Introduction
Hepatitis B is a global chronic disease caused by
the hepatitis B virus (1). One
consequence of infection with the hepatitis B virus is the
development liver fibrosis, which can determine the prognosis as
well as the therapy that is required (2). Fibrosis may progress to cirrhosis,
which is an irreversible condition that may be viewed as the
terminal stage of hepatitis. However, with the exception of a
biopsy, there are currently no reliable indicators of the degree of
liver fibrosis. Biopsies are invasive and there is a risk of
serious complications (in up to 0.4% of cases). Furthermore, the
results vary due to sampling errors, and intraobserver and
interobserver variability (3).
Therefore, the development of noninvasive examination methods is
required, including real-time elastography, transient elastography
(TE) and acoustic radiation force impulse elastography (ARFI)
(4).
Liver stiffness measurement (LSM) using TE
(FibroScan®) is accurate in identifying significant
fibrosis, and in particular cirrhosis, in a number of liver
diseases (5). This system is
equipped with a probe consisting of an ultrasonic transducer
mounted on the axis of a vibrator. A vibration of mild amplitude
and low frequency is transmitted from the vibrator to the tissue by
the transducer. This vibration induces an elastic shear wave which
propagates through the tissue. At the same time, pulse-echo
ultrasonic acquisitions are performed in order to follow the
propagation of the shear wave and measure its velocity, which is
directly associated with tissue stiffness (or elastic modulus). The
harder the tissue, the faster the shear wave propagates. Recently,
a study has shown that liver stiffness measurement using FibroScan
allows the accurate prediction of hepatic fibrosis in patients with
chronic hepatitis C virus infection (6). However, the cut-off values for
different histological stages vary substantially between studies,
patient groups and the aetiology of liver disease (5,6).
Recent studies have proposed that liver stiffness
measurement may be conducted using ARFI elastography as a novel,
reliable and accurate noninvasive approach to the evaluation of
liver fibrosis (7). Studies have
analyzed the performance of ARFI (8–13),
although a number of these reports were heterogeneous, with small
cohorts of patients and, in certain cases, without confirmation by
liver biopsy. The combination of non-invasive tests for fibrosis
may circumvent these limitations while improving diagnostic
accuracy and resolving the discordances between tests (14). In this setting, Boursier and Cales
(15) have proposed that a
combination of liver stiffness evaluation (LSE) and blood tests for
fibrosis may improve the diagnostic accuracy in patients with
chronic hepatitis C. However, in a separate study, Castéra et
al (16) reported that a
combination of LSE and blood test did not improve the accuracy with
which cirrhosis was diagnosed, although only a small number of
blood tests was used, which were not contemporaneous. Whether the
combination of ARFI and additional serological markers improves the
diagnostic accuracy, thereby reducing the requirement for liver
biopsy in patients with hepatitis B, has remained to be
determined.
The Forns’ index (FI) is based on the platelet
count, γ-glutamyl transpeptidase, age and cholesterol levels. The
presence of significant fibrosis was predicted with a 96% negative
predictive value (NPV) and 66% positive predictive value (PPV)
using this method (17).
The aim of the present study was to assess the
diagnostic accuracy of ARFI, FibroScan and FI, and to explore their
combined effectiveness in evaluating liver fibrosis, with biopsy
samples as the reference standard. In addition, the impact of
inflammatory activity and steatosis on these diagnostic methods was
investigated.
Materials and methods
Patients
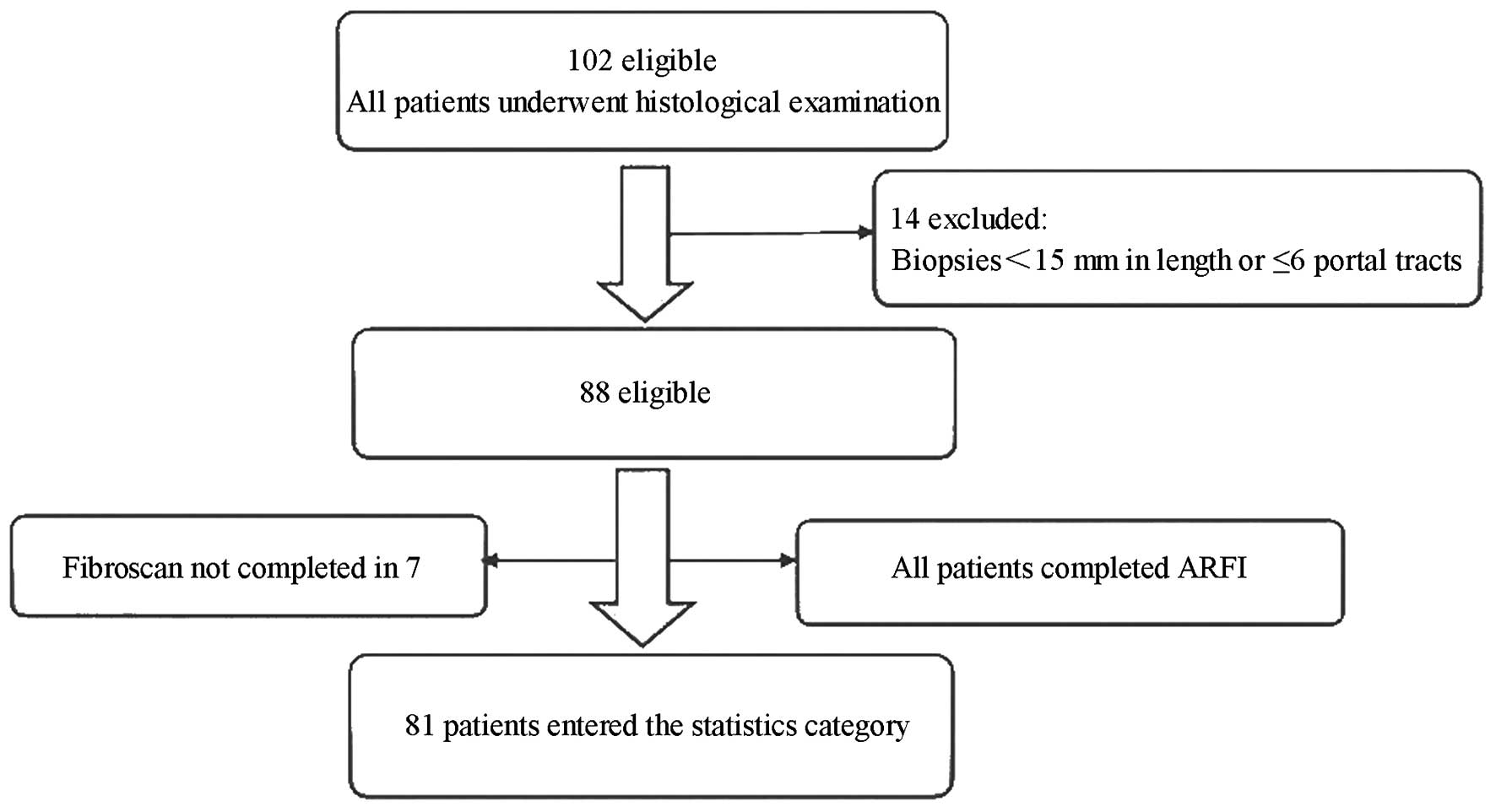
The present study comprised 81 consecutive patients
with chronic hepatitis B (CHB), who had been admitted to the
China-Japan Friendship Hospital (Beijing, China) from January 2011
to April 2013 (Fig. 1). The study
was conducted in accordance with the declaration of Helsinki and
with approval from the Ethics Committee of the China-Japan
Friendship Hospital. Written informed consent was obtained from all
participants. The diagnosis was made in accordance with guidelines
for the prevention and treatment of CHB, published by the Chinese
Medical Association in 2010 (18).
