Introduction
Colorectal carcinoma is the third most prevalent
type of cancer in adults, which has an incidence rate that
increases with age (1). Colorectal
carcinoma rarely occurs in children, with an incidence rate of
between 1 and 8 cases per million children worldwide (2). Therefore, pediatricians and pediatric
surgeons are not familiar with colorectal carcinoma in children and
its clinical manifestation are different from those in adults
(3). Colorectal carcinoma may be
detected by digital rectal examination, sigmoidoscopy or
colonoscopy. Furthermore, contrast studies, ultrasonography and
computed tomography are essential procedures for determining the
extent of the disease. Postoperative histological examination is
considered the gold standard for diagnosis. Colorectal carcinoma in
children may occur at any age, however, the majority of cases are
identified in older children; 70–95% of cases occur in children
>10 years of age (2,4–6). The
present study reports the case of colorectal carcinoma, diagnosed
as signet-ring cell carcinoma, in a 9-year-old boy.
Case report
A 9-year-old boy with no history of medical illness
was presented to the emergency department of the Children's
Hospital of Fudan University (Shanghai, China) with primary
complaints of abdominal pain, which had persisted for 1 day. This
was preceded by intermittent vomiting 5 days prior to admission,
which was treated as an intestinal obstruction in a local health
center. Family history revealed nothing of significance. On
admission, the patient appeared irritable and in distress due to
pain. Physical examination revealed abdominal distension and
tenderness in the upper abdomen with positive bowel sounds;
however, muscle tension was not palpated.
Initial laboratory tests revealed the following:
White cell count, 6,900/µl with 62.8% neutrophils; C-reactive
