Introduction
Bladder urothelial carcinoma is the most common
urological malignancy, accounting for 3.2% of all neoplastic
malignancies and is the fifth most common cancer in males,
according to 2008 cancer statistics (1). Of all malignancies of the male
genitourinary system, >90% of cases are urothelial carcinoma,
which present the highest rates of morbidity and mortality. The
recurrence rate is low following surgery without other treatments,
and in 10–20% of cases, bladder transitional cell carcinoma (BTCC)
eventually develops into muscle invasive bladder cancer, for which
the five-year survival rate is <50% (2–6).
Intravesical therapy has been demonstrated to be an effective
treatment to reduce the recurrence and progression of bladder
cancer, and intravesical administration of Bacillus
Calmette-Guérin (BCG) vaccine is able to produce an improved
therapeutic effect in high-risk, non-invasive bladder cancer
(7).
Brain-specific angiogenesis inhibitor-1 (BAI-1) was
initially described in 1997, and there have since been a number of
studies on its expression in different types of cancer. Nam et
al (8) examined 20 cases of
brain tumor, 2 samples of normal brain tissue, 5 cases of benign
brain tumor and 26 patients with malignant glioma, and identified
that BAI-1 was expressed in all normal brain tissue, benign tumor
tissues and 9 cases of malignant glioma, while no expression was
observed in the other types of tumor. Their results indicated that
the tumors that expressed BAI-1 were relatively sensitive to
treatment, and had good prognoses, while patients lacking BAI-1
expression had poor prognoses. Yoshida et al (9) studied 62 cases of colorectal cancer
and 40 samples of normal extraneoplastic colon mucosa, and observed
that the levels of thrombospondin 2 and angiopoietin-2 expression
were significantly higher, with reduced BAI-1 expression levels in
the colorectal cancer samples compared with those in the control
samples. Hatanaka et al (10) analyzed the BAI-1 gene expression in
48 cases of lung adenocarcinoma and immunohistochemically assessed
the vascular density in the tumor samples using an anti-CD34
monoclonal antibody. BAI-1 gene expression was observed in 38/48
(79.2%) cases of lung cancer. The density of tumor blood vessels in
the BAI-1 positive tumors (19.3±4.4/µm2,
1.7±0.6%) was significantly reduced compared with that in the
BAI-1-negative tumors (75.5±42.7/µm2, 5.5±1.5%),
indicating that BAI-1 may serve a function in the inhibition of
interstitial vascularization in lung adenocarcinoma. Thus, it was
hypothesized that BAI-1 may be useful as an indicator of prognosis
in urinary disease. It was therefore theorized in the present study
that BAI-1 may also act as an indicator of prognosis in bladder
urothelial carcinoma, and that BAI-1 is a potential novel target
for the treatment of these tumors. The expression of
BAI-1-associated proteins in bladder urothelial carcinoma was
examined in the present study, in order to provide a theoretical
basis for the application of BAI-1 in the treatment of bladder
cancer.
Patients and methods
Patients
Tissue blocks from 131 patients with BTCC,
pathologically confirmed between 2009 and 2011 in the Department of
Urology, Second Hospital of Tianjin Medical University (Tianjin,
China), were randomly selected, and all cases were diagnosed by
experienced pathologists. Staging of bladder cancer was performed
using the tumor, nodes and metastasis (TNM) classification of
malignant tumors (UICC) (11). The
mean age of participants was 64, with a range of 27–89 years; 88
cases were male and 43 cases were female. A total of 57 cases
(43.5%) were TNM stage T1, 50 cases (38.2%) were T2, and 24 cases
(18.3%) were T3-4. In terms of grading, a total of 90 cases (68.7%)
were classified as stages G1-2 (well/moderately differentiated) and
41 cases (31.3%) were stage G3 (poorly differentiated). In
addition, 28 cases with normal bladder mucosa tissues were selected
as controls. The study was approved by the ethics committee of the
Second Hospital of Tianjin Medical University. Written informed
consent was obtained from the patients.
Specimens
Fresh clinical BTCC specimens from 21 cases were
resected and divided into two groups according to UICC TNM staging:
8 Patients were staged as T1 and 13 patients presented with BTCC at
the advanced stages of T2-4. Normal bladder epithelial tissues from
9 cases were obtained by suprapubic prostatic hyperplasia
enucleation. The concentration of the protein extracted from the
tissue samples, which were frozen in liquid nitrogen, was detected,
and the BAI-1 protein content in the tissues was measured.
Immunohistochemistry (IHC)
The following primary antibodies were purchased from
Abcam (Cambridge, UK): Monoclonal mouse anti-human mutant p53
antibody (cat. no. ab179477; Abcam), polyclonal rabbit anti-human
BAI-1 (cat. no. ab135907; Abcam), polyclonal rabbit anti-human CD34
antibody (cat. no. ab150060, Abcam) and polyclonal rabbit
anti-human vascular endothelial growth factor (VEGF) antibody (cat.
no. ab46154; Abcam). Antibodies were diluted at a 1:100 ratio. PBS
was used for the negative control group, and bladder cancer tissue
known to be positive was used as a positive control. Polink-2
plus® polymer HRP detection system for rabbit primary
antibodies (two steps) and a 3,3′-diaminobenzidine kit were
purchased from Beijing Zhongshan Golden Bridge Biotechnology, Co.
Ltd. (Beijing, China) and were used according to the manufacturer's
instructions. Tumor cells in which the cytoplasm, nucleus or
membrane appeared brown were considered positive. Six
high-magnification fields of each slice were randomly selected
(magnification, ×400), and the average percentages of positive
cells were calculated. The following scoring method was used: 25%,
0 points; 26–50%, 1 point; 51–75%, 2 points; and >75%, 3 points.
Staining intensity was categorized as follows: Uncolored, 0 points;
pale yellow, 1 point; yellow or brown, 2 points; and brown, 3
points. According to the final points, 0–1 was (−), 2–3 points was
weakly positive (+), 4–5 points was positive (++) and >5 was
strongly positive (+++). Specimens which scored (+) to (+++) were
considered positive. The microvessel density (MVD) counting method
was as follows: According to the Tanigawa criterion (12), the high MVD areas were filtered out
initially under low magnification (10×10), then the microvascular
number of the five horizons under the ×400 field was selected and
the average was considered to be the number of tumor microvessels.
