Introduction
Hepatocellular carcinoma (HCC) is one of the most
common malignant tumors (1). In the
USA, between 1992 and 2005, the overall incidence rate of the
disease increased from 3.1 to 5.4 cases per 100,000 individuals
(2). Furthermore, during the same
period, the mortality rate of HCC increased from 3.3 to 4.0
mortalities per 100,000 individuals (2). However, as a result of advances in HCC
treatment, the one-year survival rate of HCC following diagnosis
increased from 25 to 47% between 1975 and 2005 in the USA (2). The typical features of HCC include
yellow skin, abdominal bloating and bruising easily as a result of
blood clotting abnormalities, as well as other non-specific
symptoms, such as loss of appetite, unintentional weight loss,
abdominal pain, nausea, vomiting and fatigue (3). At present, HCC is usually diagnosed by
dynamic contrast-enhanced magnetic resonance imaging or computed
tomography (4). High levels of
α-fetoprotein (~400 ng/µl) may also be a predictor of HCC in
patients exhibiting liver lesions (1–2 cm in diameter) on imaging
examination (4).
HCC develops as a result of cellular mutations,
which lead to increased levels of cell replication. Ultimately, the
increased replication rate results in cells avoiding apoptosis.
Chronic hepatitis B and/or C infections may accelerate the
progression of HCC by repeatedly activating the body's own immune
system to attack liver cells (5).
The clinical prognosis of HCC is relatively poor as
only ~10–20% of HCC lesions may be completely resected. If the
cancerous tissue cannot be removed completely, the survival time of
HCC patients is usually 3–6 months (2). The prognosis of HCC is poor as the
majority of patients present at an advanced stage of disease and at
present, medical expertise and facilities remain insufficient.
Recent studies proved that the activation of
telomerase and its upregulated activity serve as an extremely
pivotal step in the mechanism of HCC (6–8). The
activity levels of telomerase mainly rely upon the expression level
of human telomerase reverse transcriptase (hTERT). In HCC patients,
the activation of telomerase and a high expression level of the
hTERT subunit catalyzed by telomerase have been reported (1,9–11). Furthermore, hTERT expression and
telomerase activation has been identified in ≤90% of human
malignant tumors, including gastric, brain and renal cancers
(12). High hTERT expression has been
found to correlate with advanced disease and unfavorable prognoses
in various malignancies (13).
However, opinions vary significantly on aspects such as the
simultaneous detection of the hTERT protein and gene, its
correlation with clinicopathological characteristics and whether
hTERT is expressed in para-carcinoma and normal liver tissues.
Consequently, the role of hTERT in the incidence of HCC should be
further investigated. In the present study, immunohistochemical
tests (streptavidin peroxidase method) and reverse
transcription-polymerase chain reaction (RT-PCR) were employed to
simultaneously detect the expression levels of hTERT protein and
mRNA in HCC, corresponding para-carcinoma and normal liver tissues
qualitatively and quantitatively, aiming to investigate their
significance and effects in the incidence of HCC.
Subjects and methods
Study subjects
HCC tissues and corresponding para-carcinoma liver
tissues were surgically collected from 78 patients with HCC who
presented to Shandong Provincial Hospital (Jinan, Shandong, China).
The HCC tissues were kept as fresh specimens and corresponding
para-carcinoma liver tissues were embedded in paraffin for further
analysis. The para-carcinoma liver tissues were collected from
>3 cm away from the tumor margin. Among the participants, 54
were male and 24 female, with a male:female ratio of 2.25:1. The
age range was 27–78 years, with a mean age of 51 years. All
patients were diagnosed with HCC by pathological examination, and
did not undergo pre-operative radiotherapy or chemotherapy. The
clinical and pathological data were complete. Normal liver tissues
were collected from 12 patients; 8 samples from patients receiving
liver surgery and 4 samples from those undergoing hepatic
hemangioma excision, distant from the liver lesions. All samples
were confirmed to be normal liver tissues by pathological methods
and hepatitis B surface antigen (HBsAg) was negative in the serum.
