Introduction
Cavernous sinus hemangiomas (CSHs) are rare
extra-axial vascular neoplasms that reportedly account for <2%
of cavernous sinus tumors, both benign and malignant (1,2). CSHs
differ from other intra-axial cavernous malformations in the brain
as they represent true vascular neoplasms, and the associated
symptoms are produced as a result of progressive growth of the
tumor and mass effects (3).
The optimal treatment strategy for this condition
remains controversial. Microsurgical approaches may lead to severe
bleeding and even operative death (4,5). As
radiotherapy prior to surgical resection has demonstrated some
benefit, radiosurgery appears to be a promising treatment modality
for the management of lesions in the cavernous sinus. Recently,
radiosurgery is being used for primary or postoperative management
of patients with CSHs and favorable treatment results have been
reported (1,6).
Thus, the current study was conducted with the aim
of evaluating the efficacy and safety of Gamma Knife radiosurgery
(GKS) in the management of CSHs.
Materials and methods
Patient characteristics
Between August 2011 and April 2014, 7 patients with
CSH who were treated by GKS were enrolled into this retrospective
study. With regard to prior treatments, 2 patients had undergone
surgical resection prior to GKS, while the remaining 5 patients
underwent GKS as a primary treatment under the typical neuroimaging
diagnosis including sharply delineated tumors, low to isointense
mass lesions on T1-weighted images, extremely high intensity on
T2-weighted images (as bright as cerebrospinal fluid signal), and
strong homogeneous or heterogeneous enhancement in
gadolinium-enhanced imagine, as described elsewhere (1,7,8).
GKS protocol
All treatments were performed using the Leksell
Gamma Knife Perfexion™ (Elekta AB, Stockholm, Sweden). The Leksell
Model G stereotactic frame (Elekta AB) was applied to the patient's
head under local anesthesia. A high resolution and thin-slice
volumetric, gadolinium-enhanced magnetic resonance imaging (MRI)
scan was obtained the day prior to treatment. Using the GammaPlan
software (Elekta AB, Crawley, UK), the neurosurgeon and medical
physicists designed the dose plan. The radiosurgery isodose,
maximum dose and marginal dose were initially determined according
to the tumor volume calculated during dose planning. Multiple
isocenter planning was used to minimize the radiation exposure of
the optic pathway and other critical neural structures.
Follow-up examinations
Following treatment, all patients received regular
clinical and radiological follow-up at intervals of 3 months during
the first year, and at 6-month intervals thereafter. Tumor control
was classified as ‘remarkable shrinkage’ (tumor volume on follow-up
images of <50% of the volume prior to GKS), ‘minimal shrinkage’
(tumor volume of 50–75% of the tumor volume prior to GKS) or
‘stationary’ (tumor volume of 75–125% of the tumor volume prior to
GKS). ‘Tumor progression’ covered all other circumstances (9).
Results
Among the patient group, there were 2 males and 5
females, with a median age of 50.0 years (range, 39–64 years). The
predominant symptoms and signs were headache, or symptoms related
to diplopia and ophthalmoplegia. The clinical characteristics of
the patients and treatment parameters are summarized in Table I.
 | Table I.Summary of the characteristics of
patients with cavernous sinus hemangioma. |
Table I.
Summary of the characteristics of
patients with cavernous sinus hemangioma.
