Introduction
Endocrine-associated types of cancer in humans
exhibit gender-specific hormonal responsiveness; for example,
androgen responsiveness for prostate cancer in males, and estrogen
responsiveness for breast cancer in females (1). As the normal growth of certain tissues
(including the prostate and breast) is dependent upon specific
hormones, it is reasonable to assume that these hormones may be
involved in malignant growth of these organs. Under normal
conditions, hormone-stimulated tissue growth is well-modulated and
controlled and, even with continuous exposure to hormones, tissues
do not undergo unlimited growth (2).
Malignant growth of organs in response to hormones may be
attributed to upregulated activity of growth signals, or the
downregulation of signals that normally inhibit proliferation
(2).
Estrogen has a significant role in the occurrence,
malignant progression and prognosis of breast cancer (3). Estrogen receptors (ERs) and the genes
they regulate have additionally been studied as primary targets in
clinical treatment for the control of breast cancer (4). For example, ERα gene expression is a
significant event in breast cancer, and its overexpression may be
an initiating event in carcinogenesis. However, ERβ has been
identified to be highly expressed in normal and malignant breast
tissue (5,6). Previous studies have additionally
demonstrated co-expression of ERβ and ERα in human breast cancer
cells (7–9). Expression of ERα is identified in ~60%
of breast cancer tissues, and types of cancer demonstrating this
expression are known as ER-dependent (10). The majority of these ERα-positive
breast cancer cases are sensitive to endocrine therapy; however,
30% of them demonstrate endocrine therapy resistance (11). Therefore, we hypothesize that ERβ has
become an alternative indicator for the sensitivity of breast
cancer to endocrine therapy, and a promising target for the control
of tumor growth.
In the present study, immunohistochemical staining
was performed to detect the expression levels of ERβ in
postmenopausal ERα-positive breast cancers. In addition, the
influence of differential ERβ expression on the efficacy of
endocrine therapy, as well as on disease-free survival rate, was
analyzed in these patients. The importance of ERβ in guiding
endocrine therapeutic strategies for the treatment of breast
cancer, and its role in disease prognosis were evaluated to provide
a basis for determining maximum benefit in clinical treatment.
Materials and methods
Patient samples
The clinical inclusion criteria for patient samples
were as follows: i) Postmenopausal females with stage I or II
breast cancer, according to the 7th edition of the American Joint
Committee on Cancer staging manual (12); ii) ERα-positivity on
immunohistochemical staining; iii) patient underwent radical or
modified radical mastectomy; iv) cancer pathologically confirmed to
be infiltrating ductal carcinoma; and v) presence of complete
clinical and follow-up data. In total, 207 patients met these
criteria and were included in the present study. These patients
were diagnosed with breast cancer and surgically treated at the
First Affiliated Hospital of Xinjiang Medical University (Urumqi,
China), between January 2000 and December 2010. The patients were
followed up for 2–12 years. During the follow-up period, 12
patients were censored. Of the 195 patients with effective
follow-up, 140 patients were treated with endocrine therapy, whilst
55 patients were not treated with endocrine therapy.
Recurrence diagnosis was based on pathological
evidence confirmed by biopsy. Lymph node and distant metastases
were detected using CT (computed tomography), ultrasound, X-ray,
emission CT or magnetic resonance imaging. Disease-free survival
time was calculated from the date of surgery, and recurrence or
metastasis was counted on the date of diagnosis thereof.
Prior written and informed consent was obtained from
all patients, and the study was approved by the ethical review
board of Xinjiang Medical University.
Immunohistochemical staining
Breast cancer tissue specimens were fixed in 10%
formaldehyde for 24 h and subsequently embedded in paraffin. Tissue
specimens were sliced into 3-µm sections and placed in a 70°C oven
overnight. Sections were subsequently dewaxed in xylene (Beijing
Zhongshan Golden Bridge Biotechnology Co., Ltd., Beijing, China)
for 20 min and rehydrated in graded alcohols. Endogenous peroxidase
activity was blocked using a 3% solution of hydrogen peroxide
(Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd.) for 10
min. For antigen retrieval, sections were placed in EDTA antigen
retrieval solution (Beijing Zhongshan Golden Bridge Biotechnology
Co., Ltd.) and boiled for 20 min. Following cooling to room
temperature and washing with phosphate-buffered saline (PBS; Wuhan
Boster Biological Technology, Ltd., Wuhan, China), sections were
incubated with polyclonal rabbit anti-human ERβ primary antibody
(cat. no. BY-02101; 1:100; Shanghai Yueyan Biological Technology,
Co., Ltd., Shanghai, China), at 37°C for 1 h in the dark.