Ambiguously stained cells were not included in the results and
single brown endothelial cells or cell colonies were included in
the vessel count, while the blood vessels with thicker vasculature
and the lumen area with a red cell number >8 were not counted.
The Olympus BX51 Microscope system (Olympus Corporation, Tokyo,
Japan) was used to obtain images of the IHC staining
(magnification, ×400. Six horizons of each slide were blindly and
randomly selected and their images were captured, which were
quantitatively analyzed with Image-Pro Plus image analysis
software, version 4.1 (Media Cybernetics, Inc., Rockville, MD,
USA). The total optical density (OD) value of the brown staining on
each slide in each field was analyzed and calculated, and the
average OD value of each field area was calculated prior to
statistical analysis.
Western blot analysis
A total of 100 mg of the respective tissue block was
placed in a mortar and cut into pieces with clean scissors. A total
of 400 µl RIPA lysis buffer system (Santa Cruz
Biotechnology, Inc., Dallas, TX, USA) was added to the mortar prior
to grinding the tissue, which was then placed on ice. The process
of grinding the tissue and placing it on ice was repeated several
times to fully homogenize it. The protein concentration was
quantified with a Dc protein assay reagent (Bio-Rad, Hercules, CA,
USA). Equal quantities of protein were loaded and separated by 10%
SDS PAGE (for HAMP, 18%) and then transferred onto polyvinylidene
difluoride membranes (Bio-Rad). The membranes were incubated
overnight with the appropriate primary antibodies. Bound antibodies
were then visualized using alkaline phosphatase-conjugated
secondary antibodies. Quantitative analysis was performed using NIH
Image J version 1.32j software (National Institutes of Health,
Bethesda, MD, USA).
Statistical analysis
The χ2 test and Spearman's correlation
analysis were used to analyze the associations between the
clinicopathological parameters and IHC results. All data were
analyzed using SPSS software, version 17.0 (SPSS, Inc., Chicago,
IL, USA). P≤0.05 was considered to indicate a statistically
significant difference.
Results
MVD and expression of BAI-1, mutant p53
and VEGF in BTCC tissues
IHC analysis showed that BAI-1 was expressed in the
cytoplasm and cell membrane, and VEGF was present in the cytoplasm,
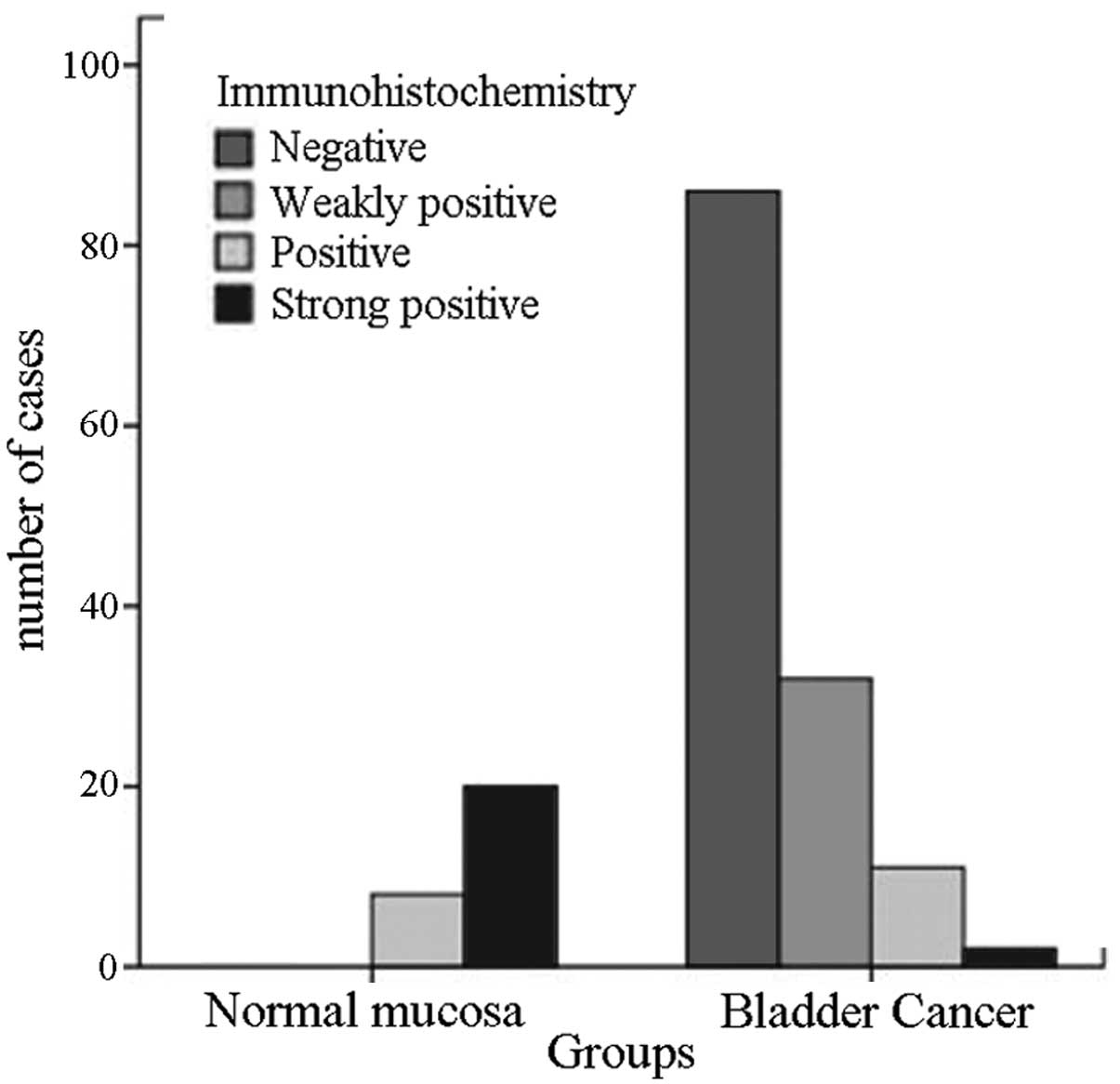
and mutant p53 was expressed in the nucleus (Fig. 1). Among the 28 normal bladder
mucosa specimens, 28 (100%), 5 (17.5%) and 1 (3.5%) were positive
for BAI-1, mutant p53 and VEGF expression, respectively (Tables I and II). Among the 131 BTCC tissue specimens,
89 (67.9%), 45 (34.4%) and 97 (74.0%) were positive for mutant p53,
BAI-1 and VEGF expression. There were significantly fewer
BAI-1-positive specimens in the BTCC group than in the normal
bladder mucosa group (P<0.01; Table
I, Fig. 2). Mutant p53 and
VEGF expression were more common in the BTCC group than those in
the normal bladder mucosa group (P<0.05; Table II). The MVD in the 28 normal
bladder mucosa samples was 0.6–1.6/high power field (HPF) with an
average of 1.2±0.35. The MVD of the 131 BTCC samples was
4.4–13.4/HPF, with an average of 8.94±2.08 (P<0.01 compared with
normal bladder mucosa) (Table
II).
