Introduction
Lung cancer is the most common type of cancer and
the leading cause of cancer mortality worldwide (1). Despite complete surgical resection,
the prognosis of lung cancer is generally poor (2), with recurrence rates of 15–30% and
5-year survival rates of 60–70% (3). Lung cancer is commonly classified
into four types: squamous cell carcinoma (SqCC), adenocarcinoma,
large cell carcinoma and small cell carcinoma, based on the
histological features (2,4,5).
Patient prognosis with SqCC is more favorable than the other
histological types (2,6). Customized chemotherapy for
unresectable or recurrent lung cancers is more frequently used for
adenocarcinoma than for SqCC (7,8). In
addition, molecular targeting therapies, including bevacizumab
(9,10), erlotinib (11,7)
and gefitinib (7) have been
developed recently. By contrast, there are few therapeutic options
for recurrent SqCC. Therefore, it is necessary to examine the
histopathological features to clarify a poor prognosis group for
SqCC.
Invasive patterns have been considered as prognostic
factors for other solid cancers (12–14).
Tumor budding is believed to be a significant invasive pattern and
has attracted interest, and is defined as isolated single cancer
cells or a cluster of cancer cells composed of fewer than five
cells (15,16). Tumor budding has been reported to
be a prognostic factor not only in the gastrointestinal tract
(16–18), but also in the tongue (19) and larynx (20). The gastrointestinal pathology
commonly describes the budding grade at the invasive front of the
cancer. However, evaluation of the budding grade is believed to be
difficult at the invasive front of lung SqCC, but tumor budding was
observed in the fibrosis and collapse at the tumor-stroma interface
of lung adenocarcinoma (21).
The aim of the present study was to identify
indicators that may be used to predict a poor prognosis for
patients with SqCC based on tumor budding and other
clinicopathological factors.
Materials and methods
Lung cancer specimens
The cancer tissue specimens were obtained from
surgically resected lung SqCC cases following the receipt of
patient informed consent, according to the Institutional Review
Board (IRB) of Tokai University Hospital. The 103 patients (97
males and 6 females; age range, 43–85 years; mean age, 67.2±9.1
years) with lung SqCC underwent radical surgery (lobectomy and
mediastinal lymphadenectomy) at Tokai University Hospital
(Kanagawa, Japan). The tumor stages were defined according to the
TNM classification of the International Union Against Cancer (UICC)
(22) and the histological types
were defined according to the World Health Organization
classifications (6). The median
postoperative follow-up duration was 1,528 (41–3,837) days.
Histological examination
The lung tissue specimens for histological analysis
were fixed with 10% buffered formalin for 24–48 h and routinely
embedded in paraffin. The tumors were cut at 5–10-mm intervals.
Tumor and lymphatic invasion were examined on 4-μm thick sections
stained with hematoxylin and eosin. Vascular and pleural invasion
were evaluated using the Verhoeff-van Gieson method.
Tumor infiltrative patterns (INF) at the invasive
front were classified into three groups according to the general
criteria for gastric cancer studies (23–25):
INFa, cancer nests demonstrate an expansion of growth and a
distinct border with the surrounding tissue; INFb, the manner of
growth and invasive pattern are between those of INFa and INFc; and
INFc, cancer nests show infiltrative growth and the borderline with
the surrounding tissue is unclear (Fig. 1). The stromal types, i.e.
cancer-stroma relationship patterns, were also classified into
three groups: medullary type, stroma is limited; intermediate type,
quantity of stroma is intermediate between those of the scirrhous
and medullary types; and scirrhous type, stroma is abundant
(23).
