Introduction
The majority of fetal cardiac tumors are primary
tumors (1) that usually occur in the
heart or pericardial cavities, with rhabdomyoma being the most
common tumor type (2). Fetal cardiac
tumors are rare, with a global incidence rate of ~0.14% (2). Notably, rhabdomyoma is frequently
associated with tuberous sclerosis (2). Heart tumors are 20–30 times more common
than pericardial tumors and 75% of primary heart tumors are benign;
malignant heart tumors are identified less frequently (3). In 1982, DeVore et al used
prenatal ultrasonic examination to diagnose fetal cardiac tumors
and to evaluate the function of the fetal heart (4,5). Since
then, ultrasonic examination has been widely used for fetal
screening, allowing for the majority of fetal cardiac tumors to be
detected (6). However, successful
resection of such tumors is rare, and literature regarding
intraoperative monitoring is limited. On ultrasonic examination,
rhabdomyoma generally exhibits a uniform high echo, a myocardial
echo which is stronger than normal and tuberous sclerosis may also
be present. The identification of multiple tumors is common, and
such tumors may cause significant hemodynamic disturbances as a
result of outflow obstruction or arrhythmias (7). The occurrence of cardiac tumors may
cause numerous types of serious blood disorder in fetuses and
neonates and may cause fetal mortality. Thus, it is necessary to
dynamically monitor the fetal cardiac hemodynamic change (8) and to continuously evaluate the function
of the fetal heart by echocardiography (9,10).
Accurate prenatal ultrasonic examination of the fetal heart
demonstrates important clinical value for the treatment and
clinical decision making of fetal cardiac tumors (11).
Materials and methods
Patients
Between January 2012 and January 2014, 9113 female
patients underwent obstetric ultrasound examination at The First
Hospital of Nanchang University (Nanchang, Jiangxi, China), and 8
of the fetuses were found to possess occupying lesions of the fetal
heart. In total, 2 out of 8 patients were primipara and the other 6
were multipara. The patients were aged between 20 and 35 years old,
with a gestational age between 21 and 34 weeks. None of the
patients possessed a history of family genetic diseases or birth
history of fetus malformation. The effect of sib mating was not
considered in the present study. The current study was conducted in
accordance with the Declaration of Helsinki (12) and with approval from the Ethics
Committee of Nanchang University (Nanchang, Jiangxi, China).
Written informed consent was obtained from all participants.
Detection of fetal heart
Voluson E8 TruScan (GE Healthcare, Chalfont St
Giles, UK) and IU22 Color Doppler Ultrasonic Diagnostic System
(Philips, Amsterdam, Netherlands) were used in the present study. A
virtual convex probe (GE Healthcare) was used at the frequency of
3.5 MHz. The fetal heart model was chosen to observe the four
cavities, long axis of the ventriculus sinister, outflow tract of
the left and right ventriculus, three vessels view, three vessels
and trachea view, short axis of the main artery, aortic arch and
ductus arteriosus arch view, in order to determine whether the
structure of the heart and blood flow were normal. This was also
performed to comprehensively identify the presence of
space-occupying masses in the heart cavity, ventricular wall or
pericardial cavity at multiple angles. The location, morphology,
size, quantity and activity of the masses could then be accurately
described. Combined with the spectrum Doppler ultrasonography, the
effect of the masses on the left and right outflow tract and
atrioventricular and semilunar valves was determined. The induction
of fetal cardiac hemodynamic changes was also determined, in
addition to the presence of abnormal cardiac function (4).
Detection of the complications
To comprehensively identify whether the fetus
possessed complications such as other malformations outside the
heart, the ultrasonic probe was switched to the common middle-late
pregnancy ultrasound mode. In this mode, it was mainly determined
whether there were abnormal echoes or space-occupying masses in the
other fetal organs or brain. All imaging data were entered into the
ultrasonic workstation at The First Hospital of Nanchang
University. Written and informed consent for the use of the
prenatal ultrasound examination was obtained from each patient.