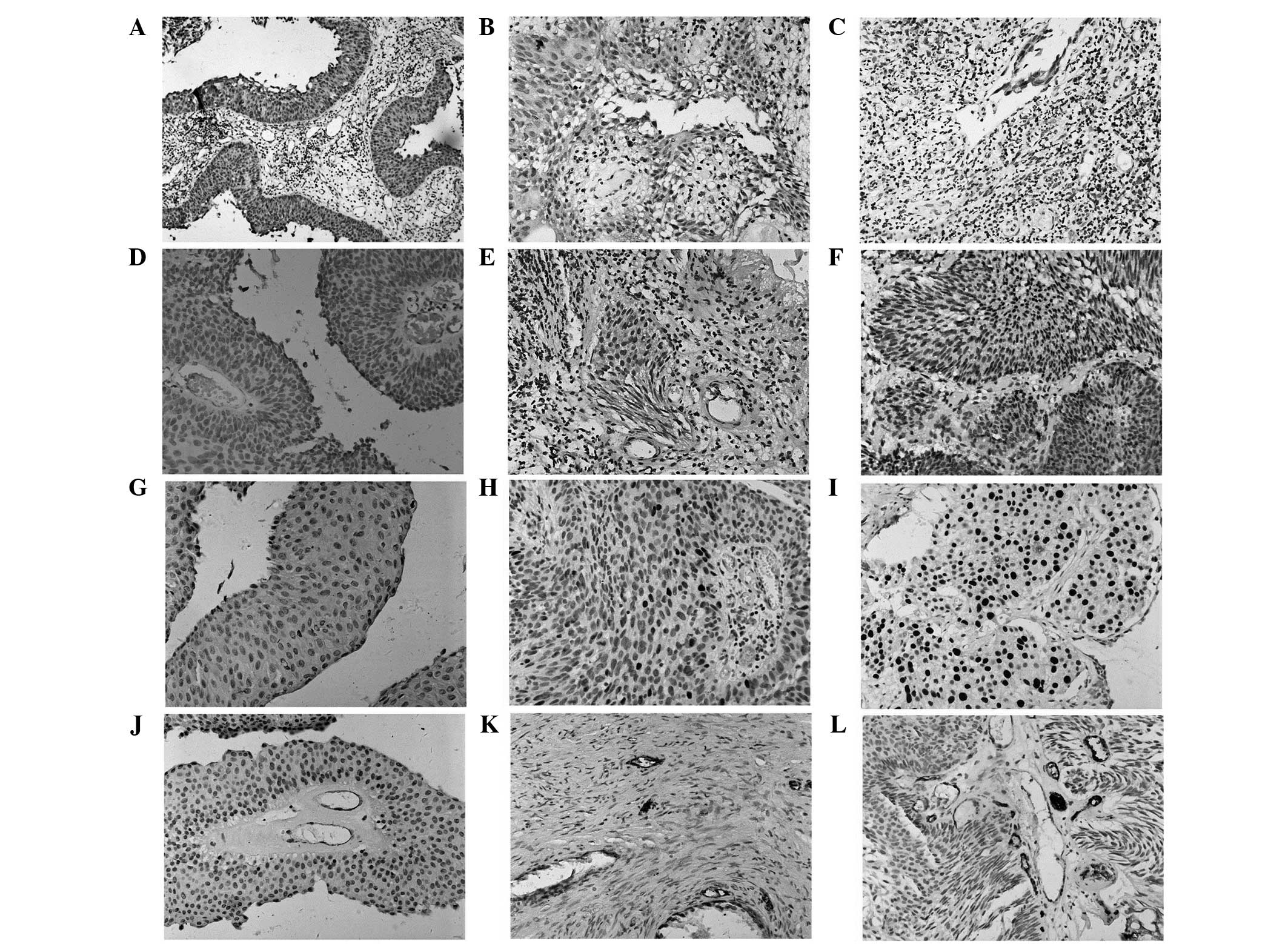 | Figure 1BAI-1, VEGF and p53 expression and MVD
in bladder mucosa from the different groups. Representative images
showing staining for BAI-1 in (A) normal bladder mucosa, (B)
T1-stage BTCC and (C) T2-4-stage BTCC; VEGF in (D) normal bladder
mucosa, (E) T1-stage BTCC and (F) T2-4-stage BTCC; p53 expression
in (G) normal bladder mucosa, (H) T1-stage BTCC and (I) T2-4-stage
BTCC; and MVD in (J) normal bladder mucosa, (K) T1-stage BTCC and
(L) T2-4-stage BTCC (A–C, magnification ×100; D–L, magnification
×200). BAI-1, brain-specific angiogenesis inhibitor-1; VEGF,
vascular endothelial growth factor; MVD, microvessel density; BTCC,
bladder transitional cell carcinoma. |
 | Table IExpression of BAI-1 in bladder
epithelial cells. |
Table I
Expression of BAI-1 in bladder
epithelial cells.
| Group | BAI-1
immunohistochemistry
| Total (%) | χ2
value | P-value |
|---|
| − (%) | + (%) | ++ (%) | +++ (%) |
|---|
| BHP | 0 (0.00) | 0 (0.00) | 8 (30.1) | 20 (69.9) | 28 (100) | 108.738 | <0.001 |
| BTCC | 86 (65.6) | 32 (24.4) | 11 (8.4) | 2 (1.5) | 131 (100) |
| Table IIExpression of p53, MVD and VEGF in
bladder epithelial cells. |
Table II
Expression of p53, MVD and VEGF in
bladder epithelial cells.