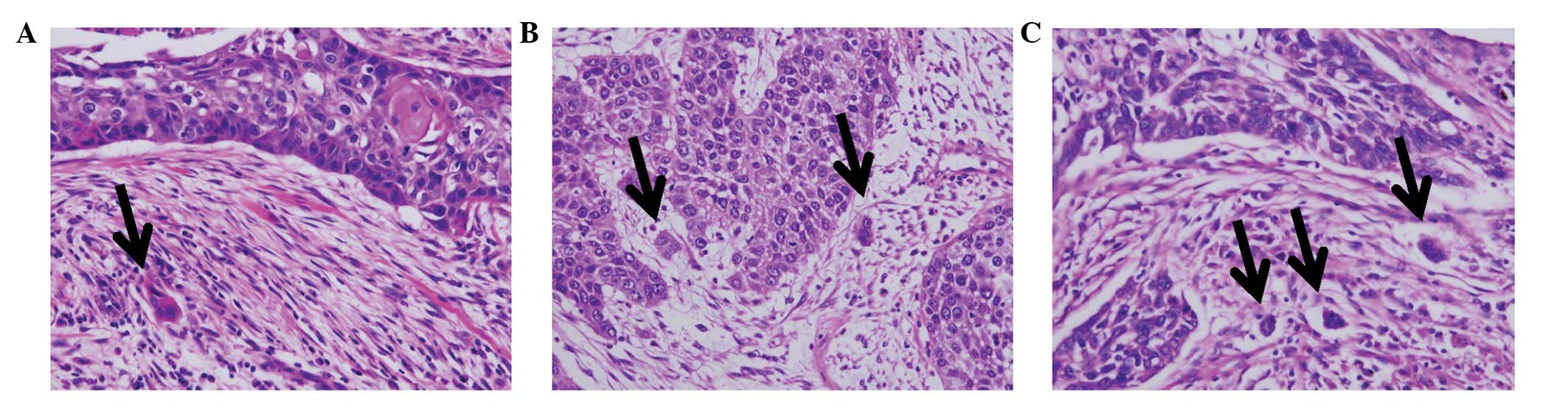
Tumor budding was defined as single cancer cells and
clusters composed of up to four cancer cells (26). These cancer cells were observed in
cancer-stroma lesions at the invasive front of the tumor. Numbers
of tumor budding foci were counted in the histological fields in
which the tumor budding intensity was maximal within the
histological section, using a ×20 objective lens as described
previously (16). In the present
study, the cases were classified into two groups: tumor
budding-positive/negative [Bud(+)/Bud(−)]. According to the number
of tumor buds per field, the cases were subclassified into three
groups: grade 0, no budding foci; grade 1, up to two budding foci;
and grade 2, three or more budding foci (Fig. 2).
Statistical analysis
Univariate analyses (Chi-square tests) were
primarily used for selecting variables on the basis of a value of
P<0.05. A Cox proportional hazards regression analysis was used
to determine the net effect of each predictor while controlling for
the effects of the other factors by univariate and multivariate
analysis. Hazard ratios (HR) and their 95% confidence intervals
(CI) were used to assess the independent contributions of
significant factors. P<0.05 was considered to indicate a
statistically significant result.
The patient survival time was measured between the
date of surgery and mortality from all causes (without
discrimination between mortalities resulting from lung carcinoma
and other causes). Survival curves were created using the
Kaplan-Meier method and compared using the log-rank test. All
analyses were performed using the SPSS II statistical software
package (version 19.0; SPSS Inc., Tokyo, Japan).
Results
Tumor INF of lung SqCC
Tumor INF were classified into three groups, INFa, b
and c, but certain cases had two components of INF, including
INFa>b. The numbers of these INF groups were as follows: INFa