The criteria for study inclusion were: i) Age, 18–65 years,
irrespective of gender; ii) CHB of various degrees in association
with liver fibrosis; iii) no intake of medication known to inhibit
liver enzymes within two weeks prior to biochemical blood analysis;
iv) history of abnormal transaminase; and v) provision of signed
informed consent by the patient. The criteria for study exclusion
were: i) Unavailability of patient consent; ii) other complicated
liver conditions, including other types of viral hepatitis,
alcoholic and nonalcoholic fatty liver disease, autoimmune
hepatitis and inherited metabolic liver disease; iii) hepatic
decompensation, including the presence of ascites; iv) body mass
index (BMI) ≥30; v) non-healed upper quadrant abdominal wound; vi)
space-occupying tumors or cysts in the right lobe of the liver or
various space-occupying tumors and cysts; and vii) acute hepatitis
or cholestatic hepatitis.
LSM
Measurements of TE using FibroScan were performed by
a single trained operator. Patients were placed in the supine
position with their right arm fully abducted. Measurements were
taken from the area over the right lobe of the liver through the
intercostal space. At least ten valid TE readings were obtained for
each patient and the median value was used for analysis. The
results are expressed in kPa. Those cases with a success rate
<60% and an interquartile range (IQR)/result ratio >0.3 were
regarded as invalid.
ARFI imaging
Immediately following the FibroScan, the same
technician performed a shear wave velocity measurement using ARFI
imaging. The right lobe of the liver was localized using a
SEQUIOA512 color ultrasound diagnostic system (Siemens Medical
Equipment Co., Ltd., Shanghai, China) at a transducer frequency of
5–12 MHz. Ten valid acquisitions were obtained in the region of
interest, with the probe positioned 2.5 cm below the skin. All
measurements were obtained at the same intercostal space, avoiding
large vessels and ribs. The mean, standard deviation (SD) and
variation coefficient (SD/mean) of the values from each patient
were recorded for statistical analysis.
FI
Laboratory test results, including tests for
hepatitis B, liver function, complete blood count and HBV-DNA were
collected. The FI was calculated using the following formula:
FI=7.811−3.131×ln[platelet (×109/L)] +
0.781×ln[γ-glutamyl transpeptidase (GGT)] + 3.647 U/L × ln[age
(years)]−0.014×cholesterol (mg/dl).
Liver histology
Liver biopsies were obtained using 16 G or 18 G
disposable needles (Bard Peripheral Vascular, Inc., Murray Hill,
NJ, USA). Liver biopsy specimens were fixed in formalin, embedded
in paraffin and stained with hematoxylin and eosin, silver, Masson
Trichrome staining and Sirius Red (all Wuhan Boster Biotechnology,
Ltd, Wuhan, China). Necro-inflammatory activity and liver fibrosis
was scored according to the biopsy criteria of the Chinese Program
of Prevention and Cure for Viral Hepatitis (Tables I and II) (19).
 | Table ICriteria for the grading of chronic
hepatitis. |
Table I
Criteria for the grading of chronic
hepatitis.
| Grading | Portal tract and
periportal inflammation | Lobular
inflammation |
|---|
| 0 | Absent | Absent |
| 1 | Portal
inflammation | Degeneration and few
potty, focal necrosis |
| 2 | Mild piecemeal
necrosis | Degeneration, spotty,
focal necrosis or acidophilic body |
| 3 | Moderate piecemeal
necrosis | Degeneration,
confluent necrosis or bridging necrosis |
| 4 | Severe piecemeal
necrosis | Widely bridging
necrosis, involved multiple lobule (multiple lobule necrosis) |
| Table IICriteria for the staging of chronic
hepatitis. |
Table II
Criteria for the staging of chronic
hepatitis.
| Staging | Degree of
fibrosis |
|---|
| 0 | Absent |
| 1 | Portal fibrosis to be
enlarged, localized perisinusoidal and intralobular fibrosis |
| 2 | Periportal fibrosis,
several fibrous septa with lobule structure remaining |
| 3 | Numerously fibrous
septa companied, Lobule structure distortion, without
cirrhosis |
| 4 | Early cirrhosis |
Statistical analysis
Quantitative variables are expressed as the median
(range) and qualitative variables as a percentage. The correlation
between the stage of fibrosis and results of the non-invasive tests
was assessed using a non-parametric test (Kruskal-Wallis analysis).
The diagnostic value of ARFI, FibroScan and FI in predicting
significant fibrosis and cirrhosis was assessed by calculating the
areas under the respective receiver operator characteristic curves
(AUROC). Comparisons of AUROCs were performed according to the
Delong method (20). Best cut-off
values were determined by optimization of the Younden index, and
sensitivity, specificity, as well as positive and negative
predictive values (PPV, NPV) were calculated from these same data.
