Introduction
Aneurysmal bone cyst (ABC) is an uncommon benign
bone tumor, more commonly affecting children than adults (1). It is mostly observed in the spine and
long bones (2). ABC was first
reported by Jaffe and Lichtenstein in 1942 (3), although the pathogenic mechanism that
produces these benign lesions is still not completely understood.
The symptoms include local swelling, pain and related functional
disorders. X-ray computed tomography (CT) scan, contrast-enhanced
CT and three-dimensional reconstruction may be used in the
diagnosis of ABC. The inferior turbinate (inferior nasal concha) is
considered an independent osteocomma with its own ossification
center. Pneumatized inferior turbinate was first described by
Zinreich et al in 1988 (4),
and is rarely observed in the clinic (5). Sinus CT examination is the gold standard
for the diagnosis of inferior turbinate gasification, with
snuffles, headache and weeping among the common clinical symptoms.
Herein we report the case of an ABC on the left zygomatic arch
concomitant with bilateral inferior turbinate gasification in an
adult female.
The study was performed in accordance with the
Declaration of Helsinki on medical protocol and ethics, and was
approved by the regional Ethical Review Board of China-Japan Union
Hospital (Changchun, China). Written informed consent was obtained
from the patient for the publication of this study and accompanying
images.
Case report
A 34-year-old Chinese Han female, suffering from
hyperplasia of the left maxillary bone for one and a half years,
was admitted to the China-Japan Union Hospital in June 2008. The
patient was otherwise healthy and had no history of giant cell
tumor, osteochondritis, hemangioma, chondroblastoma or trauma.
Routine examinations revealed that a bony prominence with a
diameter of 1.5 cm was present in the middle area of the patient's
left zygomatic arch. The bony prominence felt rigid and was
painless. There was no notable difference between the skin covering
the bony prominence and the surrounding skin.
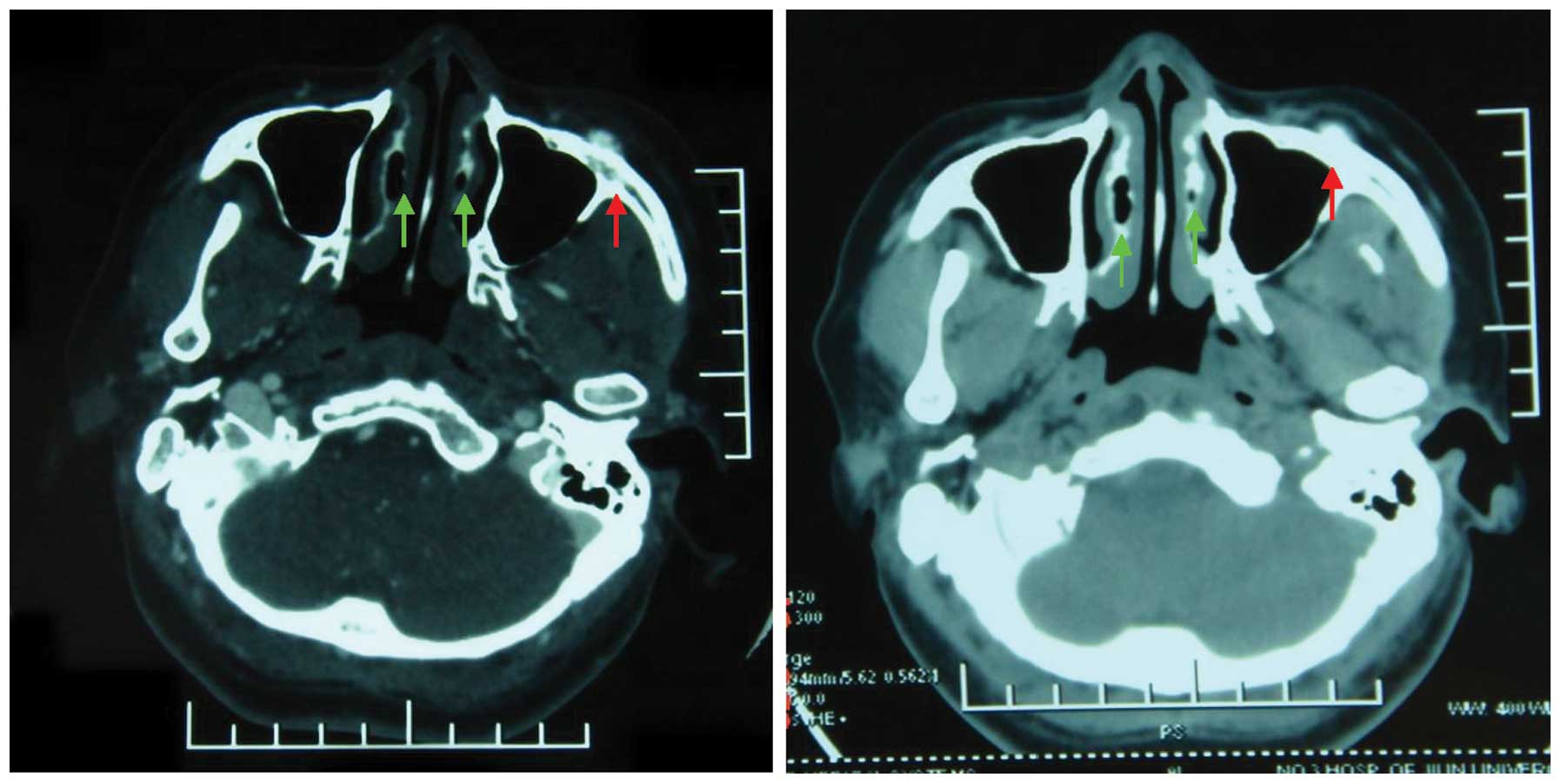
CT scans of the paranasal sinus revealed bilateral
inferior turbinate gasification and a round, alveolate high-density
cyst on the left zygomatic arch (Fig.
1). The cyst had a clear boundary and was close to the lateral
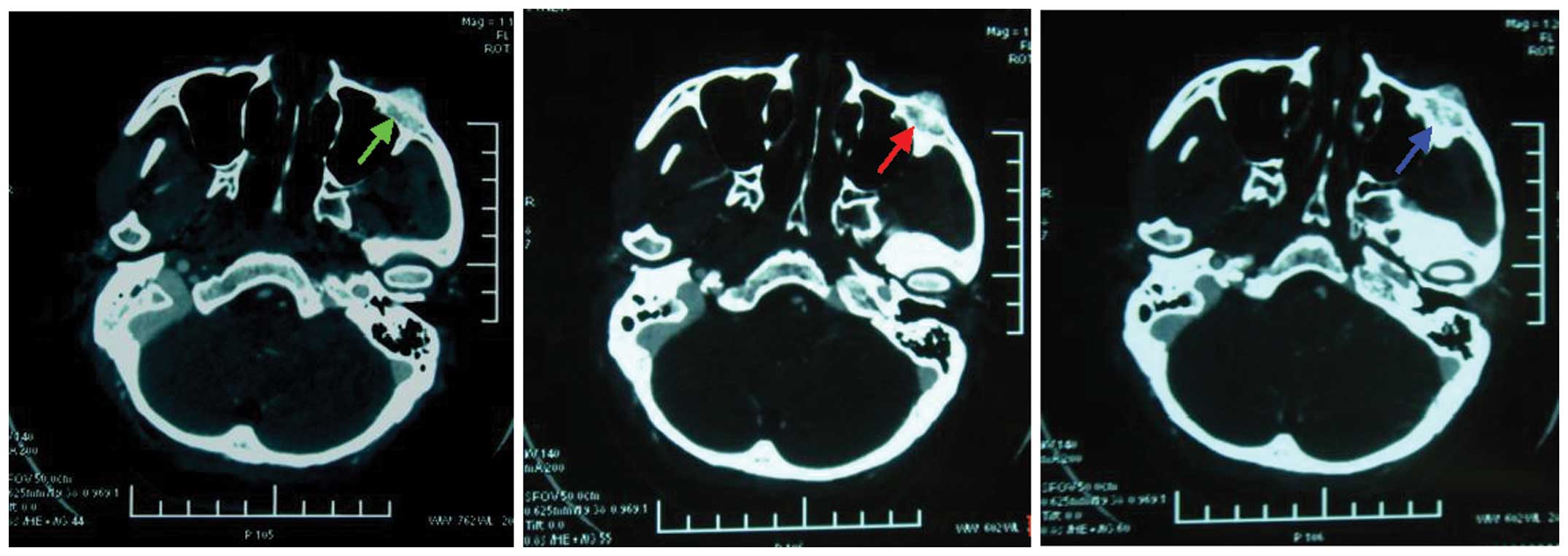
wall of the left maxillary sinus. The contrast-enhanced CT scans
revealed no distinctive enhancement characteristics in either the
arterial or venous phases (Fig. 2).
