Introduction
Primary tracheal tumors are relatively uncommon and
2 out of 3 are malignant or of intermediate malignancy, such as
squamous cell carcinoma, adenoid cystic carcinoma and carcinoid
tumors, while the remaining third are benign lesions, such as
papilloma, hemangioma and hamartoma. Schwannoma and neurofibroma
originate from Schwann cells and are usually benign lesions. They
rarely occur in the trachea and the exact frequency is unknown.
Thus far, limited cases have been reported, of which the majority
occur in the lower trachea. Previous reports have indicated that
endoscopic and surgical resection have been successfully applied in
the treatment of the disease, and as a result, the prognosis of the
disease was improved (1–4).
The present study reports the case of a patient with
a benign primary tracheal schwannoma who was treated by tracheal
resection and reconstruction following recurrence after endoscopic
resection. In addition, 51 cases of primary tracheal schwannoma
from English literature are reviewed, with emphasis on the clinical
characteristics of the disease and the selection of the
treatment.
Case report
A 53-year-old male presented to Xinhua Hospital
(Shanghai, China) on August 19th, 2013 with coughing and
dyspnea that had persisted for half a year, and increasing chest
tightness and dyspnea for 1 week. The past medical history was
significant for hypertension and diabetes. In the Outpatient
Clinic, the patient's spirometry showed a severe obstructive
ventilation defect and the following computed tomography (CT) scan
of the chest revealed a well-defined soft-tissue mass in the
trachea. The patient was admitted to the hospital and a physical
examination revealed a blood pressure of 190/120 mmHg (normal
range, <130/85 mmHg), a heart rate of 102 beats/min (normal
range, 60–100 beats/min), a respiratory rate of 23–38 breaths/min
(normal range, 12–20 breaths/min) and an oxygen saturation of 98%
on room air (normal range, >94%). Lung auscultation indicated a
prolonged expiratory phase and wheezing over the cervical tracheal
segment in the inspiratory and expiratory phases. Multiplanar
reconstructions and contrast-enhanced CT indicated a mass with
minimal enhancement, ~1.5 cm above the carina and occluding ~90% of
the tracheal lumen, while at the same time smoothly protruding into
the esophagus (Fig. 1A and B).
Flexible bronchoscopy confirmed the presence of a 2.0-cm, round,
tan-colored mass in the distal third of the trachea. The mass was
covered with several small, discrete vessels on the surface, but
was not pulsatile or friable (Fig.
1C). Gastroscopy was applied immediately and there were no
abnormalities in the esophagus mucosa. Electrosurgical snaring was
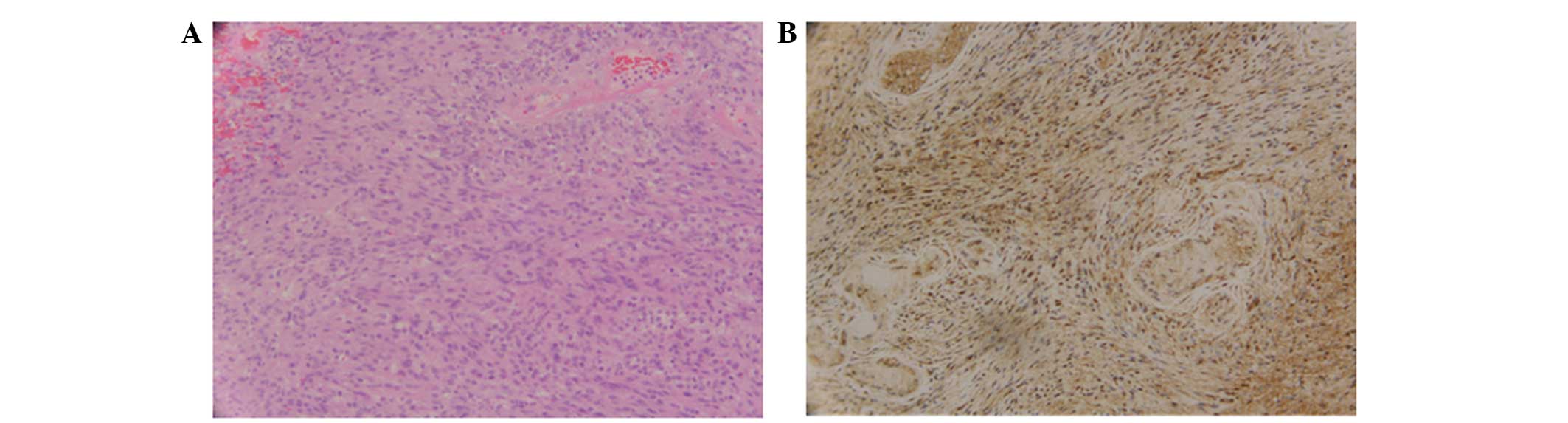
used to cut the mass under flexible bronchoscopy. Morphologically,
the tumor exhibited an Antoni A growth pattern, composed of spindle
cells with elongated palisading nuclei (Fig. 2A). A few hyalinized blood vessels were
found, whereas no clear necrosis or mitotic activity was observed
within these areas. The tumor demonstrated strong and diffuse
nuclear and cytoplasmic positivity for S-100 protein (Fig. 2B) and vimentin, but was negative for
