Introduction
Thymomas are unique neoplasms that originate in the
epithelial tissue of the thymus (1).
The prevalence of thymomas is equal in males and females, and the
age at diagnosis is typically 30–40 years, however, cases have been
described in all age groups, including rare occurrences in children
(1). In adults, thymoma accounts for
20% of anterior mediastinal neoplasms, and it is thus the most
common neoplasm of the anterior mediastinum (2). Thymomas are typically detected during
routine radiographs and in myasthenia gravis patients, ~15% of whom
are affected (1,2). These tumors are commonly associated with
indolent growth and with a variety of paraneoplastic syndromes,
most frequently myasthenia gravis (3). Approximately one-third of thymoma
patients exhibit superior vena cava syndrome, coughing, chest pain
or dysphagia; these symptoms result from compression of the
surrounding organs by an expansive mass (1). Surgery is the predominant treatment
method for thymoma. However, if there is indication that the tumor
is large and invasive, pre-operative neoadjuvant chemotherapy
and/or radiotherapy may be administered in order to reduce the size
of the mass and to improve resectability prior to surgery (1). Stage III and IV thymomas have a markedly
poorer prognosis compared with stage I and II tumors. Metastasis of
invasive thymomas may also occur, however, this is uncommon. Sites
of metastasis generally include the pleura, bones, liver or brain,
occurring in ~7% of cases (1).
Non-traumatic hemothorax is a rare condition, which
generally occurs due to the erosion of a vessel caused by a
pathological lesion. In tuberculosis of the lung, the pulmonary
arteries or their branches are the vessels generally involved
(4). The present study reports a rare
case of hemothorax caused by a ruptured thymoma, which necessitated
urgent surgery.
Case report
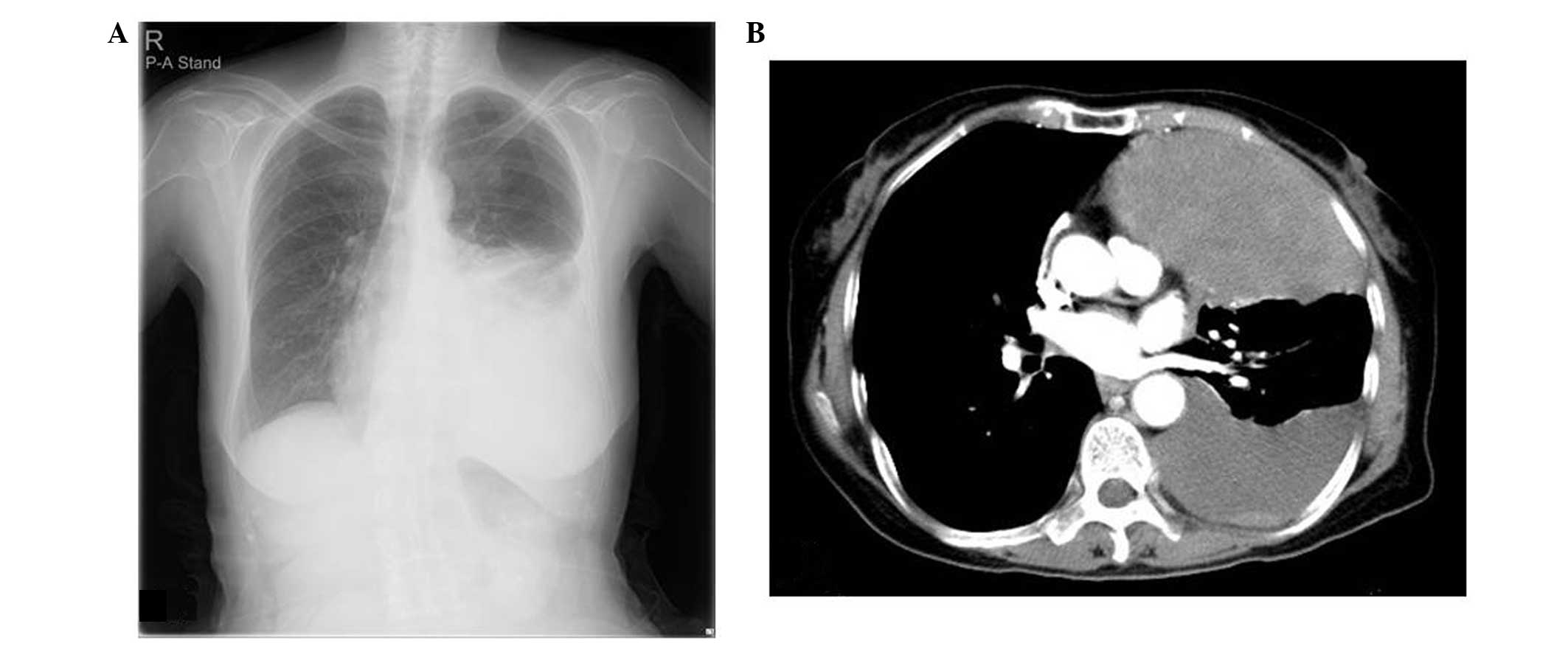
A 77-year-old, previously healthy female was
referred to Kobe University Hospital (Kobe, Hyōgo, Japan) hospital
with an acute onset of chest pain in December, 2012. Chest
roentgenography and computed tomography revealed a mass occupying
the anterior mediastinum and left hemithorax, a left-sided pleural
effusion, and a normal aorta and great vessels (Fig. 1). Progressive anemia was noted
following admission. A diagnosis of a left hemothorax caused by
rupture of the anterior mediastinal mass was suspected, and