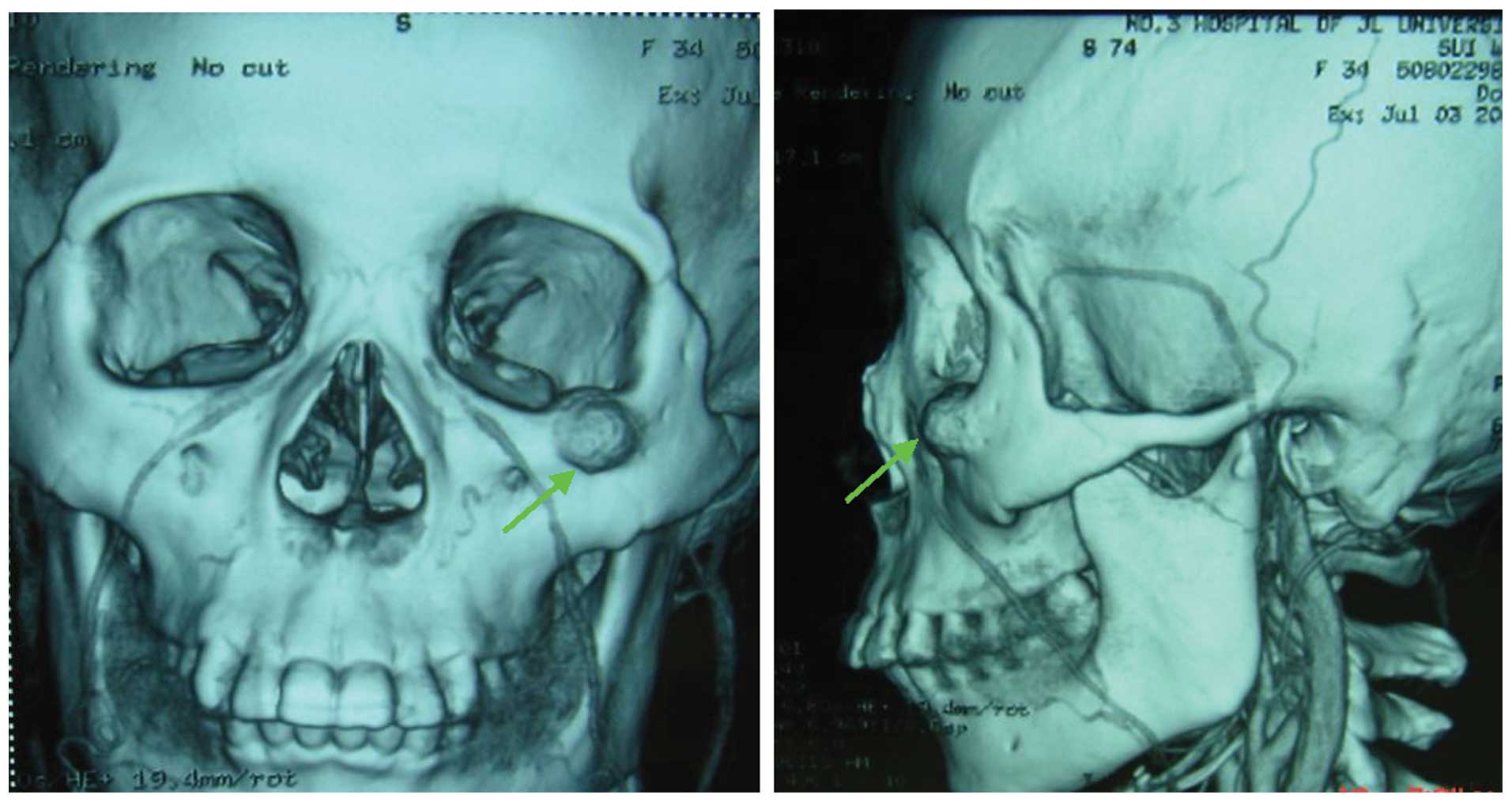
In addition, three-dimensional maxillofacial reconstruction
revealed a round cyst located in the area where the left zygomatic
arch intersected the maxillary bone (Fig.