cytokeratin, desmin, cluster of differentiation 117 and smooth
muscle actin. The histological and immunohistochemical findings
were consistent with benign schwannoma. Argon plasma coagulation
(APC) combined with electronic snaring was applied twice and 75% of
the mass was removed. The shortness of breath was resolved
immediately and the patient was discharged on day 3 post-treatment.
However, chest tightness recurred 2 weeks later. Bronchoscopic
examination was employed again and a relapse of the mass in the
same region of the trachea was confirmed. A 3-cm segment of the
trachea was subsequently resected and an anastomosis was performed.
The resection margins were free of tumor. There were no
post-operative complications and no recurrence in the 1 year
follow-up period. At the time of writing, the patient was well with
no evidence of disease.
The patient provided written informed consent for
the publication of this study. Furthermore, the study was approved
by the Ethics Committee of Xinhua Hospital Affiliated to Shanghai
Jiaotong University School of Medicine.
Discussion
Neurogenic tumors, schwannoma and neurofibroma are
the main benign tumors arising from the peripheral nerves.
Schwannoma is much less common than neurofibroma, and usually
occurs in the head, neck, retroperitoneum, extremities and
mediastinum (5,6). The tumor is extremely rare in the
trachea, being more frequently reported in the lungs and
bronchi.
The present study reviewed the literature between
1950 and 2013, and identified 51 cases of primary tracheal
schwannoma (1–3,7–22). In these cases, schwannoma mainly
occurred in adults (78.4%; 40/51), with a predilection for women
(30 females and 20 males; gender of 1 case was not stated). The
majority of the cases occurred in the distal third of the trachea,
followed by the proximal and then the middle third of the trachea.
Of the 51 cases, 26 were reported in Asian populations, followed by
North American and European populations. The clinical symptoms and
signs depended on the tumor location, size and degree of airway
obstruction. Coughing, wheezing and dyspnea as airway obstruction
symptoms were commonly reported, while hemoptysis, hoarseness and
chest pain were also reported in tracheal schwannoma. Of the 51
patients, 15 presented with wheezing or stridor on physical
examination. Half of the patients were initially misdiagnosed with
asthma, and treatment was delayed for an average of 17 months from
the onset of symptoms. The tumor size varied from 1.0 to 4 cm. The
tumors were commonly 1–3 cm and only 3 cases exhibited a tumor of
>3 cm in diameter in the trachea. In terms of management, 19
patients underwent endoscopic resection of the mass and 29 received
surgical resection. Among the patients whose masses were resected
by the endoscopic technique, laser with or without a
CO2, electronic snaring, APC, cryotherapy, endoscopic
excision and microdebridement were applied. However, 4 cases were
reported with relapse and were further treated by surgery (4,23,24). In total, 3.9% (2/51) of patients
presented with malignant schwannoma. Overall, 3 cases succumbed to
complications, including renal insufficiency, post-operative
infection and hypoxic brain damage induced by acute airway
obstruction.