Results
Out of the 8 fetuses identified to possess fetal
cardiac tumors, 2 fetuses possessed tumors located within one
cardiac ventricle and 6 fetuses possessed tumors located in
multiple ventricular cavities or ventricular walls. In total, 6
patients requested termination of the pregnancy and the other 2
patients continued with the pregnancy. Out of the 8 fetuses with
cardiac tumors, only 2 demonstrated arrhythmia.
All 8 fetuses possessed a hyperechoic or slightly
hyperechoic mass, without evident pedicle, and the masses did not
move in large amplitude with cardiac contraction and diastole. No
significant hemodynamic disorder or induced obstruction of valves
was identified (Table I).
 | Table I.Ultrasonic manifestation of the fetal
cardiac tumors identified in 8 fetuses. |
Table I.
Ultrasonic manifestation of the fetal
cardiac tumors identified in 8 fetuses.
| No. | Gestational age,
weeks | Single or multiple
lesions | Echo | Location of mass | Activity | Pathological
diagnoses |
|---|
| 1 | 23 | Single | Hyperechoic | Left ventricle | Tiny | Rhabdomyoma,
confirmed by color ultrasound following birth |
| 2 | 21 | Single | Hyperechoic | Left ventricle | Tiny | Rhabdomyoma |
| 3 | 26 | Multiple | Slightly
hyperechoic | Left and right
ventricles | Tiny | Fibroma |
| 4 | 33 | Multiple | Hyperechoic | Right ventricle and
interventricular septum | Slight | Rhabdomyoma,
confirmed by color ultrasound following birth |
| 5 | 34 | Multiple | Slightly
hyperechoic | Left and right
ventricles and interventricular septum | Slight | Rhabdomyoma |
| 6 | 24 | Multiple | Hyperechoic | Interventricular
septum and apex of heart | Tiny | Rhabdomyoma |
| 7 | 26 | Multiple | Hyperechoic | Apex of heart and
left ventricle | Tiny | Hemangioma |
| 8 | 30 | Multiple | Hyperechoic | Left and right
ventricles and apex of heart | Tiny | Rhabdomyoma |
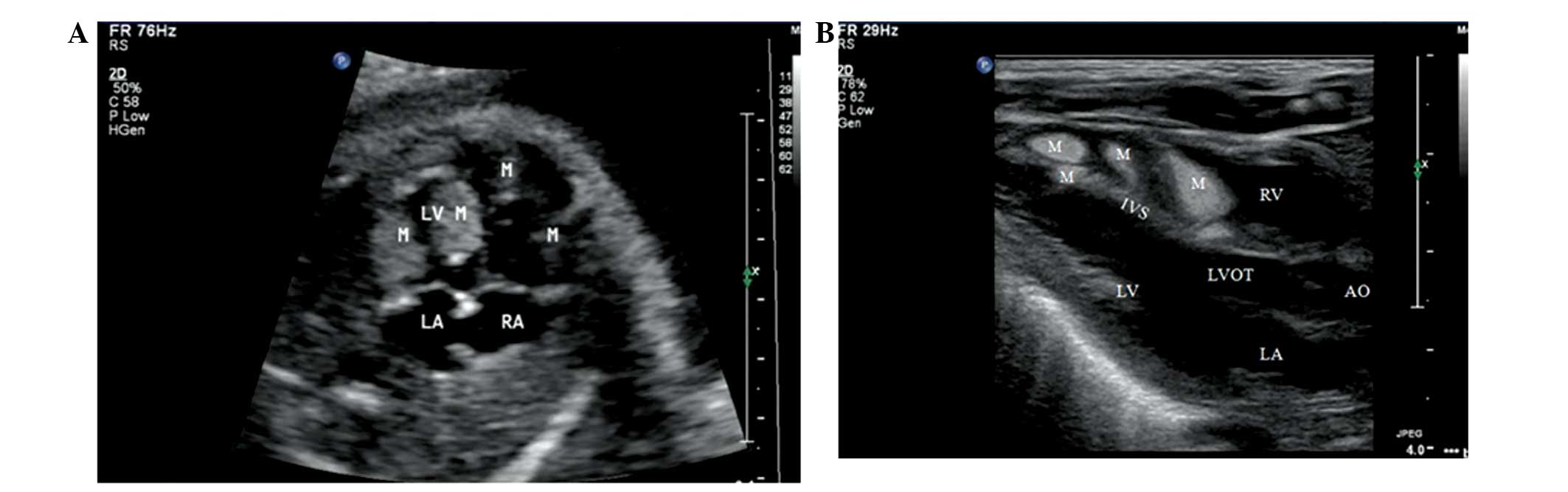
In total, 1 patient (No. 4; Table I) continued with the pregnancy and the
fetus was followed up during pregnancy and subsequent to birth by
cardiac echocardiographic examination (Fig. 1).
