, Bartrons R
and Roselló-Catafau J: Ubiquitin-proteasome system inhibitors and
AMPK regulation in hepatic cold ischaemia and reperfusion injury:
possible mechanisms. Clin Sci (Lond). 123:93–98. 2012. View Article : Google Scholar
|
|
29
|
Turkmen K, Martin J, Akcay A, et al:
Apoptosis and autophagy in cold preservation ischemia.
Transplantation. 91:1192–1197. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Jiang M, Liu K, Luo J and Dong Z:
Autophagy is a renoprotective mechanism during in vitro hypoxia and
in vivo ischemia-reperfusion injury. Am J Pathol. 176:1181–1192.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kaushal GP: Autophagy protects proximal
tubular cells from injury and apoptosis. Kidney Int. 82:1250–1253.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Petrovski G, Das S, Juhasz B, Kertesz A,
Tosaki A and Das DK: Cardioprotection by endoplasmic reticulum
stress-induced autophagy. Antioxid Redox Signal. 14:2191–2200.
2011. View Article : Google Scholar
|
|
33
|
Jiang S, Guo R, Zhang Y, Zou Y and Ren J:
Heavy metal scavenger metallothionein mitigates deep
hypothermia-induced myocardial contractile anomalies: role of
autophagy. Am J Physiol Endocrinol Metab. 304:E74–E86. 2013.
View Article : Google Scholar :
|
|
34
|
Hamacher-Brady A, Brady NR and Gottlieb
RA: Enhancing macroautophagy protects against ischemia/reperfusion
injury in cardiac myocytes. J Biol Chem. 281:29776–29787. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Loos B, Genade S, Ellis B, Lochner A and
Engelbrecht AM: At the core of survival: autophagy delays the onset
of both apoptotic and necrotic cell death in a model of ischemic
cell injury. Exp Cell Res. 317:1437–1453. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gurusamy N, Lekli I, Gorbunov NV,
Gherghiceanu M, Popescu LM and Das DK: Cardioprotection by
adaptation to ischaemia augments autophagy in association with
BAG-1 protein. J Cell Mol Med. 13:373–387. 2009. View Article : Google Scholar
|
|
37
|
Huang C, Yitzhaki S, Perry CN, et al:
Autophagy induced by ischemic preconditioning is essential for
cardioprotection. J Cardiovasc Transl Res. 3:365–373. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sala-Mercado JA, Wider J, Undyala VV, et
al: Profound cardioprotection with chloramphenicol succinate in the
swine model of myocardial ischemia-reperfusion injury. Circulation.
122:S179–S184. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Shi R, Weng J, Zhao L, Li XM, Gao TM and
Kong J: Excessive autophagy contributes to neuron death in cerebral
ischemia. CNS Neurosci Ther. 18:250–260. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Balduini W, Carloni S and Buonocore G:
Autophagy in hypoxia-ischemia induced brain injury. J Matern Fetal
Neonatal Med. 25 Suppl 1:30–34. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Fischer S, Cassivi SD, Xavier AM, et al:
Cell death in human lung transplantation: apoptosis induction in
human lungs during ischemia and after transplantation. Ann Surg.
231:424–431. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Ng CS, Wan S and Yim AP: Pulmonary
ischaemia-reperfusion injury: role of apoptosis. Eur Respir J.
25:356–363. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kitanaka C and Kuchino Y:
Caspase-independent programmed cell death with necrotic morphology.
Cell Death Differ. 6:508–515. 1999. View Article : Google Scholar : PubMed/NCBI
|