| Parameter | BHP (n=28) | BTCC (n=131) | P value |
|---|
| VEGF, n (%) | | | <0.001 |
| − | 27 (96.5) | 34 (26.0) | |
| + | 1 (3.5) | 97 (74.0) | |
| p53, n (%) | | | <0.001 |
| − | 23 (82.5) | 42 (32.1) | |
| + | 5 (17.5) | 89 (67.9) | |
| MVD (n/HPF) | 1.20±0.35a | 8.94±2.08 | <0.05 |
Image analysis software was used to measure the ODs
of all the IHC sections, and the results demonstrated that the mean
OD value of BAI-1 staining in normal bladder mucosa samples was
significantly higher than that in the BTCC samples (Table III). The OD values of the
specimens correlated with the clinical stage, consistent with the
statistics of positive IHC staining scores. The OD analysis results
for mutant p53 were also consistent with those of VEGF (Table III, Fig. 3). As the statistical method to
determine the MVD used the capillary number density as a
measurement, the OD analysis method was not used to measure the
MVD.
| Table IIIExpression levels of p53, BAI-1 and
VEGF in bladder epithelial cells (n=159). |
Table III
Expression levels of p53, BAI-1 and
VEGF in bladder epithelial cells (n=159).
| Type of tissue | n | BAI-1 (OD) | VEGF (OD) | p53 (OD) |
|---|
| Normal | 28 | 176.81±97.01 | 6.54±5.42 | 23.8631±19.58 |
| T1 | 57 | 69.28±79.62 | 43.754±23.19 | 116.29±34.92 |
| T2-4 | 74 | 27.27±27.71 | 217.28±124.99 | 449.89±240.56 |
| F value | | 11.885 | 28.557 | 15.712 |
| P value | | <0.001 | <0.001 | <0.001 |
Association of BAI-1 with
clinicopathological parameters of epithelial cancer
The association between BAI-1, VEGF, mutant p53 and
MVD and age, gender, tumor grade, stage and number were further
analyzed. Mutant p53 was observed to be positively correlated with
the tumor grade, stage and whether multiple occurrence existed or
not. With the increasing tumor grade and stage, the rate of
positivity for mutant p53 expression increased correspondingly
(P<0.001; Table IV), the rate
in the multiple tumor group (93.2%) was significantly higher than
that in the single tumor group (64.4%; P<0.001). The correlation
between mutant p53 expression and age or gender was not identified
to be statistically significant (P>0.05) (Table IV).
| Table IVAssociation between BAI-1, p53, VEGF
and MVD and clinicopathological features in 131 cases of bladder
cancer. |
Table IV
Association between BAI-1, p53, VEGF
and MVD and clinicopathological features in 131 cases of bladder
cancer.
| Characteristic | Total, n (%) | p53, n (%)
| BAI-1, n (%)
| VEGF, n (%)
| MVDa (n/HPF) |
|---|
| − | + | − | + | − | + |
|---|
| Total (n) | | 42 | 89 | 86 | 45 | 34 | 97 | |
| Age (years) |
| ≤64 | 53 (40.3) | 18 (33.3) | 35 (63.7) | 36 (67.9) | 17 (32.1) | 16 (30.2) | 37 (69.8) | 8.80±2.31 |
| >64 | 78 (59.7) | 24 (30.8) | 54 (69.2) | 50 (64.1) | 28 (65.9) | 18 (23.1) | 60 (76.9) | 9.06±1.69 |
| P-value | | 0.142 | | 0.129 | | 0.334 | | 0.58 |
| Gender |
| Male | 88 (67.2) | 28 (31.8) | 60 (68.2) | 57 (64.8) | 31 (35.2) | 25 (27.9) | 63 (72.1) | 8.67±2.11 |
| Female | 43 (32.8) | 14 (32.5) | 29 (67.5) | 29 (67.4) | 14 (32.6) | 9 (20.9) | 34 (79.1) | 8.93±1.79 |
| P-value | | 0.205 | | 0.143 | | 0.927 | | 0.62 |
| Stage |
| T1 | 57 (46.8) | 30 (52.6) | 27 (47.4) | 19 (33.3) | 38 (66.7) | 27 (47.4) | 30 (42.6) | 6.79±1.17 |
| T2-4 | 74 (53.2) | 12 (16.2) | 62 (83.8) | 67 (90.5) | 7 (9.5) | 7 (9.5) | 67 (90.5) | 9.88±1.87 |
