Introduction
Carcinoma of unknown primary site (CUP) is defined
as metastatic cancer that is present in the absence of an
identifiable primary tumor site, even following thorough clinical
examinations and diagnostic studies. CUP is a heterogeneous group
of nosological entities based on histological, clinical,
therapeutic and prognostic characteristics, and accounts for 3–5%
of all malignancies. According to its histopathological
characteristics, CUP can be classified into four major subtypes:
well- or moderately-differentiated adenocarcinomas;
undifferentiated or poorly-differentiated adenocarcinomas or
carcinomas; squamous cell carcinomas (SCC); and undifferentiated
neoplasms. SCC accounts for 15% of CUP, conferring a poor
prognosis, with a median survival time of only 6–9 months (1,2), and these
patients are usually treated with aggressive multimodal therapy
similar to patients with locally advanced head and neck cancer. The
present study describes a case of SC CUP with abdominal wall
lesions as the primary symptom, 3 months after laparoscopic
unilateral left salpingo-oophorectomy.
Case report
In March 2013, a 54-year-old female (gravida 2, para
1) presented with a left ovarian cyst measuring 7 cm during a
regular medical examination in a local hospital. There was no
history of loss of appetite, weight loss or any other bladder- or
bowel-associated symptoms. A clinical evaluation was made with
regard to ultrasound and serological markers. Ultrasound
examination showed a left ovarian cyst of 7×6×5 cm, with a normal
uterus, right ovary and fallopian tubes. The serum level of
carbohydrate antigen 19-9 (CA19-9) was above normal at 94.4 U/ml
(reference range, 0–35.0 U/ml). Cancer antigen 125 (CA125), SCC
antigen (SCC-Ag), α-fetoprotein (AFP), carcinoembryonic antigen
(CEA) and neuron-specific enolase (NSE) levels were all within the
normal ranges. A provisional diagnosis of an ovarian endometrioid
cyst was made.
The patient underwent a laparoscopic unilateral left
salpingo-oophorectomy. The left ovarian mass, adhering to the broad
ligament, was removed along with the fallopian tube. The cyst broke
upon separating the adhesion and ‘chocolate-like’ fluid flowed into
the pelvic cavity. The cyst wall was removed through the
laparoscopic puncture hole on the right abdominal wall. There were
no other abnormalities in the abdominal cavity, which was irrigated
with normal saline several times prior to closure.
Histopathological analysis identified the mass as an endometrioid
cyst.
The patient reported pain from the right laparoscopy
puncture site at 3 months post-surgery. A 6.2×3.3-cm subcutaneous
nodule was found by computed tomography (CT) imaging (Fig. 1). Furthermore, the serum CA19-9 level
was level further increased at 113.5 U/ml. The CA125, SCC-Ag, AFP,
CEA and NSE levels remained within the normal reference ranges. A
wide surgical excision of the lesion with safety margins was
performed and the abdominal wall was repaired with a reinforcing
polypropylene mesh on September 2, 2013. Histopathologically, the
surgical specimen contained a metastatic well-differentiated SCC
with the following immunohistochemical staining results: p63(++),
cytokeratin (CK)5/6(++), CK7(partially+), CK20(−), high molecular
weight CK(++) and E-cad(+), with a Ki-67 of 10% (Fig. 2).
Due to the malignant nature of the disease, the
patient was admitted at the Zhejiang Cancer Hospital (Hangzhou,
China) for immediate further treatment on October 15, 2013. The
first aim was to identify the primary site using a human papilloma
virus test, cervical biopsy, gastroscopy examination and
laryngoscopic examination, all of which were negative. Histological
materials that were prepared at the time of the first surgery were
examined section by section, and were all found to be without
malignancy. Positron emission tomography (PET)/CT imaging was
performed and revealed hypermetabolic lesions in the right pelvic
cavity (tumor size, 4.3×2.6 cm) and right inguinal lymph node
(tumor size, 0.5×0.9 cm). A biopsy of this inguinal lymph node
revealed moderately-differentiated metastatic SCC (Fig. 3). The final treatment decision
following a multidisciplinary discussion was to perform a
laparotomy with a hysterectomy, right salpingo-oophorectomy,
omentectomy, pelvic lymph node excision and multiple biopsies of
the peritoneum. The surgical exploration found no ascites, a normal
right ovary, a normal appendix, and a twisted and thickened right
Fallopian tube adhering to the right ureter and rectal wall. A hard
nodule ~3 cm in diameter was present on the left laparoscopy
puncture site and left uterine broad ligament area, respectively.