(11, 10.7%); INFa>b (10, 9.7%); INFb (43, 41.7%); INFb>c (31,
30.1%); INFb<c (4, 3.9%); and INFc (4, 3.9%). The cases with an
INFc component [INF(+) = INFb>c, INFb<c and INFc] showed a
poor outcome, compared with those without the INFc component
[INFc(−) = INFa, INFa>b and INFb] (Table I). The stromal types, i.e., the
cancer-stroma relationship patterns, were divided into three
groups, as follows: medullary (39, 37.9%); intermediate (31,
30.1%); and scirrhous types (33, 32.0%). The correlations between
the tumor INF and clinicopathological features are summarized in
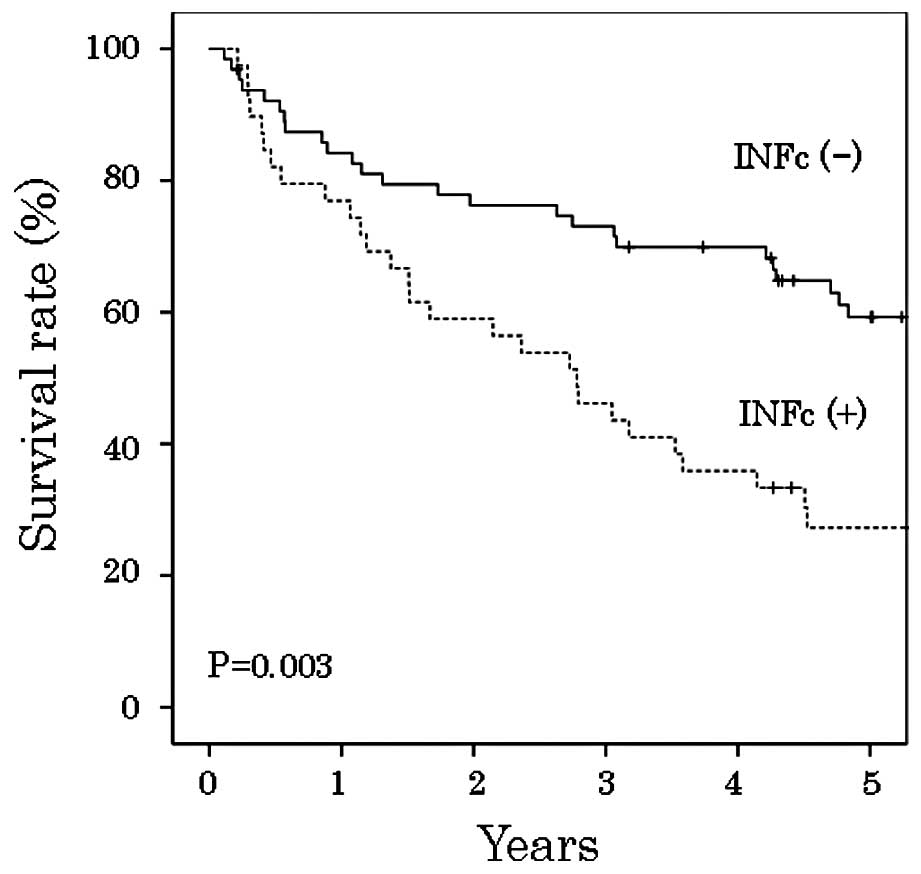
Table II. INFc(+) cases showed
significantly higher incidences of venous invasion (P=0.014) and
the scirrhous stromal type (P<0.001) than INFc(−) cases. Using
the Kaplan-Meier method and log-rank test, the overall patient
survival rate following curative resection was lower in INFc(+)
than in INFc(−) cases (P=0.003; Fig.
3).
 | Table IInfiltration patterns in lung squamous
cell carcinoma patients. |
Table I
Infiltration patterns in lung squamous
cell carcinoma patients.
| Variable | No. of patients
(%) | P-value | Hazard ratio | 95% confidence
interval |
|---|
| INFa | 11 (10.7) | 0.134 | 1.203 | 0.945–1.531 |
| INFa>b, b, b>c,
b<c, c | 92 (89.3) | | | |
| INFa, a>b | 21 (20.4) | 0.859 | 1.062 | 0.547–2.060 |
| INFb, b>c, b<c,
c | 82 (79.6) | | | |
| INFa, a>b, b | 64 (62.1) | 0.003 | 2.209 | 1.301–3.749 |
| INFb>c, b<c,
c | 39 (37.9) | | | |
| INFa, a>b, b,
b>c | 95 (92.2) | 0.363 | 1.535 | 0.610–3.860 |
| INFb<c, c | 8 (7.8) | | | |
| INFa, a>b, b,
b>c, b<c | 99 (96.1) | 0.961 | 1.036 | 0.252–4.255 |
| INFc | 4 (3.9) | | | |
| Table IITumor infiltration patterns and
clinicopathological features of lung squamous cell carcinoma. |
Table II
Tumor infiltration patterns and
clinicopathological features of lung squamous cell carcinoma.
