Introduction
Renal cell carcinoma (RCC) is the most frequent
primary malignancy in the adult kidney, accounting for 3% of all
adult tumors. Each year, >200,000 individuals are diagnosed with
this type of cancer all over the world and >100,000 succumb to
it (1,2). Clear-cell renal-cell carcinoma
(CCRCC) is the most common type of RCC, which accounts for ~80% of
all cases of RCC (3). CCRCC is
highly aggressive and resistant to conventional chemotherapy
(4). At present, the most
efficient treatment for CCRCC is surgical resection. In the case of
localized tumors, this therapy potentially cures affected patients.
However, most patients have developed distant metastases at the
time of diagnosis. Distant metastasis and local recurrence
frequently occurs in 1/3 of patients receiving radical surgical
treatment, among whom only 4–6% are sensitive to chemotherapy.
Therefore, in spite of the significant progress made in recent
years in improving surgical technology and chemotherapy, the
five-year survival rate of CCRCC remains low. Thus, it is urgently
required to elucidate the associated mechanism underlying
chemoresistance in CCRCC and provide a basis for developing novel
efficient approaches for CCRCC treatment.
Phosphatase and tensin homolog (PTEN) is a
dual-specificity phosphatase with protein phosphatase and lipid
phosphatase activity, and PTEN was the first phosphatase identified
as a tumor suppressor. It was reported that PTEN participates in
multiple signaling pathways and has important roles in regulating
cell growth, apoptosis, adhesion, migration and invasion (5). Increasing evidence demonstrated that
PTEN has a vital role in tumor development, and the absence or
mutation of PTEN was frequently discovered in various tumors,
including CCRCC (6–8). Mutation of the PTEN in mice leds to
high susceptibility to cancer (9).
Furthermore, tissue-specific deletion of PTEN in breast, skin and
prostate resulted in tumorigenesis (10,11).
PTEN mutations are rarely present in CCRCC; however, decreased PTEN
protein expression levels were detected, suggesting that PTEN is
involved in CCRCC development.
Akt is a member of the serine/threonine protein
kinase family, which has an important role in regulating cell
proliferation and apoptosis (12).
It has been demonstrated that Akt is activated in numerous
malignant tumors, including colorectal (13), ovarian (14), endometrial (15) and thyroid cancer (16) as well as CCRCC (17). Activated Akt inhibits cell
apoptosis and promotes cell proliferation through phosphorylating
downstream substrates, including B-cell lymphoma 2-associated death
promoter (18), caspase-9
(19,20), nuclear factor-κB kinases (21,22)
and HDM2 (23). PTEN is a specific
antagonist of phosphatidylinositol(3,4,5)-trisphosphate (PIP3), which blocks
phosphoinositide 3-kinase (PI3K)/Akt signaling through
dephosphorylating PIP3 to PIP2, leading to cell apoptosis (24). It has been demonstrated that
deficiency of PTEN resulted in activation of Akt, followed by
phosphorylation of its downstream substrates (25). HDM2 is an important substrate of
Akt, which functions as a negative regulator of tumor suppressor
p53. Akt promotes nuclear location of HDM2, which is crucial for
HDM2 to inhibit transcriptional activity of p53 and target p53 for
degradation (26). Thus, PTEN may
exert inhibitory effects on p53 through regulating Akt signaling,
which promotes the translocation of HDM2 (27).
PTEN is dysregulated in CCRCC (8,17)
and a deficiency of PTEN was correlated with poor prognosis in
patients with advanced CCRCC (28). All these data indicated that loss
of PTEN is important during CCRCC development, while it has
remained elusive whether it is involved in chemoresistance of
CCRCC. The present study assessed the expression of PTEN in CCRCC.
Furthermore, the effects of short hairpin (sh)RNA-mediated PTEN
knockdown in ACHN cells on Akt/HDM2 signaling, apoptosis induced by
etoposide, cell proliferation, the interaction between HDM2 and
p53, and the expression of p53 were evaluated. The present study
illustrated that low expression of PTEN in CCRCC contributes to
chemoresistance through activation of the Akt/HDM2 signaling
pathway.
Materials and methods
Cell lines and cell culture
ACHN cells were purchased from the Cell Bank of
Chinese Academy of Sciences (Shanghai, China) and cultured in RPMI
1640 supplemented with 10% fetal bovine serum (FBS), 100 U/ml
penicillin and 100 U/ml streptomycin. Cells were maintained in a
humidified incubator at 5% CO2 at 37°C (29).
Human CCRCC and paired normal renal
tissues
Five primary CCRCC and paired normal renal tissues
were collected, between January 2010 and July 2011, from the Second
Hospital, Jilin University (Changchun, China; 4 male and 1 female).
All cases were confirmed clinical and pathologically and staged in
accordance with the 2009 TNM staging classification system
(30). The samples were
snap-frozen in liquid nitrogen and stored at −80°C until further
analysis or fixed in 4% paraformaldehyde. Written informed consent
was obtained from all the patients or their guardians, and the
protocol was approved by the Ethics Committee of the Second
Hospital affiliated to Jilin University (Changchun, China).