|
|
|
|
|
| Tumor volume
(cm3) |
|
|
|---|
|
|
|
|
|
|
|
|
|
|---|
| Age (years) | M/F | Presenting
symptom | Pre-GKS
treatment | Dose (Gy) | IntraGKS | End | Follow-up
(months) | Volume reduction |
|---|
| 45 | F | Headache | None | 14 | 10.5 | 5.9 | 6 | MS |
| 59 | M | Diplopia | Surgery | 15 | 3.8 | 1.1 | 12 | RS |
| 63 | F | Facial
hypoesthesia | None | 14 | 10.6 | 2.2 | 22 | RS |
| 41 | F | Diplopia | Biopsy | 10 | 33.2 | 2.5 | 40 | RS |
| 39 | F | Headache | None | 12 | 17.5 | 2.0 | 28 | RS |
| 50 | M | Ophthalmoplegia | None | 15 | 6.5 | 1.2 | 16 | RS |
| 64 | F | Headache | None | 15 | 5.3 | 1.3 | 18 | RS |
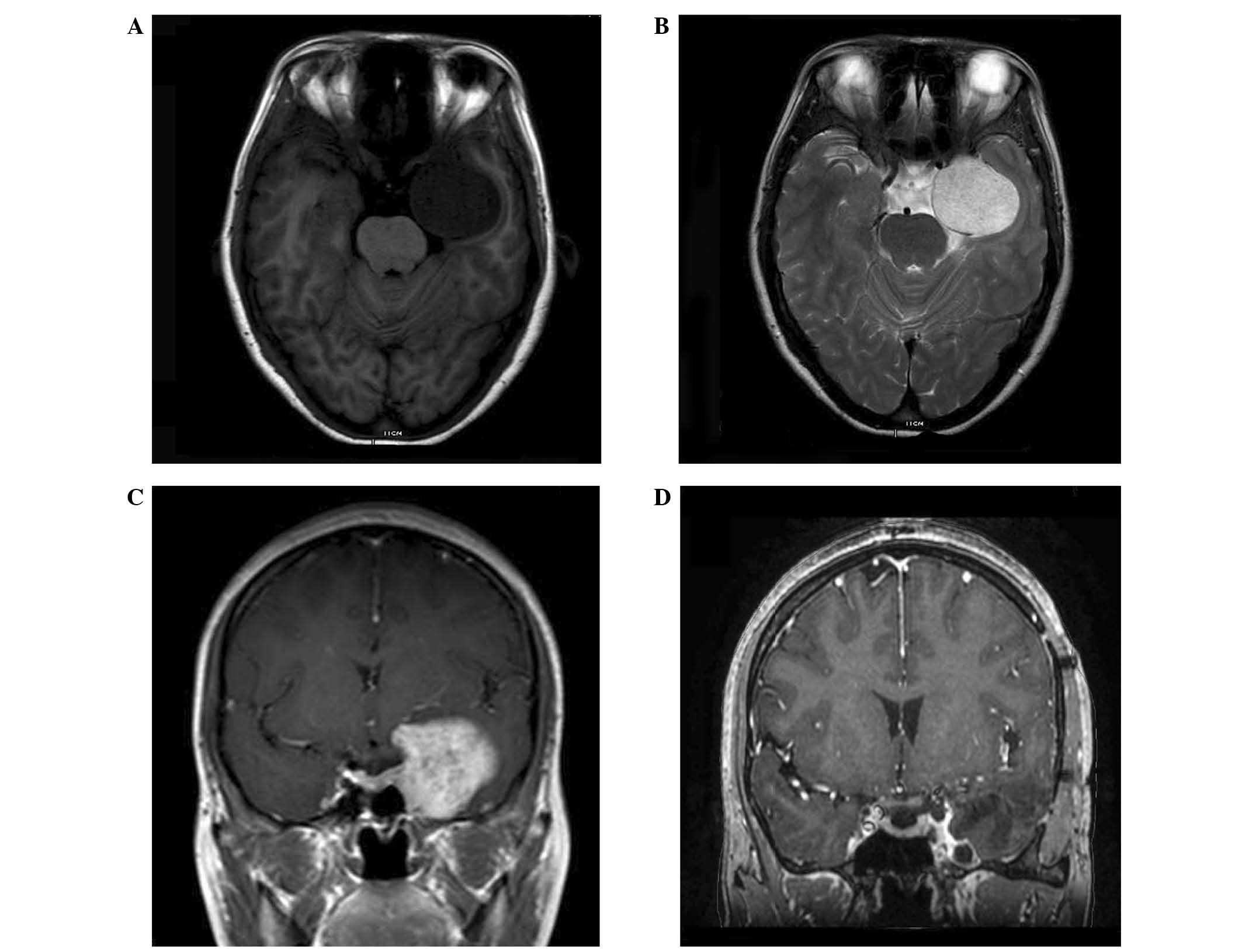
Radiologically, an iso or low signal intensity on
T1-weighted MRI, and a bright, high signal intensity on T2-weighted
MRI was observed in all patients. All tumors exhibited strong
enhancement following administration of the contrast medium
gadolinium-diethylene triamine pentaacetic acid (Fig. 1A–C).