One fetus (No. 2; Table
I) was found to possess a 10×6 mm oval high echo, with wide
basement membrane but without pedicle, in the left ventricular
cavity of the fetal heart at the first ultrasonic examination at
the gestational age of 21 weeks (Fig.
2A). This pregnancy was continued and a follow-up was
performed. At 26 weeks gestation, a check-up was performed and it
was found that the hyperechoic mass in the left ventricular cavity
of the fetal heart had increased to ~16×10 mm and an additional
hyperechoic mass 7×6 mm in size was found in the right ventricular
cavity (Fig. 2B). The patient then
chose to terminate the pregnancy. Autopsy examination confirmed
that the masses were rhabdomyoma (Fig. 2C
and D) and there were multiple nodules in each of the fetal
kidneys.
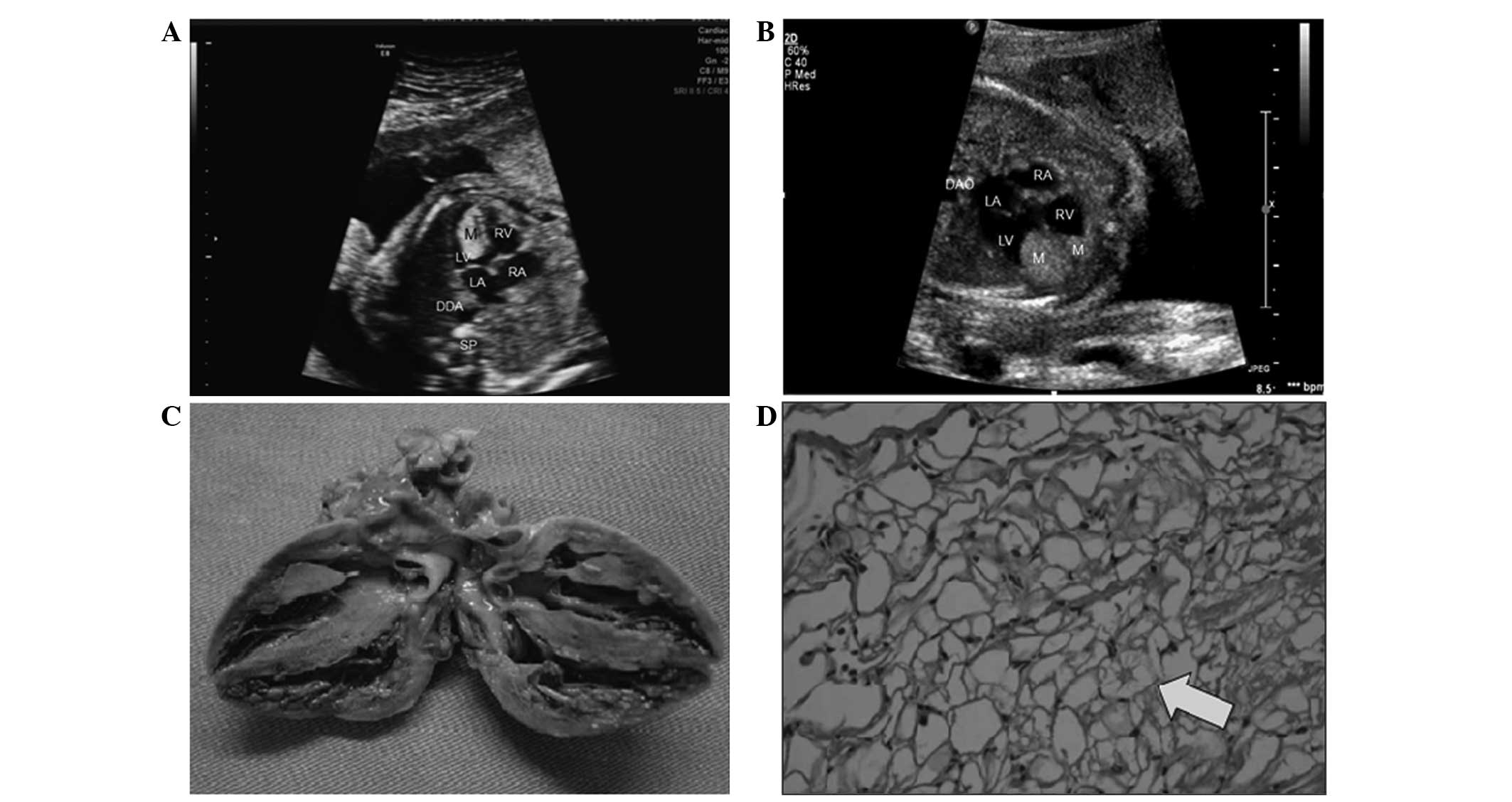 | Figure 2.Fetal electrocardiography performed on
a pregnant woman at 21 weeks gestation revealed a single tumor
located in the LV of the fetal heart. After 5 weeks, the patient
was followed up and it was found that the hyperechoic mass in the
left ventricular cavity of the fetal heart had increased, and
another hyperechoic mass was found in the right ventricular cavity.
The patient then chose to terminate the pregnancy. Autopsy
examination confirmed that the masses were rhabdomyoma. (A) Fetal
electrocardiography performed on a pregnant woman at 21 weeks
gestation revealed a single tumor located in the LV of the fetal
heart. (B) Fetal electrocardiography performed on a pregnant woman
at 26 weeks gestation revealed two masses located in the LV and RV
of the fetal heart. (C) Anatomic image of the fetal heart captured
subsequent to autopsy. (D) Microscopic histological observation of
rhabdomyoma revealing that the cells were vacuolated in unequal