Reagents and antibodies
Antibody against phosphorylated (p)-HDM2 (Ser166;
1:1,000, Rabbit polyclonal antibody, cat. no. 3521) was purchased
from Cell Signaling Technology (Danvers, MA, USA). Antibodies
against total (T)-Akt (1:1,000, Rabbit polyclonal; cat. no.
ab8806), p-AKT (Ser473; 1:1000, Rabbit Polyclonal; cat. no.
ab66138), HDM2 (1:1,000, Mouse monoclonal; cat. no. ab10567), PTEN
(1:1,000, Rabbit polyclonal, cat. no. ab31392) and p53 (1:1,000,
Rabbit monoclonal; cat. no. ab179477) were purchased from Abcam
(Cambridge, UK); poly (ADP ribose) polymerase (PARP cleaved), p53
upregulated modulator of apoptosis (PUMA, 1:1,000; mouse
monoclonal; cat. no. sc-374223), GAPDH (1:1,000; mouse monoclonal;
cat. no. sc-365062), rabbit anti-mouse immunoglobulin (Ig)
G-horseradish peroxidase (HRP; 1:2,000; cat. no. sc-358922) and
mouse anti-rabbit IgG-HRP (cat. no. sc-2357) were obtained from
Santa Cruz Biotechnology, Inc. (Dallas, TX, USA). Protein A/G-beads
and the enhanced chemiluminescence (ECL) immunoblotting detection
reagent were purchased from Santa Cruz Biotechnology, Inc.;
Etoposide was from Sigma-Aldrich (St Louis, MO, USA); Lipofectamine
2000 and TRIzol were purchased from Invitrogen Life Technologies
(Carlsbad, CA, USA); Moloney murine leukemia virus (M-MLV) reverse
transcriptase was from Promega (Madison, WI, USA). SYBR polymerase
chain reaction (PCR) premixture was from Applied Biosystems (Foster
City, CA, USA). Cell Counting Kit-8 was from Dojindo Laboratories
(Kumamoto, Japan). pSUPERIOR.puro plasmid was obtained from
Oligoengine (Seattle, WA, USA).
Plasmid construction and
transfection
The PTEN (GenBank accession number, NM_000314;
AAGACCATAACCCACCACAGC) shRNA target sequences were designed by
GeneChem Company (Montreal, Quebec, Canada) (forward,
5′-GACCAUAACCCACCACAGCTT-3′ and reverse,
5′-GCUGUGGUGGGUUAUGGUCTT-3′). The oligonucleotide-annealed products
were subcloned into pSUPERIOR.puro (Oligoengine) between the
BglII and HindIII sites.
For transfection, ACHN cells were seeded onto a
96-well plate (5×103 cells/well) and following 24 h,
cells were transfected with the indicated shRNA using Lipofectamine
2000 according the manufacturer’s instructions.
Quantitative (q)PCR analysis
The total mRNA of tissues and ACHN cells was
prepared using TRIzol according to the manufacturer’s instructions.
Reverse transcription was performed with M-MLV reverse
transcription kit. qPCR assays were performed with iTaq Fast SYBR
Green Supermix (Bio-Rad) on a 7500 Fast Real-Time PCR System
(Applied Biosystems, Foster City, CA, USA). The primers for qPCR
were as follows: PTEN 5′-GTTCAGTGGCGGAACTTGCAATCCT-3′ (forward) and
5′-TCCCGTCGTGTGGGTCCTGA-3′ (reverse). Cycling conditions were as
follows: 40 cycles of 95°C for 15 sec; 95°C for 20 sec and 60°C for
1 min. ΔΔCT method was used for the quantification of
the products.
Western blot analysis
Tissues or cells were collected and homogenized in
radioimmunoprecipitation (RIPA) lysis buffer [50 mM Tris-HCl (PH
7.4), 150 mM NaCl, 1 mM phenyl methyl sulphonyl fluoride (PMSF;
Beyotime Institute of Biotechnology, Shanghai, China), 1% Triton
X-100 (Beyotime Institute of Biotechnology), 0.1% SDS (Amresco, OH,
USA), 1% sodium deoxycholic acid (Amresco) and 1X protease
inhibitor cocktail (Sigma-Aldrich)]. Then the homogenate was
centrifuged at 7,300 × g for 10 min and the supernatant was
collected. The protein concentration was measured using the
bicinchoninic acid (BCA) protein assay kit (Beyotime, Shanghai,
China). 40 µg protein was subjected to 12% SDS-PAGE
(Beyotime Institute of Biotechnology) and then electrophoretically
transferred to a polyvinylidene difluoride (PVDF) membrane
(Millipore Corp., Billerica, MA, USA). Following blocking with 5%
skimmed milk (Amresco) for 1 h at room temperature, the membrane
was incubated with the primary antibody for 1 h at room
temperature. The membrane was washed with Tris-buffered saline
containing Tween 20 (TBST; Beyotime Institue of Biotechnology)
three times for 5 min each time. Then the membrane was incubated
with HRP-conjugated secondary antibody for 1 h at room temperature.
Following three washes with TBST, the positive signal was
visualized using ECL Advanced Solution (Pierce, Thermo Fisher
Scientific, Waltham, MA, USA).
