Introduction
Extranodal natural killer (NK)/T-cell lymphoma is
markedly associated with Epstein-Barr virus (EBV) and is clinically
aggressive, with a poor prognosis. This type of lymphoma is
predominantly located in the nasal cavity and paranasal sinus, but
rarely occurs in the stomach (1). The
specific immunophenotype demonstrates the expression of CD56, CD2,
CD3ε and cytotoxic granule-associated protein, diffuse expression
of EBV-encoded RNA (EBER), and no expression of surface
CD3− (2). In the majority
of patients with NK/T-cell lymphoma, CD56 is expressed and CD30 is
not expressed or partially expressed, but the absence of CD56
expression and presence of CD30 expression is rare (2). The expression of CD30 is also a
characteristic of cutaneous T-cell lymphoma or anaplastic large
T-cell lymphoma (ALCL) (3).
Therefore, the overlap of immunohistochemical phenotypes between
different tumors may occasionally result in a misdiagnosis. To the
best of our knowledge, no study has reported gastric NK/T-cell
lymphoma without CD56 expression and with diffuse CD30 expression.
It is extremely important to differentiate NK/T-cell lymphoma from
other gastric neoplasms, including poorly-differentiated
adenocarcinoma, ALCL, NK-cell lymphoproliferative lymphomatoid
gastropathy and enteropathy-associated T-cell lymphoma (EATL) type
I.
Case report
A 41-year-old woman presented to the First
Affiliated Hospital of Dalian Medical University (Dalian, Liaoning,
China) in January 2013, with a history of various clinical symptoms
for 2 months, including epigastric pain and abdominal distention,
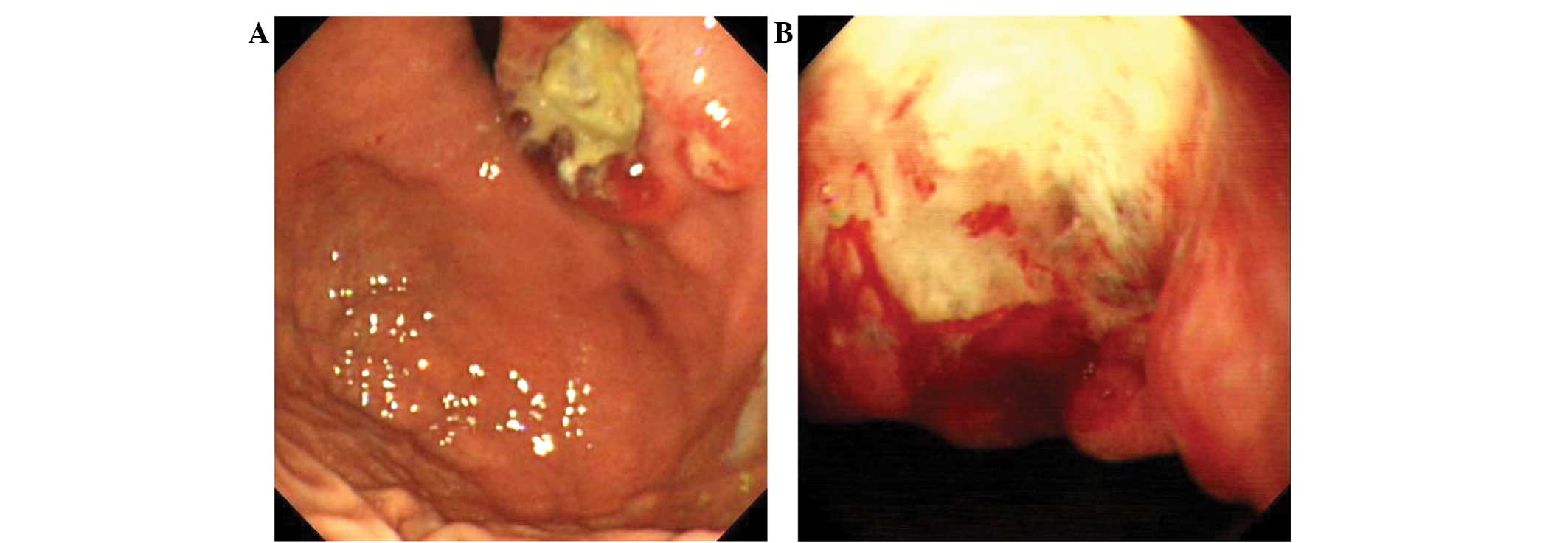
which had been ongoing for two months. An endoscopic examination
revealed an ulcer located in the cardia of the stomach, which was
4.0×3.5 cm in size (Fig. 1A and B).
