Introduction
Cancers of unknown primary (CUPs) represent a
heterogeneous group of metastatic tumors for which the site of
origin cannot be diagnosed on a standardized diagnostic work-up at
the time of diagnosis. CUP accounts for 3–5% of all malignancies
(1,2).
At present, CUP is the fifth and eighth most common
cancer diagnosis in women and men, respectively (3). The majority of cases have an
unfavourable prognosis, with a life expectancy that ranges from 6
to 9 months (4).
Without a specific diagnosis, the management of
these patients is more difficult, as the treatment is typically
empirical, with non-specific antineoplastic drugs used in
combination in a range of chemotherapy regimens, but with no one
treatment schedule superior to the others (5).
Primary tumor cells exhibit characteristic genetic
expression that is maintained among the metastatic cells;
therefore, it is possible to identify the primary site by comparing
the genetic profile of the metastatic cells to a genetic profile
database of different types of tumors. Therefore, various gene
expression profiling methods have been developed in order to aid in
identifying the primary tumor (6).
The current study presents the case of a patient
with a diagnosis of CUP in which gene expression profiling was
performed and the patient benefited from a specific systemic
chemotherapy treatment, established as a result of having taken
into account this information of the presumed primary site. Written
informed consent was obtained from the patient.
Case report
A 49-year-old male, non-smoker, with no notable
medical history, was admitted to the Miguel Servet University
Hospital (Zaragoza, Spain) in September 2013 due to right inguinal
pain and swelling of the ipsilateral leg. The patient had a good
performance status of 1 and a normal physical examination, with the