For the specimens used for mRNA detection, necrotic tissues and
blood clots were immediately removed after surgery, and the tissues
were frozen in liquid nitrogen (−80°C) within 30 min. The samples
prepared for subsequent immunochemical tests were subject to
formaldehyde fixation, dehydration, conventional paraffin embedding
and sectioning to a thickness of 4 µm. The samples were finally
diagnosed and graded by physicians from the Department of Pathology
(Shandong Provincial Hospital). Ethical approval was obtained from
the Medical Ethics Committee of Shandong Provincial Hospital
Affiliated to Shandong University. In addition, written informed
consent was obtained from all patients.
Materials and reagents
Anti-hTERT rabbit polyclonal antibody S-P reagent
kits (1:100 dilution) were purchased from Zymed Life Technologies
(Carlsbad, CA, USA). The confirmed positive tissue sections were
utilized as positive controls and the primary antibody was replaced
by phosphate-buffered saline in the negative controls.
Immunohistochemical tests
During the immunohistochemical test, 4-µm paraffin
sections were dewaxed at 65°C and treated with 3% hydrogen peroxide
for endogenous peroxidase inactivation for 5 min prior to microwave
antigen retrieval. Supplementary primary antibody was added for
overnight incubation at 4°C, followed by incubation with
biotin-labeled secondary antibody at 37°C for 30 min and
streptavidin-labeled horseradish peroxide enzyme at 37°C for 30
min. The cells were visualized with diaminobenzidine under a light
microscope after the slides had been irrigated, double stained with
hematoxylin and covered with a cover slip. Positive cells presented
with yellow-brownish particles within cytoplasm. The sections were
evaluated by two experienced physicians from the Department of
Pathology, who were blinded to the study. Next, the sections were
graded by a half-quantitative method: 0 points, <25% positive
target cells; 1 point, 25–50%; 2 points, 51–57%; and 3 points,
>75%. Color visualization was evaluated and graded by the
presence of color or not and the following color scale: 0 points,
no cellular staining; 1 point, light yellow-brownish; 2 points,
yellow-brownish; and 3 points, brown. The final score was
calculated from the sum of the two scores: A score of <2 was
deemed as (−), while a score of 2–3 was defined as (+), 4–5 as (++)
and ≥6 as (+++).
RT-PCR
Extraction of total RNA
The experimental procedures were conducted strictly
according to the manufacturer's instructions. Briefly, total RNA
was extracted from cells using an Invitrogen Trizol RNA extraction
kit (Thermo Fisher Scientific, Inc., Waltham, MA, USA). A total of
1 ml Trizol was used for each sample. The first-strand cDNA was
synthesized from 500 ng total RNA using an iScript cDNA synthesis
kit (Bio-Rad Laboratories, Inc., Hercules, CA, USA). Quantitative
PCR was performed using an icycler iQ™ system (Bio-Rad
Laboratories, Inc.) and the TaqMan-iQ™Supermix kit (Bio-Rad
Laboratories, Inc.). The conditions for RT-PCR are: denaturation at
94°C for 50 sec, annealing at 58°C for 45 sec and extension at
72°C, for a total of 30 cycles.
cDNA synthesis
The total volume of the reaction system was 25 µl,
supplemented with 5 µl 5X RT buffer, 5 µl dNTP, 0.5 µl RNA
template, 5 µl random primer [oligo(dT)], 1 µl reverse
transcriptase M-MLV, 0.5 µl RNAase inhibitor RNasin and 10.5 µl
water free from RNase. Denaturation was performed at 42°C for 60
min and annealing at 95°C for 5 min.
PCR amplification and quantitative analysis
The primers for hTERT and internal standard GAPDH
were designed as follows using Genefisher software (Bielefeld
University, Bielefeld, Germany): hTERT forward,
5′-TTTCTGGAGCTGCTTGGGAA-3′ and reverse, 5′-GAAGAGCCTGAGCAGCTCGA-3′
(44-bp product); and GAPDH forward, 5′-TCCTCTGACTTCAACAGCGACACC-3′
and reverse, 5′-TCTCTCTTCCTCTTGTCGTCTTGG-3′ (286-bp product). With
regard to the amplification system, 5.0 µl 10X PCR buffer, 4.0 µl
MgO, 2 µl dNTP, 2 µl cDNA, 1 µl of each primer (1 mmol/l) and 2 µl
Taq DNA polymerase were used and adjusted to 50 µl by adding double
distilled water. For the amplification conditions, hTERT was
subjected to denaturation at 94°C for 50 sec, annealing at 58°C for
45 sec and extension at 72°C, for a total of 30 cycles. GAPDH
underwent denaturation at 94°C for 30 sec, annealing at 56°C for 30
sec and extension at 72°C, for 26 cycles in total. The PCR
amplification products were subjected to electrophoresis on 1.5%
agarose gels and then images were captured by utilizing the GDS8000
Gel Documentation System (UVP Inc., Upland, CA, USA).