Subsequently, sections were incubated with horseradish
peroxidase-conjugated goat anti-rabbit IgG secondary antibodies
(cat. no. K500711; 1:200; Shanghai Gene Biological Technology Co.,
Ltd., Shanghai, China). at 37°C for 30 min in the dark. Following
antibody incubation, sections were developed using
3,3′-diaminobenzidine chromogenic reagent (Beijing Zhongshan Golden
Bridge Biotechnology Co., Ltd.) for 5 min and counterstained by
hematoxylin (Beijing Zhongshan Golden Bridge Biotechnology Co.,
Ltd.). Following hydrochloric acid differentiation and dehydration
in graded alcohols, sections were mounted using neutral gum
(Beijing Zhongshan Golden Bridge Biotechnology Co., Ltd.).
ERβ-positive breast cancer tissue samples served as positive
controls. In the negative controls, secondary antibody was replaced
by PBS.
Immunohistochemical staining results were evaluated
by an experienced pathologist. Cells exhibiting brown staining were
classified as ERβ-positive cells. A total of five random high-power
fields were evaluated using a Leica DM LB2 microscope (Leica,
Wetzlar, Germany). The ERβ-positive rate was the ratio of the
number of ERβ-positive cells to the total number of cells in each
field. An ERβ-positive rate <1% was defined as ERβ-negative [ERβ
(−)]. A positive rate of 1–10% was defined as ERβ-weak-positive
[ERβ (+)]. An ERβ-positive rate of 11–70% was defined as
ERβ-positive [ERβ (++)]. An ERβ-positive rate >70% was defined
as ERβ-strong-positive [ERβ (+++)]. Expression levels of ERα were
classified into the following four categories: ERα-negative (−),
<30% positive rate; ERα-weak-positive (+), 30–40% positive rate;
ERα-positive (++), 40–60% positive rate; and ERα-strong-positive
(+++), >60% positive rate (13).
HER-2 expression levels were defined according to the 2009 HER-2
Detection Guide (14), as follows:
HER-2 (−), no staining; HER-2 (+), weak or incomplete cell membrane
staining; HER-2 (++), 10–30% of invasive cancer cells exhibiting
weak to moderate, complete but non-uniform membrane staining; HER-2
(++), >30% of invasive cancer cells showing strong, complete and
uniform membrane staining.
Statistical analysis
SPSS version 17.0 (SPSS, Inc., Chicago, IL, USA) was
used for statistical analyses. The rank-sum test was utilized for
evaluation of the association between ERβ expression levels and
clinical indices. Disease-free survival rates were calculated using
the Kaplan-Meier method. The log-rank test was utilized to compare
the disease-free survival rates between groups with varying ERβ
expression levels. Cox regression analysis was performed to assess
the influence of ERβ expression levels and additional
clinicopathological indices on the disease-free survival rates of
postmenopausal breast cancer patients. P<0.05 was considered to
indicate a statistically significant difference.