emergency surgery was conducted. Upon opening the left pleural
cavity, ~1,350 ml of blood was released. An anterolateral
thoracotomy was performed by video-assisted thoracoscopic surgery,
revealing a large, encysted hematoma along the tumor (72×43×43 mm),
extending from the left anterior mediastinum into the left pleural
cavity and ending with a rupture. Hemorrhage on the cut surface of
the tumor was observed (Fig. 2A and
B). An analysis of frozen sections using hematoxylin and eosin
staining (Sakura Finetek Nihonbashi-Hamacho, Tokyo, Japan) revealed
a hemorrhagic lesion with lymphocytic infiltration and epithelial
elements, indicative of thymoma, and a thymo-partial thymectomy was
subsequently performed, removing the maximal possible volume of
hematoma. The thymoma was completely resected en bloc with part of
the left upper lobe of the thymus (Fig.
2C). A pathological examination revealed that the tissue was
composed of broad fibrous bands separating proliferating epithelial
cells (highlighted by cytokeratin AE1/AE3 immunostaining) admixed
with small lymphoid cells, indicating a diagnosis of
lymphocyte-rich (type B1) thymoma (World Health Organization
classification) (5,6) (Fig. 2D).
The tumor showed hemorrhage and rupture, and no capsular invasion
(Masaoka stage 2), and was continuous with the hematoma resulting
from partial destruction of its epithelial lining (1). In addition, coagula and fibrin calculi
contained tissue from the thymoma, and a diagnosis of hemothorax
formation due to hemorrhage from the ruptured thymoma was
determined. The patient was discharged on post-operative day 13
following an uneventful recovery, and was in good health at the
six-month follow-up examination.
Written informed consent for the present study was
obtained from the patient.
Discussion
The rupture of mediastinal teratomas has been
recognized as a cause of chest pain and massive pleural effusion
(7,8);
however, the rupture of thymomas is rare. To the best of our
knowledge, only six cases, including the present case, of ruptured
thymic tumor have been reported. Caplin et al (9) reported a case of a hemothorax resulting
from the spontaneous rupture of a thymoma in a 51-year-old male who
underwent treatment by posterolateral thoracotomy. Templeton et
al (10) reported a case of
hemothorax due to rupture of a thymoma simulating aortic dissection
in a 63-year-old male; only a biopsy was performed in this case.