For univariate analysis, bivariate Spearman’s rank correlation
coefficient was calculated to measure the association between FI,
ARFI, FibroScan and other variables, including steatosis. For the
subsequent multivariate analysis, a linear regression analysis was
performed in order to identify the independent variables
influencing the accuracy of the three diagnostic methods. For
multiple values, analysis of variance with Chi-squared test was
used. Statistical analyses were performed with SPSS, version 17.0
(SPSS, Inc., Chicago, IL, USA). P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient characteristics
The baseline clinical and biochemical
characteristics of the patients are summarized in Table III. The subjects consisted of 71
males (87.7%). The mean age of the patients was 41±11.4 years. The
mean BMI was 23±3.0.
| Table IIIBaseline characteristics (n=81). |
Table III
Baseline characteristics (n=81).
| Characteristic | Fibrosis stage, n (%)
|
|---|
| Total | S0 | S1 | S2 | S3 | S4 |
|---|
| Male gender | 71 (87.7) | 2 (22.2) | 21 (84.0) | 24 (96.0) | 13 (81.2) | 8 (100) |
| Age (years) | 41±11.4 | 38±12.3 | 38±10.2 | 40±11.9 | 46±12.0 | 48±6.2 |
| Steatosis | 30/74 | 0/1 | 11/25 | 7/24 | 9/16 | 3/8 |
| (n/total) | | | | | | |
| Inflammation | – | 9 (G0:9 G1:0 G2:0
G3:0 G4:0) | 25 (G0:0 G1:11
G2:14 G3:0 G4:0) | 25 (G0:0 G1:5 G2:14
G3:6 G4:0) | 16 (G0:0 G1: 3 G2:7
G3:5 G4:1) | 8 (G0:0 G1: 1 G2:5
G3:2 G4:0) |
| BMI | 23±3.0 | 22±1.9 | 23±2.0 | 24±3.5 | 23±3.3 | 25±3.6 |
| GGT | 58±66.5 | 98±42.9 | 36±7.4 | 41±7.3 | 68±14.8 | 129±56.3 |
| PLT | 176±63.4 | 199±35.3 | 205±46.9 | 182±71.3 | 140±58.7 | 112±56.6 |
| TBIL | 17±21.9 | 41±24.0 | 15±1.4 | 13±0.8 | 17±1.7 | 16±4.4 |
| CHO | 6±12.6 | 5±0.4 | 10±5.0 | 5±0.2 | 4±0.2 | 5±0.5 |
| ALP | 78±35.1 | 105±58.3 | 64±11.6 | 66±17.0 | 85±27.4 | 85±14.6 |
| PT (INR) | 1±0.1 | 0.9±0.1 | 1.0±0.1 | 1.0±0.1 | 1.0±0.1 | 1.1±0.1 |
| ALB | 44±9.4 | 46±2.3 | 43±14.1 | 46±3.5 | 43±9.4 | 43±2.9 |
Correlation between stage of fibrosis
assessed by biopsy and that measured using non-invasive
methods
A significant association was identified between the
stage of fibrosis and the values obtained by ARFI, FibroScan and
FI. The median values of ARFI according to fibrosis stage were
1.28±0.21, 1.33±0.32, 1.43±045, 2.07±0.61 and 1.98±0.52 m/s for
S0–S4, respectively, while the median FibroScan measurements were
4.8±0.01, 6.69±0.23, 9.87±2.11, 14.8±3.24 and 24.2±5.11 kPa for
S0–S4, respectively, and the mean FI scores in patients with S0,
S1, S2, S3 and S4 stages of liver fibrosis were 6.75±1.17,
6.21±1.38, 7.23±2.25, 8.68±1.71 and 10.31±1.58, respectively
(Fig. 2).
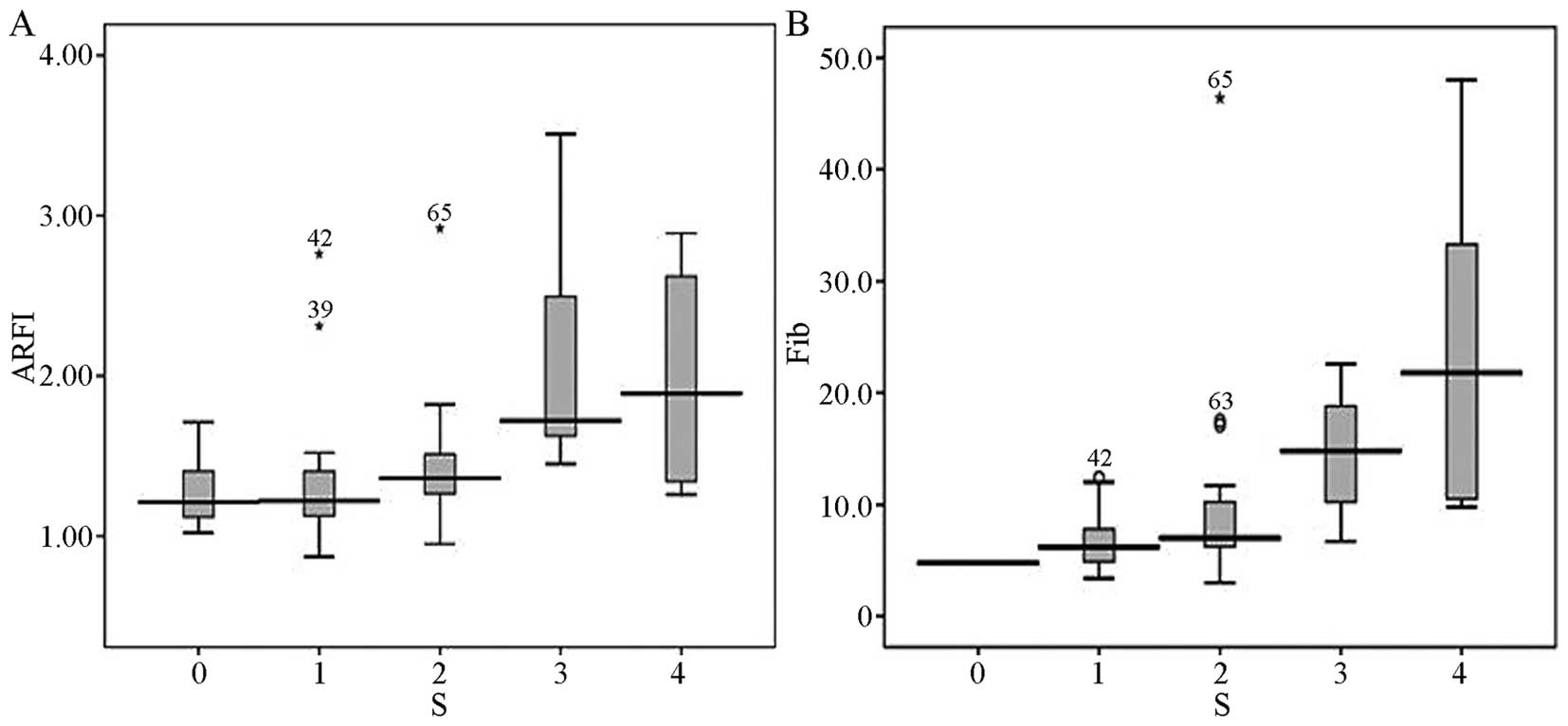 | Figure 2Median ARFI and liver stiffness values
in patients with different stages of liver fibrosis. (A) Median
ARFI values in patients with S0, S1, S2, S3 and S4 were 1.28, 1.33,
1.43, 2.07 and 1.98 m/s, respectively. (B) Median liver stiffness
values in patients with S0, S1, S2, S3 and S4 were 4.8, 6.69, 9.87,
14.8 and 24.2 kPa, respectively. Upper horizontal line, maximum
value beside outlier; lower horizontal line, the minimum value;
middle horizontal line, median; box, ¼–3/4 of values;
star/circle/dot, outliers. ARFI, acoustic radiation force impulse
elastography; Fib, FibroScan. |
The normal distribution using Pearson’s correlation
and the partial distribution using the Spearman’s correlation
demonstrated that the three diagnostic methods significantly
correlated with the stage of fibrosis [ARFI (r=0.577, P<0.001);
FibroScan (r=0.629, P<0.001); and FI (r=0.539, P<0.001)].