Results
ERβ overexpression decreases the
disease-free survival rate and affects the prognosis of
postmenopausal patients with ERα-positive breast cancer
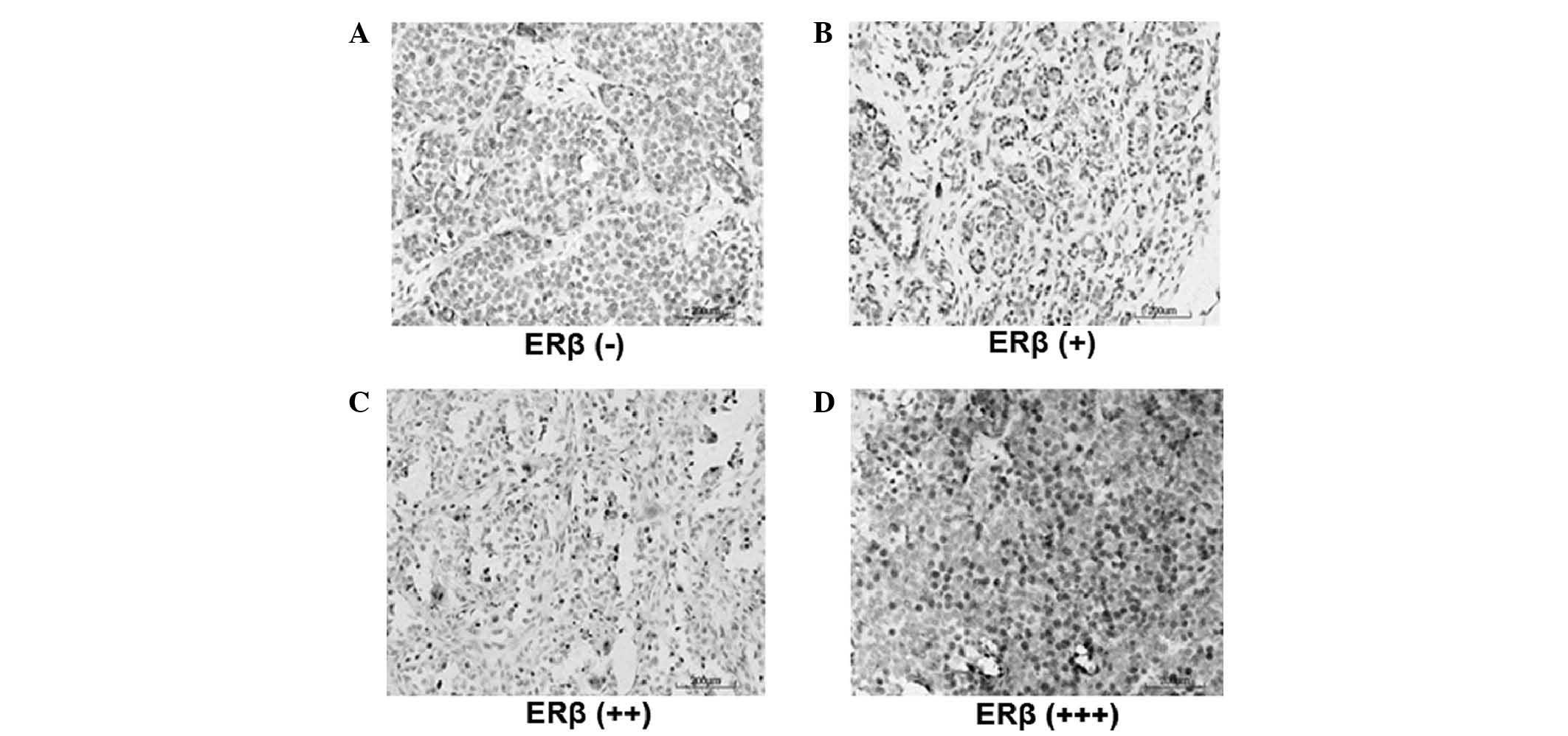
In order to investigate the role of ERβ in the
development and progression of breast cancer, the expression levels
of ERβ in ERα-positive patients were detected by
immunohistochemistry. Representative immunohistochemical results
are shown in Fig. 1. Cells exhibiting
brown staining were considered ERβ-positive cells. Based on the
percentage of ERβ-positive cells, ERβ expression was divided into
four groups: ERβ (−) (Fig. 1A), ERβ
(+) (Fig. 1B), ERβ (++) (Fig. 1C) and ERβ (+++) (Fig. 1D). Subsequently, the association
between clinicopathological index and ERβ expression was evaluated.
As revealed in Table I, lymph node
metastasis, clinical stage, and ERα and HER2 expression levels were
not significantly correlated with ERβ expression levels (P=0.372,
P=0.576, P=0.578 and P=0.068, respectively). By contrast, tumor
diameter did demonstrate a significant correlation with ERβ
expression levels (P=0.002); higher ERβ expression levels
accompanied greater tumor diameters.
 | Table I.Association between
clinicopathological indices and ERβ expression levels in
postmenopausal ERα-positive breast cancer patients (n=195),
investigated by rank sum test. |
Table I.