| P-value | | <0.01 | | <0.01 | | <0.01 | | <0.01 |
| Grade |
| G1-2 | 90 (68.7) | 35 (31.5) | 55 (68.5) | 46 (51.1) | 44 (48.9) | 32 (35.6) | 58 (64.4) | 7.63±1.46 |
| G3 | 41 (31.3) | 4 (9.8) | 37 (90.2) | 40 (97.6) | 1 (2.4) | 2 (4.9) | 39 (95.1) | 9.55±2.07 |
| P-value | | 0.01 | | <0.01 | | <0.01 | | <0.01 |
| Multiplicity |
| Single | 87 (66.4) | 39 (35.6) | 48 (64.4) | 53 (60.9) | 34 (39.1) | 27 (31.0) | 60 (69.0) | 8.01±1.90 |
| Multiple | 44 (25.0) | 3 (6.8) | 41 (93.2) | 33 (75.0) | 11 (25.0) | 7 (15.9) | 37 (84.1) | 9.47±2.31 |
| P-value | | <0.01 | | <0.05 | | <0.05 | | 0.17 |
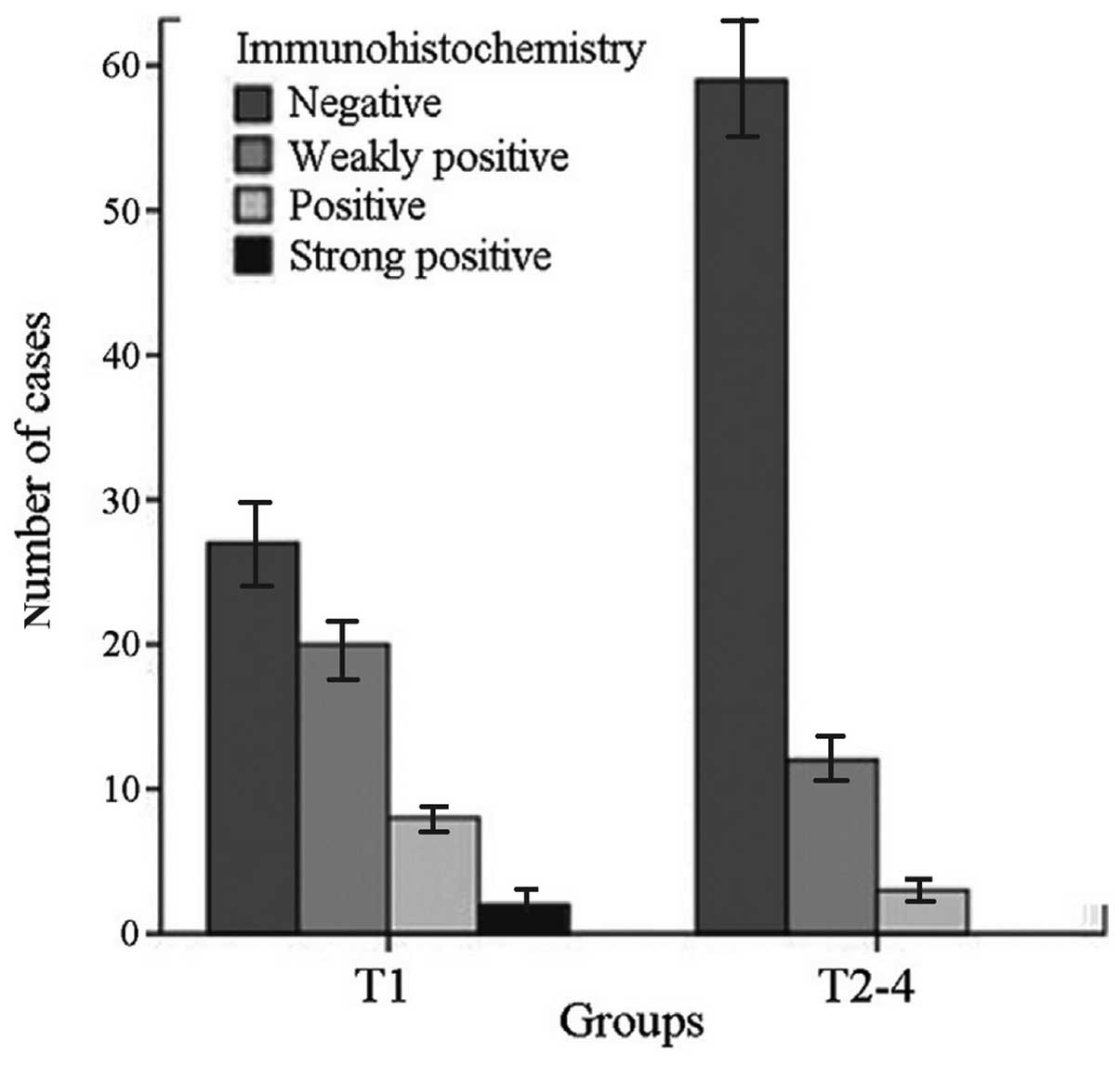
BAI-1 was negatively correlated with tumor grade,
stage and multiple tumor occurrence (Table IV); with increasing tumor grade
and stage, the BAI-1-positive rate decreased correspondingly
(P<0.01) (Tables IV and
V, Fig. 4). The BAI-1-positive rate in the
multiple BTCC group (25%) was significantly lower than that in the
single group (39.1%; P<0.05). No significant correlation was
observed between BAI-1 expression and age or gender.
| Table VBAI-1 expression in tissues at
different clinical stages of bladder transitional cell
carcinoma. |
Table V
BAI-1 expression in tissues at
different clinical stages of bladder transitional cell
carcinoma.
| Stage | BAI-1
immunohistochemistry, n (%)
| Total, n (%) | χ2
value | P value |
|---|
| − | + | ++ | +++ |
|---|
| T1 | 27 (47.4) | 20 (35.1) | 8 (14.0) | 2 (3.5) | 57 (100) | 17.138 | <0.001 |
| T2-4 | 59 (79.7) | 12 (16.2) | 3 (4.1) | 0 (0.0) | 74 (100) |
| Total | 86 | 32 | 11 | 2 | 131 | | |
VEGF was positively correlated with tumor grade,
stage and multiple tumor occurrence; as the tumor grade and stage
increased, the rate of positivity for VEGF expression increased
accordingly (P<0.01; Table
IV). The rate of positivity for VEGF expression in the multiple
BTCC group (84.1%) was significantly higher than that in the single
BTCC group (69.0%) (P<0.05; Table
IV). The correlation of VEGF expression with age or gender was
not statistically significant.
The MVD was positively correlated with the tumor
grade and stage (Table IV). As
the tumor grade and stage increased, the MVD in each high
magnification microscopic field increased correspondingly. The MVD
in the multiple BTCC group was not significantly higher than that
in the single BTCC group. Correlations between MVD and age, gender
and multiple occurrence were not identified as significant
(Table IV).
Correlation analysis
The IHC ODs were used to perform a correlation
analysis between BAI-1 and mutant p53 and VEGF (Table III). The results indicated a
negative correlation with the average ODs, which were more accurate
than the IHC scoring values; therefore, the mean ODs were used for
the calculations. In the Spearman's rank correlation analysis,
BAI-1 was identified to be negatively correlated with mutant p53
(r=−0.675, P<0.001), VEGF (r=−0.661, P<0.001) and MVD
(r=−0.406, P=0.002), indicating that BAI-1 may be regulated by
mutant p53, and this regulation is lost following the mutation of
mutant p53, resulting in the reduction of BAI-1 expression. In
addition, BAI-1 regulated the expression of VEGF; VEGF was
upregulated and the capillary number increased when a reduction in
the levels of BAI-1 expression was observed.