Pulmonary function and CT were useful for forming an
early diagnosis. Pulmonary function, particularly flow-volume
curves, showed upper airway obstruction, which prompted the
clinicians to proceed with further examinations. In the present
case, the severe obstructive ventilation defect on spirometry
assisted the locating of the mass in the trachea. CT was used to
define the tumor size, location, and intratracheal and
extratracheal extension. Bronchoscopy as a further examination
technique could directly view the mass in the lumen, and evaluate
the extent and vascularity of the lesion and its association to the
peritracheal tissue. Bronchoscopy was also useful in the biopsy and
incision of the tumor.
As reported previously, tracheal resection and
endoscopic excision could be utilized in the management of tracheal
schwannoma (8,21,25). In
the present patient, the huge sessile mass in the trachea was
confirmed by bronchoscopy. In the study by Lee et al
(26), a sessile mass in left main
bronchus was successfully removed by using APC and rigid
bronchoscopy tip, and the patient was only followed up for 4
months. Due to the reluctance of the present patient to accept
surgery initially, treatment with endoscopic snaring combined with
APC was performed, and an incomplete initial resection was
confirmed 2 weeks later. The patient then underwent segmental
tracheal resection and tracheal reconstruction, and no recurrence
was found in 1 year of follow-up.
The management of tracheal schwannoma should
consider the size and extratracheal component of the tumor, the
cardiopulmonary function in the patient and the pedicle of the
tumor. For patients with pedunculated and completely intraluminal
tumors (20), or in those with severe
underlying diseases (27), endoscopic
resection may provide a reasonable treatment option. For those
patients with huge and sessile schwannomas in the trachea and
non-cardiopulmonary function restriction, surgical resection is
indispensable as an optimal treatment method (3). However, prior reports also indicated
that endoscopic resection in schwannoma has the possibility of
local recurrence (4,23,24),
whereas no relapse was recorded in cases of surgical resection. As
for local recurrence following endoscopic resection, surgery should
be chosen.
In conclusion, primary tracheal schwannoma is rare.
The tumor usually causes airway obstruction and the symptoms of
this are common between cases. Pulmonary function, CT and
bronchoscopy are useful for the diagnosis. The treatment of choice
depends on the condition of the patient, whereas surgery must be
chosen when local recurrence follows endoscopic treatment. Although
the prognosis of primary tracheal schwannoma is favorable,
long-term follow-up after tumor removal is required.
References
|
1
|
Davies MJ, Hall DR and Ross BA: Rare
tracheal tumours: Two case reports of primary neurogenic tumours
occurring in the trachea. Respir Med. 87:145–146. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tang LF, Chen ZM and Zou CC: Primary
intratracheal neurilemmoma in children: Case report and literature
review. Pediatr Pulmonol. 40:550–553. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Righini CA, Lequeux T, Laverierre MH and
Reyt E: Primary tracheal schwannoma: One case report and a
literature review. Eur Arch Otorhinolaryngol. 262:157–160. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kasahara K, Fukuoka K, Konishi M, Hamada
K, Maeda K, Mikasa K and Kimura H: Two cases of endobronchial
neurilemmoma and review of the literature in Japan. Intern Med.
42:1215–1218. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Takeda S, Miyoshi S, Minami M and Matsuda
H: Intrathoracic neurogenic tumors-50 years' experience in a
Japanese institution. Eur J Cardiothorac Surg. 26:807–812. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
DasGupta TK, Brasfield RD, Strong EW and
Hajdu SI: Benign solitary Schwannomas (neurilemomas). Cancer.