The nodule on the left uterine broad ligament area formed a compact
adhesion to the rectum and left ureter.
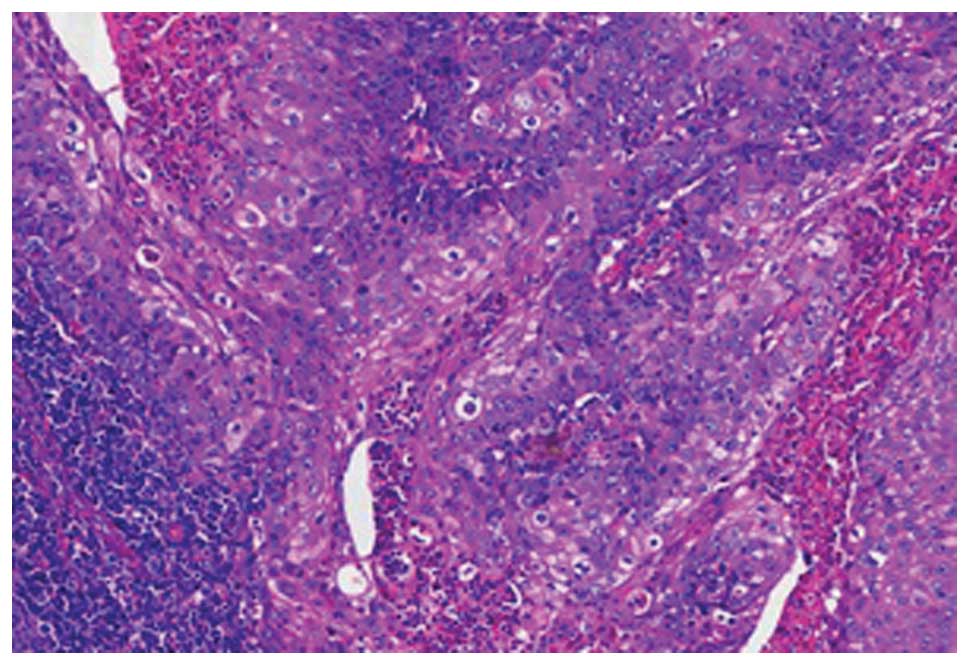
Immunohistochemical analysis showed
poorly-differentiated invasive or metastatic SCC in the left broad
ligament, the pouch of Douglas and the left lower abdominal wall
(Fig. 4), which stained positive for
the SC markers CK5/6 and p63, slightly positive for the glandular
epithelial cell marker CK7, and was negative for CK20. The right
ovary, right Fallopian tube and pelvic lymph nodes were free of
tumor.
Following the surgery, the patient received
chemotherapy every 3 weeks for ~6 months. The first chemotherapy
cycle was with cisplatin/Taxol (cisplatin, 70 mg/m2;
Taxol, 150 mg/m2), which was followed by 7 cycles of
carboplatin/Taxol (carboplatin, AUC = 5; Taxol, 150
mg/m2) due to severe vomiting. During chemotherapy, the
serum levels of CA19-9 declined to 18.2 U/ml until the eighth
cycle. Pelvic CT imaging showed recurrence in the right pelvic
cavity, dilatation of the right ureter and right hydronephrosis.
Following the ureteroneocystostomy, the patient was planned to
receive palliative pelvic external irradiation with a total dose of
45 Gy in 25 fractions, 5 days per week, to eradicate any pelvic
residual disease. However, liver metastasis and pelvic progression
(Fig. 5), which caused intestinal
obstruction, were found after radiotherapy with 10.8 Gy in 6
fractions, and a transverse colostomy was performed. Supportive
care, rather than radiotherapy, was provided. After 1 month, the
patient succumbed to intestinal bleeding, thrombocytopenia and
multiple organ failure.
Discussion
CUP are defined as a histologically proven
metastatic malignant tumors with a poor prognosis, whose primary
site cannot be identified following a thorough pre-treatment workup
(3). CUP is the seventh most
prevalent cancer in the world and the fourth most common cause of
cancer-associated mortality in males and females. Among all
malignancies, CUP, with a variety of biological characteristics,
accounts for 3–5%; ~50% of which are diagnosed as well- to
moderately-differentiated metastatic adenocarcinoma, 30% as
undifferentiated or poorly-differentiated carcinoma, 15% as SCC and
the remaining 5% as undifferentiated neoplasms (4). For SC CUP, the axillary lymph nodes,
inguinal lymph nodes, mediastinum and bone are the most common
sites of occurrence. The present study reported a rare case of SC
CUP with abdominal wall lesions as a primary symptom.