Immunoprecipitation
A total of 10 µl protein A-sepharose slurry
(Santa Cruz Biotechnology, Inc.) was added to the lysate prepared
as above. The mixture was agitated at 4°C for 30 min and then
centrifuged at 7,200 × g for 5 min. The supernatant was collected
and transferred to a fresh Eppendorf tube. Subsequently, 2
µg of the indicated antibodies and 20 µl of the
protein A-sepharose slurry were added to the pre-cleared lysate,
and incubation was performed overnight at 4°C with continuous
agitation. The immunocomplexes were washed three times with
pre-cooled RIPA lysis buffer and precipitated proteins were eluted
by boiling in 20–40 µl 1X SDS-PAGE loading buffer (Beyotime
Institute of Biotechnology). The samples were then subjected to
western blot analysis.
Immunohistochemistry
Tissues were fixed with parafor-maldehyde (4%;
Sigma-Aldrich), then embedded in paraffin and sectioned. Sections
were deparaffinized in xylol (Beyotime Institute of Biotechnology)
and rehydrated in a graded ethanol series (China National
Medicines, Shanghai, China). Following antigen retrieval by
microwave heating (600 W; 15 min; P70F23P-G5; Galanz, Guangdong,
China), the sections were incubated in non-immune serum (Santa Cruz
Biotechnology, Inc.) for 30–60 min at room temperature and then
blotted with the indicated primary antibody against p-Akt, p-HDM2
(Ser166), p53 or PTEN, overnight at 4°C. The next day, the sections
were incubated in rabbit HRP-conjugated secondary antibody for 1 h
at room temperature.
Finally, the sections were visualized with
3,3′-diamino-benzidine hydrochloride (Sigma-Aldrich) and
counterstained with hematoxylin (Beyotime Institute of
Biotechnology).
Cell cycle analysis
Cells were detached with 0.25% trypsin (Beyotime
Institute of Biotechnology), collected, washed with ice-cold
phosphate-buffered saline (PBS; Beyotime Institute of
Biotechnology) and then fixed in 70% ice-cold ethanol for 1 h. The
cell suspension was centrifuged for 5 min at 1,000 rpm. The
supernatant was removed and cells were re-suspended in PBS.
Subsequently, 50 µg/ml RNase A (Promega) and 25 µg/ml
propidium iodide (PI; Sigma-Aldrich) were added and kept at 37°C
for 30 min. The DNA contents of >10,000 cells were detected
using a FACSCalibur (BD Biosciences, San Jose, CA, USA).
Quantitative analysis of the cell cycle distribution was performed
using WinMDI 2.9 (Dr Joseph Trotter, The Scripps Institute, La
Jolla, CA, USA).
CCK8 assay
24 h prior to transfection, 2.5×103 cells
were seeded onto 96-well cell culture plates. Transfection was
performed using Lipofectamine 2000 according to the manufacturer’s