Statistical analysis
The data were analyzed using SPSS 17.0 statistical
software (SPSS, Inc., Chicago, IL, USA) and employed χ2
tests and t-tests. P<0.05 was considered to indicate a
statistically significant difference.
Results
Expression of hTERT protein in HCC and
para-carcinoma tissues
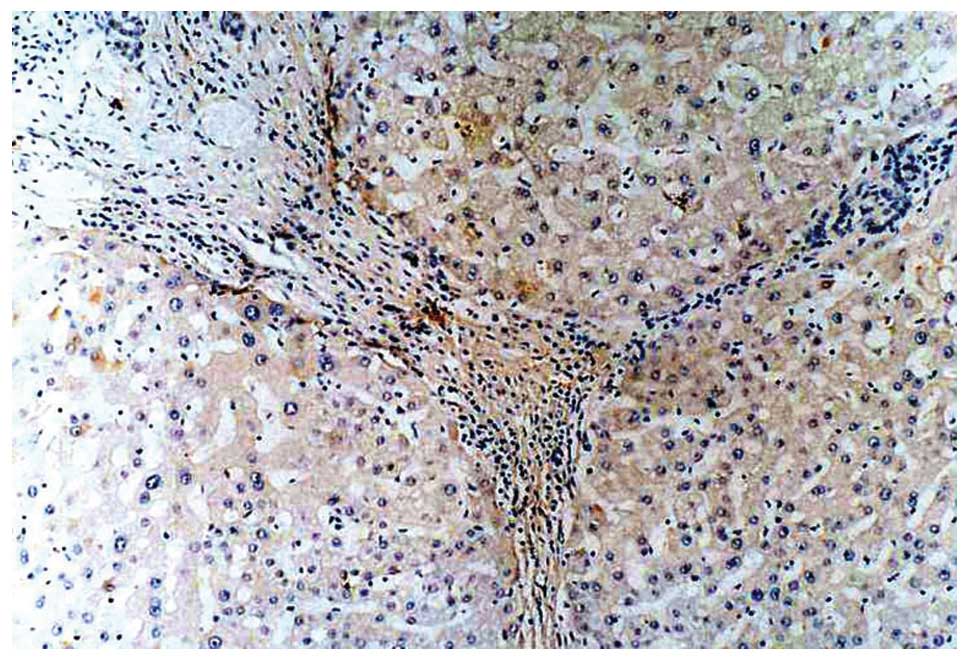
Positive expression of hTERT protein was mainly
observed within the cytoplasm, displayed as yellow-brownish
particles or lamellae staining in the cytoplasm, but was
occasionally also observed in the nucleus. The positive cells were
distributed in a diffuse or dispersed pattern. Positive hTERT
protein expression was observed in 66 out of the 78 HCC tissues
(positive rate, 84.62%; Fig. 1) and
in 8 out of the 78 para-carcinoma tissues (positive rate, 10.26%).
The positive rates significantly differed between the two groups
(P<0.01), as illustrated in Table
I. Among the 78 HCC samples, 36 were graded as (+++), 20 as
(++), 10 as (+) and 12 as (−). For the 78 corresponding
para-carcinoma tissues, positive signals were observed in the
atypical proliferative liver cells of 8 samples (Fig. 2), 1 of which showed weak positive
expression (+) and 2 of which exhibited weak or moderate expression
(++) in the hepatic portal area or few mononuclear cells among
fibrous tissues. No positive expression was observed in the 12
normal liver samples and the negative controls.
 | Table I.Expression of hTERT protein and mRNA
in hepatocellular carcinoma and para-carcinoma tissues. |
Table I.