Prior to reaching a diagnosis of CUP, various
examinations are required in order to identify the primary site.
These examinations should include a detailed medical history, a
complete physical examination, including pelvic and rectal
examinations, a full blood count and biochemistry analysis, a
urinalysis and stool occult blood testing, a histopathological
review of any biopsy material using immunohistochemistry, chest
radiography, CT imaging of the abdomen and pelvis, and in certain
cases, mammography (4,5). In the present case, the patient
underwent a laparoscopic left salpingo-oophorectomy 3 months
previously, therefore the pathological material obtained was
examined section by section using immunohistochemistry to exclude
an ovarian origin. In addition, HPV testing, cervical biopsy,
gastroscopy and laryngoscopy were performed, all of which were
negative. Whole-body fludeoxyglucose-PET/CT imaging has been proven
to be useful not only in search for the primary focus, but also for
metastases in patients with CUP (1,4,6). Therefore, in order to locate the primary
origin, and determine the number of metastases and their locations,
the patient in the present study received a PET/CT scan, which
demonstrated hypermetabolic lesions in the right pelvic cavity
(tumor size, 4.3×2.6 cm) and right inguinal lymph node (tumor size,
0.5×0.9 cm). Histopathological examination of the lymph node
revealed moderately-differentiated metastatic SCC.
Routine evaluation of commonly used epithelial serum
tumor markers, including CA19-9, CA125, SCC-Ag and CEA, usually
have no diagnostic value in identifying the primary site (1,4); however,
these markers could be used to predict recurrence and metastasis.
In the present case, the pre-operative serum CA19-9 level was
elevated at 94.4 U/ml, while the levels of SCC-Ag, CA125, AFP, CEA
and NSE were all within the normal reference ranges. During the
course of therapy, the serum CA19-9 level was monitored closely;
the level decreased to a minimum of 18.2 U/ml and began to rise
when the disease progressed and spread to other organs, with a
maximum level of 211.1 U/ml. In this case, CA19-9 was an important
marker for monitoring tumor recurrence and could be used to
evaluate the response to chemotherapy treatment.
CUP remains an extremely aggressive disease with a
poor prognosis. The median survival time is between 4 and 12 months
(4,7–10), and the
5-year survival rate is <10% (11). Tamam et al (6) recorded a median survival time of 9
months for patients with CUP, with a life expectancy between 5 and
25 months, while Fehri et al (8) stated that the median survival time was 7
months. In the present study, the tumor progressed rapidly and
metastasized to the liver in a short period of time, and the
patient succumbed to fever, electrolyte disturbance and
malnutrition at 10 months post-diagnosis.
Treatment regimens differ according to the location
of the tumor. Although chemotherapy has a role in the treatment of
CUP, no regimen has been established as a standard first-line
therapy (12). The majority of
clinical studies have shown good response rates of 32–55% for
cisplatin-based regimens in patients with CUP. According to
Nishimori et al (13),
cisplatin/docetaxel chemotherapy was shown to be effective with
tolerable toxicity in patients with CUP. The overall response rate
was 62.5% and the median disease-free survival time was 8.7 months.
The 1-year overall survival (OS) rate was 68.8%, and the median OS
time was 22.7 months. By meta-analysis, Lee et al (14) found that platinum-based regimens
showed a tendency towards better outcomes compared with
non-platinum regimens in terms of survival. The median survival
time was 9.4 months, the 1-year survival rate was 36.9% and the
2-year survival rate was 19.7%. Depending on the pathological
characteristics, the location of the tumor and the individual
performance status (PS), a multimodal therapy that combines
cytoreductive surgery, radiation and chemotherapy may be performed
in certain cases (15). In the
present case, due to the identification of a pelvic mass and
affected inguinal lymph node, surgery was performed followed by
Taxol and cisplatin/carboplatin treatment. By the 8th cycle of
chemotherapy, the serum CA19-9 level had stopped decreasing and
began to increase, and pelvic CT imaging showed recurrence in the
right pelvic cavity, dilatation of the right ureter and right
hydronephrosis. Palliative pelvic external radiation was
administered following the ureteroneocystostomy due to residual
pelvic lesions; however, the efficacy was limited.
One of the most important targets when treating
cancer patients should be prolonging the survival time. Although
platinum-based chemotherapy or acceptance into clinical trials may
be offered to patients of a relatively young age and good PS,
supportive care should be recommended for other patients (16). Following the transverse colostomy
procedure in the present case, the majority of treatments were
subsequently stopped, with the exception of supportive care.