instructions. 24 h post-transfection, 30 µM etoposide or
mock were added. Following a further 24 h incubation, 10 µl
CCK-8 solution was added to each well of the plate, followed by 1 h
incubation at 37°C. The optical density (OD) was then measured at
450 nm using a microplate reader (MK3; Thermo Fisher Scientific).
The cell inhibitory rate was calculated according to the following
equation:
[1−(ODexperiment−ODblank)/(ODcontrol−ODblank)]
×100%. All experiments were performed in triplicate and repeated
three independent times.
Statistical analysis
Values are expressed as the mean + standard error.
Student’s t-test was used for statistical analysis of the data to
determine the differences between the groups using SPSS 11.5 for
Windows software (SPSS, Inc., Chicago, IL, USA). P<0.05 was
considered to indicate a statistically significant difference
between values.
Results
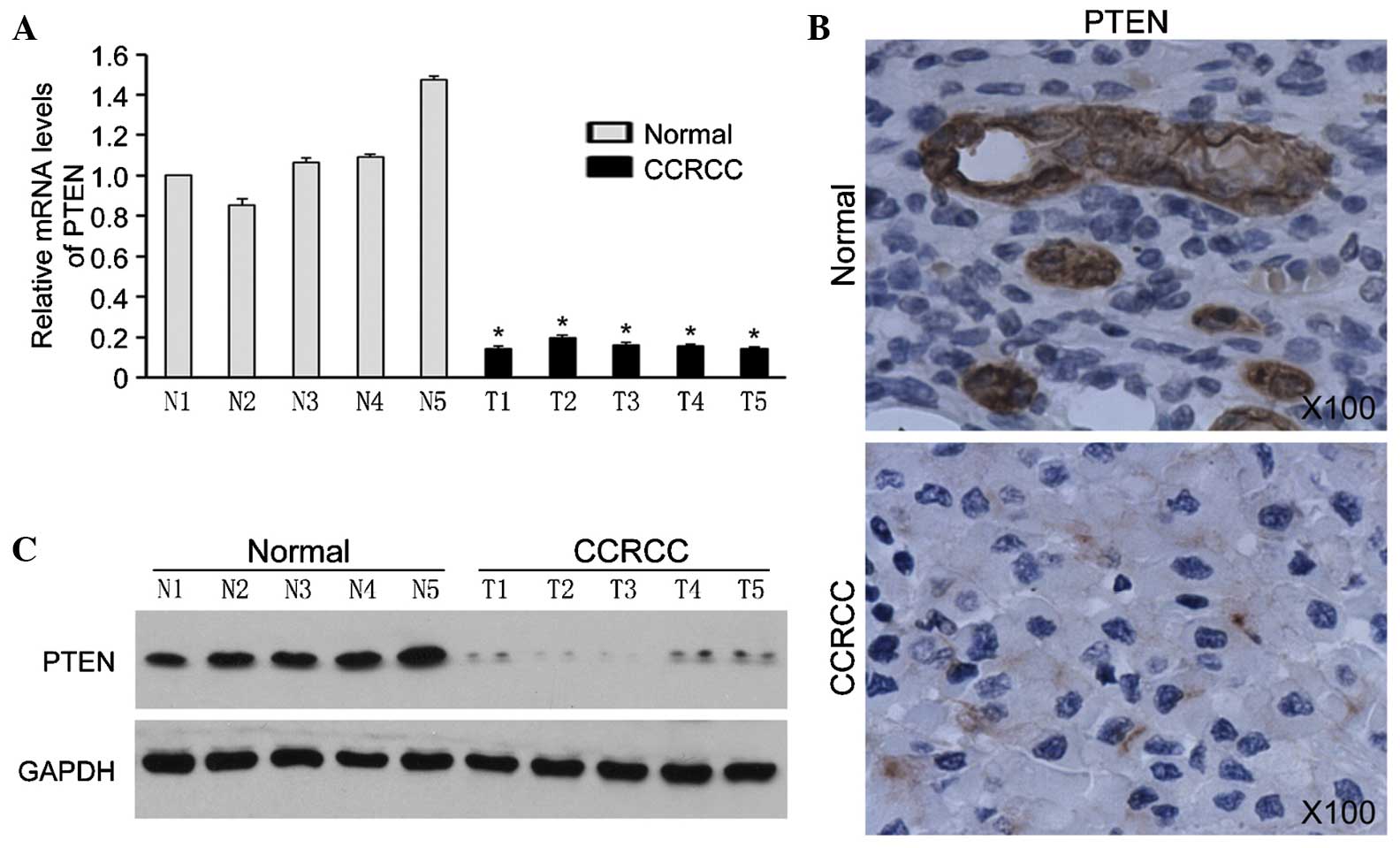
PTEN is overexpressed in CCRCC
tissues
In the present study, the expression of PTEN was
analyzed in five pairs of CCRCC tissues and the corresponding
normal renal tissues. qPCR analysis showed that PTEN mRNA was
decreased in CCRCC tissues (Fig.
1A). In accordance with the qPCR results, western blot analysis
and immunohistochemistry showed that the expression levels of PTEN
protein were obviously decreased in CCRCC tissues (Fig. 1B and C). These results suggested
that loss of PTEN is correlated with CCRCC development.
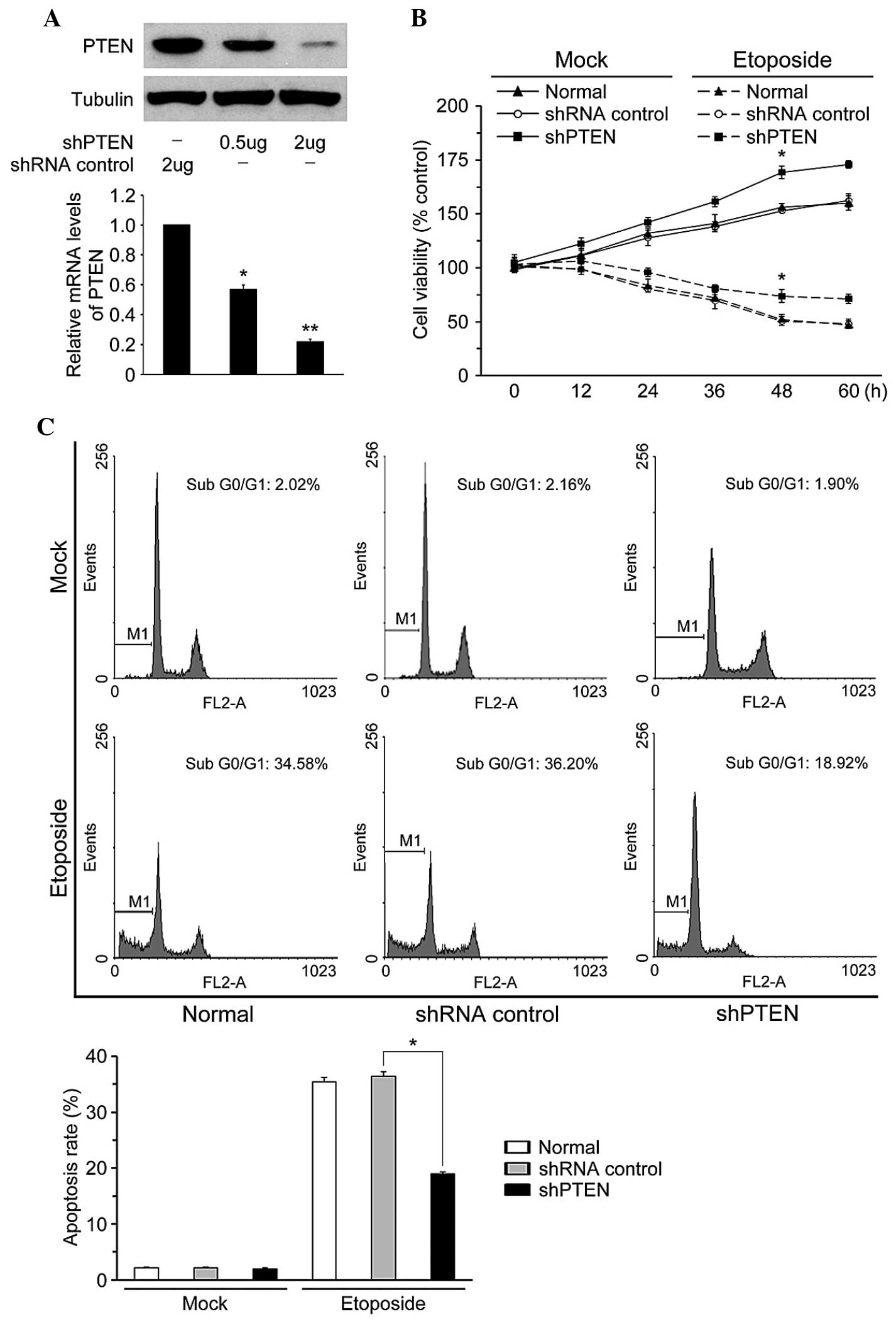
PTEN knockdown inhibits ACHN cell
apoptosis induced by etoposide
To identify whether PTEN has a role in the
sensitivity of CCRCC to chemotherapy drugs, PTEN was silenced in
the CCRCC cell line ACHN using shRNA. As shown in Fig. 2A, following transfection with PTEN
shRNA, PTEN was effectively downregulated in ACHN cells. Results of
the CCK-8 assay showed that knockdown of PTEN promoted
proliferation of ACHN cells with or without treatment with
etoposide (Fig. 2B). Cell cycle
analysis revealed that treatment with etoposide induced cell cycle
arrest and apoptosis in ACHN cells, while PTEN knockdown resulted
in a decreased sub G0/G1 phase population in the presence or
absence of etoposide (Fig. 3C).
These results demonstrated that loss of PTEN in ACHN cells
inhibited etoposide-induced cell apoptosis and promoted cell
proliferation.
 | Figure 3Effect of etoposide on the expression
of different endogenous proteins of the Akt pathway in ACHN cells.
(A) Western blot analysis of cleaved-PARP, PUMA, p-AKT (Ser473),
T-AKT, p-HDM2, HDM2 and p53 in ACHN cells with indicated treatment.