Expression of hTERT protein and mRNA
in hepatocellular carcinoma and para-carcinoma tissues.
| Specimen | n | hTERT protein
expression, n (positive rate) | χ2 | P-value | hTERT mRNA
expression, n (positive rate) | χ2 | P-value |
|---|
| Liver cancer
tissues | 78 | 66 (84.62) | 76.74 | <0.01 | 61 (78.21) | 74.21 | <0.01 |
| Para-carcinoma
tissues | 78 | 8
(10.26) |
|
| 7 (8.97) |
|
|
Expression of hTERT mRNA in HCC and
para-carcinoma tissues
As shown in Fig. 1,
the positive rate of hTERT mRNA expression was 78.21% (61/78) in
the HCC tissues and 8.97% (7/78) in the para-carcinoma tissues.
Statistical significance was observed between the HCC and
para-carcinoma tissues regarding the positive rate of hTERT mRNA
expression (P<0.01). No hTERT mRNA expression was detected in
the normal hepatic tissues.
Association between hTERT gene
expression and the clinicopathological characteristics of HCC
All patients were grouped according to gender, age,
size of primary tumor, degree of differentiation, the presence of
portal venous tumor thrombosis, serum α-fetoprotein (AFP) level and
the presence of HBsAg. The expression levels of hTERT mRNA were
qualitatively and quantitatively compared. As illustrated in
Table II, and Fig. 3, positive hTERT protein expression at
the translational level and the relative value of hTERT mRNA
expression at the transcriptional level were not correlated with
age, gender or tumor size (P>0.05). The expression level of HCC
samples of Edmondson grades I and II (14) were significantly higher compared with
those of Edmondson grades III and IV (P<0.05), which were
associated with the presence of portal venous tumor thrombosis
(P<0.05), the level of serum AFP (P<0.05) and the presence of
HBsAg (P<0.01).
 | Figure 3.Association between
clinicopathological parameters and expression level of hTERT mRNA
in HCC tissues. Lanes: M, DNA marker; 1, AFP >400 µg/l,
expression level of hTERT mRNA in HCC; 2, AFP <400 µg/l,
expression level of hTERT mRNA in HCC; 3, HBsAg(+), expression
level of hTERT mRNA in HCC; 4, HBsAg(−), expression level of hTERT
mRNA in HCC. Comparison between lanes 2 and 3, P<0.05;
comparison between lanes 4 and 5, P<0.01. GAPDH was used as an
internal standard. hTERT, human telomerase reverse transcriptase;
HCC, hepatocellular carcinoma. |
| Table II.Association between
clinicopathological characteristics and hTERT protein and mRNA
expression in hepatocellular carcinoma tissues. |
Table II.
Association between
clinicopathological characteristics and hTERT protein and mRNA
expression in hepatocellular carcinoma tissues.
| Pathological
indices | Number of cases | Positive expression
rate of hTERT protein (%) | Expression level of
hTERT mRNA (mean ± SD) | P-value |
|---|
| Gender |
|
|
| >0.05 |
| Male | 54 | 88.71 | 1.551±0.020 |
|
|
Female | 24 | 88.69 | 1.539±0.016 |
|
| Age, years |
|
|
| >0.05 |
| ≤50 | 31 | 86.36 | 1.38±0.013 |
|
|
>50 | 47 | 85.71 | 1.575±0.020 |
|
| Tumor size, cm |
|
|
| >0.05 |
|
<5 | 19 | 80.07 | 1.534±0.027 |
|
| ≥5 | 59 | 82.04 | 1.571±0.021 |
|
| Edmondson
classification |
|
|
| <0.05 |
| I–II | 33 | 76.04a |
1.501±0.027a |
|
|
III–IV | 45 | 96.01 | 1.564±0.012 |
|
| Degree of
differentiation |
|
|
| <0.05 |
| Good | 26 | 78.05a |
1.531±0.012a |
|
| Poor | 52 | 95.96 | 1.595±0.025 |
|
| Portal vein tumor
thrombus |
|
|
| <0.05 |
| Yes | 30 | 77.78a |
1.573±0.016a |
|
| No | 48 | 95.99 | 1.504±0.026 |
|
| AFP, µg/l |
|
|
| <0.05 |
|
<400 | 25 | 72.22a |
1.537±0.013a |
|
|
>400 | 53 | 93.18 | 1.574 ±0.024 |
|
| HbsAg |
|
|
| <0.01 |
|
Negative | 20 | 61.54b |
1.501±0.017b |
|
|
Positive | 58 | 97.96 | 1.579±0.025 |
|
|
Discussion
Similar to other malignant tumors, HCC possesses the
vital biological characteristic of cell immortality, which is
acquired mainly from the activation and upregulation of telomerase.