protein, 66 mg/l; hemoglobin, 116.0 g/l; urea, 3.10 mmol/l; serum
creatinine, 28.0 µmol/l; sodium, 136 mmol/l; potassium, 3.7 mmol/l;
glutamic-pyruvic transaminase, 5 IU/l; glutamic oxalacetic
transaminase, 11 IU/l; and albumin, 41 g/l. Urinalysis results were
normal. Abdomen X-ray revealed an incomplete obstruction of the
upper section of the colon.
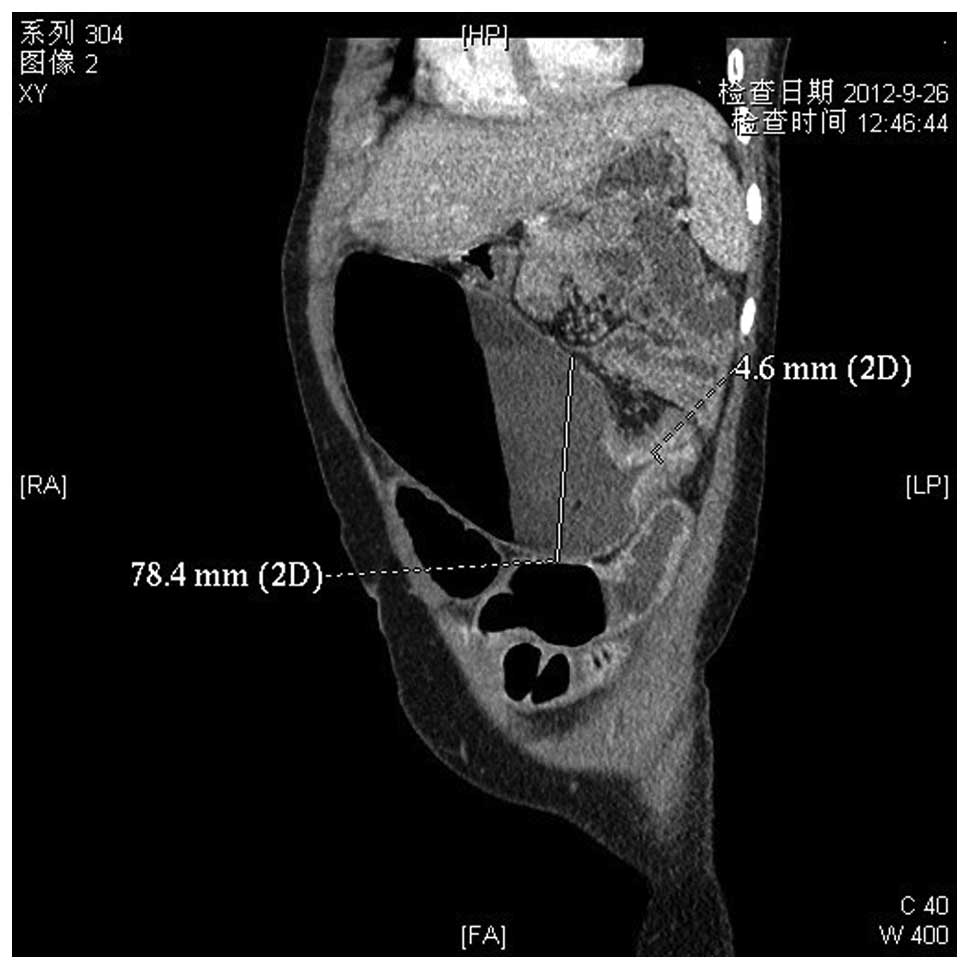
The patient was treated with a third-generation
cephalosporin and fluid infusion, accompanied by fasting and
gastrointestinal decompression. Following 3 days of treatment, the
intestinal obstruction was not relieved. A further abdominal
enhanced computed tomography (CT) scan depicted significant
stenosis in the transverse colon proximal to the splenic flexure,
with local bowel wall thickening; therefore, an occupying lesion
could not be excluded (Fig. 1). An
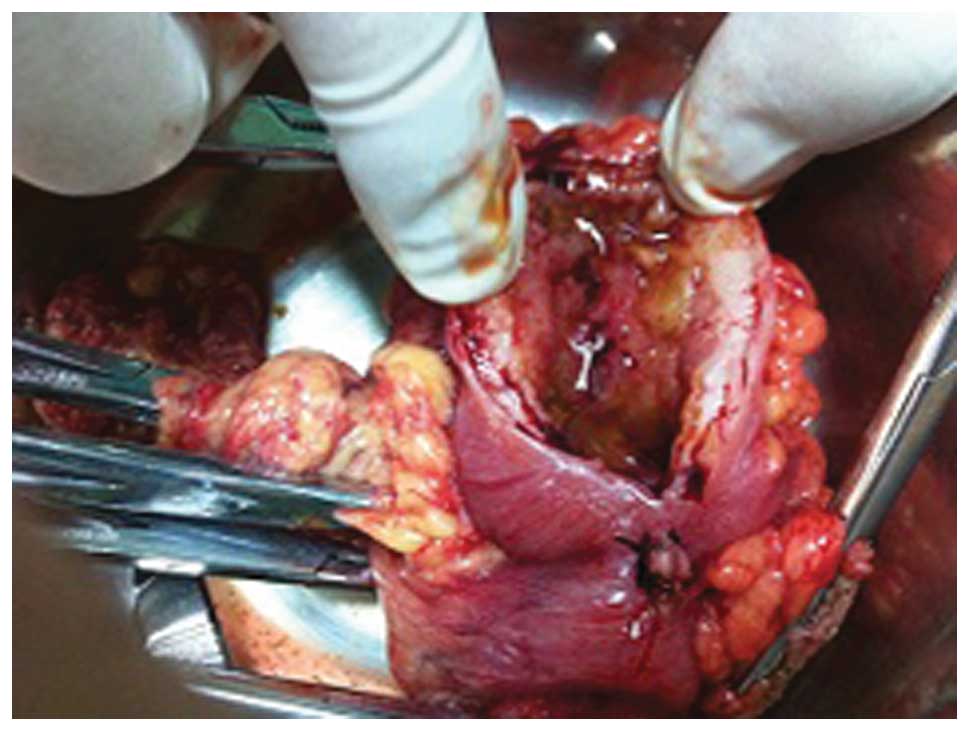
emergency laparotomy was performed in order to diagnose the mass.
During surgery, a mass measuring 4×4 cm was identified in the
transverse colon proximal to the splenic flexure (Fig. 2), which formed a near complete
obstruction of the enteric cavity. The proximate colon was notably
expanded (maximum diameter, ~10 cm) and the distant colon was
narrow (diameter, ~4 cm). Following proximate bowel decompression,
the retroperitoneal lymphaden and liver were explored, although no
abnormalities were observed. The transverse colon where the mass
was located was excised (5 cm surgical margin around the tumor) and
a single lumen stoma was performed at the proximate end. Due to
insufficient bowel preparation for the emergency operation, I-stage
anastomosis was at great risk of postoperative infection and
leaking. Lymph node dissection was not performed because a
diagnosis of colorectal carcinoma had not been considered.