exception of the swelling of the right leg. Inguinal
ultrasonography (US) did not reveal any pathology. Since no symptom
improvement was achieved over time, US was performed again in
February 2014, which revealed multiple enlarged abdominal lymph
nodes, including retroperitoneal and para-aortic nodes, the largest
measuring 32 mm in diameter.
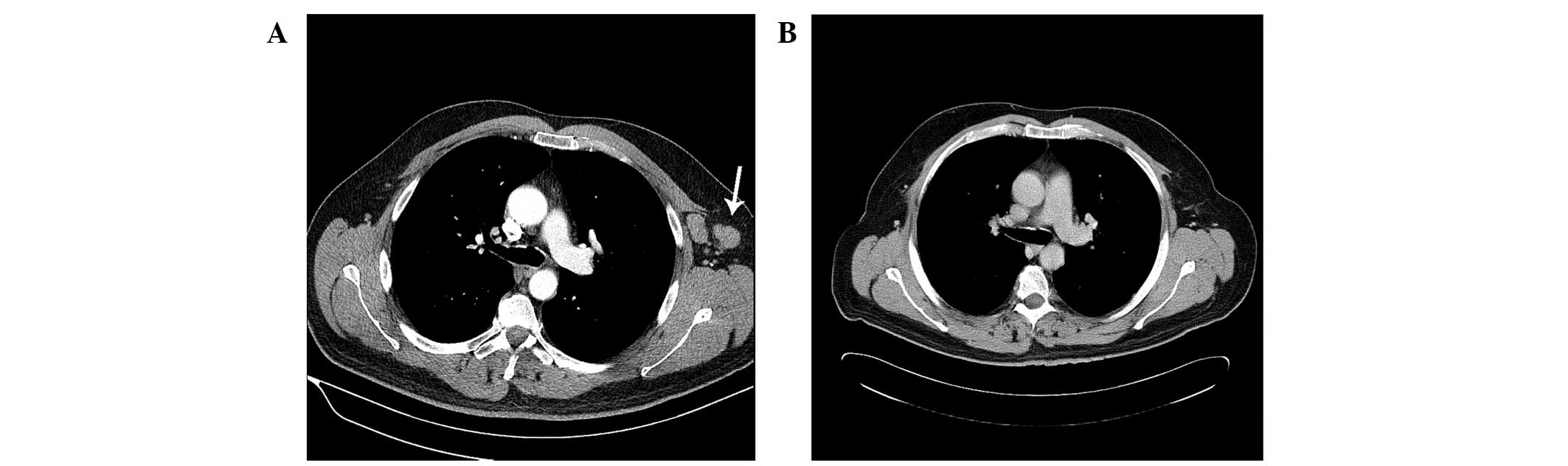
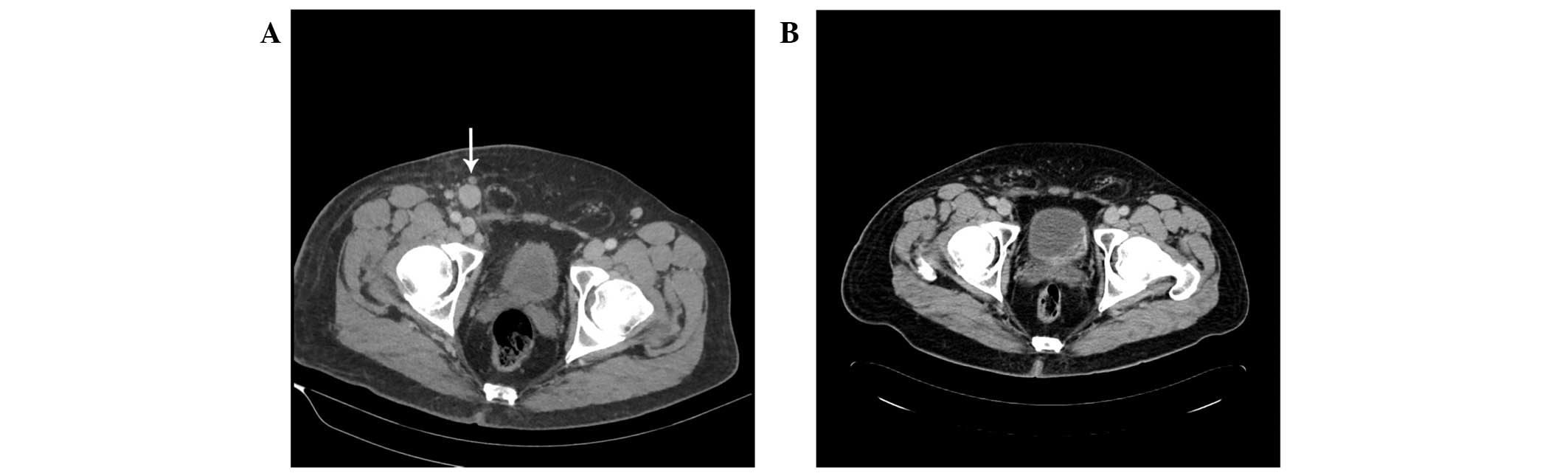
Total body computed tomography (CT) and
fluorodeoxyglucose positron emission CT were performed and a
poliadenopathic condition, involving the left axillary, cervical,
supraclavicular, mediastinal, retroperitoneal, para-aortic, iliac
and bilateral inguinal lymph nodes, was found. The largest node, in
the right inguinal area, measured 41 mm at its largest
diameter.
Laboratory tests revealed a markedly increased
carcinoembryonic antigen (CEA) level (33 U/ml; normal range for
non-smokers, 0–2.5 U/ml; normal range for smokers, 0–5 U/ml), but
the α-fetoprotein, β-human chorionic gonadotropin,
prostate-specific antigen (PSA), cancer antigen 19.9 and β2
microglobulin levels were within laboratory normal ranges. On March
3, 2014, the patient underwent an excisional biopsy of the right
inguinal lymph node. The pathology report showed an adenocarcinoma,
without identifying the primary site. An extensive range of
immunohistochemistry (IHC) tests were performed, which resulted in
positivity for cytokeratin (CK)7, CK8, CAM5.2, CEA, epithelial
membrane antigen (EMA), AE1:AE3, E-cadherin and GDFP-15, and
negativity for ALC, S-100, vimentin, PLAP, inhibin, cluster of
differentiation 30, CK20, CK5/6, PSA, thyroid transcription
factor-1, CDX-2, RE, RP and human epidermal growth factor-2
(Table I). No EGFR gene mutation was
found. The Ki-67 proliferation index was 70%.
 | Table I.Immunohistochemistry results. |
Table I.