Supportive care in patients with active and incurable SC CUP should
be more widely considered.
The prognostic factors reported for CUP, including
age, gender, PS, weight loss, pathological subtype, tumor location,
number of metastatic sites and serum markers, have been examined in
several previous studies (11,17–19).
Kodaira et al (18) conducted
a retrospective analysis for OS in 58 consecutive CUP patients
treated with carboplatin plus paclitaxel (Taxol) therapy. The study
showed that poor PS, low serum albumin level, pleural effusion, and
bone and liver metastases were adverse prognostic factors. In 311
patients with CUP diagnosed in a single university center between
1988 and 2011, analysis of the clinical, pathological and
laboratory data led Petrakis et al (19) to propose that clinicopathological CUP
subgroup and PS were independent prognostic factors. SC CUP with
metastasis in the liver has been shown to be associated with a
particularly poor prognosis. In a retrospective analysis of 49
patients, the median survival time ranged between 1.7 and 10 months
(20). The patient reported in the
present study had a good PS, but the pathological subtype was
poorly-differentiated SCC with multiple metastases within the
pelvic cavity, abdominal wall, inguinal lymph node and liver. The
patient survived for only 10 months after the diagnosis.
Additional points also require consideration in the
present case study. First, although all the available pathological
material from the first surgery was examined and the results were
shown to be malignancy-free, the possibility of primary SCC of the
ovary could not be completely excluded. In the first surgery, all
the resected tissues, including the cyst wall, left ovary and
Fallopian tube, were transferred into an internal bag and removed
through the 10-mm puncture hole on the right abdominal wall. Due to
the large volume, these tissues were cut into several sections
while in the bag. Cutting the cyst wall is not optimal for good
subsequent pathological examinations, and it is therefore not
certain that the complete cyst wall was examined without any
omission. Second, the ‘chocolate-like’ fluid that flowed into the
pelvic cavity upon breaking of the ovarian cyst may have caused the
spread and implantation of potential malignancy, even though the
peritoneal cavity was irrigated. During such clinical work,
experience from the present case study would maintain the
recommendation of using a bag to remove tissues from the abdominal
cavity, even in cases where the lesions are considered to be
benign. In addition, thorough washing of the abdominal cavity upon
tumor rupture, should be performed. During laparoscopic surgery, a
method to remove resected tumor tissues that are much larger than
the puncture holes should be considered with regard to the
requirement for a comprehensive histopathology analysis.
In conclusion, the present study describes a rare
case of SC CUP with abdominal wall lesions as the primary symptom.
To the best of our knowledge, this is the first case study to have
investigated this tumor type. The diagnosis, pathogenesis,
treatment and prognosis of this type of tumor has generally been
considered poor, thus, additional case reports are required to
facilitate the clinical diagnosis and the appropriate course of
treatment for affected patients.
Abbreviations:
|
CUP
|
carcinoma of unknown primary site
|
|
CT
|
computed tomography
|
|
CA19-9
|
carbohydrate antigen 19-9
|
|
CA125
|
cancer antigen 125
|
|
SCC
|
squamous cell carcinoma
|
|
SCC-Ag
|
SCC antigen
|
|
AFP
|
α-fetoprotein
|
|
CEA
|
carcinoembryonic antigen
|
|
NSE
|
neuron-specific enolase
|
|
HPV
|
human papilloma virus
|
|
PET/CT
|
positron emission tomography/computed
tomography
|
|
OS
|
overall survival
|
|
PS
|
performance status
|
References
|
1
|
Pavlidis N, Briasoulis E, Hainsworth J and
Greco FA: Diagnostic and therapeutic management of cancer of an
unknown primary. Eur J Cancer. 39:1990–2005. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Matsubara N, Mukai H, Nagai S and Itoh K:
Review of primary unknown cancer: Cases referred to the National
Cancer Center Hospital East. Int J Clin Oncol. 15:578–582. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pouessel D, Thezenas S, Culine S, Becht C,
Senesse P and Ychou M: Hepatic metastases from carcinomas of
unknown primary site. Gastroenterol Clin Biol. 29:1224–1232. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pavlidis N and Fizazi K: Carcinoma of
unknown primary (CUP). Crit Rev Oncol Hematol. 69:271–278. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kwee TC and Kwee RM: Combined FDG-PET/CT
for the detection of unknown primary tumors: Systematic review and
meta-analysis. Eur Radiol. 19:731–744. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tamam MO, Mulazimoglu M, Guveli TK, Tamam
C, Eker O and Ozpacaci T: Prediction of survival and evaluation of
diagnostic accuracy whole body 18F-fluora-2-deoxyglucose positron
emission tomography/computed tomography in the detection carcinoma
of unknown primary origin. Eur Rev Med Pharmacol Sci. 16:2120–2130.