hTERT is a pivotal protein component involved in the regulation of
telomerase. hTERT gene expression complies with the expression of
telomerase activity, which is of great significance for maintaining
the length of chromosome telomeres, preserving unlimited cell
reproduction and proliferation (15–18). The
present study simultaneously detected the expression levels of the
hTERT gene in HCC, para-carcinoma and normal liver tissues from
quantitative, qualitative and localization perspectives. In
particular, the association between hTERT gene expression and the
clinicopathological parameters of HCC tissues were analyzed, which
provided a solid foundation to assess the effect of hTERT in the
incidence and development of HCC. To properly prevent the incidence
of RNA degradation during sample collection and the experimental
procedures, and to minimize the errors resulting from tissue weight
differences and operational errors, the Ct ratio between hTERT and
GAPDG mRNA reverse transcription amplification products with stable
expression was utilized to evaluate the expression level of
hTERT.
Compared with the 62 para-carcinoma tissue samples,
the expression levels of the hTERT gene in the HCC tissues was
significantly enhanced at the translational and transcriptional
levels (both P<0.01), indicating the high positive expression of
the hTERT gene in HCC tissues. The positive expression rates of
hTERT protein and mRNA were 84.62 and 78.21% in the HCC tissues,
which was consistent with the rates of 87.68 and 84.02% reported by
Toshikuni et al (19),
indicating that the high expression of the hTERT gene may be
essential in the incidence and progression of HCC.
The findings in the present study further confirm
that hTERT gene expression is not correlated with patient age,
gender or tumor size (P<0.05), whereas positive expression is
gradually enhanced with the decreased differentiation degree of
HCC, with statistical significance (P<0.05), which is consistent
with the fidnings of previous studies (1,9,10). The quantitative analysis of hTERT
activity revealed that the expression level of HCC of Edmondson
grades III and IV was 1.54±0.012, which was significantly higher
compared with the value of 1.501±0.027 for Edmondson grades I and
II (P<0.05), suggesting that hTERT gene expression is correlated
with the differentiation of HCC. The expression level of hTERT mRNA
was 1.75±0.26 in the patients with portal venous tumor thrombosis,
with a significant difference (P<0.05), indicating that the
hTERT gene is probably associated with the invasion and metastasis
of HCC.
Additionally, when using an AFP level of 400 µg/l as
a standard, the expression of the hTERT gene in the HCC tissues
positive for AFP was significantly higher than that in those
negative for AFP (P<0.05). The expression level of hTERT mRNA in
the HCC patients with HBV infection (presence of HBsAg) was
1.579±0.025, which was significantly higher than the level of
0.501±0.017 in the HBsAg-negative HCC group (P<0.01). These
outcomes indicate that certain effective components corresponding
to HBV interact with hTERT mRNA, and the potential role of these
two factors in the incidence of HCC and the underlying regulatory
mechanism will be the focus of our future investigations.
Taken together, the present results showed that the
activation and expression of hTERT was closely correlated with HCC,
with an extremely vital role in the incidence and progress of HCC
and the invasion and metastasis of tumors. hTERT is a promising
evaluation marker for the diagnosis, malignant progress and
prognosis of HCC, serving as an ideal target for the gene therapy
of the cancer.
Acknowledgements
This study was supported by the Natural Science
Foundation of Shandong Province, China (grant no. Y2008C22) and the
Excellent Youth Scientist Foundation of Shandong Province, China
(grant no. 2007BS03038).
References
|
1
|
Iliopoulos D, Satra M, Drakaki A,
Poultsides GA and Tsezou A: Epigenetic regulation of hTERT promoter
in hepatocellular carcinomas. Int J Oncol. 34:391–399.
2009.PubMed/NCBI
|
|
2
|
Vente MA, Wondergem M, van der Tweel I,
van den Bosch MA, Zonnenberg BA, Lam MG, van Het Schip Ad and
Nijsen JF: Yttrium-90 microsphere radioembolization for the
treatment of liver malignancies: A structured meta-analysis. Eur
Radiol. 19:951–959. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wong PY, Xia V, Imagawa DK, Hoefs J and Hu
KQ: Clinical presentation of hepatocellular carcinoma (HCC) in
Asian-Americans versus non-Asian-Americans. J Immigr Minor Health.