Fukuse et al (11) reported a
case of mediastinal hematoma due to thymomal hemorrhage in a
70-year-old male who was treated by full median sternotomy with
anterolateral thoracotomy. Shimokawa et al (12) reported a case of mediastinal
hemorrhage and hemothorax due to rupture of a thymoma in a
71-year-old female who subsequently underwent partial sternotomy
with hemitransection of the sternum to the left fourth intercostal
space. Santoprete et al (13)
reported a case of mediastinal hemorrhage and hemothorax due to
rupture of a thymoma in a 73-year-old female who underwent
treatment by clamshell incision. In these six cases, including the
present case, sudden onset of dyspnea and chest pain were the first
clinical manifestations and all patients were healthy prior to
onset.
In the present case, controlling the left pulmonary
hilar vessels and evacuating the hematoma were priorities.
Anterolateral thoracotomy with video-assisted thoracoscopic surgery
enabled access to the mediastinum and pleural cavities, and rapid
control of the tumor. The present case, as well as other previously
reported cases, illustrates that sudden-onset dyspnea and chest
pain in a previously healthy individual, which co-occurs with acute
mediastinal widening on chest roentgenography, may be indicative of
ruptured thymoma.
References
|
1
|
Thomas CR, Wright CD and Loehrer PJ:
Thymoma: State of the art. J Clin Oncol. 17:2280–2289.
1999.PubMed/NCBI
|
|
2
|
Gerein AN, Srivastava SP and Burgess J:
Thymoma: A ten year review. Am J Surg. 136:49–53. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Loehrer PJ Sr, Jiroutek M, Aisner S,
Aisner J, Green M, Thomas CR Jr, Livingston R and Johnson DH:
Combined etoposide, ifosfamide, and cisplatin in the treatment of
patients with advanced thymoma and thymic carcinoma: An intergroup
trial. Cancer. 91:2010–2015. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Janik M, Straka L, Krajcovic J, et al:
Non-traumatic and spontaneous hemothorax in the setting of forensic
medical examination: A systematic literature survey. Forensic Sci
Int. 236:22–29. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rosai J and Sobin LH: World Health
Organization. International Histological Classification of Tumours:
Histological Typing of Tumours of the Thymus. 2nd. Springer-Verlag
Berlin Heidelberg; Germany: 1999
|
|
6
|
Okumura M, Ohta M, Tateyama H, et al: The
World Health Organization histologic classification system reflects
the oncologic behavior of thymoma: A clinical study of 273
patients. Cancer. 94:624–632. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Choi SJ, Lee JS, Song KS and Lim TH:
Mediastinal teratoma: CT differentiation of ruptured and unruptured
tumors. AJR Am J Roentogenol. 171:591–594. 1998. View Article : Google Scholar
|
|
8
|
Sasaka K, Kurihara Y, Nakajima Y, et al:
Spontaneous rupture: A complication of benign mature teratomas of
the mediastinum. AJR Am J Roentogenol. 170:323–328. 1998.
View Article : Google Scholar
|
|
9
|
Caplin JL, Gullan RW, Dymond DS, Bradley
SMO, Hill IM and Banim SO: Hemothorax due to rupture of a benign
thymoma. Jpn Heart J. 26:123–125. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Templeton PA, Vainright JR, Rodriguez A
and Diaconis JN: Mediastinal tumors presenting as spontaneous
hemothorax, simulating aortic dissection. Chest. 93:828–830. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fukuse T, Matsukura T, Nakamura A, Kosaka
S and Tamada J: Mediastinal hematoma due to thymoma hemorrhage - A
case report. Nihon Kyobu Geka Gakkai Zasshi. 39:930–934. 1991.(In
Japanese). PubMed/NCBI
|
|
12
|
Shimokawa S, Watanabe S, Sakasegawa K and
Tani A: Ruptured thymoma causing mediastinal hemorrhage resected
via partial sternotomy. Ann Thorac Surg. 71:370–372. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Santoprete S, Ragusa M, Urbani M and Puma
F: Shock induced by spontaneous rupture of a giant thymoma. Ann
Thorac Surg. 83:1526–1528. 2007. View Article : Google Scholar : PubMed/NCBI
|