Diagnosis of S≥2 and cirrhosis using
individual and combinations of methods
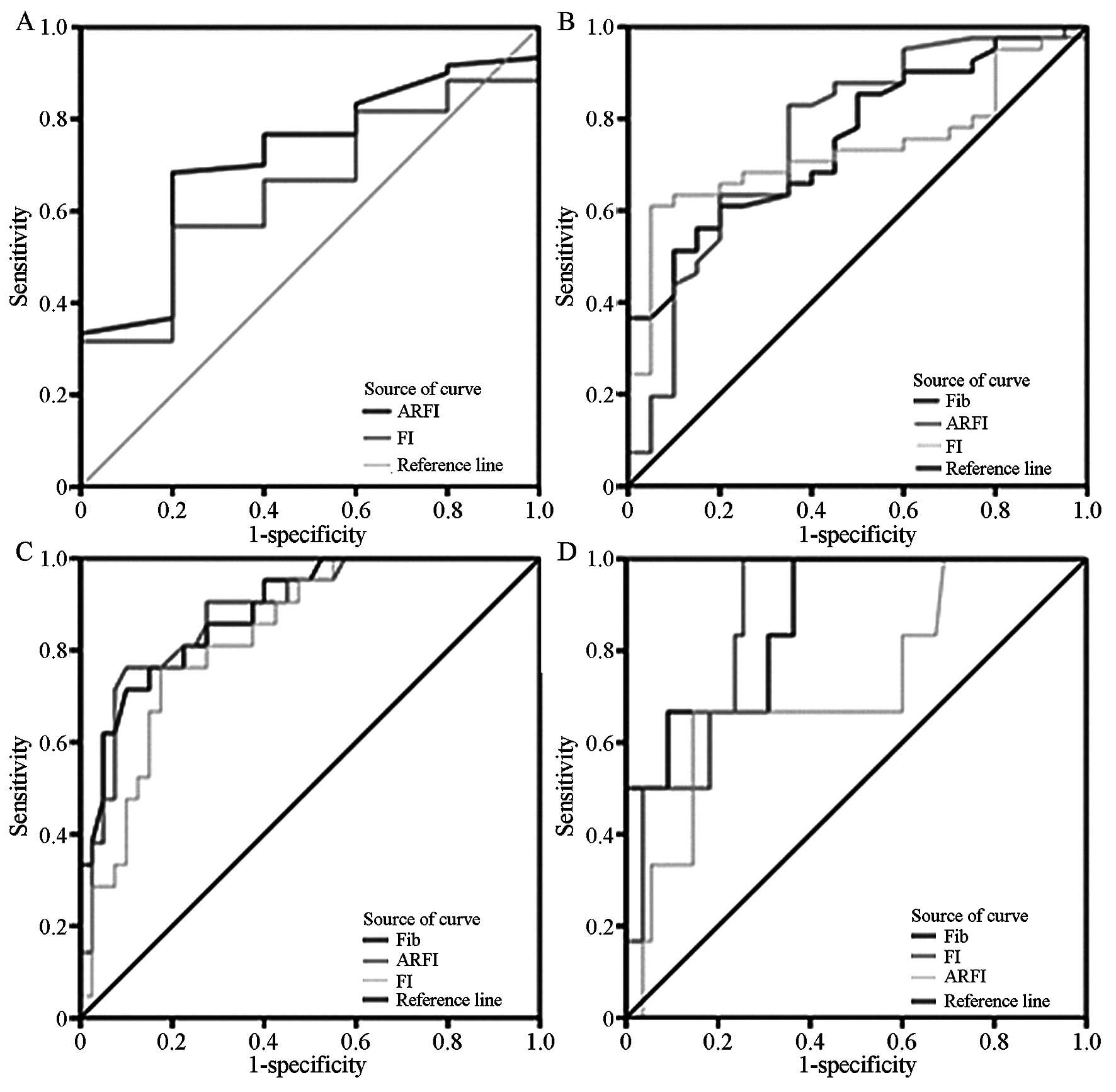
In order to evaluate the power of ARFI, FibroScan
and FI to accurately predict the stage of fibrosis in this
population of patients, an ROC analysis was performed. This
analysis revealed that the AUROCs of ARFI, FibroScan and FI
compared with the stage of fibrosis, as determined by liver biopsy,
were 0.790±0.084, 0.838±0.074 and 0.814±0.721, respectively, for
S≥2. Table IV and Fig. 3 depict the AUROCs and show the
diagnostic performance of the three methods.
| Table IVDiagnostic performance of ARFI,
FibroScan and FI for the diagnosis of different histological
stages. |
Table IV
Diagnostic performance of ARFI,
FibroScan and FI for the diagnosis of different histological
stages.