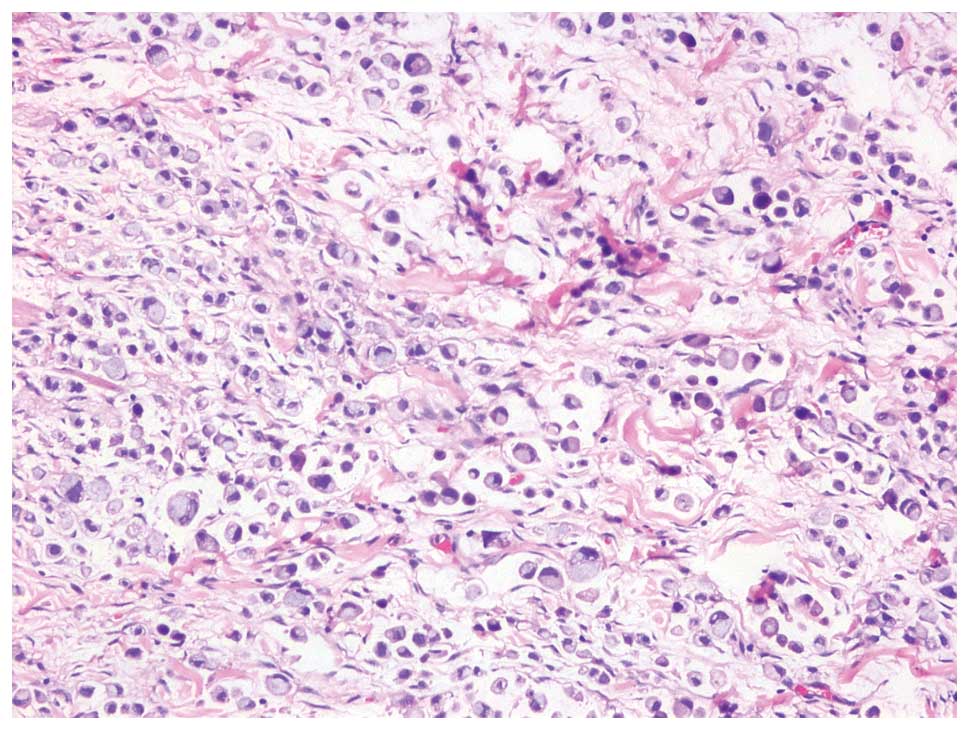
Histological examination of the mass revealed signet-ring cell
carcinoma, encroaching the intestinal canal (Fig. 3). Further laboratory tests revealed
the following: Cancer antigen (CA)125 expression, 85.4 IU/ml
(reference, <35 IU/ml); CA19-9 expression, 12.9 U/ml (reference,
<37 U/ml); and carcinoembryonic antigen (CEA) expression, 0.9
ng/ml (reference, <5.0 ng/ml). Abdomen ultrasonography as well
as cephalic, chest and abdomen CT scans and bone scintigraphy
demonstrated no metastases. The stage of tumor was determined to be
Tumor3NodexMetastasis0 and Duke's
stage B or C (7). Lymphadenectomy and
postoperative adjuvant chemotherapy were planned to be perform.
However, the patient's parents objected to therapy and the patient
was discharged 2 weeks following surgery.
The patient underwent chemotherapy 7 times in
another hospital for one year following surgery. Following one
year, the patient returned to the Children's Hospital of Fudan
University in order to close the stoma. The patient underwent
re-operation, during which a mesenteric lymph node metastasis was
identified. An abdominal CT follow-up revealed mesenteric lymph
node metastasis and CEA expression had risen to 87.0 ng/ml
(reference, <5.0 ng/ml). The patient succumbed to the disease at
2 weeks following discharge from hospital; cephalic CT scans
revealed metastases.
Discussion
Signet-ring cell carcinoma, a type of colorectal
carcinoma, is scarcely diagnosed in children. Sultan et al
(3) reported that signet-ring cell
carcinoma accounted for 18% of colorectal carcinomas in children
and adolescents.
Adult cases of colorectal cancer usually present
with manifestations that include abdominal pain, hematochezia,
difficult defecation and attenuated stool (8). However, in children it is difficult to
decipher their primary complaint and neoplastic lesions are
generally more severe when examined by a physician due to parents'
negligence. Patients commonly present with advanced intestinal
obstruction symptoms on admission, as in the current case report.
Early symptoms of the current patient included intermittent
vomiting and abdominal pain, and the diagnosis was determined by an
emergency surgery, during which the intestinal obstruction became
obvious. Therefore, the possibility of a tumor should be considered
for every child admitted to hospital with intestinal obstruction
symptoms, incurable abdominal pain or changed bowel evacuation
habits. B-mode ultrasound or enhanced CT contribute to the early
identification of colorectal carcinoma; however, the principal
method of colorectal carcinoma diagnosis is colonoscopy, with an
accuracy of 90–95% (9). Final
diagnosis is dependent on pathological examination. CEA is a
reference index of auxiliary diagnosis and relapse monitoring,
though it has no tumor specificity.