3). The surface of the cyst was fairly smooth, and the superior
wall of the left maxillary sinus was intact.
The patient underwent resection of the cyst on the
left maxillary bone. On examination, the cyst appeared alveolate,
and no clear boundary could be identified with the surrounding
normal bones. Arterial blood was drawn by puncture, and compression
was applied to stop the bleeding. Curettage of the cyst was
performed. The left maxillary sinus was not affected by the
cyst.
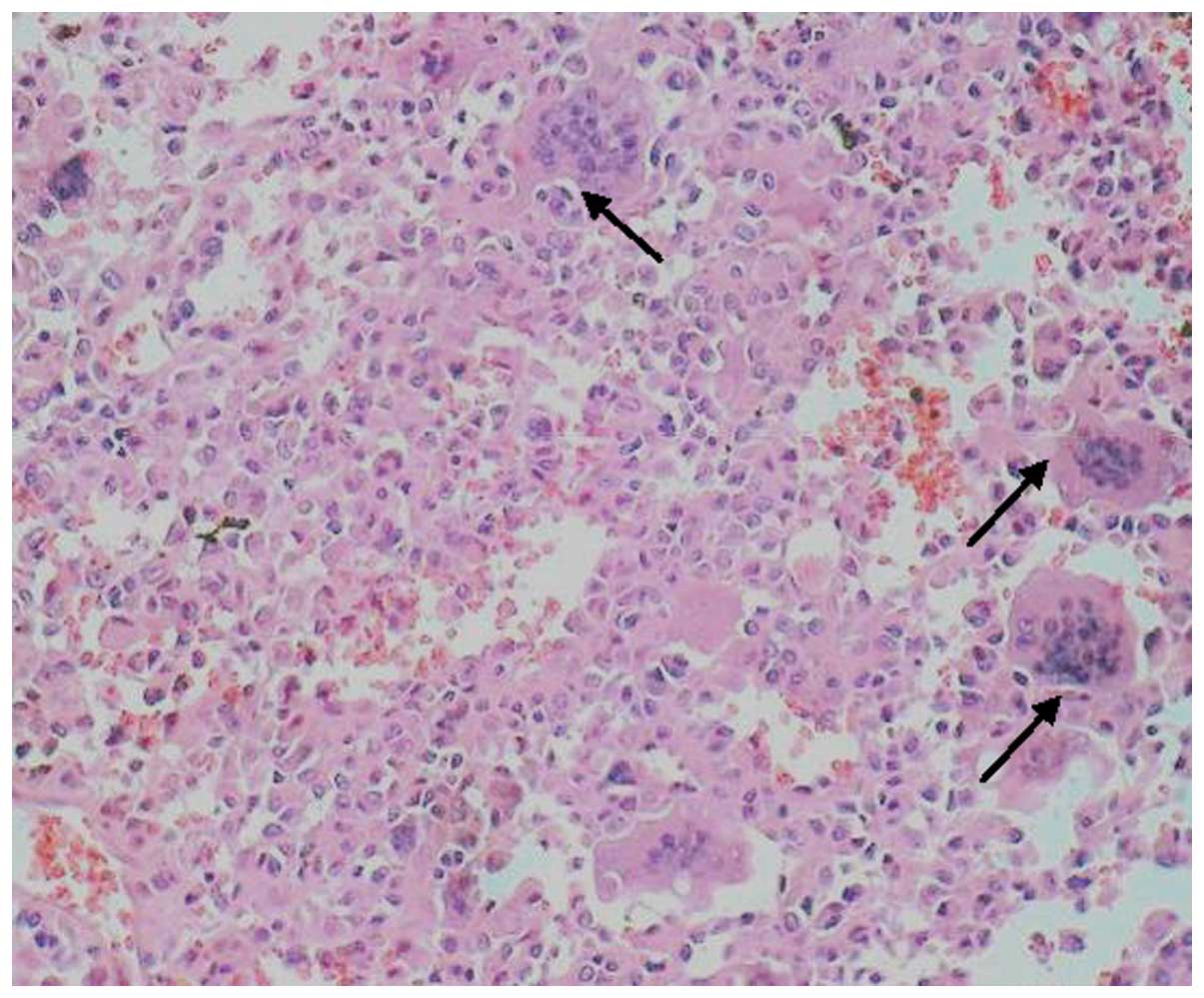
The blood lacuna and connective tissue compartment
are shown in Fig. 4. Tissue cells and
osteoclast-like multinuclear giant cells were observed under an
optical microscope. There was no evidence of new reactive bone
formation.