Association between
clinicopathological indices and ERβ expression levels in
postmenopausal ERα-positive breast cancer patients (n=195),
investigated by rank sum test.
| Clinicopathological
features | No. of cases | Mean rank-order | P-value |
|---|
| Tumor diameter,
cm |
|
|
|
| ≤2 | 100 | 86.85 | 0.002a |
|
>2 | 95 | 109.74 |
|
| Lymph node
metastasis |
|
|
|
| L=0 | 139 | 95.09 | 0.372 |
| 1≤
L<4 | 39 | 94.27 |
|
|
L>4 | 17 | 112.91 |
|
| Clinical stage |
|
|
|
| I | 79 | 95.51 | 0.576 |
| II | 116 | 99.70 |
|
| ERα expression
level |
|
|
|
| + | 94 | 95.27 | 0.578 |
| ++ | 81 | 98.60 |
|
| +++ | 20 | 108.40 |
|
| HER2 expression
level |
|
|
|
| − | 104 | 91.15 | 0.068 |
| +/++ | 43 | 112.37 |
|
| +++ | 48 | 99.96 |
|
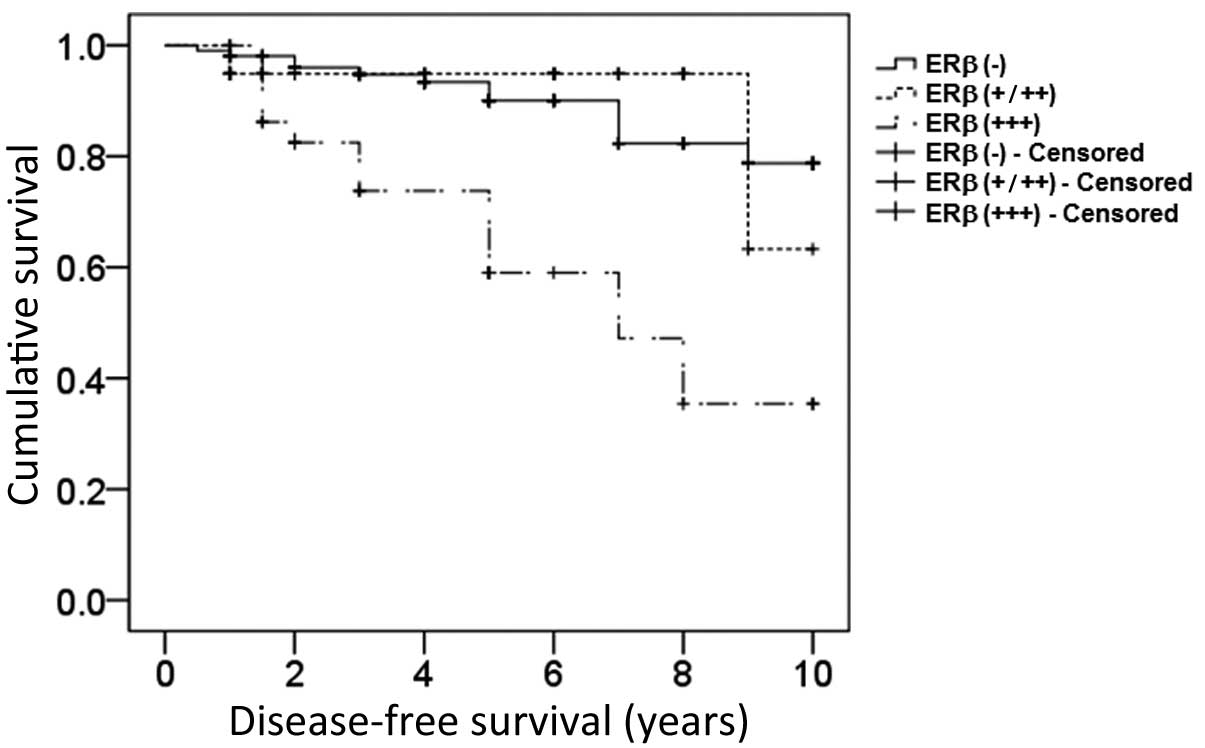
Subsequently, it was investigated whether ERβ
expression affected the disease-free survival rate and prognosis of
postmenopausal patients with ERα-positive breast cancer. The
results demonstrated that ERβ overexpression significantly
decreased the disease-free survival rate in postmenopausal breast
cancer patients (log-rank test, 20.277; P=0.002; Fig. 2). Furthermore, Cox regression analysis
revealed that neither chemotherapy, radiotherapy or endocrine
therapy were independent prognostic factors, while late clinical
stage and ERβ overexpression represented independent prognostic
risk factors for postmenopausal breast cancer patients [P=0.001;
odds ratio (OR), >1; Table
II].
| Table II.Analysis of prognostic factors by Cox
regression analysis in ERα-positive postmenopausal breast cancer
patients (n=195). |
Table II.