| Variable | No. of patients
(%) | INFc(−) (%) | INFc(+) (%) | P-value |
|---|
| Age at surgery
(years) |
| <68 | 53 (51.5) | 37 (69.8) | 16 (30.2) | 0.098 |
| ≥68 | 50 (48.5) | 27 (54.0) | 23 (46.0) | |
| Gender |
| Male | 97 (94.2) | 61 (62.9) | 36 (37.1) | 0.528 |
| Female | 6 (5.8) | 3 (50.0) | 3 (50.0) | |
| Tumor size (mm) |
| ≤30 | 39 (37.9) | 23 (59.0) | 16 (41.0) | 0.606 |
| >30 | 64 (62.1) | 41 (64.1) | 23 (35.9) | |
| Lymph node
metastasis |
| n(−) | 70 (68.0) | 46 (65.7) | 24 (34.3) | 0.276 |
| n(+) | 33 (32.0) | 18 (54.5) | 15 (45.5) | |
| Lymphatic
invasion |
| ly(0, 1) | 84 (81.6) | 55 (65.5) | 29 (34.5) | 0.142 |
| ly(2, 3) | 19 (18.4) | 9 (47.4) | 10 (52.6) | |
| Venous
invasion |
| v(−) | 53 (51.5) | 39 (73.6) | 14 (26.4) | 0.014 |
| v(+) | 50 (48.5) | 25 (50.0) | 25 (50.0) | |
| Histological
differentiation |
| Well,
moderate | 90 (87.4) | 53 (58.9) | 37 (41.1) | 0.074 |
| Poor | 13 (12.6) | 11 (84.6) | 2 (15.4) | |
| Stromal type |
| Medullary,
intermediate | 70 (68.0) | 53 (75.7) | 17 (24.3) | <0.001 |
| Scirrhous | 33 (32.0) | 11 (33.3) | 22 (66.7) | |
Tumor budding of lung SqCC
Regarding tumor budding, there were 54 (52.4%) cases
with the Bud(+) type and 49 (47.6%) cases with the Bud(−) type.
Bud(+) cases included 22 cases (40.8%) with one budding focus, 20
cases (37.0%) with two budding foci, 6 cases (11.1%) with three
budding foci and 6 cases (11.1%) with >four budding foci. The
correlations between the tumor budding types and
clinicopathological features are summarized in Table III. Lymph node metastasis
(P=0.001), lymphatic invasion (P=0.002), the scirrhous stromal type
(P=0.016) and infiltrative pattern (P<0.001) showed
significantly higher incidences in the Bud(+) type. The overall
survival rate following curative resection was lower in patients
with the Bud(+) type than in those with the Bud(−) type
(P<0.001, log-rank test, Fig.
4). Using the Kaplan-Meier method and log-rank test, the
patient outcome of the Bud(−) group was significantly better than
that of the Bud(+) group; (P<0.001; Fig. 4).
| Table IIITumor budding and clinicopathological
features of lung squamous cell carcinoma. |
Table III
Tumor budding and clinicopathological
features of lung squamous cell carcinoma.
| Variable | No. of patients
(%) | Bud(−) (%) | Bud(+) (%) | P-value |
|---|
| Age at surgery
(years) |
| <68 | 53 (51.5) | 27 (50.9) | 26 (49.1) | 0.481 |
| ≥68 | 50 (48.5) | 22 (44.0) | 28 (56.0) | |
| Gender |
| Male | 97 (94.2) | 44 (45.4) | 53 (54.6) | 0.071 |
| Female | 6 (5.8) | 5 (83.3) | 1 (16.7) | |
| Tumor size
(mm) |
| ≤30 | 39 (37.9) | 19 (48.7) | 20 (51.3) | 0.856 |
| >30 | 64 (62.1) | 30 (46.9) | 34 (53.1) | |
| Lymph node
metastasis |
| n(−) | 70 (68.0) | 41 (58.6) | 29 (41.4) | 0.001 |
| n(+) | 33 (32.0) | 8 (24.2) | 25 (75.8) | |
| Lymphatic
invasion |
| ly(0, 1) | 84 (81.6) | 46 (54.8) | 38 (45.2) | 0.002 |
| ly(2, 3) | 19 (18.4) | 3 (15.8) | 16 (84.2) | |
| Venous
invasion |
| v(−) | 53 (51.5) | 27 (50.9) | 26 (49.1) | 0.481 |
| v(+) | 50 (48.5) | 22 (44.0) | 28 (56.0) | |
| Histological
differentiation |
| Well,
moderate | 90 (87.4) | 43 (47.8) | 47 (52.2) | 0.913 |
| Poor | 13 (12.6) | 6 (46.2) | 7 (53.8) | |
| Stromal type |
| Medullary,
intermediate | 70 (68.0) | 39 (55.7) | 31 (44.3) | 0.016 |
| Scirrhous | 33 (32.0) | 10 (30.3) | 23 (69.7) | |
| Infiltrating
pattern |
| INFc(−) | 64 (62.1) | 41 (64.1) | 23 (35.9) | <0.001 |
| INFc(+) | 39 (37.9) | 8 (20.5) | 31 (79.5) | |
Clinicopathological significance of tumor
INF/tumor budding
The univariate analyses identified six factors
associated with increased mortality in patients with lung SqCC
(Table IV): tumor size (HR,
1.897; 95% CI, 1.059–3.396); lymph node metastasis (HR, 3.028; 95%
CI, 1.785–5.136); lymphatic invasion (HR, 3.298; 95% CI,
1.827–5.952); histological differentiation (HR, 2.092; 95% CI,
1.050–4.168); tumor infiltrative patterns (HR, 2.209; 95% CI,
1.301–3.749); and tumor budding (HR, 3.276; 95% CI, 1.841–5.827).