GAPDH was loaded as the internal control. (B)
Co-immunoprecipitation of HDM2 in normal cells or clear-cell renal
carcinoma cells were precipitated for HDM2 and immunoblotted for
p53, p-HDM2 and HDM2 in ACHN cells with indicated treatment. shRNA,
small hairpin RNA; PTEN, phosphatase and tensin homolog; p,
phosphorylated; T, total; PUMA, p53 upregulated modulator of
apoptosis; IgG, immunoglobulin G; PARP, poly(ADP ribose)
polymerase; I P, immunoprecipitation. |
PTEN inhibition leads to activation of
AKT/HDM2 and downregulation of p53
PTEN is a specific antagonist of PIP3, which blocks
PI3K/Akt signaling through dephosphorylation of PIP3 (24). Increasing evidence showed that loss
of PTEN resulted in abnormal activity of Akt (31). In the present study,
etoposide-treatment of ACHN cells increased phosphorylation of Akt
(Fig. 3A); furthermore, HDM2, an
important substrate of Akt, was significantly inhibited. p53, PUMA
and cleaved PARP were obviously induced. Knockdown of PTEN in ACHN
greatly reversed the inhibition effect of etoposide on Akt and HDM2
activation. The etoposide-induced upregulation of p53, PUMA and
cleaved PARP were also reduced following PTEN knockdown. These
results suggested that PTEN knockdown activated the Akt/HDM2
signaling pathway and blocked p53-dependent cell apoptosis
(Fig. 3A).
HDM2 is a negative regulator of tumor suppressor
p53, which inhibits the transcriptional activity of p53 and targets
p53 for degradation (26).
Immunoprecipitation results showed that knockdown of PTEN enhanced
the interaction between p53 and HDM2 (Fig. 3B). The results further demonstrate
that loss of PTEN in ACHN cells activated the Akt/HDM2 signaling
pathway and promoted the interaction between p53 and HDM2, which
led to degradation of p53 and resulted in block of apoptosis
induced by etoposide.
Activation of AKT/HDM2 leads to degration
of p53 and enhances cell proliferation
To further verify that PTEN deficiency is critical
in chemoresistance of CCRCC, the Akt/HDM2 signaling pathway in
CCRCC tissues was analyzed. Western blot analysis showed that HDM2,
p-HDM2 (ser166) and p-AKT were upregulated in CCRCC tissues
alongside low p53 expression (Fig.
4A). The immunohistochemistry results were in accordance with
the western blot results (Fig.
4B). Furthermore, immunoprecipitation also revealed that
interaction between p53 and HDM2 was increased in CCRCC tissues.
These data confirmed that loss of PTEN in CCRCC is attributed to
activation of Akt/HDM2 and enhancement of the interaction between
p53 and HDM2, eventually resulting in a reduction of p53.