Analysis of prognostic factors by Cox
regression analysis in ERα-positive postmenopausal breast cancer
patients (n=195).
| Clinicopathological
features | β coefficient | SEM | Wald value | P-value | Odds ratio | 95% CI |
|---|
| ERβ expression
level |
|
|
|
|
|
|
| − | NA | NA | 14.911 | 0.001a | NA | NA |
| +/++ | –0.223 | 0.664 | 0.113 | 0.737 | 0.800 | 0.218–2.943 |
| +++ | 1.529 | 0.447 | 11.699 | 0.001a | 4.612 | 1.921–11.074 |
| Clinical stage | NA | NA | 7.687 | 0.021a | NA | NA |
| II | 1.440 | 0.629 | 5.246 | 0.022a | 4.223 | 1.231–14.484 |
| III | 2.084 | 0.768 | 7.366 | 0.007a | 8.037 | 1.784–36.199 |
| Chemotherapy | 0.325 | 0.514 | 0.398 | 0.528 | 1.384 | 0.505–3.792 |
| Radiotherapy | 0.266 | 0.472 | 0.317 | 0.573 | 1.305 | 0.517–3.293 |
| Endocrine
therapy | 0.410 | 0.525 | 0.608 | 0.435 | 1.506 | 0.538–4.217 |
ERβ overexpression decreases the
disease-free survival rate and affects the prognosis of
ERα-positive postmenopausal breast cancer patients treated with
endocrine therapy
In order to identify whether ERβ overexpression
influenced the therapeutic effects of endocrine therapy,
disease-free survival rate and prognosis were assessed in
postmenopausal ERα-positive breast cancer patients treated with
endocrine therapy. As demonstrated in Fig. 3, the upregulated expression of ERβ
significantly decreased the disease-free survival rate in
postmenopausal breast cancer patients treated with endocrine
therapy (log-rank test, 19.473; P=0.003). In addition, Cox
regression analysis indicated that expression levels of ERβ were
the only independent prognostic factor, with ERβ overexpression
representing the prognostic risk factor (P=0.013; OR, >1), while
clinical stage, chemotherapy, and radiotherapy were not independent
factors (P=0.066, P=0.562 and P=0.871, respectively; Table III).
| Table III.Analysis of prognostic factors by Cox
regression analysis in postmenopausal ERα-positive breast cancer
patients treated with endocrine therapy (n=140). |
Table III.
Analysis of prognostic factors by Cox
regression analysis in postmenopausal ERα-positive breast cancer
patients treated with endocrine therapy (n=140).
| Clinicopathological
features | β coefficient | SEM | Wald value | P-value | Odds ratio | 95% CI |
|---|
| ERβ expression
level |
|
|
|
|
|
|
| − | NA | NA | 8.729 | 0.013a | NA | NA |
|
+/++ | −1.118 | 222.746 | 0.003 | 0.960 | <0.001 | 3.502–5.606 |
|
+++ | 1.472 | 0.498 | 8.726 | 0.003a | 4.612 | 1.641–11.570 |
| Clinical stage | NA | NA | 5.422 | 0.066 | NA | NA |
| II | 1.388 | 0.784 | 3.136 | 0.077 | 4.006 | 0.862–18.612 |
|
III | 2.040 | 0.877 | 5.410 | 0.020 | 7.693 | 1.379–42.937 |
| Chemotherapy | 0.333 | 0.574 | 0.336 | 0.562 | 1.395 | 0.453–4.295 |
| Radiotherapy | 0.099 | 0.609 | 0.026 | 0.871 | 1.104 | 0.335–3.642 |
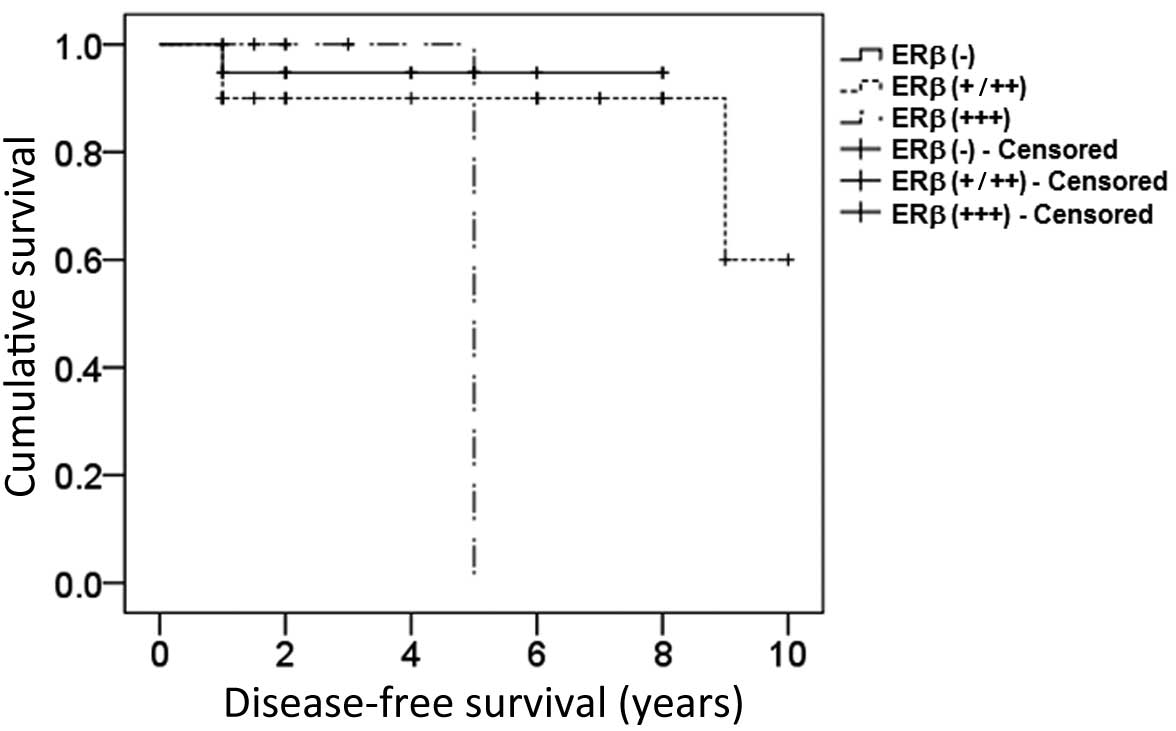
ERβ expression levels do not affect
disease-free survival rate or prognosis in ERα-positive