The scirrhous stromal type did not significantly affect the
survival of patients with lung SqCC (HR, 1.229; 95% CI,
0.706–2.139). The multivariate analysis is summarized in Table V. Tumor budding (HR, 2.766; 95% CI,
1.497–5.109) and lymph node metastasis (HR, 1.937; 95% CI,
1.097–3.419) remained significant predictors of patient
mortality.
| Table IVClinicopathological features and
survival in lung squamous cell carcinoma patients. |
Table IV
Clinicopathological features and
survival in lung squamous cell carcinoma patients.
| Variable | No. of patients
(%) | P-value | Hazard ratio | 95% confidence
interval |
|---|
| Age at surgery
(years) |
| <68 | 53 (51.5) | 0.131 | 1.502 | 0.885–2.548 |
| ≥68 | 50 (48.5) | | | |
| Gender |
| Male | 97 (94.2) | 0.904 | 0.939 | 0.339–2.602 |
| Female | 6 (5.8) | | | |
| Tumor size
(mm) |
| ≤30 | 39 (37.9) | 0.031 | 1.897 | 1.059–3.396 |
| >30 | 64 (62.1) | | | |
| Lymph node
metastasis |
| n(−) | 70 (68.0) | <0.001 | 3.028 | 1.785–5.136 |
| n(+) | 33 (32.0) | | | |
| Lymphatic
invasion |
| ly(0, 1) | 84 (81.6) | <0.001 | 3.298 | 1.827–5.952 |
| ly(2, 3) | 19 (18.4) | | | |
| Venous
invasion |
| v(−) | 53 (51.5) | 0.145 | 1.486 | 0.873–2.530 |
| v(+) | 50 (48.5) | | | |
| Histological
differentiation |
| Well,
moderate | 90 (87.4) | 0.036 | 2.092 | 1.050–4.168 |
| Poor | 13 (12.6) | | | |
| Stromal type |
| Medullary,
intermediate | 70 (68.0) | 0.465 | 1.229 | 0.706–2.139 |
| Scirrhous | 33 (32.0) | | | |
| Infiltrating
pattern |
| INFc(−) | 64 (62.1) | 0.003 | 2.209 | 1.301–3.749 |
| INFc(+) | 39 (37.9) | | | |
| Budding |
| Bud(−) | 49 (47.6) | <0.001 | 3.276 | 1.841–5.827 |
| Bud(+) | 54 (52.4) | | | |
| Table VMultivariate analysis of
clinicopathological features and survival of lung squamous cell
carcinoma patients. |
Table V
Multivariate analysis of
clinicopathological features and survival of lung squamous cell
carcinoma patients.
| Variable | No. of patients
(%) | P-value | Hazard ratio | 95% confidence
interval |
|---|
| Tumor size
(mm) |
| ≤30 | 39 (37.9) | 0.064 | 1.774 | 0.968–3.250 |
| >30 | 64 (62.1) | | | |
| Lymph node
metastasis |
| n(−) | 70 (68.0) | 0.023 | 1.937 | 1.097–3.419 |
| n(+) | 33 (32.0) | | | |
| Budding |
| Bud(−) | 49 (47.6) | 0.001 | 2.766 | 1.497–5.109 |
| Bud(+) | 54 (52.4) | | | |
Discussion
In the present study, we analyzed tumor budding and
the other clinicopathological factors of lung SqCC and clarified
that tumor budding and the INFc(+) type are correlated with the
malignant potential of lung SqCC. Generally, 52% of the SqCC cases
had foci of tumor budding, i.e., the Bud(+) type, and showed higher
rates of lymph node metastasis and a lower overall survival rate. A
previous study reported that tumors with a single-cell invasive
component were a useful prognostic factor for small peripheral SqCC
of the lung, while there was no significant association between
patterns and patient prognosis (27). To the best of our knowledge, the
present study is the first to describe the correlation between
tumor budding and the prognosis of patients with SqCC of the
lung.