| Variable | Mode | ≥S1 | ≥S2 | ≥S3 | S4 |
|---|
| Cut-off | ARFI | 1.295 | 1.295 | 1.54 | 1.835 |
| Fib | – | 10.3 | 11.85 | 9.4 |
| FI | 6.82 | 7.55 | 7.902 | 8.45 |
| AUROCs | ARFI | 0.720 | 0.762 | 0.884 | 0.723 |
| Fib | 0 | 0.753 | 0.888 | 0.873 |
| FI | 0.650 | 0.735 | 0.832 | 0.876 |
| 95%CI | ARFI | 0.524–0.916 | 0.627–0.896 | 0.798–0.970 | 0.501–0.944 |
| Fib | – | 0.631–0.875 | 0.805–0.970 | 0.740–1.006 |
| FI | 0.452–0.828 | 0.610–0.861 | 0.731–0.933 | 0.771–0.981 |
| Se (%) | ARFI | 68.3 | 82.9 | 76.2 | 66.7 |
| Fib | – | 51.2 | 71.4 | 100 |
| FI | 56.7 | 61.0 | 76.2 | 100 |
| Sp (%) | ARFI | 80.0 | 65.0 | 90.0 | 85.5 |
| Fib | – | 90.0 | 90.0 | 63.6 |
| FI | 80.0 | 95.0 | 82.5 | 74.5 |
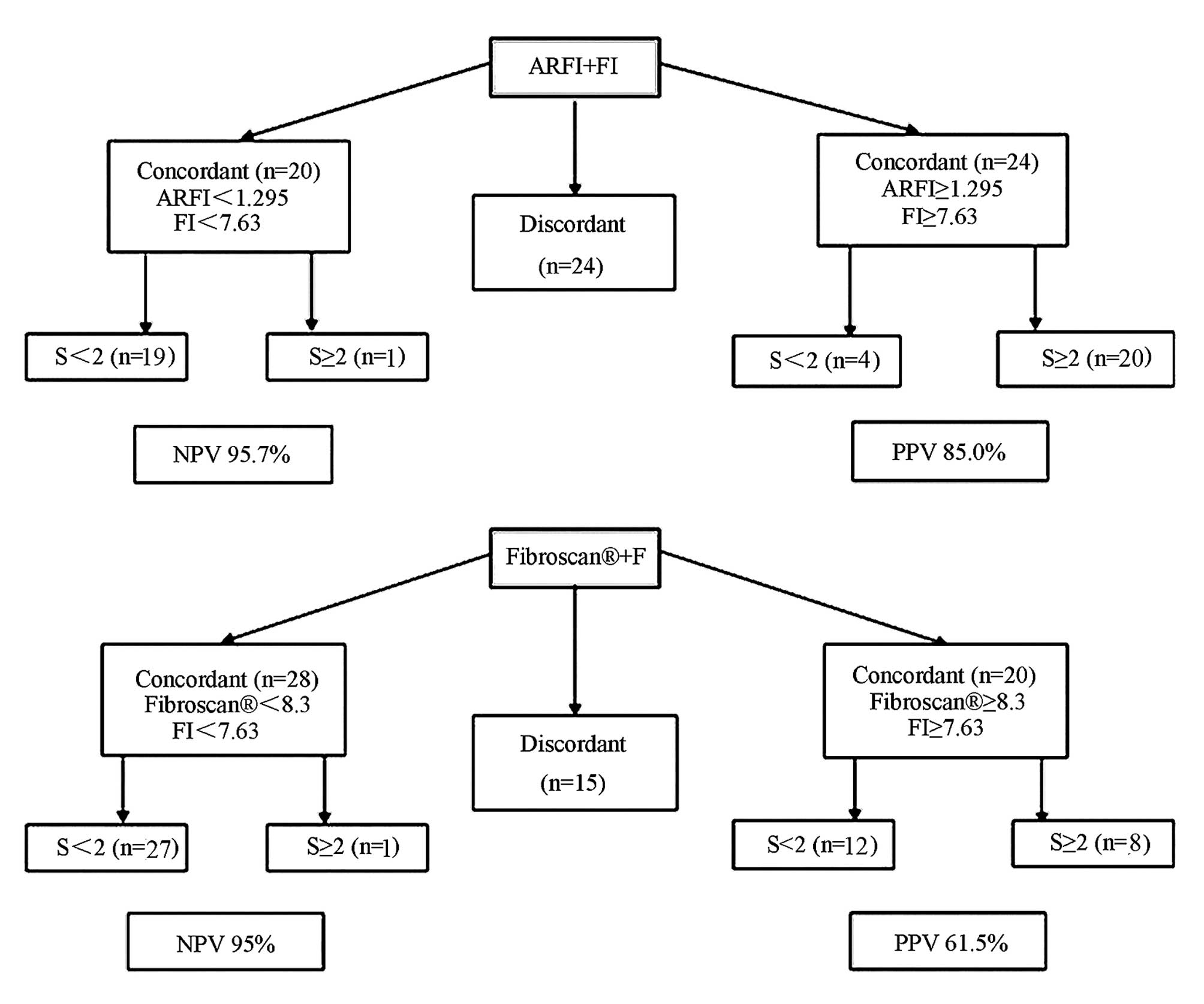
When the methods were combined using the cut-offs
shown in Table IV, the PPV for
the joint use of FI and ARFI for the diagnosis of S≥2 was 85.0%,
while the NPV was 95.7%. Similarly, the PPV and NPV for the
combination of FibroScan and FI were 61.5 and 95.0%, respectively,
for S≥2 (Table V, Fig. 4).
| Table VDiagnostic performance of FI with
either ARFI or FibroScan for the diagnosis of S≥2. |
Table V
Diagnostic performance of FI with
either ARFI or FibroScan for the diagnosis of S≥2.
| Mode | PPV | NPV | FPR (%) | FNR (%) | Se (%) | Sp (%) | Accuracy |
|---|
| ARFI + FI | 85.0 | 95.7 | 12.0 | 5.6 | 94.4 | 88.0 | 90.7 |
| Fib + FI | 61.5 | 95 | 34.5 | 5.9 | 94.1 | 65.5 | 76.1 |
Inflammation is correlated with
fibrosis
ARFI measurements were 1.21, 1.25, 1.41, 1.71 and
2.4 m/s for inflammation grades G0, G1, G2, G3 and G4, respectively
(P=0.005). FibroScan measurements were 4.8, 6.8, 7.8, 13.4 and 22.6
kPa for inflammation grades G0, G1, G2, G3 and G4, respectively
(P=0.002). Finally, for FI they were 6.76±1.17, 6.48±1.58,
7.61±2.22, 8.82±2.29 and 9.51±2.18 for inflammation grades G0, G1,
G2, G3 and G4, respectively (P=0.034). There was no significant
different between G0 and G1 as well as between G2, G2 and G3,
although there were statistically significant differences between
G0 and G3 as well as G1 and G3. Spearman’s correlation test was
performed in order to identify whether inflammation altered the
prediction of fibrosis by the various diagnostic methods. There was
no significant correlation between the degree of inflammation and
the stage of fibrosis.