The patient was followed up for 4 years. The ABC did
not reoccur and no other postoperative symptoms were observed.
Discussion
The majority of ABC cases occur in the spine or long
bones of female patients less than 20 years old (6,7). In
general, the pathophysiology of ABC is consequential rather than
causal, induced by hemodynamic abnormalities in local blood vessels
due to giant cell tumor, osteochondritis, hemangioma,
chondroblastoma or trauma. An ABC on the zygomatic arch is rather
rare.
In the present study, an alveolate high-density cyst
was present on the left zygomatic arch of the patient. Her left
maxillary sinus was not affected by the cyst. The ABC in this case
was considered primary, as no notable antecedent disease was
observed, although the pathogenic mechanism was unclear.
The standard treatment for ABCs consists mainly of
surgical resection, which may involve a simple cyst resection or
radical resection. The necessity of a bone graft depends on the
size of the bone defect (8). The
resection area is custom-determined by the characteristics of the
pre-existing lesion. If the lesion is caused by trauma or the
etiology is unclear, a pure cyst resection should be performed.
Alternatively, arterial embolization may be applied in those cases
where surgical resection is not feasible, and the clinical outcome
is considered equal to that of surgery (9). There is no consensus with regard to
whether radiotherapy should be applied before surgery, to reduce
intraoperative hemorrhage, or after surgery, to reduce the risk of
recurrence. However, compression with control is recommended if
required to alleviate bleeding, as intraoperative hemorrhage is
common. In particular, severe bleeding usually occurs when the cyst
is large. In these cases artery ligation combined with
interventional vascular embolization may be applied to reduce
bleeding prior to surgery. The recurrence rate of ABC has been
reported to be 20%, and 90% of these cases occurred within two
years of surgery (6). The recurrence
rate is generally correlated with the etiology, and ABCs induced by
giant cell tumor or trauma recurred relatively frequently.
The inferior turbinate is an independent bone that
originates from the lateral nasal wall. It is covered with a thick
mucous membrane that contains a plexus cavernosus (10). Pneumatized inferior turbinate has been
rarely reported in the clinical setting (11), and reports of bilateral inferior
turbinate gasification are rarer still (12,13). The
potential pathogenic mechanisms for inferior turbinate gasification
include: i) pneumatization induced by involvement of epithelial
cells in the cartilage framework of the inferior turbinate; ii)
disease in the maxillary sinus; iii) articulation defects between
the maxillary process of the palatine bone and the maxillary
bone.
In the present case, there were no evident clinical
symptoms for bilateral inferior turbinate gasification; it was
identified incidentally through CT examination of the ABC.
Therefore, none of the three pathogenic mechanisms described above
apply in this case. Oztürk et al (14) indicated that the formation of inferior
turbinate gasification may also be gene-related. Winnepenninckx
et al (15) reported that a
specific gene (mapped to 17p13) was involved in the development of
an ABC. Therefore, we consider that a gene abnormality might be
responsible in the present case, as the ABC and inferior turbinate
gasification were maxillofacial and characterized by a bubble
change in the bone substance. However, gene mutation screening was
refused by the patient so this cannot be confirmed.