24:355–366. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dutta R, Kumar A, Kaushal S and Choudhary
SK: A case of carinal schwannoma resected under cardiopulmonary
bypass. Indian J Cancer. 48:366–368. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Melendez J, Cornwell L, Green L and Casal
RF: Treatment of large subglottic tracheal schwannoma with
microdebrider bronchoscopy. J Thorac Cardiovasc Surg. 144:510–512.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Erol MM, Uzun H, Tekinbas C, Gunduz A,
Turedi S and Kosucu P: A case of intratracheal schwannoma
presenting at the emergency department with a diagnosis of
asthmatic attack. J Emerg Med. 39:589–591. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shah SS, Karnak D, Shah SN, Biscotti C,
Murthy S and Mehta AC: Clinical-pathologic conference in general
thoracic surgery: A malignant peripheral nerve sheath tumor of the
trachea. J Thorac Cardiovasc Surg. 132:1455–1459. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Pang LC: Primary neurilemoma of the
trachea. South Med J. 82:785–787. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nio M, Sano N, Kotera A, Shimanuki Y,
Takeyama J and Ohi R: Primary tracheal schwannoma (neurilemoma) in
a 9-year-old girl. J Pediatr Surg. 40:E5–E7. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dincer SI, Demir A, Kara HV, Fener N and
Altin S: Primary tracheal schwannoma: A case report. Acta Chir
Belg. 106:254–256. 2006.PubMed/NCBI
|
|
14
|
Takeda K, Horiuchi M, Nakaya M, Yamaguchi
K and Fujikawa A: Schwannoma of the trachea; a new resection
technique. Auris Nasus Larynx. 30:425–427. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kitagawa H, Kawase H, Wakisaka M, Satou Y,
Satou H, Furuta S and Nakada K: Six cases of children with a benign
cervical tumor who required tracheostomy. Pediatr Surg Int.
20:51–54. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Murata T, Shino M, Yasuoka Y and
Chikamatsu K: Subglottic Schwannoma: A report of a rare case that
was treated with medial thyrotomy. Am J Otolaryngol. 34:569–573.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hamdan AL, Moukarbel RV, Tawil A, ElKhatib
M and Hadi U: Tracheal schwannoma: A misleading entity. Middle East
J Anesthesiol. 20:611–613. 2010.PubMed/NCBI
|
|
18
|
Thomas R, Christopher DJ, Thangakunam B
and Samuel R: Tracheal schwannoma as a mimic of bronchial asthma.
Singapore Med J. 53:e95–e96. 2012.PubMed/NCBI
|
|
19
|
Rusch VW and Schmidt RA: Tracheal
schwannoma: management by endoscopic laser resection. Thorax.
49:85–86. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Weiner DJ, Weatherly RA, DiPietro MA and
Sanders GM: Tracheal schwannoma presenting as status asthmaticus in
a sixteen-year-old boy: Airway considerations and removal with the
CO2 laser. Pediatr Pulmonol. 25:393–397. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dorfman J, Jamison BM and Morin JE:
Primary tracheal schwannoma. Ann Thorac Surg. 69:280–281. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Nass RL and Cohen NL: Neurilemoma of the
trachea. Arch Otolaryngol. 105:220–221. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Horovitz AG, Khalil KG, Verani RR, Guthrie
AM and Cowan DF: Primary intratracheal neurilemoma. J Thorac
Cardiovasc Surg. 85:313–317. 1983.PubMed/NCBI
|
|
24
|
Jung YY, Hong ME, Han J, Kim TS, Kim J,
Shim YM and Kim H: Bronchial schwannomas: Clinicopathologic
analysis of 7 cases. Korean J Pathol. 47:326–331. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Stouffer CW, Allan RW, Shillingford MS and
Klodell CT: Endobronchial schwannoma presenting with bronchial
obstruction. Interact Cardiovasc Thorac Surg. 10:133–134. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lee BR, Choi YD, Kim YI, Lim SC and Kwon
YS: Endobronchial schwannoma treated by rigid bronchoscopy with
argon plasma coagulation. Tuberc Respir Dis. 73:174–177. 2012.
View Article : Google Scholar
|
|
27
|
Feldhaus RJ, Anene C and Bogard P: A rare
endobrochial neurilemmoma (Schwannoma). Chest. 95:461–462. 1989.
View Article : Google Scholar : PubMed/NCBI
|