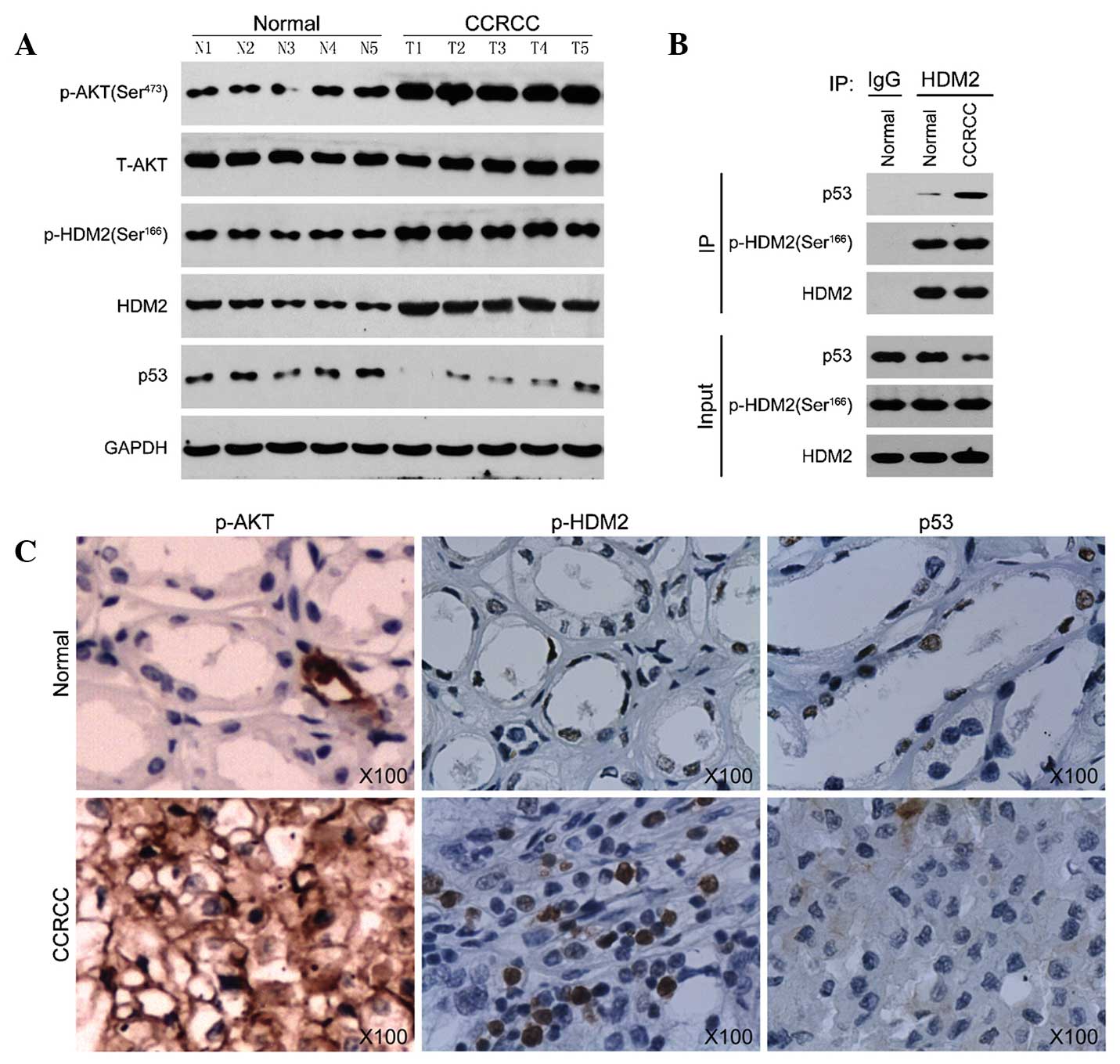 | Figure 4HDM2 interacts with p53 in CCRCC. (A)
Protein levels of p-AKT (Ser473), T-AKT, p-HDM2, HDM2 and p53 in
non-tumor kidney tissues (normal, N1–N5) and CCRCC (T1–T5). GAPDH
was used as the internal control. (B) Co-immunoprecipitation of
HDM2 in normal cells or CRCC were precipitated for HDM2 and
immunoblotted for p53, p-HDM2 and HDM2. (C) Representative
micrographs of immunohistochemical staining for p-AKT (Ser473),
p-HDM2 and p53 in non-tumor kidney tissues and CCRCC
(magnification, x100). CCRCC, clear-cell renal cell carcinoma; p,
phosphorylated; T, total; IgG, immunoglobulin G; I P,
immunoprecipitation. |
Discussion
In the present study, it was found that PTEN was
depressed in CCRCC, which was involved in the resistance of CCRCC
to chemotherapy. Further investigation revealed that loss of PTEN
activated Akt/HDM2 and promoted degradation of p53, which
attributes to resistance of CCRCC cell apoptosis induced by
etoposide.
PTEN is a dual and protein phosphatase, and it has
been demonstrated that loss of PTEN is closely associated with
tumorigenesis. In the present study, it was also found that the
expression of PTEN protein and mRNA was downregulated in CCRCC,
which was in accordance with the results of previous studies
(8,17). The present study suggested that
loss of PTEN has an important role during CCRCC development.
Etoposide is a commonly used anti-tumor drug, which induces
apoptosis of numerous types of tumor cell. Treatment of ACHN with
etoposide enhanced cell apoptosis and inhibited cell proliferation.
Knockdown of PTEN in ACHN cells using PTEN shRNA increased cell
proliferation, and the apoptotic rate decreased from 34.58 to
18.92%. These results demonstrated that deficiency of PTEN is
associated with chemoresistance of CCRCC.