2012.PubMed/NCBI
|
|
7
|
Hemminki K, Bevier M, Hemminki A and
Sundquist J: Survival in cancer of unknown primary site:
Population-based analysis by site and histology. Ann Oncol.
23:1854–1863. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fehri R, Rifi H, Alboueiri A, Malouche D,
Ayadi M, Rais H and Mezlini A: Carcinoma of unknown primary:
Retrospective study of 437 patients treated at Salah Azaiez
Institute. Tunis Med. 91:205–208. 2013.PubMed/NCBI
|
|
9
|
FernandezCotarelo MJ, GuerraVales JM,
Colina F and de la Cruz J: Prognostic factors in cancer of unknown
primary site. Tumori. 96:111–116. 2010.PubMed/NCBI
|
|
10
|
Kwee TC, Basu S, Cheng G and Alavi A: FDG
PET/CT in carcinoma of unknown primary. Eur J Nucl Med Mol Imaging.
37:635–644. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Abruzzese JL, Abbruzzese MC, Hess KR,
Raber MN, Lenzi R and Frost P: Unknown primary carcinoma: Natural
history and prognostic factors in 657 consecutive patients. J Clin
Oncol. 12:1272–1280. 1994.PubMed/NCBI
|
|
12
|
Briasoulis E, Kalofonos H, Bafaloukos D,
Samantas E, Fountzilas G, Xiros N, Skarlos D, Christodoulou C,
Kosmidis P and Pavlidis N: Carboplatin plus paclitaxel in unknown
primary carcinoma: A phase II Hellenic Cooperative Oncology Group
Study. J Clin Oncol. 18:3101–3107. 2000.PubMed/NCBI
|
|
13
|
Nishimori H, Takahashi S, Kiura K, Ennishi
D, Kobayashi T, Sano K, Shinozaki E, Yokoyama M, Mishima Y, Terui
Y, et al: Cancer of unknown primary site: A review of 28 cases and
the efficacy of cisplatin/docetaxel therapy at a single institute
in Japan. Acta Med Okayama. 64:285–291. 2010.PubMed/NCBI
|
|
14
|
Lee J, Hahn S, Kim DW, Kim J, Kang SN, Rha
SY, Lee KB, Kang JH and Park BJ: Evaluation of survival benefits by
platinums and taxans for an unfavourable subset of carcinoma of
unknown primary: A systematic review and meta-analysis. Br J
Cancer. 108:39–48. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pentheroudakis G, Lazaridis G and Pavlidis
N: Axillary nodal metastases from carcinoma of unknown primary
(CUPAX): A systematic review of published evidence.
Breast Cancer Res Treat. 119:1–11. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Briasoulis E, Pavlidis N and Felip E: ESMO
Guidelines Working Group: Cancers of unknown primary site: ESMO
clinical recommendations for diagnosis, treatment and follow-up.
Ann Oncol. 20 (Suppl 4):154–155. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pasterz R, Savaraj N and Burgess M:
Prognostic factors in metastatic carcinoma of unknown primary. J
Clin Oncol. 4:1652–1657. 1986.PubMed/NCBI
|
|
18
|
Kodaira M, Takahashi S, Yamada S, Ueda K,
Mishima Y, Takeuchi K, Yamamoto N, Ishikawa Y, Yokoyama M, Saotome
T, et al: Bone metastasis and poor performance status are
prognostic factors for survival of carcinoma of unknown primary
site in patients treated with systemic chemotherapy. Ann Oncol.
21:1163–1167. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Petrakis D, Pentheroudakis G, Voulgaris E
and Pavlidis N: Prognostication in cancer of unknown primary (CUP):
Development of a prognostic algorithm in 311 cases andreview of the
literature. Cancer Treat Rev. 39:701–708. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lazaridis G, Pentheroudakis G, Fountzilas
G and Pavlidis N: Liver metastases from cancer of unknown primary
(CUPL): A retrospective analysis of presentation, management and
prognosis in 49 patients and systematic review of the literature.
Cancer Treat Rev. 34:693–700. 2008. View Article : Google Scholar : PubMed/NCBI
|