Evaluation of the budding grades varies in different
histological types, while it has been strictly defined based on
histological criteria. Frequent budding foci tend to be observed in
adenocarcinoma. In numerous organs, ten budding foci of
adenocarcinoma are set as a cut-off value for high-grade budding
(16,21). By contrast, five budding foci per
high-power field are set as the cut-off value for SqCC (17,19,20).
In this study, we used the actual numbers of budding foci for
histological evaluation since only a few budding foci were found in
the lung SqCC samples. Patient prognoses were significantly
different between the cases with and without budding foci, i.e.,
all or no tumor budding in lung SqCC, while there was no
significant difference among the numbers of budding foci.
Therefore, the presence of budding foci is an important indicator
directly associated with the prognosis of lung SqCC patients.
The conventional INF factors are classified
according to the infiltration patterns and show the entire growth
patterns at the tumor invasive front. However, INF factors do not
extensively demonstrate actual aggressive tumor growth patterns. In
the present study, a close correlation was observed between Bud(+)
and INFc(+) (P<0.001). Bud(+) and INFc(+) are differently
defined, while the two factors reflect local INF of tumor growth.
Therefore, multivariate analysis revealed tumor budding, but not
INF, as a significant indicator of high malignant potential and a
poor patient prognosis.
Several studies have reported several transient
molecular alterations which occur during tumor budding (16,17,19,21,28)
and experimental analyses have demonstrated interactions between
cellular adhesion molecules, including β-catenin, E-cadherin, CD44
and laminin-5γ2, and tumor budding in colorectal carcinoma
(29,30). Previously, other studies reported
that the overexpression of laminin-5γ2 is a significant prognostic
factor in lung adenocarcinoma (21,30).
However, there have been no immunohistochemical/molecular
examinations using lung SqCC cases. Therefore, we plan to perform
studies to clarify the pathological mechanisms of budding formation
in lung SqCC using immunohistochemical/molecular analyses in the
future.
In conclusion, tumor budding, i.e., the Bud(+) type,
of lung SqCC shows locally aggressive growth and is a useful
indicator of the lymph node status and prognosis.
References
|
1
|
Ferlay J, Shin HR, Bray F, Forman D,
Mathers C and Parkin DM: Estimates of worldwide burden of cancer in
2008: GLOBOCAN 2008. Int J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Beadsmoore CJ and Screation NJ:
Classification, staging and prognosis of lung cancer. Eur J Radiol.
45:8–17. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Goldstraw P, Crowley J, Chansky KJ, et al:
The IASLC Lung Cancer Staging Project: proposals for the revision
of the TNM stage groupings in the forthcoming (seventh) edition of
the TNM classification of malignant tumours. Thorac Oncol.
2:706–714. 2007. View Article : Google Scholar
|
|
4
|
Marchesani W: Über den primären
Bronchialkrebs. Frankf Z Path. 30:158–190. 1924.(In German).
|
|
5
|
Kayser K, Bauer A, David H and Kayser G:
Historical aspects of pulmonary pathology with specific emphasis on
ancient reports. Electronic Journal of Pathology and Histology.
9.2:32–37. 2003.
|
|
6
|
Travis WD, Brambilla E, Müller-Hermelin HK
and Harris CC; World Health Organization Classification of Tumours.
Pathology and Genetics. Tumours of the Lung, Pleura, Thymus and
Heart. IARC Press; Lyon: 2004
|
|
7
|
Hong J, Kyung SY, Lee SP, et al:
Pemetrexed versus gefitinib versus erlotinib in previously treated
patients with non-small cell lung cancer. Korean J Intern Med.
25:294–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rossi A, Ricciardi S, Maione P, de Marinis
F and Gridelli C: Pemetrexed in the treatment of advanced
non-squamous lung cancer. Lung Cancer. 66:141–149. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sandler A, Gray R, Perry MC, et al:
Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell
lung cancer. N Engl J Med. 355:2542–2550. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Reck M, von Pawel J, Zatloukal P, et al:
Phase III trial of cisplatin plus gemcitabine with either placebo
or bevacizumab as first-line therapy for nonsquamous non-small-cell
lung cancer: AVAil. J Clin Oncol. 27:1227–1234. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rosell R, Perez-Roca L, Sanchez JJ, et al:
Customized treatment in non-small-cell lung cancer based on EGFR
mutations and BRCA1 mRNA expression. PLoS One. 4:e51332009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Okada K, Kijima H, Imaizumi T, et al:
Wall-invasion pattern correlates with survival of patients with
gallbladder adenocarcinoma. Anticancer Res. 29:685–691.