Signet-ring cell carcinoma has an aggressive
clinical course and a high lymphatic metastasis rate; it is known
to metastasize early and 60–100% of children are at advanced stage
on admission, stage C or D according to Dukes staging (7). Radical surgery is the preferred
treatment for signet-ring cell carcinoma, even for patients of
advanced stages. In addition, signet-ring cell carcinoma first
metastasizes to para-intestinal lymph nodes and the range of
metastasis is ~10 cm from the tumor (10).
As signet-ring cell carcinoma rarely occurs in
children, frozen pathological examinations should be performed for
highly suspect malignant tumors. In addition, the intestinal
incisal edge should be >10 cm away from the tumor at initial
surgery in order to help prevent metastasis. As it is rare for
signet-ring cell carcinoma to be identified in patients with
intestinal obstruction manifestations during surgery, preoperative
overall examinations and bowel preparation are insufficient.
Therefore it is a dilemma whether to choose palliative or radical
resection when tumors are discovered during surgery. In the present
case study, palliative fistulation was performed at the initial
exploratory laparotomy due to insufficient preoperative bowel
preparation and high risk of primary inosculation.
Postoperative chemotherapy is indispensable to
colorectal carcinoma; at present, adjuvant chemotherapy with
5-fluorouracil is generally accepted, in particular for stage III
or IV patients, as it has been found to reduce the rate of relapse
and increase survival rates (11).
Postoperative radiotherapy is unable to increase the survival rate
of patients with tumors that are difficult to completely resect;
however, palliative radiotherapy may effectively relieve the
clinical symptoms of metastasized lesions (12).
In conclusion, colorectal carcinomas in children are
rare and provide a lack of typical clinical symptoms and
radiological data, as demonstrated in the present case study. In
addition, the clinical symptoms are often undervalued by parents
and doctors; this therefore results in poor prognosis of advanced
stage tumors, when diagnosed. It is therefore suggested that
malignancies should be considered by pediatricians and pediatric
surgeons for differential diagnosis when patients present with
intestinal obstruction symptoms, incurable abdominal pain or
changed bowel evacuation habits, as early diagnosis and treatment
decreases the mortality rate of patients. This is of particular
importance for signet-ring cell carcinoma of the colon or rectum,
as it has a poor prognosis at advanced stages.
References
|
1
|
Jemal A, Siegel R, Ward E, Hao Y, Xu J and
Thun MJ: Cancer statistics, 2009. CA Cancer J Clin. 59:225–249.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yang R, Cheung MC, Zhuge Y, Armstrong C,
Koniaris LG and Sola JE: Primary solid tumors of the colon and
rectum in the pediatric patient: A review of 270 cases. J Surg Res.
161:209–216. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sultan I, Rodriguez-Galindo C, El-Taani H,
et al: Distinct features of colorectal cancer in children and
adolescents: A population-based study of 159 cases. Cancer.
116:758–765. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Brown RA, Rode H, Millar AJ,
Sinclair-Smith C and Cywes S: Colorectal carcinoma in children. J
Pediatr Surg. 27:919–921. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Karnak I, Ciftci AO, Senocak ME and
Büyükpamukçu N: Colorectal carcinoma in children. J Pediatr Surg.
34:1499–1504. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vastyan AM, Walker J, Pintér AB, Gerrard M
and Kajtar P: Colorectal carcinoma in children and adolescents - a
report of seven cases. Eur J Pediatr Surg. 11:338–341. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Radhakrishnan CN and Bruce J: Colorectal
cancers in children without any predisposing factors. A report of
eight cases and review of the literature. Eur J Pediatr Surg.
13:66–68. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hill DA, Furman WL, Billups CA, et al:
Colorectal carcinoma in childhood and adolescence: A
clinicopathologic review. J Clin Oncol. 25:5808–5814. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Beck DE: Colorectal cancer screening. Clin
Colorectal Surg. 14:1152001.
|
|
10
|
Schumacher P, Dineen S, Barnett C Jr,
Fleming J and Anthony T: The metastatic lymph node ratio predicts
survival in colon cancer. Am J Surg. 194:827–832; discussion,
831–832. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Goldberg RM: N9741: A phase III study
comparing irinotecan to oxaliplatin-containing regimens in advanced
colorectal cancer. Clin Colorectal Cancer. 2:812002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Labianca R, Beretta G, Gatta G, De Braud F
and Wils J: Colon cancer. Crit Rev Oncol Hematol. 51:145–170. 2004.
View Article : Google Scholar : PubMed/NCBI
|