Tumor suppressor gene p53 has an important role in
regulating cell cycle and cell apoptosis and is frequently mutated
or deleted in various tumors. The mechanism of action of most
chemotherapy drugs is the induction of p53-mediated apoptosis.
Therefore, tumors harboring p53 mutations are associated with
chemoresistance and poor prognosis (32–34).
While p53 mutations are seldom detected in CCRCC, these tumors are
frequently resistant to chemotherapy (35–37).
The present study found that p53 and PUMA were overexpressed in
etoposide-treated ACHN cells, and the percentage of apoptotic cells
significantly increased, which suggested that etoposide induced
apoptosis of ACHN cells in a p53-dependent manner.
The PI3K/Akt signaling pathway has a key role in the
development of numerous tumor types, including CCRCC (17). PTEN is an antagonist of PI3K, which
dephosphorylates PIP3 and blocks signaling downstream of activated
PI3K (24). HDM2 is a substrate of
PI3K/Akt and also a ubiquitin ligase of p53. Akt phosphorylates
serines 166 and 186 on HDM2, which induces translocation of HDM2
from the cytoplasm into the nucleus where it binds to p53 and
promotes p53 degradation (38–40).
To elucidate the mechanism underlying the role of PTEN deficiency
in CCRCC resistance to chemotherapy, the present study examined the
PI3K/Akt signaling pathway in etoposide-treated ACHN cells. The
results showed that etoposide was able to inhibit the activation of
Akt and HDM2, and the expression of p53 and PUMA was also
depressed. Furthermore, an immunoprecipitation assay showed that
the interaction between HDM2 and p53 was reduced. From the above
data it was deduced that in CCRCC, loss of PTEN may activate the
Akt/HDM2 interaction, leading to suppression of p53 and hence
blocking apoptosis induced by chemotherapy. This was confirmed by
knockdown of PTEN in ACHN cells, as decreased expression of PTEN in
ACHN cells markedly reversed the etoposide-mediated inhibition of
Akt/HDM2 and led to downregulation of p53.
Finally and importantly, the present study examined
Akt/HDM2 signaling in CCRCC tissues and also found that HDM2,
p-HDM2 (ser166) and p-Akt were increased, accompanied with
depressed p53. Furthermore, the amount of p53 co-precipitated with
HDM2 in CCRCC was obviously increased. These results further
demonstrated that CCRCC resistance to chemotherapy caused by PTEN
deficiency was associated with the Akt/HDM2 signaling pathway.
In conclusion, the present study illustrated that
loss of PTEN in CCRCC led to activation of the Akt/HMD2
interaction, inhibition of p53 and protection of CCRCC cells from
etoposide-induced apoptosis. These results provided a mechanistic
explanation of why CCRCC cells with PTEN deficiency are resistant
to chemotherapy and support a rationale for combining conventional
chemotherapy drugs, such as etoposide, with modalities that
activate p53 for the efficient treatment of CCRCC.
References
|
1
|
Jemal A, Murray T, Ward E, et al: Cancer
statistics, 2005. CA Cancer J Clin. 55:10–30. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zbar B, Klausner R and Linehan WM:
Studying cancer families to identify kidney cancer genes. Annu Rev
Med. 54:217–233. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cohen HT and McGovern FJ: Renal-cell
carcinoma. N Engl J Med. 353:2477–2490. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Myers MP, Pass I, Batty IH, et al: The
lipid phosphatase activity of PTEN is critical for its tumor
supressor function. Proc Natl Acad Sci USA. 95:13513–13518. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li J, Yen C, Liaw D, et al: PTEN, a
putative protein tyrosine phosphatase gene mutated in human brain,
breast and prostate cancer. Science. 275:1943–1947. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rizvi MM, Alam MS, Ali A, Mehdi SJ, Batra
S and Mandal AK: Aberrant promoter methylation and inactivation of
PTEN gene in cervical carcinoma from Indian population. J Cancer
Res Clin Oncol. 137:1255–1262. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brenner W, Färber G, Herget T, Lehr HA,
Hengstler JG and Thüroff JW: Loss of tumor suppressor protein PTEN
during renal carcinogenesis. Int J Cancer. 99:53–57. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Suzuki A, de la Pompa JL, Stambolic V, et
al: High cancer susceptibility and embryonic lethality associated
with mutation of the PTEN tumor suppressor gene in mice. Curr Biol.
8:1169–1178. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Backman SA, Ghazarian D, So K, et al:
Early onset of neoplasia in the prostate and skin of mice with
tissue-specific deletion of Pten. Proc Natl Acad Sci USA.
101:1725–1730. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Li G, Robinson GW, Lesche R, et al:
Conditional loss of PTEN leads to precocious development and
neoplasia in the mammary gland. Development. 129:4159–4170.
2002.PubMed/NCBI
|
|
12
|
Franke TF, Kaplan DR and Cantley LC: PI3K:
downstream AKTion blocks apoptosis. Cell. 88:435–437. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Itoh N, Semba S, Ito M, Takeda H, Kawata S
and Yamakawa M: Phosphorylation of Akt/PKB is required for
suppression of cancer cell apoptosis and tumor progression in human
colorectal carcinoma. Cancer. 94:3127–3134. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kurose K, Zhou XP, Araki T, Cannistra SA,
Maher ER and Eng C: Frequent loss of PTEN expression is linked to
elevated phosphorylated Akt levels, but not associated with p27 and
cyclin D1 expression, in primary epithelial ovarian carcinomas. Am
J Pathol. 158:2097–2106. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kanamori Y, Kigawa J, Itamochi H, et al:
Correlation between loss of PTEN expression and Akt phosphorylation
in endometrial carcinoma. Clin Cancer Res. 7:892–895.