Immunohistochemistry results.
| Result | Antigen |
|---|
| Positivity | CK7, CK8, CAM5.2,
CEA, EMA, AE1:AE3, E-cadherin, GDFP-15 |
| Negativity | CD45, S-100,
vimentin, PLAP, inhibin, CD30, CK20, CK5/6, PSA, TTF1, CDX2, RE,
RP, HER2 |
This IHC profile suggested the lungs, breasts,
salivary glands and sweat glands as the most likely primary tumor
locations. In order to select the most adequate therapy, a tumor
gene expression profiling test was performed. This novel diagnostic
technique allows the prediction of the tumor origin based on gene
expression patterns that are retained from the tissues of origin
(7). A salivary gland adenocarcinoma
was the main diagnosis with a probability of 90%. Breast
adenocarcinoma could not be excluded, with a probability of 6%. The
patient received standard advanced salivary gland first-line
chemotherapy consisting of a 50mg/m2 cisplatin,
50mg/m2 doxorubicin and 500mg/m2
cyclofosfamide (CAP) regimen every three weeks.
After 6 cycles of CAP for 18 weeks, CT revealed a
partial response of all the lymph nodes, with a significant
decrease in size of the left axillary, mediastinal and right
inguinal lymph nodes (Figs.
1–3). Subsequently, the patient
continued follow-up with stable disease until Februrary 2015, when
progression occurred (brain and liver metastases). Two different
regimens of chemotherapy (carboplatin-taxol and vinorelbine) were
administered with no response. In July 2015, the patient presented
a worsened performance status and was admitted due to seizures.
Discussion
By definition, CUP is a histologically confirmed
malignant tumor that is not compatible with a primary neoplasm in
the biopsy area, and which has an origin that remains unclear once
a thorough clinical history, complete physical examination and
basic complementary studies have been performed (8).
CUP can be classified as an adenocarcinoma (50–70%),
poorly-differentiated carcinoma (20–30%), squamous cell carcinoma
(5–8%) or undifferentiated malignant neoplasm (2–3%) depending on
its histological characteristics (9,10).
There is little published data on adenocarcinomas of
unknown origin with lymphadenopathy presentation. The majority of
the studies published describe mediastinal and cervical lymph node
presentations (11–14). Different approaches have been used for
treatment; in one approach, surgery is the cornerstone of the
treatment, whereas in another, platinum-based chemotherapy is used,
with progression-free survival times of 38 and 30 months,
respectively (11,14).
Recent advances made with regard to specific
treatments for each cancer type together with the continuous
development of novel therapies should benefit the primary tumor
prediction in patients with CUP, providing improved therapies and
prognosis.
Traditionally, the majority of patients have been
treated with empiric chemotherapy, including platinum- and
taxane-based chemotherapy regimes, with poor results (median
survival time, 6–8 months) (15,16). As
randomised controlled trials have not established any effective
therapies for such patients, empirical systemic treatments that
consider the performance status of the patients are widely
accepted. In recent years, novel targeted drugs and personalized
medicine have had increasing roles in oncological therapy. As a
result, with more specific and targeted drugs, therapy with a
single empiric combination chemotherapy regimen becomes
increasingly inadequate.
Gene expression profiling assays correctly
identified the site of origin in 85% of cases in blinded studies of
tumors of known origin, and was found to favorably compare with IHC
staining (17,18). The best use of gene expression
profiling to form a diagnosis appears to be for cases with
inconclusive IHC staining. The site-specific treatment of
carcinomas of unknown primary site based on gene expression
profiling and/or IHC predictions appears to result in improvements
in the overall patient outcome (19,20).