sizes and the nuclei were located in the center of the cells, with
a small amount of surrounding cytoplasm in a spider-like radial
distribution (arrow). Stain, hematoxylin and eosin; magnification,
×400. M, masses; LV, left ventricle; RV, right ventricle; LA, left
atrium; RA, right atrium; DAO, descending aorta; SP, spinal. |
Discussion
Fetal cardiac tumors mostly occur as primary tumors
and the incidence rate accounts for 1/10,000 cases of fetal heart
disease, among which >90% are benign (1). Rhabdomyoma remains the most common
histological type of fetal cardiac tumor at present, accounting for
60% of lesions, followed by teratoma, fibroids and hemangioma
(13–16).
As detected using echocardiography, fibroma
demonstrates equal echo and teratoma demonstrates an uneven echo,
usually in the pericardium, while hemangioma demonstrates low echo
nodules, with internal tubular echo, or exhibits rich blood flow
signals by Doppler ultrasonic examination (11). Rhabdomyoma generally exhibits uniform
high echo, stronger than normal myocardial echo, and are usually
multiple space-occupying lesions (17,18).
Rhabdomyoma may be combined with tuberous sclerosis (19) or damage to other organs, including
brain, kidney and liver damage (6).
In the present study, the fetal cardiac tumor in 1 fetus
demonstrated an increase in size and number when follow-up was
performed, while the nodular shadows in the fetal kidneys did not
exhibit any evident abnormal echo. The subsequent autopsy
examination identified nodules in the kidneys (20). It has been reported that a small
number of rhabdomyoma lesions demonstrate a diminishing trend
during the years subsequent to birth, and certain lesions disappear
naturally (21). Certain studies have
even considered fetal cardiac rhabdomyoma to not be a true tumor,
but as a hamartoma (22).