postmenopausal breast cancer patients without endocrine
therapy
To further clarify the specific influence of ERβ
expression on endocrine therapy in postmenopausal breast cancer,
the association between ERβ expression levels and disease-free
survival rate or prognosis in breast cancer patients without
endocrine therapy was investigated. The results suggested that the
expression levels of ERβ were not statistically correlated with
disease-free survival of postmenopausal breast cancer patients
without endocrine therapy (log-rank test, 2.291; P=0.102; Fig. 4). Cox regression analysis indicated
that neither clinical stage, chemotherapy, radiotherapy or ERβ
expression levels represented independent prognostic risk factors
in breast cancer patients not treated with endocrine therapy
(P=0.496, P=0.990, P=0.497 and P=0.368, respectively; Table IV).
| Table IV.Analysis of prognostic factors by Cox
regression analysis in postmenopausal ERα-positive breast cancer
patients not treated with endocrine therapy (n=55). |
Table IV.
Analysis of prognostic factors by Cox
regression analysis in postmenopausal ERα-positive breast cancer
patients not treated with endocrine therapy (n=55).
| Clinicopathological
features | β coefficient | SEM | Wald value | P-value | Odds ratio | 95% CI |
|---|
| ERβ expression
level |
|
|
|
|
|
|
| − | NA | NA | 2.001 | 0.368 | NA | NA |
|
+/++ | 0.372 | 1.194 | 0.097 | 0.756 | 1.450 | 0.140–15.062 |
|
+++ | 1.539 | 1.251 | 1.512 | 0.219 | 4.659 | 0.401–54.123 |
| Clinical stage | 0.785 | 1.153 | 0.463 | 0.496 | 2.192 | 0.229–20.987 |
| Chemotherapy | −13.121 | 1076.095 | 0.000 | 0.990 | <0.001 | NA |
| Radiotherapy | 0.622 | 0.916 | 0.461 | 0.497 | 1.862 | 0.309–11.223 |
Discussion
ERβ serves a significant role in the genesis and
progression of breast cancer, and expression levels of ERβ have
been observed to be associated with endocrine therapy resistance
(15,16). However, whether ERβ expression causes
breast cancer to become more sensitive or resistant to endocrine
therapy remains to be elucidated. Chang et al (17) suggested that high mRNA expression of
ERβ may influence the therapeutic effects of endocrine drugs,
leading to endocrine therapy resistance. However, Esslimani-Sahla
et al (18) revealed that ERβ
overexpression was able to increase the sensitivity of breast
cancer to endocrine therapy. In the present study, an
immunohistochemical assay was used to assess the expression levels
of ERβ in postmenopausal ERα-positive breast cancer patients, and
the association between ERβ expression levels and endocrine therapy
efficacy or disease-free survival rate were additionally
investigated. The results provided evidence of the significance of
ERβ expression in the endocrine therapy resistance of breast
cancer, and provided experimental data that may be useful for the
individualized assessment of endocrine therapy and prognosis in
breast cancer patients.