Therefore, gene expression profiling should be included in the
diagnosis of a patient when IHC staining is not able to predict a
single site of origin. Site-specific treatment, based on a tissue
of origin diagnosis, should replace empiric chemotherapy in
patients with CUP.
Salivary gland cancer (SGC), such as that diagnosed
in the present case, is uncommon and accounts for <5% of all
cancers of the head and neck (21).
Different types of SGC have considerably variable histological
patterns and behavior. The tumors are classified according to the
2005 World Health system (22), in
which 24 histological subtypes are listed. In total, >75% of all
SGCs are accounted for by mucoepidermoid carcinoma, adenoid cystic
carcinoma and adenocarcinoma, as described by the Memorial
Sloan-Kettering experience (23). The
characteristics of slow growth, multiple local recurrences and
prolonged clinical course, often with delayed distant metastasis,
have all been attributed to SGCs (23).
Salivary gland malignancies may exhibit distant
metastatic disease, with the best example data shown in studies of
adenoid cystic carcinoma. The most common site of distant
metastasis is the lungs (24),
followed by the liver and bones.
Metastatic presentation of unknown primary is
uncommon for salivary gland carcinomas. Florentine et al
(25) reported a patient who had
metastatic bone disease from unknown primary as the initial
diagnosis, and the patient's further medical history showed a
record of early-stage adenoid cystic carcinoma (ACC) of the soft
palate, which had been diagnosed and resected 3 months earlier. The
bone histopathology was compatible with ACC.
To the best of our knowledge, the present study is
the first report of multiple lymph nodes metastases as the only
presentation in salivary gland adenocarcinoma.
CAP, the most commonly studied regimen for cancer,
is an actively used regimen for SGC (26–28). In a
study by Alberts et al (29)
responses were observed that included 2 patient who experienced
complete remission, from a total of 5 patients. Kaplan et al
(26) recorded 5 objective responses,
including 1 complete response, from a total of 6 patients.
Additionally, 3 complete and 3 partial remissions, from a total of
13 patients, were reported in the study by Dreyfuss et al
(27).
The present patient benefited from a site-specific
treatment; however, if the primary site had not been known, a
different regimen of chemotherapy would have had been used and
since no optimum chemotherapy regimen has been identified for CUP,
a worse patient outcome would be expected (30). The patient underwent gene expression
profiling with CancerTYPE ID (BioTheranostics, Inc., San Diego, CA,
USA), in order to aid in the identification of the primary site.
The CancerTYPE ID assay is a 92-gene reverse
transcription-polymerase chain reaction assay that allows the
identification of 30 main tumor types and 54 subtypes (17). There is also another gene expression
profiling assay currently commercially available, which uses 64
tissue-specific microRNAs to enable the identification of 42 tumor
types, using a microarray technology known as the Cancer Origin
Test (Rosetta Genomics, Rehovot, Israel) (18). These two assays were validated using
biopsies of tumors from known primary sites. Biopsies were taken
from either the primary site or a metastatic site; tumors with
well-differentiated and poorly-differentiated histology were
included. In these validation studies, each of which included
specimens from several hundred tumors, the two assays each
correctly identified 85% of the tumors included (17,18).
Regarding the present case study, the patient
benefited from a site-specific treatment according to the
prediction of the gene expression profiling assay, and experienced
a partial response for all lesions following use of a chemotherapy
widely used in salivary gland adenocarcinoma. Gene expression
profiling is a valuable addition to a diagnostic evaluation.
Nevertheless, ongoing clinical trials are required to refine these
recommendations.
References
|
1
|
Pavlidis N and Fizazi K: Cancer of unknown
primary (CUP). Crit Rev Oncol Hematol. 54:243–250. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Varadhachary GR, Abbruzzese JL and Lenzi
R: Diagnostic strategies for unknown primary cancer. Cancer.