When a small and single occupying lesion is
identified in the fetal heart, the patient should receive dynamic
observation and close follow up (21). However, systemic examination of the
nervous system and organs of the fetus should be performed using
magnetic resonance imaging (MRI) to identify any damage to other
organs (23). In the present study, 2
patients continued with the pregnancy when occupying lesions in the
fetal heart were identified. Follow-up was performed for 1 patient
from early gestation, subsequent to the identification of a single
and small occupying lesion in the fetus, while the other patient
was in late gestation and no more abnormality was identified during
the follow-up period. Each of the 2 patients underwent MRI but no
other evident pathological change was found. Under these
circumstances, the fetus may survive. However, it is reported that
the recurrence rate is ≤50% (24) and
the prognosis is poor. Thus, pregnancy should be terminated when
recurrence is identified (25), as a
more serious hemodynamic disorder is also likely to occur in the
neonatal period and lead to neonatal mortality or neurological
symptoms, or other severe complications (26). Therefore, all patients in the present
study were constantly followed up prior to the time of writing.
Ultrasonic examination possesses numerous
characteristics, such as non-invasiveness, a lack of radiation,
repeatability and high diagnostic rate, which indicates that this
examination is the best choice for detecting fetal cardiac
space-occupying lesions (10). With
the constant improvement of ultrasonographic technology and the
improved knowledge of diagnostic ultrasonography, early cardiac
tumors may be accurately detected (24). However, this should be differentiated
with strong echo spots in the ventricular cavity and certain normal
heart structures, such as the small papillary muscle (25). Therefore, it should be dynamically and
closely followed up in order to avoid misdiagnosis or missed
diagnosis (21). During the follow up
period, the observations should be compared with the previous
examination, to enable the observation of changes in tumor size and
the resulting abnormal heart function or blood stream obstruction.
Close and dynamic prenatal follow-up may aid in the reduction of
the fatality rate and rapidly allow ultrasonic diagnosis to provide
additional important novel clinical information for obstetricians
and pediatricians. Therefore, prenatal ultrasonic diagnosis of
space-occupying lesions in the fetal heart possesses considerable
clinical value and is conducive to a healthy birth and good care in
developing countries.
References
|
1
|
Silverman N: Primary cardiac tumors. Ann
Surg. 191:127–138. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Smythe JF, Dyck JD, Smallhorn JF and
Freedom RM: Natural history of cardiac rhabdomyoma in infancy and
childhood. Am J Cardiol. 66:1247–1249. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Stellingwerff GC, Hess J and Bogers AJ:
Left ventricular rhabdomyoma. A case report. J Cardiovas Surg
(Torino). 40:131–133. 1999.
|
|
4
|
DeVore GR, Hakim S, Kleinman CS and
Hobbins JC: The in utero diagnosis of an interventricular septal
cardiac rhabdomyoma by means of real-time-directed, M-mode
echocardiography. Am J Obstet Gynecol. 143:967–969. 1982.PubMed/NCBI
|
|
5
|
DeVore GR: Assessing fetal cardiac
ventricular function. Semin Fetal Neonatal Med. 10:515–541. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Van der Hauwaert LG: Cardiac tumors in
infancy and childhood. Br Heart J. 33:125–132. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Björkhem G, Lundström NR and Lingman G:
Intracardiac rhabdomyomas in neonates: Report of three cases. Acta
Paediatr. 81:712–715. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hamner LH III, Kaye MF and Weingold AB:
Difficulty of fetal monitoring in a fetus with intracardiac tumors.
Obstet Gynecol. 73:477–481. 1989.PubMed/NCBI
|
|
9
|
Matsui M and Gardiner H: Current aspects
of fetal cardiovascular function. Fetal Matern Med Rev. 19:61–84.