At the time of radiosurgery, the mean volume of the
CSHs was 12.5±10.2 cm3 (range, 5.3–33.2 cm3),
and the median marginal dose at the 50% isodose line was 14.0 Gy
(range, 10.0–15.0 Gy).
Tumor control was achieved in all patients during
the follow-up period. Remarkable shrinkage was achieved in 6
patients and minimal shrinkage was achieved in 1 patient. The
patient with minimal shrinkage was observed during the 6 months
follow-up, and the volume was reduced from 10.5 cm3 to
5.9 cm3 (reduced 44%). In another patient with 40 months
of follow-up, the tumor volume reduced from 33.2 cm3 to
2.5 cm3, only 7.5% of the initial volume. No patients
experienced tumor progression prior to the date of last
follow-up.
The most common presenting symptom was cranial
neuropathy, which affected 4 patients. In these patients, remission
of cranial neuropathies was observed following treatment by GKS.
Headache was present in 3 patients and was completely resolved
following treatment. No adverse radiation effects were observed in
the patients during the follow-up period.
Discussion
Although recent advances in microsurgical techniques
have been made, the use of surgery to remove CSHs is frequently
challenging (5); this is due to the
critical anatomical structures located in the cavernous sinus, and
the persistent bleeding from the tumor during surgical resection or
even attempted biopsy sampling (6).
In a study by Linskey et al (4), in which 52 surgical cases in the
literature were reviewed, the total removal rate was only 44%, and
cranial neuropathies were exacerbated by surgery in 12 patients
(44.4%).
For patients with residual or inoperable tumors,
radiotherapy often demonstrates benefits in terms of remarkable
tumor shrinkage (10,11). Considering the proximity of the optic
nerve and optic chiasm, which are considered to be organs at risk
of damage during radiotherapy, the use of stereotactic irradiation
is increasing (6). Iwai et al
(12) reported the first case of CSHs
treated with GKS in 1999. Since that time, GKS has been used for
primary or postoperative management of patients with CSHs, and
favorable treatment results have been reported (1,6,13).
A previous meta-analysis reported that stereotactic
radiosurgery (SRS) is an effective and safe treatment option for
patients with CSHs; tumor shrinkage was identified in >90% of
patients, and new cranial neuropathies developed in only 1.7% of
patients (1). In the present study,
remarkable post-GKS tumor shrinkage was also identified without
causing any new deficits. The long-term results appear to be
favorable, and no surgical interventions have been required so
far.
The marginal doses delivered to the lesions require
the thorough consideration of radiation injury of the critical
structures around the cavernous sinus, including the optic
apparatus. Nakamura et al (14) suggested that the treatment of CSHs
necessitated lower radiosurgical doses compared with those required
for other benign tumors. Yamamoto et al (6) analyzed dose-treatment responses in 38
reported cases of CSH treated with radiosurgery, suggesting that a
peripheral dose of 14–15 Gy was sufficient for controlling CSH
growth, and that 10–12 Gy was the threshold dose for the control of
tumor growth. In the current study, 1 patient who was diagnosed by
biopsy had a tumor volume of 33.2 cm3 and was treated
with a low marginal dose (10 Gy). The tumor volume was subsequently
reduced to only 7.5% of the initial volume, which indicated that
CSH were highly radiosensitive. The ipsilateral abducens nerve
palsy was observed to be in a state of partial remission during the
40 months of follow-up (Fig. 1D).