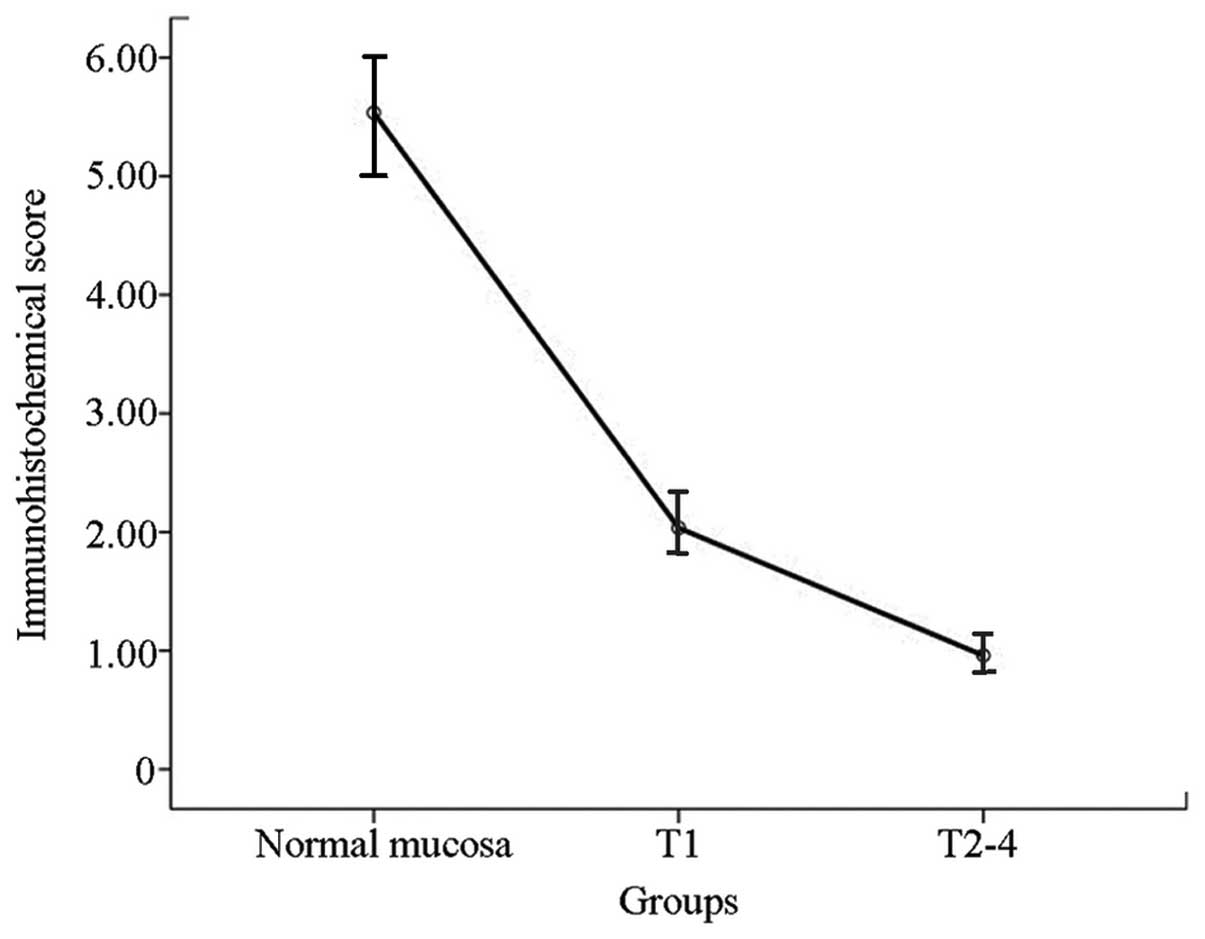
BAI-1 decreases with the increase in
tumor score
The results of the western blot analysis conducted
on the freshly resected bladder cancer samples and normal bladder
tissues were consistent with those of the IHC analysis. The BAI-1
protein content in the BTCC group was lower than that in the
corresponding normal bladder mucosa, and was correlated with the
clinical stage. In stage T1 samples, the BAI-1 content was
significantly reduced as sompared with that in normal bladder
mucosa, while BAI-1 was absent in T2-4 urothelial carcinoma tissues
was absent (Fig. 5). In analogy
with the western blot results, correlation of tumor staging with
immunohistochemical scoring of BAI-1 also showed that BAI-1 was
significantly decreased with increasing tumor stage (Fig. 6).
Discussion
In a study of functional p53 binding sites in human
brain glioma in 1997, a novel target gene was isolated and termed
BAI-1 (13). Although initially
identified in glioma tissues, subsequent studies demonstrated that
BAI-1 existed in other tissues, including kidney and colon, and was
associated with the clinical tumor stage indicating the progression
of the malignancy; the BAI-1 content was reduced or absent with the
increase in tumor stage. Thus, the present study aimed to quantify
the normal bladder mucosa paraffin tissue sections by IHC and
detected fresh normal bladder tissue protein by western blot
analysis. It was indicated that BAI-1 existed in normal bladder
tissues. By analyzing 131 paraffin-embedded specimens from patients
with BTCC and 21 specimens from patients with fresh urothelial
carcinoma, it was demonstrated that BAI-1 protein levels in the
bladder cancer samples were significantly lower than those in the
normal bladder tissues; this change in protein levels exhibited a
correlation with the clinical stage and whether multiple occurrence
existed or not. BAI-1 levels were reduced with the increase of
clinical stage; BAI-1 was almost absent in the T2-4 tumor tissues,
and BAI-1 levels in multiple BTCC were significantly lower than
those in the single tumors. The present study indicated that BAI-1
was expressed in a larger percentage of normal bladder epithelial
tissues compared with that of urothelial cell carcinoma samples.
Furthermore, the content of BAI-1 was negatively correlated with
the staging of bladder carcinoma. BAI-1 may serve an important
function in the suppression of tumor development.
BAI-1 is a p53 target gene, and the present study
hypothesized that the reduced levels of BAI-1 in BTCC may be
associated with a reduction of p53 mutations in tumor tissues. p53
is one of the most common established suppressor genes observed in
the study of human malignancies. Previous studies have demonstrated
that numerous oncogenes or tumor suppressor genes can recognize and
bind to p53, thus regulating it at the transcriptional level
(14). In the stage of tumor
progression, p53 gene mutation leads to angiogenesis, which is
conducive to the rapid growth of the tumor, and the tumor often
enters the late tumor stage. The p53 gene can be divided into
wild-type and mutant-type. The wild-type is an unstable regulatory
protein with a half-life of 20 min. The p53 protein most commonly
detected in urothelial carcinoma by IHC methods is the mutant-type.