2009.PubMed/NCBI
|
|
13
|
Song KY, Hur H, Jung CK, et al: Impact of
tumor infiltration pattern into the surrounding tissue on prognosis
of the subserosal gastric cancer (pT2b). Eur J Surg Oncol.
36:563–567. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kong KY, Park JY, Kim DY, et al:
Prognostic significance of stromal microinvasion in the intestinal
type of ovarian mucinous adenocarcinoma. Ann Surg Oncol.
18:3462–3468. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Morodomi T, Isomoto H, Shirouzu K,
Kakegawa K, Irie K and Morimatsu M: An index for estimating the
probability of lymph node metastasis in rectal cancers. Lymph node
metastasis and the histopathology of actively invasive regions of
cancer. Cancer. 63:539–543. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ueno H, Murphy J, Jass JR, Mochizuki H and
Talbot IC: Tumour ‘budding’ as an index to estimate the potential
of aggressiveness in rectal cancer. Histopathology. 40:127–132.
2002.
|
|
17
|
Nakanishi Y, Ohara M, Doumen H, Kimura N,
Ishidate T and Kondo S: Correlation between tumor budding and
post-resection prognosis in patients with invasive squamous cell
carcinoma of the thoracic esophagus. World J Surg. 35:349–356.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ohike N, Coban I, Kim GE, et al: Tumor
budding as a strong prognostic indicator in invasive ampullary
adenocarcinomas. Am J Surg Pathol. 34:1417–1424. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang C, Huang H, Huang Z, et al: Tumor
budding correlates with poor prognosis and epithelial-mesenchymal
transition in tongue squamous cell carcinoma. J Oral Pathol Med.
40:545–551. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sarioglu S, Acara C, Akman FC, et al:
Tumor budding as a prognostic marker in laryngeal carcinoma. Pathol
Res Pract. 206:88–92. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yamaguchi Y, Ishii G, Kojima M, et al:
Histopathologic features of the tumor budding in adenocarcinoma of
the lung: tumor budding as an index to predict the potential
aggressiveness. J Thorac Oncol. 5:1361–1368. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM Classification of Malignant Tumors. 7th edition. Wiley;
Hoboken, NJ: 2009
|
|
23
|
Japanese Gastric Cancer Association.
Japanese Classification of Gastric Carcinoma - 2nd English Edition.
Gastric Cancer. 1:10–24. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Maehara Y, Oshiro T, Adachi Y, Ohno S,
Akazawa K and Sugimachi K: Growth pattern and prognosis of gastric
cancer invading the subserosa. J Surg Oncol. 55:203–208. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Haraguchi M, Yamamoto M, Saito A, et al:
Prognostic value of depth and pattern of stomach wall invasion in
patients with an advanced gastric carcinoma. Semin Surg Oncol.
10:125–129. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hase K, Shatney C, Johnson D, Trollope M
and Vierra M: Prognostic value of tumor ‘budding’ in patients with
colorectal cancer. Dis Colon Rectum. 36:627–635. 1993.
|
|
27
|
Maeshima AM, Maeshima A, Asamura H and
Matsuno Y: Histologic prognostic factors for small-sized squamous
cell carcinomas of the peripheral lung. Lung Cancer. 52:53–58.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Prall F: Tumour budding in colorectal
carcinoma. Histopathology. 50:151–162. 2007. View Article : Google Scholar
|
|
29
|
Shinto E, Tsuda H, Ueno H, et al:
Prognostic implication of laminin-5 gamma 2 chain expression in the
invasive front of colorectal cancers, disclosed by area-specific
four-point tissue microaarays. Lab Invest. 85:257–266. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Moriya Y, Niki T, Yamada T, Matsuno T,
Kondo H and Hirohashi S: Increased expression of laminin-5 and its
prognostic significance in lung adenocarcinomas of small size. An
immunohistochemical analysis of 102 cases. Cancer. 91:1129–1141.
2001. View Article : Google Scholar : PubMed/NCBI
|