In order to assess the influence of hepatic
inflammation on the ARFI, FibroScan and FI scores, patients with
liver fibrosis and significant inflammation (G2 or higher) were
compared with patients with fibrosis but without inflammation (G0).
In this analysis, no significant correlation between ARFI,
FibroScan and FI results, with inflammation grades was detected
(Table VI).
| Table VIDiagnostic performance of ARFI,
FibroScan and FI for G<2 and G≥2. |
Table VI
Diagnostic performance of ARFI,
FibroScan and FI for G<2 and G≥2.
| Stage | Mode | G<2 | G≥2 | P-value |
|---|
| S1 | ARFI | 1.13 | 1.285 | 0.201 |
| Fib | 6.7 | 6.15 | 0.688 |
| FI | 6.14±1.88 | 6.27±1.57 | 0.841 |
| S2 | ARFI | 1.36 | 1.41 | 0.406 |
| Fib | 6.5 | 8.15 | 0.227 |
| FI | 6.09±1.81 | 7.59±2.30 | 0.199 |
| S3 | ARFI | 1.5 | 2.085 | 0.136 |
| Fib | 7.7 | 16.85 | 0.101 |
| FI | 8.16±1.65 | 8.80±1.78 | 0.579 |
Influence of steatosis on prediction of
fibrosis
The effects of concomitant steatosis on the results
obtained by the different diagnostic methods were investigated.
Therefore, all patients were divided into one group with hepatitis
B and fatty liver and another group with uncomplicated hepatitis B.
No statistically significant differences were detected between the
two groups (P-values were 0.403, 0.162 and 0.200,
respectively).
Univariate correlation analysis was performed
between ARFI, FibroScan and FI, and other variables, including
steatosis. The stage of fibrosis was the variable most
significantly correlated with ARFI, FibroScan and FI scores.
Platelet count, prothrombin time, activity grade and γ-glutamyl
transpeptidase levels were also significantly correlated with ARFI,
FibroScan and FI, while the presence of steatosis was not (Table VII).
| Table VIIUnivariate correlation analysis
between ARFI, FibroScan, Forns’ index and other variables. |
Table VII
Univariate correlation analysis
between ARFI, FibroScan, Forns’ index and other variables.
| Variable | FibroScan
| ARFI
| Forns’ index
|
|---|
| Correlation
coefficient | P-value | Correlation
coefficient | P-value | Correlation
coefficient | P-value |
|---|
| Fibrosis stage | 0.629 | <0.001 | 0.577 | <0.001 | 0.528 | <0.001 |
| Platelet count | −0.380 | 0.001 | −0.359 | 0.001 | −0.803 | <0.001 |
| Prothrombin
time | 0.347 | 0.004 | 0.259 | 0.025 | 0.359 | 0.002 |
| Albumin | −0.239 | 0.074 | −0.377 | 0.003 | −0.219 | 0.092 |
| Age | 0.202 | 0.094 | 0.202 | 0.094 | 0.202 | 0.094 |
| Bilirubin | 0.250 | 0.039 | 0.181 | 0.118 | 0.325 | 0.004 |
| Activity grade | 0.451 | <0.001 | 0.441 | <0.001 | 0.337 | 0.004 |
| Body mass
index | 0.300 | 0.014 | 0.005 | 0.965 | 0.100 | 0.407 |
| Gender | −0.012 | 0.920 | −0.012 | 0.920 | −0.012 | 0.920 |
| HbeAg
positivity | 0.040 | 0.743 | 0.040 | 0.743 | 0.040 | 0.743 |
| Alkaline
phosphatase | 0.294 | 0.015 | 0.414 | <0.001 | 0.106 | 0.365 |
| γ-glutamyl
transpeptidase | 0.680 | <0.001 | 0.338 | 0.004 | 0.460 | <0.001 |
| Steatosis
score | 0.170 | 0.163 | −0.100 | 0.407 | 0.154 | 0.216 |
Table VIII shows
the results of the linear regression analysis used to identify the
independent variables influencing ARFI, FibroScan and FI. Steatosis
failed to show a statistically significant effect.
| Table VIIIMultivariate analysis toward
predicting ARFI, FibroScan and Forns’ index. |
Table VIII
Multivariate analysis toward
predicting ARFI, FibroScan and Forns’ index.
| Variable | FibroScan
| ARFI
| Forns’ index
|
|---|
| Estimate | P-value | Estimate | P-value | Estimate | P-value |
|---|
| Fibrosis stage | 0.384 | 0.001 | 0.042 | 0.768 | 0.179 | 0.047 |
| Steatosis | 0.139 | 0.108 | −0.062 | 0.559 | 0.111 | 0.128 |
| Platelet | 0.006 | 0.951 | −0.084 | 0.131 | −0.675 | <0.001 |
| Prothrombin
time | 0.088 | 0.319 | 0.282 | 0.017 | 0.069 | 0.384 |
| Bilirubin | 0.120 | 0.146 | – | – | 0.106 | 0.156 |
| Activity grade | −0.043 | 0.629 | 0.112 | 0.332 | −0.046 | 0.575 |
| Body mass
index | 0.116 | 0.180 | – | – | – | – |
| Alkaline
phosphatase | 0.017 | 0.844 | 0.339 | 0.005 | – | – |
| γ-glutamyl
transpeptidase | 0.497 | <0.001 | 0.399 | 0.002 | 0.108 | 0.182 |
Discussion
Liver biopsy is currently the gold standard used to
determine the stage of liver fibrosis, with the results being used
to assess the disease stage as well to decide on the appropriate
therapy (9). However, a biopsy is
an invasive test, which requires the patient to be hospitalized and
is associated with certain risks, including pain and bleeding. In
addition, liver biopsies are more expensive than noninvasive tests
and the results are subject to sampling errors. A further
limitation of liver biopsy is that different pathologists may
interpret the same sample differently, which may result in
discrepancies in disease staging. Therefore, noninvasive tests have
recently been developed. ARFI and TE (FibroScan) are rapid
techniques with highly reproducible results that may be used for
measuring liver tissue stiffness. A number of studies have
demonstrated the accuracy of these methods in assessing the degree
of hepatic fibrosis (17,21).