The mutant p53 protein expression rate increases with the
progression of the malignancy, reflecting that the high degree of
expression of mutant p35 in bladder cancer causes its
aggressiveness and high metastatic potential (15). Expression of mutant p53 protein in
bladder cancer tissues has been indicated to be significantly
correlated with grading and staging. The increase of mutant p53
protein was a result of the inactivation of wild-type p53,
suggesting that the action of the p53 tumor suppressor gene was
weakened or lost (15,16). In the present study, the rate of
mutant p53 expression in low-grade, low-stage and in single-tumor
bladder cancer was lower than that in the high-grade, high-stage
and multiple-tumor bladder cancer. The upregulation of mutant p53
expression levels in the present study was negatively correlated
with the reduction of BAI-1 expression levels, indicating that the
mutations and inactivation of p53 in bladder cancer may lead to
BAI-1 downregulation.
As the tumor diameter reaches >1–2 mm, tumor
tissues are challenged to obtain sufficient oxygen and nutrients,
dependent on the growth of further blood vessels (17). The present study observed that
BAI-1 expression was negatively correlated with VEGF and MVD. The
BAI-1 extracellular fragment comprises five repeats of the TSP-1
fragment that was initially isolated from thrombin-stimulated
platelet membrane by Baenziger et al (18). Their in vivo experiments
demonstrated that TSP-1 was an endogenous angiogenesis inhibitor in
the tumor microenvironment. Other studies have indicated that TSP-1
can inhibit tumor growth and the occurrence and development of
tumors (19–21). TSP-1 and its receptor CD36 serve an
important role in the inhibition of angiogenesis. The endothelial
cells of small blood vessels and certain epithelial and stromal
cells may express CD36. CD36 is required for TSP-1 binding and the
inhibition of angiogenesis. In previous in vitro
experiments, CD36 was able to mediate TSP-1 to inhibit the
formation of endothelial cells and migration of blood vessels
(22,23). The outer membrane structure of
BAI-1 has five TSP-1 repeats, which supports the theory of an anti
vascular function via the inhibition of endothelial cell
proliferation (24).
VEGF is a cytokine of the platelet-derived growth
factor family that is widely distributed in the brain, kidney,
liver and other tissues in humans and other animals, and can
produce numerous biological effects. VEGF is able to promote the
proliferation of endothelial cells, increase vascular permeability,
promote angiogenic support (25)
and inhibit apoptosis of tumor cells. TSP-1 may affect the activity
of VEGF through the following mechanisms: TSP-1 is able to inhibit
the activity of matrix metalloproteinase-9 so that the
extracellular matrix releases VEGF. This leads to tumor matrix
formation, angiogenesis and tumor cell transfer. Furthermore, TSP-1
is able to combine with VEGF to mediate the uptake and clearance of
VEGF (26).
In the 1990s, Folkman (27) demonstrated that tumor growth
occurred in two distinct phases, e.g. the initial slow growth phase
of blood vessels and the rapid growth phase, which confirms that
the tumor blood vessels were newly generated vessels. New blood
vessel network systems provide adequate oxygen and nutrients for
tumor growth to ensure the rapid proliferation of tumor cells.
Under normal circumstances, the process of angiogenesis is under
strict control, while during tumorigenesis, a loss of cell cycle
regulation and a switch from the suppression phenotype of
capillaries into the active phenotype is present (28). MVD is used in tumor vasculature as
the gold standard for evaluation of tumor-induced angiogenesis, and
is closely associated with tumor malignant behavior (recurrence and
metastasis) (29). Bergers and
Benjamin (30) indicated that
vascular tissue formation reflects the aggressiveness of the tumor,
and a high MVD is associated with high probability of tumor cells
entering the blood circulation; the tumor invasion and metastasis
potential of malignant tumors increases as with increasing MVD.
Therefore, MVD can be used to characterize the tumor growth,
invasion ability, malignancy potential and prognosis to a certain
extent.
In the present study, BAI-1 was negatively
correlated with VEGF expression and MVD in the clinical samples.
Based on the structure and function of BAI-1 binding fragments in
the outer membrane, it was theorized that BAI-1 inhibits the
formation of vascular endothelial cells and microvascular
proliferation by inhibiting the expression of VEGF via TSP-1. Thus,
low BAI-1 expression may promote tumor proliferation, invasion and
metastasis.
BAI-1 is a G protein-coupled receptor (GPCR), which
is a type of transmembrane receptor protein with seven
transmembrane helices (31). GPCRs
combine and regulate the activity of G proteins, which are a vital
class of signaling receptor molecules (32). Diseases associated with the GPCRs
are numerous, and ~40% of modern drugs use GPCRs as therapy
targets. The aim of research and development of modern drugs is to
locate, identify and prepare targets of drug screening (molecular
drug targets). Drug targets are drug binding sites, including the
locui, receptors, enzymes, ion channels, nucleic acids and other
biological macromolecules. Identification of novel drug targets is
the initial task in drug development. As a member of the GPCR
family, BAI-1 has the potential to become a novel target for anti
angiogenic therapy in the future.
In summary, BAI-1 expression was assessed in human
bladder epithelial cells from patients with BTCC or in healthy
bladder mucosa, and the levels of BAI-1 expression were
demonstrated to be associated with the clinical stage as well as
the multiplicity of tumor occurrence. The BAI-1 downregulation in
urothelial carcinoma may be associated with p53 mutations. As a
target protein of p53 regulation, BAI-1 is downregulated when
wild-type p53 becomes mutated. The reduction or absence of BAI-1
may result in the increase in VEGF levels, leading to an increase
in tumor microvessel density, thus prompting tumorigenesis and
tumor progression. Therefore, BAI-1 protein levels have the
potential to be a predictor of malignancy in tumor prognosis.
Additionally, the study of the BAI-1 pathway in bladder urothelial
carcinoma will contribute to the elucidation of the pathogenesis of
bladder cancer and provide evidence for the use of inhibitors, with
BAI-1 as a target. Thus, BAI-1 may be a novel target for cancer
therapy.
References
|
1
|
Jemal A, Siegel R, Ward E, et al: Cancer
statistics, 2008. CA Cancer J Clin. 58:71–96. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rübben H, Lutzeyer W, Fischer N, Deutz F,
Lagrange W and Giani G: Natural history and treatment of low and
high risk superficial bladder tumors. J Urol. 139:283–285.