13:842–848. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
El-Serag HB: Hepatocellular carcinoma. N
Engl J Med. 365:1118–1127. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chen CJ, Yang HI, Su J, Jen CL, You SL,
Huang GT and Iloeje UH: REVEAL-HBV Study Group: Risk of
hepatocellular carcinoma across a biological gradient of serum
hepatitis B virus DNA level. JAMA. 295:65–73. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huo LF, Tang JW, Huang JJ, Huang PT, Huang
CF, Kung HF and Lin MC: Cancer immunotherapy targeting the
telomerase reverse transcriptase. Cell Mol Immunol. 3:1–11.
2006.PubMed/NCBI
|
|
7
|
Mizukoshi E, Nakamoto Y, Marukawa Y, Arai
K, Yamashita T, Tsuji H, Kuzushima K, Takiguchi M and Kaneko S:
Cytotoxic T cell responses to human telomerase reverse
transcriptase in patients with hepatocellular carcinoma.
Hepatology. 43:1284–1294. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wu KJ, Grandori C, Amacker M, Simon-Vermot
N, Polack A, Lingner J and Dalla-Favera R: Direct activation of
TERT transcription by c-MYC. Nat Genet. 21:220–224. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Saini N, Srinivasan R, Chawla Y, Sharma S,
Chakraborti A and Rajwanshi A: Telomerase activity, telomere length
and human telomerase reverse transcriptase expression in
hepatocellular carcinoma is independent of hepatitis virus status.
Liver Int. 29:1162–1170. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li JH, Liu Y, Wang HF, et al: Construction
of hTERT promoter-driven TRAIL expression vector and its inhibitory
effects on hepatoma cell proliferation. Journal of Jilin University
(medicine edition). 36:825–831. 2010.(In Chinese).
|
|
11
|
Yang YJ, Chen H, Huang P, Li CH, Dong ZH
and Hou YL: Quantification of plasma hTERT DNA in hepatocellular
carcinoma patients by quantitative fluorescent polymerase chain
reaction. Clin Invest Med. 34:E2382011.PubMed/NCBI
|
|
12
|
Qian Y, Yang L and Cao S: Telomeres and
telomerase in T cells of tumor immunity. Cell Immunol. 289:63–69.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tabori U, Ma J, Carter M, Zielenska M,
Rutka J, Bouffet E, Malkin D and Hawkins C: Human telomere reverse
transcriptase expression predicts progression and survival in
pediatric intracranial ependymoma. J Clin Oncol. 24:1522–1528.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Edmondson HA and Steiner PE: Primary
carcinoma of the liver: A study of 100 cases among 48,900
necropsies. Cancer. 7:462–503. 1954. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Takahashi S, Kitamoto M, Takaishi H,
Aikata H, Kawakami Y, Nakanishi T, Shimamoto F, Tahara E, Tahara H,
Ide T, et al: Expression of telomerase component genes in
hepatocellular carcinomas. Eur J Cancer. 36:496–502. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang PH, Zou L and Tu ZG: RNAi-hTERT
inhibition hepatocellular carcinoma cell proliferation via
decreasing telomerase activity. J Surg Res. 131:143–149. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Miura N, Osaki Y, Nagashima M, Kohno M,
Yorozu K, Shomori K, Kanbe T, Oyama K, Kishimoto Y, Maruyama S, et
al: A novel biomarker TERTmRNA is applicable for early detection of
hepatoma. BMC Gastroenterol. 10:462010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lanson NA Jr, Friedlander PL,
Schwarzenberger P, Kolls JK and Wang G: Replication of an
adenoviral vector controlled by the human telomerase reverse
transcriptase promoter causes tumor-selective tumor lysis. Cancer
Res. 63:7939–7941. 2003.
|
|
19
|
Toshikuni N, Nouso K, Higashi T,
Nakatsukasa H, Onishi T, Kaneyoshi T, Kobayashi Y, Kariyama K,
Yamamoto K, Tsuji T, et al: Expression of telomerase associated
protein 1 and telomerase transcriptase in hepatocellular carcinoma.
Br J Cancer. 82:833–837. 2000. View Article : Google Scholar : PubMed/NCBI
|