In the current study, Cox regression analysis was
used to assess the effects of clinical stage, chemotherapy,
radiotherapy and endocrine therapy on the prognosis of ERα-positive
breast cancer in postmenopausal patients. The results demonstrated
that clinical stage and ERβ expression levels represented
independent prognostic factors for postmenopausal ERα-positive
breast cancer (P=0.001) while, for breast cancer patients treated
with endocrine therapy, ERβ overexpression was the only independent
prognostic risk factor (P=0.003; OR=4.612). These findings suggest
that ERβ expression may have a direct impact on ERα-positive breast
cancer prognosis in patients treated with endocrine therapy, and
ERβ overexpression may lead to endocrine therapy resistance. Chung
et al (19) revealed that the
expression levels of ERβ may affect the transcription of certain
genes. Downregulated ERβ expression modulates cell cycle- and
apoptosis-associated genes via the transforming growth factor-β
signaling pathway, and inhibits cell proliferation-associated genes
(20). This indicates that ERβ
expression represents a risk factor during the carcinogenesis of
breast cancer. In agreement with this, Park et al (21) identified that ERβ expression levels
were negatively associated with the histological grading of breast
cancer, and ERβ overexpression indicated poor prognosis for breast
cancer patients. In the present study, the results from the patient
group without endocrine therapy suggested there was no significant
association between ERβ expression levels and the disease-free
survival rate of breast cancer patients (P=0.205). Cox regression
analysis revealed that clinical stage, postoperative chemotherapy,
radiotherapy and ERβ expression levels were not significantly
associated with disease prognosis, indicating that ERβ expression
levels were not a prognostic factor for breast cancer patients not
treated with endocrine therapy. Based on the above results, ERβ may
represent an independent prognostic factor for ERα-positive breast
cancer patients treated with endocrine therapy. It is thus proposed
that, in ERα-positive postmenopausal breast cancer patients, ERβ
may influence breast cancer prognosis via affecting endocrine
therapy efficacy, and its overexpression is closely correlated with
endocrine therapy resistance. However, in order to achieve a
definite conclusion, additional evidence from postmenopausal breast
cancer patient samples not treated with endocrine therapy is
required.
In conclusion, ERβ overexpression resulted in
endocrine therapy resistance and poor prognosis in postmenopausal
ERα-positive breast cancer patients treated with endocrine therapy,
which suggested that ERβ may be useful as an indicator for the
assessment of endocrine therapy efficacy. ERβ expression evaluation
may provide evidence for whether certain breast cancer patients are
suitable for endocrine therapy and may be used as an indicator of
individual endocrine therapy efficacy.
Acknowledgements
The present study was supported by the Natural
Science Foundation of Xinjiang Uygur Autonomous Region (grant no.
2011211A069) and the National Clinical Key Subject-General Surgery
Construction Project (grant no. 2100299).
References
|
1
|
De Coster S, van Leeuwen DM, Jennen DG,
Koppen G, Den Hond E, Nelen V, Schoeters G, Baeyens W, van Delft
JH, Kleinjans JC and van Larebeke P: Gender-specific transcriptomic
response to environmental exposure in Flemish adults. Environ Mol
Mutagen. 54:574–588. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bergan HE, Kittilson JD and Sheridan MA:
PKC and ERK mediate GH-stimulated lipolysis. J Mol Endocrinol.