The FI is based on platelet count, GGT, age and
cholesterol. The presence of significant fibrosis has been shown to
be predicted with a 96% negative predictive value (NPV) and a 66%
positive predictive value (PPV) (22). Novel scores or biomarkers have been
used to improve the prediction of fibrosis and may help to detect
severe fibrosis, although they lack sensitivity and specificity
(20,23). Therefore, it is probable that a
combination of different non-invasive markers may be required to
ensure accurate diagnoses. Boursier et al (21) have suggested that a combination of
LSE and blood tests for fibrosis may improve diagnostic accuracy in
patients with chronic hepatitis C. However, their study did not
evaluate the statistical differences between the area under the
receiver operating characteristic curves, which is the only
diagnostic index used for fibrosis tests and their combination.
Furthermore, in clinical practice these methods assessing liver
elasticity may be effected by a number of factors; predominantly by
hepatic fibrosis, but also by necrosis-inflammatory activity
(16), body mass index (24), steatosis (25) and extrahepatic cholestasis
(26,27).
In the present study, measurements obtained by ARFI
and FibroScan as well as FI scores were significantly correlated
with the stage of fibrosis in patients with hepatitis B, as
assessed by liver biopsy, which suggested that these noninvasive
diagnostic methods were adequate for evaluation of the stage of
liver fibrosis.
Recent studies have suggested that the combination
of serum markers with FibroScan is highly accurate in the
identification of liver fibrosis (28). In the present study, the
combination of FI with either FibroScan or ARFI increased the PPV
and NPV of any of the tests individually and provided reliable
identification of significant fibrosis and cirrhosis in a large
proportion of patients. These results suggested that a large number
of patients with liver fibrosis may be diagnosed and staged without
any biopsy required.
A number of factors affect liver stiffness. Studies
have shown that inflammation activity can alter the LSM value
(29). Coco et al (30) reported that liver stiffness
increased 1.3- to 3-fold following temporary increases in the
levels of alanine transaminase, but that it decreased to baseline
values thereafter. The same study demonstrated that liver stiffness
was significantly different in patients with hepatitis inflammation
in comparison with patients with stable biochemical markers. It was
postulated that the inflammatory infiltrate and edema may have had
an impact on the TE value (31).
In the present study, the results of assessment
using ARFI, FibroScan and FI were significantly different depending
on the grade of inflammation. Further comparison of the interclass
groups G0 and G1 as well as G2, G2 and G3 demonstrated no
significant differences, although there were statistically
significant differences between G0 and G3, and between G1 and G3.
It may be that inflammatory activity stimulates the activation and
proliferation of hepatic stellate cells, thus increasing the levels
of collagen I and III.
Hepatic steatosis may be another factor that
influences liver stiffness values. Fatty tissues are softer than
healthy liver parenchyma, which reduces liver stiffness (30,32).
A number of studies have investigated the impact of steatosis on
liver stiffness. Sandrin et al (33) reported that elasticity measurements
were correlated with the stage of fibrosis only and not with
necro-inflammatory activity or steatosis grades in patients with
chronic hepatitis C. A recent study conducted on healthy subjects
suggested that liver stiffness values are not influenced by
steatosis (34). In the present study, no significant difference in
elasticity was detected between patients with hepatitis B who had
fatty liver and those who did not. Furthermore, in the univariate
analysis, steatosis had no influence on the results of the three
methods of diagnosis in patients with CHB. There are naturally
limitations to the present study: The ALT levels were not
considered, and as ALT was recently shown to be a significant
factor influencing LSM (33), the
results of the present study may be misleading. Furthermore, the
results are based on a small sample size; the number of patients
with fatty liver was only 30. Thus, larger, multicenter studies are
required to confirm or refute these findings.
In conclusion, ARFI, FibroScan and FI were proven to
be reliable methods with which to assess fibrosis in patients with
hepatitis B. Indeed, the combined use of FI with either ARFI or
FibroScan appears to be a promising approach, which may increase
the diagnostic accuracy of these tests individually. In addition,
combining these approaches resolves the majority of discordant
results between non-invasive tests and improves the reliable
individual diagnosis for significant fibrosis and cirrhosis, thus
reducing the requirement for liver biopsies. Inflammatory activity
may influence the diagnostic value of these methods to a certain
extent. However, steatosis did not produce a significant impact on
the diagnostic values in patients with CHB. The methods evaluated
in the present study are an ideal tool for diagnosis and detecting
changes in the stage of fibrosis and may therefore be useful for
monitoring disease progression and regression, as well as in
predicting clinical outcomes in the future.
Acknowledgments
This study was supported by Beijing Science &
Technology Commission (grant no. D121100003912002).
References
|
1
|
Iroezindu MO, Agbaji OO, Daniyam CA,
Isiguzo GC, Isichei C and Akanbi MO: Liver function test
abnormalities in Nigerian patients with human immunodeficiency
virus and hepatitis B virus co-infection. Int J STD AIDS.
24:461–467. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wang J, Guo L, Shi X, Pan W, Bai Y and Ai
H: Real-time elastography with a novel quantitative technology for
assessment of liver fibrosis in chronic hepatitis B. Eur J Radiol.
81:e31–e36. 2012. View Article : Google Scholar
|
|
3
|
Frieser M, Lindner A, Meyer S, et al:
Spectrum and bleeding complications of sonographically guided
interventions of the liver and pancreas. Ultraschall Med.
30:168–174. 2009.In German. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tatsumi C, Kudo M, Ueshima K, et al:
Noninvasive evaluation of hepatic fibrosis using serum fibrotic
markers, transient elastography (FibroScan®), and real-time tissue
elastography. Intervirology. 51(Suppl 1): 27–33. 2008. View Article : Google Scholar
|
|
5
|
Friedrich-Rust M, Ong MF, Martens S, et
al: Performance of transient elastography for the staging of liver
fibrosis: a meta-analysis. Gastroenterology. 134:960–974. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Satio H, Tada S, Nakamoto N, et al:
Efficacy of non-invasive elastometry on staging of hepatic
fibrosis. Hepatol Res. 29:97–103. 2004. View Article : Google Scholar
|
|
7
|
Friedrich-Rust M, Nierhoff J, Lupsor M, et
al: Performance of Acoustic Radiation Force Impulse imaging for the
staging of liver fibrosis: a pooled meta-analysis. J Viral Hepat.