2008. View Article : Google Scholar
|
|
10
|
Van Mieghem T, DeKoninck P, Steenhaut P
and Deprest P: Methods for prenatal assessment of fetal cardiac
function. Prenat Diagn. 29:1193–1203. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hornberger LK: Role of quantitative
assessment in fetal echocardiography. Ultrasound Obstet Gynecol.
35:4–6. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
World Medical Association: WMA Declaration
of Helsinki - Ethical principles for medical research involving
human subjects. http://www.chcuk.co.uk/pdf/Declaration_of_Helsinki_2008_Version.pdfAccessed.
October 20–2014
|
|
13
|
Schmaltz AA and Apitz J: Primary heart
tumors in infancy and childhood: Report of four cases and review of
literature. Cardiology. 67:12–22. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jentarra GM, Rice SG, Olfers S, Saffen D
and Narayanan V: Evidence for population variation in TSC1 and TSC2
gene expression. BMC Med Genet. 12:292011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
McAllister HA Jr: Primary tumors of the
heart and pericardium. Pathol Annu. 14:325–355. 1979.PubMed/NCBI
|
|
16
|
Foster ED, Spooner EW, Farina MA, Shaher
RM and Alley RD: Cardiac rhabdomyoma in the neonate: Surgical
management. Ann Thorac Surg. 37:249–253. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Roach ES, Smith M, Huttenlocher P, Bhat M,
Alcorn D and Hawley L: Diagnostic criteria: Tuberous sclerosis
complex. Report of the Diagnostic Criteria Committee of the
National Tuberous Sclerosis Association. J Clin Neurol. 7:221–224.
1992.
|
|
18
|
Mühler EG, Kienast W, Turniski-Harder V
and von Bernuth G: Arrhythmias in infants and children with primary
cardiac tumours. Eur Heart J. 15:915–921. 1994.PubMed/NCBI
|
|
19
|
Jóźwiak S, Kotulska K, Kasprzyk-Obara J,
Domańska-Pakieła D, Tomyn-Drabik M, Roberts P and Kwiatkowski D:
Clinical and genotype studies of cardiac tumors in 154 patients
with tuberous sclerosis complex. Pediatrics. 118:e1146–e1151. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen CP, Su YN, Hung CC, Shih JC and Wang
W: Novel mutation in the TSC2 gene associated with prenatally
diagnosed cardiac rhabdomyomas and cerebral tuberous sclerosis. J
Formos Med Assoc. 105:599–603. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dal Prato L, Borini A, Coticchio G,
Cattoli M and Flamigni P: Half-dose depot triptorelin in pituitary
suppression for multiple ovarian stimulation in assisted
reproduction technology: A randomized study. Hum Reprod.
19:2200–2205. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yim SF, Lok IH, Cheung LP, Briton-Jones
CM, Chiu TT and Haines CJ: Dose-finding study for the use of
long-acting gongadotrophin-releasing hormone analogues prior to
ovarian stimulation for IVF. Hum Reprod. 16:492–494. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sonigo P, Elmaleh A, Fermont L, Delezoíde
AL, Mirlesse V and Brunelle F: Prenatal MRI diagnosis of fetal
cerebral tuberous sclerosis. Pediatr Radiol. 26:1–4. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gresser CD, Shime J, Rakowski H, Smallhorn
JF, Hui A and Berg JJ: Fetal cardiac tumor: A prenatal
cardiographic marker for tuberous sclerosis. Am J Obstet Gynecol.
156:689–690. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Holley DG, Martin GR, Brenner JI, Fyfe DA,
Huhta JC, Kleinman CS, Ritter SB and Silverman NH: Diagnosis and
management of fetal tumors. A multicenter experience and review of
published reports. J Am Coll Cardiol. 26:516–520. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bertolini P, Meisner H, Paek SU and
Sebening F: Special considerations on primary cardiac tumors in
infancy and childhood. Thorac Cardiovasc Surg. 38(Suppl 2):
164–167. 1990. View Article : Google Scholar : PubMed/NCBI
|