51:213–224. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nair HB, Perla RP, Kirma NB, Krishnegowda
NK, Ganapathy M, Rajhans R, Nair SS, Saikumar P, Vadlamudi RK and
Tekmal RR: Estrogen receptor-beta mediates the protective effects
of aromatase induction in the MMTV-Her-2/neu × aromatase double
transgenic mice. Horm Cancer. 3:26–36. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ali S and Coombes RC: Estrogen receptor
alpha in human breast cancer: Occurrence and significance. J
Mammary Gland Biol Neoplasia. 5:271–281. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Omoto Y, Inoue S, Ogawa S, Toyama T,
Yamashita H, Muramatsu M, Kobayashi S and Iwase H: Clinical value
of the wild-type estrogen receptor beta expression in breast
cancer. Cancer Lett. 163:207–212. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Roger P, Sahla ME, Mäkelä S, Gustafsson
JA, Baldet P and Rochefort H: Decreased expression of estrogen
receptor beta protein in proliferative preinvasive mammary tumors.
Cancer Res. 61:2537–2541. 2001.PubMed/NCBI
|
|
7
|
Hayashi SI, Eguchi H, Tanimoto K, Yoshida
T, Omoto Y, Inoue A, Yoshida N and Yamaguchi Y: The expression and
function of estrogen receptor alpha and beta in human breast cancer
and its clinical application. Endocr Relat Cancer. 10:193–202.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fox EM, Davis RJ and Shupnik MA: ERbeta in
breast cancer - onlooker, passive player, or active protector?
Steroids. 73:1039–1051. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Edge SB, Byrd DR, Compton CC, et al:
Breast. AJCC cancer staging manual (7th). (New York, NY). Springer.
347–376. 2010.
|
|
10
|
Osborne CK and Schiff R: Mechanisms of
endocrine resistance in breast cancer. Annu Rev Med. 62:233–247.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mestron A, Webb SM, Astorga R, et al:
Epidemiology, clinical characteristics, outcome, morbidity and
mortality in acromegaly based on the Spanish Acromegaly Registry
(Registro Espanol de Acromegalia, REA). Eur J Endocrinol.
151:439–446. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li SL and Chen XPWK: The biological
characteristics and clinical treatments of breast cancer. Sl L:
Beijing: Science Press. 2004.
|
|
13
|
Hammond ME, Hayes DF, Wolff AC, Mangu PB
and Temin S: American society of clinical oncology/college of
american pathologists guideline recommendations for
immunohistochemical testing of estrogen and progesterone receptors
in breast cancer. J Oncol Pract. 6:195–197. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Guideline Recommendations for HER2
Detection in Breast Cancer Group: Guidelines for HER2 detection in
breast cancer, the 2009 version. Zhonghua Bing Li Xue Za Zhi.
38:836–840. 2009.(In Chinese). PubMed/NCBI
|
|
15
|
Yager JD and Davidson NE: Estrogen
carcinogenesis in breast cancer. N Engl J Med. 354:270–282. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chaves VE, Júnior FM and Bertolini GL: The
metabolic effects of growth hormone in adipose tissue. Endocrine.
44:293–302. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chang HG, Kim SJ, Chung KW, Noh DY, Kwon
Y, Lee ES and Kang HS: Tamoxifen-resistant breast cancers show less
frequent methylation of the estrogen receptor beta but not the
estrogen receptor alpha gene. J Mol Med (Berl). 83:132–139. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Esslimani-Sahla M, Simony-Lafontaine J,
Kramar A, Lavaill R, Mollevi C, Warner M, Gustafsson JA and
Rochefort H: Estrogen receptor beta (ER beta) level but not its ER
beta cx variant helps to predict tamoxifen resistance in breast
cancer. Clin Cancer Res. 10:5769–5776. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chung YL, Sheu ML, Yang SC, Lin CH and Yen
SH: Resistance to tamoxifen-induced apoptosis is associated with
direct interaction between Her2/neu and cell membrane estrogen
receptor in breast cancer. Int J Cancer. 97:306–312. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mosselman S, Polman J and Dijkema R: ER
beta: Identification and characterization of a novel human estrogen
receptor. FEBS Lett. 392:49–53. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Park BW, Kim KS, Heo MK, Ko SS, Hong SW,
Yang WI, Kim JH, Kim GE and Lee KS: Expression of estrogen
receptor-beta in normal mammary and tumor tissues: Is it protective
in breast carcinogenesis? Breast Cancer Res Treat. 80:79–85. 2003.
View Article : Google Scholar : PubMed/NCBI
|