100:1776–1785. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Altman E and Cadman E: An analysis of 1539
patients with cancer of unknown primary site. Cancer. 57:120–124.
1986. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pavdilis N, Briasoulis E, Hainsworth J and
Greco FA: Diagnostic and therapeutic management of cancer of an
unknown primary. Eur J Cancer. 30:1990–2005. 2003.
|
|
5
|
Golfinopoulos V, Pentheroudakis G, Salanti
G, Nearchou AD, Ioannidis JP and Pavlidis N: Comparative survival
with diverse chemotherapy regimens for cancer of unknown primary
site: Multiple-treatments meta-analysis. Cancer Treat Rev.
35:570–573. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Varadhachary GR, Talantov D, Raber MN,
Meng C, Hess KR, Jatkoe T, Lenzi R, Spigel DR, Wang Y, Greco FA, et
al: Molecular profiling of carcinoma of unknown primary and
correlation with clinical evaluation. J Clin Oncol. 26:4442–4448.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Su AI, Welsh JB, Sapinoso LM, Kern SG,
Dimitrov P, Lapp H, Schultz PG, Powell SM, Moskaluk CA, Frierson HF
Jr and Hampton GM: Molecular classification of human carcinoma by
use of gene expression signatures. Cancer Res. 61:7388–7393.
2001.PubMed/NCBI
|
|
8
|
Greco FA and Hainsworth JD: Cancer of
unknown primary siteCancer: Principles & Practice of Oncology.
DeVita VT Jr, Hellman S and Rosenberg SA: 6th. Lippincott Williams
& Wilkins; Philadelphia: pp. 2537–2560. 2001
|
|
9
|
Van de Wouw AJ, Janssen-Heijnen ML,
Coebergh JW and Hillen HF: Epidemiology of unknown primary tumours;
incidence and population-based survival of 1285 patients in
Southeast Netherlands, 1984–1992. Eur J Cancer. 38:409–413. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hess KR, Abbruzzese MC, Lenzi R, Raber MN
and Abbruzzese JL: Classification and regression tree analysis of
1000 consecutive patients with unknown primary carcinoma. Clin
Cancer Res. 5:3403–3410. 1999.PubMed/NCBI
|
|
11
|
Harada H, Yamashita Y, Kuraoka K and
Taniyama K: Sequential mediastinal lymphadenectomy of an unknown
primary tumor. The Ann Thorac Surg. 95:687–689. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nakano T, Endo S, Endo T, Hasegawa T,
Nakayama M, Sugiyama Y and Hironaka M: Multimodal treatment for
multistation mediastinal lymph node adenocarcinoma: A case report.
Ann Thorac Cardiovasc Surg. 18:136–139. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
SorghoLougue LC, Luciani A, Kobeiter H,
Zelek L, Malhaire C, Deux JF, Brun B, Piedbois P and Rahmouni A:
Adenocarcinomas of unknown primary (ACUP) of the mediastinum
mimicking lymphoma: CT findings at diagnosis and follow-up. Eur J
Radiol. 59:42–48. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pepper C, Pai I, Hay A, Deery A, Wilson P,
Williamson P and Pitkin L: Investigation strategy in the management
of metastatic adenocarcinoma of unknown primary presenting as
cervical lymphadenopathy. Acta Otolaryngol. 134:838–842. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Briasoulis E, Kalofonos H, Bafaloukos D,
Samantas E, Fountzilas G, Xiros N, Skarlos D, Christodoulou C,
Kosmidis P and Pavlidis N: Carboplatin plus paclitaxel in unknown
primary carcinoma: A phase II Hellenic cooperative oncology group
study. J Clin Oncol. 18:3101–3107. 2000.PubMed/NCBI
|
|
16
|
Culine S, Lortholary A, Voigt JJ, Bugat R,
Théodore C, Priou F, Kaminsky MC, Lesimple T, Pivot X, Coudert B,
et al: Cisplatin in combination with either gemcitabine or
irinotecan in carcinomas of unknown primary site: Results of a
randomized phase II study-trial for the French study group on
carcinomas of unknown primary (GEFCAPI 01). J Clin Oncol.