19:e212–e219. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Boursier J, Isselin G, Fouchard-Hubert I,
et al: Acoustic radiation force impulse: a new ultrasonographic
technology for the widespread non-invasive diagnosis of liver
fibrosis. Eur J Gastroenterol Hepatol. 22:1074–1084. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Haque M, Robinson C, Owen D, Yoshida EM
and Harris A: Comparison of acoustic radiation force impulse
imaging (ARFI) to liver biopsy histologic scores in the evaluation
of chronic liver disease: a pilot study. Ann Hepatol. 9:289–293.
2010.PubMed/NCBI
|
|
10
|
Kim JE, Lee JY, Kim YJ, et al: Acoustic
radiation force impulse elastography for chronic liver disease:
comparison with ultrasoundbased scores of experienced radiologists,
Child-Pugh scores and liver function tests. Ultrasound Med Biol.
36:1637–1643. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kuroda H, Kakisaka K, Tatemichi Y, et al:
Non-invasive evaluation of liver fibrosis using acoustic radiation
force impulse imaging in chronic hepatitis patients with hepatitis
C virus infection. Hepatogastroenterology. 57:1203–1207. 2010.
|
|
12
|
Palmeri ML, Wang MH, Rouze NC, et al:
Non-invasive evaluation of hepatic fibrosis using acoustic
radiation forcebased shear stiffness in patients with nonalcoholic
fatty liver disease. J Hepatol. 55:666–672. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rizzo L, Calvaruso V, Cacopardo B, et al:
Comparison of transient elastography and acoustic radiation force
impulse for non-invasive staging of liver fibrosis in patients with
chronic hepatitis C. Am J Gastroenterol. 106:2112–2120. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fierbinteanu-Braticevici C, Andronescu D,
Usvat R, Cretoiu D, Baicus C and Marinoschi G: Acoustic radiation
force imaging sonoelastography for noninvasive staging of liver
fibrosis. World J Gastroenterol. 15:5525–5532. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Boursier J and Cales P: Combination of
fibrosis tests: sequential or synchronous? Hepatology. 50:656–657.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Castéra L, Vergniol J, Foucher J, et al:
Prospective comparison of transient elastography, Fibrotest, APRI,
and liver biopsy for the assessment of fibrosis in chronic
hepatitis C. Gastroenterology. 128:343–350. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Castéra L, LeBail B, Roudot-Thoraval F, et
al: Early detection in routine clinical practice of cirrhosis and
oesophageal varices in chronic hepatitis C: comparison of transient
elastography (FibroScan) with standard laboratory tests and
non-invasive scores. J Hepatol. 50:59–68. 2009. View Article : Google Scholar
|
|
18
|
Chinese Society of Hepatology and Chinese
Society of Infectious Diseases Chinese Medical Association: The
guideline of prevention and treatment for chronic hepatitis B (2010
version). Chin J Hepatology. 19:13–24. 2011.In Chinese.
|
|
19
|
Chinese Society of Hepatology and Chinese
Society of Infectious Diseases Chinese Medical Association: Chinese
program of prevention and cure for viral hepatitis. Chin J Intern
Med. 40:62–68. 2001.In Chinese.
|
|
20
|
Forns X, Ampurdanès S, Llovet JM, et al:
Identification of chronic hepatitis C patients without hepatic
fibrosis by a simple predictive model. Hepatology. 36:986–992.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Boursier J, de Ledinghen V, Zarski JP, et
al: Comparison of eight diagnostic algorithms for liver fibrosis in
hepatitis C: new algorithms are more precise and entirely
non-invasive. Hepatology. 55:58–67. 2012. View Article : Google Scholar
|
|
22
|
DeLong ER, DeLong DM and Clarke-Pearson
DL: Comparing the areas under two or more correlated receiver
operating characteristic curves: a nonparametric approach.
Biometrics. 44:837–845. 1988. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Joka D, Wahl K, Moeller S, et al:
Prospective biopsy-controlled evaluation of cell death biomarkers
for prediction of liver fibrosis and nonalcoholic steatohepatitis.
Hepatology. 55:455–464. 2012. View Article : Google Scholar
|
|
24
|
Verveer C, Zondervan PE, ten Kate FJ, et
al: Evaluation of transient elastography for fibrosisassessment
compared with large biopsies in chronic hepatitis B and C. Liver
Int. 32:622–628. 2012. View Article : Google Scholar
|
|
25
|
Myers RP, Pomier-Layrargues G, Kirsch R,
et al: Discordance in fibrosis staging between liver biopsy and
transient elastography using the fibroscan XL probe. J Hepatol.
56:564–570. 2012. View Article : Google Scholar
|
|
26
|
Gaia S, Carenzi S, Barilli AL, et al:
Reliability of transient elastography for the detection of fibrosis
in non-alcoholic fatty liver disease and chronic viral hepatitis. J
Hepatol. 54:64–71. 2011. View Article : Google Scholar
|
|
27
|
Harata M, Hashimoto S, Kawabe N, et al:
Liver stiffness in extrahepatic cholestasis correlates positively
with bilirubin and negatively with alanine aminotransferase.
Hepatol Res. 41:423–429. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Millonig G, Reimann FM, Friedrich S, et
al: Extrahepatic cholestasis increases liver stiffness (FibroScan)
irrespective of fibrosis. Hepatology. 48:1718–1723. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Boursier J, Vergniol J, Sawadogo A, et al:
The combination of a blood test and Fibroscan improves the
non-invasive diagnosis of liver fibrosis. Liver Int. 29:1507–1515.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Coco B, Oliveri F, Maina AM, et al:
Transient elastography: a new surrogate marker of liver fibrosis
influenced by major changes of transaminases. J Viral Hepat.
14:360–369. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Arena U, Vizzutti F, Corti G, et al: Acute
viral hepatitis increases liver stiffness values measured by
transient elastography. Hepatology. 47:380–384. 2008. View Article : Google Scholar
|
|
32
|
Scheuer PJ, Ashrafzdeh P, Sherlock S,
Brown D and Dusheiko GM: The pathology of hepatitis C. Hepatology.
15:567–571. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sandrin L, Fourquet B, Hasquenoph JM, et
al: Transient elastograhpy: a new noninvasive method for assessment
of hepatic fibrosis. Ultrasound Med Biol. 29:1705–1713. 2003.
View Article : Google Scholar : PubMed/NCBI
|