2001.PubMed/NCBI
|
|
16
|
Ringel MD, Hayre N, Saito J, et al:
Overexpression and overactivation of Akt in thyroid carcinoma.
Cancer Res. 61:6105–6111. 2001.PubMed/NCBI
|
|
17
|
Hager M, Haufe H, Kemmerling R, et al:
Increased activated Akt expression in renal cell carcinomas and
prognosis. J Cell Mol Med. 13:2181–2188. 2009. View Article : Google Scholar
|
|
18
|
Datta SR, Dudek H, Tao X, et al: Akt
phosphorylation of BAD couples survival signals to the
cell-intrinsic death machinery. Cell. 91:231–241. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
del Peso L, González-García M, Page C,
Herrera R and Nuñez G: Interleukin-3-induced phosphorylation of BAD
through the protein kinase Akt. Science. 278:687–689. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cardone MH, Roy N, Stennicke HR, et al:
Regulation of cell death protease caspase-9 by phosphorylation.
Science. 282:1318–1321. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ozes ON, Mayo LD, Gustin JA, Pfeffer SR,
Pfeffer LM and Donner DB: NF-kappaB activation by tumour necrosis
factor requires the Akt serine-threonine kinase. Nature. 401:82–85.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Romashkova JA and Makarov SS: NF-kappaB is
a target of AKT in anti-apoptotic PDGF signalling. Nature.
401:86–90. 1999. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ashcroft M, Ludwig RL, Woods DB, et al:
Phosphorylation of HDM2 by Akt. Oncogene. 21:1955–1962. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Waite KA and Eng C: Protean PTEN: form and
function. Am J Hum Genet. 70:829–844. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cantley LC and Neel BG: New insights into
tumor suppression: PTEN suppresses tumor formation by restraining
the phosphoinositide 3-kinase/AKT pathway. Proc Natl Acad Sci USA.
96:4240–4245. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mayo LD and Donner DB: A
phosphatidylinositol 3-kinase/Akt pathway promotes translocation of
Mdm2 from the cytoplasm to the nucleus. Proc Natl Acad Sci USA.
98:11598–11603. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mayo LD, Dixon JE, Durden DL, Tonks NK and
Donner DB: PTEN protects p53 from Mdm2 and sensitizes cancer cells
to chemotherapy. J Biol Chem. 277:5484–5489. 2002. View Article : Google Scholar
|
|
28
|
Velickovic M, Delahunt B, McIver B and
Grebe SK: Intragenic PTEN/MMAC1 loss of heterozygosity in
conventional (clear-cell) renal cell carcinoma is associated with
poor patient prognosis. Mod Pathol. 15:479–485. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hirata H, Hinoda Y, Ueno K, Majid S, Saini
S and Dahiya R: Role of secreted frizzled-related protein 3 in
human renal cell carcinoma. Cancer Res. 70:1896–1905. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Martinez-Salamanca JI, Huang WC, Millan I,
Bertini R, Bianco FJ, Carballido JA, et al: Prognostic impact of
the 2009 UICC/AJCC TNM staging system for renal cell carcinoma with
venous extension. Eur Urol. 59:120–127. 2011. View Article : Google Scholar
|
|
31
|
Georgescu MM: PTEN tumor suppressor
network in PI3K-Akt pathway control. Genes Cancer. 1:1170–1177.
2010. View Article : Google Scholar
|
|
32
|
Johnstone RW, Ruefli AA and Lowe SW:
Apoptosis: a link between cancer genetics and chemotherapy. Cell.
108:153–164. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ko LJ and Prives C: p53: puzzle and
paradigm. Genes Dev. 10:1054–1072. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wallace-Brodeur RR and Lowe SW: Clinical
implications of p53 mutations. Cell Mol Life Sci. 55:64–75. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Tomasino RM, Morello V, Tralongo V, et al:
p53 expression in human renal cell carcinoma: an
immunohistochemical study and a literature outline of the
cytogenetic characterization. Pathologica. 86:227–233.
1994.PubMed/NCBI
|
|
36
|
Vasavada SP, Novick AC and Williams BR:
P53, bcl-2 and Bax expression in renal cell carcinoma. Urology.
51:1057–1061. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Roberts AM, Watson IR, Evans AJ, Foster
DA, Irwin MS and Ohh M: Suppression of hypoxia-inducible factor
2alpha restores p53 activity via Hdm2 and reverses chemoresistance
of renal carcinoma cells. Cancer Res. 69:9056–9064. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ogawara Y, Kishishita S, Obata T, et al:
Akt enhances Mdm2-mediated ubiquitination and degradation of p53. J
Biol Chem. 277:21843–21850. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhou BP, Liao Y, Xia W, Zou Y, Spohn B and
Hung MC: HER-2/neu induces p53 ubiquitination via Akt-mediated MDM2
phosphorylation. Nat Cell Biol. 3:973–982. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Mayo LD and Donner DB: The PTEN, Mdm2, p53
tumor suppressor-oncoprotein network. Trends Biochem Sci.
27:462–467. 2002. View Article : Google Scholar : PubMed/NCBI
|