21:3479–3482. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Erlander MG, Ma XJ, Kesty NC, Bao L,
Salunga R and Schnabel CA: Performance and clinical evaluation of
the 92-gene real-time PCR assay for tumor classification. J Mol
Diagn. 13:493–503. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Meiri E, Mueller WC, Rosenwald S, Zepeniuk
M, Klinke E, Edmonston TB, Werner M, Lass U, Barshack I, Feinmesser
M, et al: A second-generation microRNA-based assay for diagnosing
tumor tissue origin. Oncologist. 17:801–812. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Greco FA, Lennington WJ, Spigel DR,
Varadhachary GR and Hainsworth JD: Carcinoma of unknown primary
site: Outcomes in patients with a colorectal molecular profile
treated with site-specific chemotherapy. J Cancer Ther. 3:37–43.
2012. View Article : Google Scholar
|
|
20
|
Hainsworth JD, Schnabel CA, Erlander MG,
Erlander MG, Haines DW III and Greco FA: A retrospective study of
treatment outcomes in patients with carcinoma of unknown primary
site and a colorectal cancer molecular profile. Clin Colorectal
Cancer. 11:112–118. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Laurie SA and Licitra L: Systemic therapy
in the palliative management of advanced salivary gland cancers. J
Clin Oncol. 24:2673–2678. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Barnes L, Eveson JW, Reichart P and
Sidransky D: Tumours of the Salivary GlandsWorld Health
Organization Classification of Tumors: Pathology and Genetics of
Head and Neck Tumours. World Health Organization; Lyon, France: pp.
209–282. 2005
|
|
23
|
Spiro RH: Salivary neoplasms: Overview of
a 35-year experience with 2,807 patients. Head Neck Surg.
8:177–184. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hamper K, Lazar F, Dietel M, Caselitz J,
Berger J, Arps H, Falkmer U, Auer G and Seifert G: Prognostic
factors for adenoid cystic carcinoma of the head and neck: A
retrospective evaluation of 96 cases. J Oral Pathol Med.
19:101–107. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Florentine BD, Fink T, Avidan S,
Braslavsky D, Raza A and Cobb CJ: Extra-salivary gland
presentations of adenoid cystic carcinoma: A report of three cases.
Diagn Cytopathol. 34:491–494. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kaplan MJ, Johns ME and Cantrell RW:
Chemotherapy for salivary gland cancer. Otolaryngol Head Neck Surg.
95:165–170. 1986.PubMed/NCBI
|
|
27
|
Dreyfuss AI, Clark JR, Fallon BG, Posner
MR, Norris CM Jr and Miller D: Cyclophosphamide, doxorubicin and
cisplatin combination chemotherapy for advanced carcinomas of
salivary gland origin. Cancer. 60:2869–2872. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Licitra L, Cavina R, Grandi C, Palma SD,
Guzzo M, Demicheli R and Molinari R: Cisplatin, doxorubicin and
cyclophosphamide in advanced salivary gland carcinoma: A phase II
trial of 22 patients. Ann Oncol. 7:640–642. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Alberts DS, Manning MR, Coulthared SW,
Koopmann CF Jr and Herman TS:
Adriamycin/cis-platinum/cyclophosphamide combination chemotherapy
for advanced carcinoma of the parotid gland. Cancer. 47:645–648.
1981. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Golfinopoulos V, Pentheroudakis G, Salanti
G, Nearchou AD, Ioannidis JP and Pavlidis N: Comparative survival
with diverse chemotherapy regimens for cancer of unknown primary
site: Multiple-treatments meta-analysis. Cancer Treat Rev.
35:570–573. 2009. View Article : Google Scholar : PubMed/NCBI
|