The current study had several limitations, including
its small sample size, lack of pathological confirmation and
relatively short follow-up period. However, the results may still
be helpful considering the prompt response of the CSHs to GKS
relatively soon after treatment, and given the rarity of CSHs.
In conclusion, GKS appears to be an effective and
safe treatment modality for the management of CSHs, and may be used
as a primary treatment in such cases. Further studies with
long-term follow-up and larger numbers of cases are necessary to
optimize the treatment conditions and verify the benefit of this
treatment.
Glossary
Abbreviations
Abbreviations:
|
CSH
|
cavernous sinus hemangioma
|
|
GKS
|
Gamma Knife radiosurgery
|
|
MRI
|
magnetic resonance imaging
|
|
SRS
|
stereotactic radiosurgery
|
References
|
1
|
Wang X, Mei G, Liu X, Dai J, Pan L and
Wang E: The role of stereotactic radiosurgery in cavernous sinus
hemangiomas: A systematic review and meta-analysis. J Neurooncol.
107:239–245. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gliemroth J, Missler U and Sepehrnia A:
Cavernous angioma as a rare neuroradiologic finding in the
cavernous sinus. J Clin Neurosci. 7:554–557. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chou CW, Wu HM, Huang CI, Chung WY, Guo
WY, Shih YH, Lee LS and Pan DH: Gamma knife surgery for cavernous
hemangiomas in the cavernous sinus. Neurosurgery. 67:611–616. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Linskey ME and Sekhar N: Cavernous sinus
hemangiomas: A series, a review and an hypothesis. Neurosurgery.
30:101–108. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhou LF, Mao Y and Chen L: Diagnosis and
surgical treatment of cavernous sinus hemangiomas: An experience of
20 cases. Surg Neurol. 60:31–36. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yamamoto M, Kida Y, Fukuoka S, Iwai Y,
Jokura H, Akabane A and Serizawa T: Gamma Knife radiosurgery for
hemangiomas of the cavernous sinus: A seven-institute study in
Japan. J Neurosurg. 112:772–777. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fraser JF, Mass AY, Brown S, Anand VK and
Schwartz TH: Transnasal endoscopic resection of a cavernous sinus
hemangioma: Technical note and review of the literature. Skull
Base. 18:309–315. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kida Y, Kobayashi T and Mori Y:
Radiosurgery of cavernous hemangiomas in the cavernous sinus. Surg
Neurol. 56:117–123. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Song SW, Kim DG, Chung HT, Paek SH, Han
JH, Kim YH, Kim JW, Kim YH and Jung HW: Stereotactic radiosurgery
for cavernous sinus hemangiomas. J Neurooncol. 118:163–168. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rigamonti D, Pappas CT, Spetzler RF and
Johnson PC: Extracerebral cavernous angiomas of the middle fossa.
Neurosurgery. 27:306–310. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Shibata S and Mori K: Effect of radiation
therapy on extracerebral cavernous hemangioma in the middle fossa.
Report of three cases. J Neurosurg. 67:919–922. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Iwai Y, Yamanaka K, Nakajima H and Yasui
T: Stereotactic radiosurgery for cavernous sinus cavernous
hemangioma-case report. Neurol Med Chir (Tokyo). 39:288–290. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Thompson TP, Lunsford LD and Flickinger
JC: Radiosurgery for hemangiomas of the cavernous sinus and orbit:
Technical case report. Neurosurgery. 47:778–783. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nakamura N, Shin M, Tago M, Terahara A,
Kurita H, Nakagawa K and Ohtomo K: Gamma knife radiosurgery for
cavernous hemangiomas in the cavernous sinus. Report of three
cases. J Neurosurg. 97:477–480. 2002.PubMed/NCBI
|