This study constitutes the first case report of an
ABC on the left zygomatic arch concomitant with bilateral inferior
turbinate gasification, observed in a Chinese Han female who was
successfully treated with surgical resection of the cyst. The case
was considered to be associated with an abnormality of specific
genes.
References
|
1
|
Zenonos G, Jamil O, Governale LS, Jernigan
S, Hedequist D and Proctor MR: Surgical treatment for primary
spinal aneurysmal bone cysts, experience from Children's Hospital
Boston. J Neurosurg Pediatr. 9:305–315. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dekeuwer P, Odent T, Cadilhac C, Journeau
P, Langlais J, Padovani JP, Glorion C and Pouliquen JC: Aneurysmal
bone cyst of the spine in children, a 9-year follow-up of 7 cases
and review of the literature. Rev Chir Orthop Reparatrice Appar
Mot. 89:97–106. 2003.(In French). PubMed/NCBI
|
|
3
|
Jaffe HL and Lichtenstein L: Solitary
unicameral bone cyst: with emphasis on the roentgen picture the
pathologic appearance and the pathogenesis. Arch Surg.
44:1004–1025. 1942. View Article : Google Scholar
|
|
4
|
Zinreich SJ, Mattox DE, Kennedy DW,
Chisholm HL, Diffley DM and Rosenbaum AE: Concha bullosa, CT
evaluation. J Comput Assist Tomogr. 12:778–784. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pittore B: AlS afi W and Jarvis SJ: Concha
bullosa of the inferior turbinate: an unusual cause of nasal
obstruction. Acta Otorhinolaryngol Ital. 31:47–49. 2011.PubMed/NCBI
|
|
6
|
Triantafillidou K, Venetis G, Karakinaris
G, Iordanidis F and Lazaridou M: Variable histopathological
features of 6 cases of aneurysmal bone cysts developed in the jaws,
review of the literature. J Craniomaxillofac Surg. 40:e33–e38.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rajput D, Tungaria A, Jaiswal A and Jain
V: Aneurysmal bone cyst of clivus and C1 C2: case report and review
of literature. Turk Neurosurg. 22:105–108. 2012.PubMed/NCBI
|
|
8
|
Karabouta I, Tsodoulos S and Trigonidis G:
Extensive aneurysmal bone cyst of the mandible, surgical resection
and immediate reconstruction. Histopathology. Oral Surg Oral Med
Oral Pathol. 71:148–150. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Donati D, Frisoni T, Dozza B, DeGroot H,
Albisinni U and Giannini S: Advance in the treatment of aneurysmal
bone cyst of the sacrum. Skeletal Radiol. 40:1461–1466. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Christmas DA Jr, Merrell RA Jr, Mirante JP
and Yanagisawa E: Pneumatized inferior turbinate: report of three
cases. Ear Nose Throat J. 83:152–153. 2004.PubMed/NCBI
|
|
11
|
Uzun L, Ugur MB and Savranlar A:
Pneumatization of the inferior turbinate. Eur J Radiol. 51:99–101.
2004.
|
|
12
|
Gocmen H, Oğuz H, Ceylan K and Samim E:
Infected inferior turbinate pneumatization. Eur Arch
Otorhinolaryngol. 262:979–981. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kharoubi S: Pneumatization (concha
bullosa) of the inferior turbinate: case report and literature
review. Rev Laryngol Otol Rhinol (Bord). 131:321–324. 2010.(In
French). PubMed/NCBI
|
|
14
|
Oztürk A, Alataş N, Oztürk E, San I,
Sirmatel O and Kat N: Pneumatization of the inferior turbinates,
incidence and radiologic appearance. J Comput Assist Tomogr.
29:311–314. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Winnepenninckx V, Debiec-Rychter M,
Jorissen M, Bogaerts S and Sciot R: Aneurysmal bone cyst of the
nose with 17p13 involvement. Virchows Arch. 439:636–639. 2001.
View Article : Google Scholar : PubMed/NCBI
|