1988.PubMed/NCBI
|
|
3
|
Sharifiaghdas F and Beigi FM: Impalpable
testis: laparoscopy or inguinal canal exploration? Scand J Urol
Nephrol. 42:154–157. 2008. View Article : Google Scholar
|
|
4
|
Reuter VE: The pathology of bladder
cancer. Urology. 67(Suppl 1): 11–18. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sylvester RJ, van der Meijden AP and Lamm
DL: Intravesical bacillus Calmette-Guerin reduces the risk of
progression in patients with superficial bladder cancer: a
meta-analysis of the published results of randomized clinical
trials. J Urol. 168:1964–1970. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lamm DL, Blumenstein BA, Crissman JD, et
al: Maintenance bacillus Calmette-Guerin immunotherapy for
recurrent TA, T1 and carcinoma in situ transitional cell carcinoma
of the bladder: a randomized Southwest Oncology Group Study. J
Urol. 163:1124–1129. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Davis JW, Sheth SI, Doviak MJ and
Schellhammer PF: Superficial bladder carcinoma treated with
bacillus Calmette-Guerin: progression-free and disease specific
survival with minimum 10-year followup. J Urol. 167:494–501. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Nam DH, Park K, Suh YL and Kim JH:
Expression of VEGF and brain specific angiogenesis inhibitor-1 in
glioblastoma: prognostic significance. Oncol Rep. 11:863–869.
2004.PubMed/NCBI
|
|
9
|
Yoshida Y, Oshika Y, Fukushima Y, et al:
Expression of angiostatic factors in colorectal cancer. Int J
Oncol. 15:1221–1225. 1999.PubMed/NCBI
|
|
10
|
Hatanaka H, Oshika Y, Abe Y, et al:
Vascularization is decreased in pulmonary adenocarcinoma expressing
brain-specific angiogenesis inhibitor 1 (BAI1). Int J Mol Med.
5:181–183. 2000.PubMed/NCBI
|
|
11
|
Sobin LH and Wittekind C: TNM
Classification of Malignant Tumors (UICC). 6th edition. Wiley-Liss;
New York, NY: pp. 199–203. 2002
|
|
12
|
Kagan VE, Kisin ER, Kawai K, et al: Toward
mechanism-based antioxidant interventions: lessons from natural
antioxidants. Ann NY Acad Sci. 959:188–198. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kuwano M, Nakamura Y and Tokino T: A novel
brain-specific p53-target gene, BAI1, containing thrombospondin
type-1 repeats inhibits experimental angiogenesis. Oncogene.
15:2145–2150. 1997. View Article : Google Scholar
|
|
14
|
Kim E and Deppert W: The versatile
interactions of p53 with DNA: when flexibility serves specificity.
Cell Death Differ. 13:885–889. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Piaton E, Faÿnel J, Ruffion A, Lopez JG,
Perrin P and Devonec M: p53 immunodetection of liquid based
processed urinary samples helps to identify bladder tumours with a
higher risk of progression. Br J Cancer. 93:242–247. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wei M, Wanibuchi H, Morimura K, et al:
Carcinogenicity of dimethylarsinic acid in male F334 rats and
genetic alterations in induced urinary bladder tumors.
Carcinogenesis. 23:1387–1397. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Anderson JC, McFarland BC and Gladson CL:
New molecular targets in angiogenic vessels of glioblastoma
tumours. Expert Rev Mol Med. 10:e232008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Baenziger NL, Brodie GN and Majerus PW: A
thrombin-sensitive protein of human platelet membranes. Proc Natl
Acad Sci USA. 68:240–243. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Naumov GN, Bender E, Zurakowski D, et al:
A model of human tumor dormancy: an angiogenic switch from the
nonangiogenic phenotype. J Natl Cancer Inst. 98:316–325. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Okada K, Hirabayashi K, Imaizumi T, et al:
Stromal thrombospondin-1 expression is a prognostic indicator and a
new marker of invasiveness in intraductal papillary-mucinous
neoplasm of the pancreas. Biomed Res. 31:13–19. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Greenaway J, Lawler J, Moorehead R,
Bornstein P, Lamarre J and Petrik J: Thrombospondin-1 inhibits VEGF
levels in the ovary directly by binding and internalization via the
low density lipoprotein receptor-related protein-1 (LRP-1). J Cell
Physiol. 210:807–818. 2007. View Article : Google Scholar
|
|
22
|
Dawson DW, Pearce SF, Zhong R, Silverstein
RL, Frazier WA and Bouck NP: CD36 mediates the in vitro inhibitory
effects of thrombospondin-1 on endothelial cells. J Cell Biol.
138:707–717. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Dawson DW, Volpert OV, Pearce SF, et al:
Three distinct D-amino acid substitutions confer potent
antiangiogenic activity on an inactive peptide derived from a
thrombospondin-1 type 1 repeat. Mol Pharmacol. 55:332–338.
1999.PubMed/NCBI
|
|
24
|
Koh JT, Kook H, Kee HJ, et al:
Extracellular fragment of brain-specific angiogenesis inhibitor 1
suppresses endothelial cell proliferation by blocking alphavbeta5
integrin. Exp Cell Res. 294:172–184. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nicosia RF: What is the role of vascular
endothelial growth factor-related molecules in tumor angiogenesis?
Am J Pathol. 153:11–16. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kang SY and Watnick RS: Regulation of
tumor dormancy as a function of tumor-mediated paracrine regulation
of stromal TSP-1 and VEGF expression. APMIS. 116:638–647. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Folkman J: What is the evidence that
tumors are angiogenesis dependent? J Natl Cancer Inst. 82:4–6.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I. The value of histological
grade in breast cancer: Experience from a large study with
long-term follow-up. Histopathology. 41:154–161. 2002.PubMed/NCBI
|
|
29
|
Kato T, Steers G, Campo L, et al:
Prognostic significance of microvessel density and other variables
in Japanese and British patients with primary invasive breast
cancer. Br J Cancer. 97:1277–1286. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bergers G and Benjamin LE: Tumorigenesis
and the angiogenic switch. Nat Rev Cancer. 3:401–410. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
El Moustaine D, Granier S, Doumazane E, et
al: Distinct roles of metabotropic glutamate receptor dimerization
in agonist activation and G-protein coupling. Proc Natl Acad Sci
USA. 109:16342–16347. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
New DC and Wong YH: Molecular mechanisms
mediating the G protein-coupled receptor regulation of cell cycle
progression. J Mol Signal. 2:22007. View Article : Google Scholar : PubMed/NCBI
|