Following an endoscopic biopsy, an initial diagnosis of a
poorly-differentiated adenocarcinoma was made. Subsequently, a
total gastrectomy with regional lymph node dissection was
performed. The resected ulcer was irregular in shape with raised
edges and was covered with pale yellow exudates. The cut face of
the ulcer was gray and solid, and the tumor infiltrated the whole
wall of the stomach.
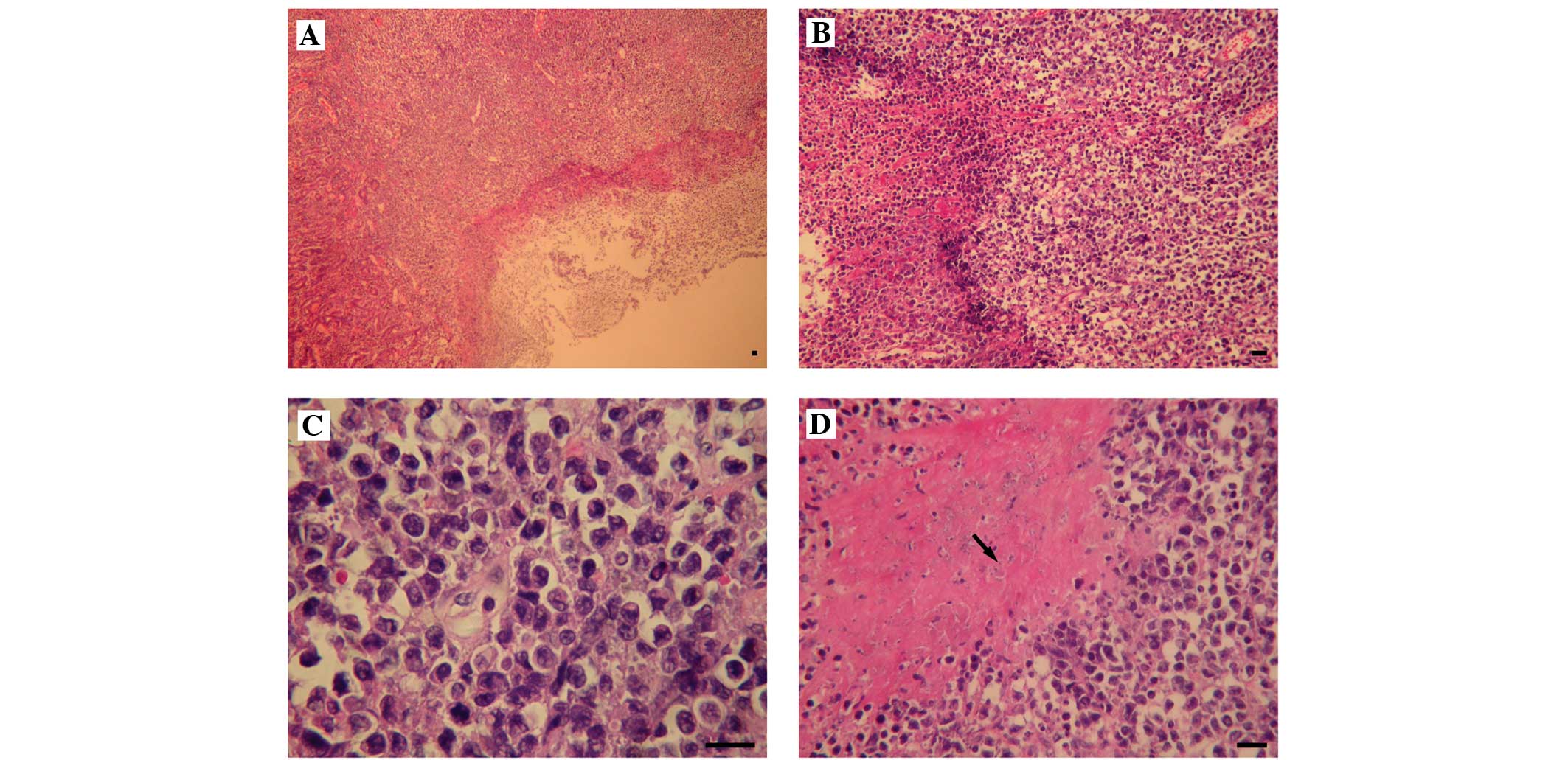
A microscopic examination of the gastric ulcerative
lesion revealed that the majority of the surface was overlaid with
necrosis and the whole layer was infiltrated with discohesive and
monomorphous atypical cells (Fig. 2A and
B). The tumor cells were large with an irregular kidney shape
and possessed dense or vesicular nuclei with abundant eosinophilic
cytoplasm (Fig. 2C). Neutrophils and
eosinophils were observed at the periphery of the tumor. Minor
coagulative necrosis was evident (Fig.
2D). Angiocentric and angiodestructive growth patterns and
large nucleoli were not observed.
Immunohistochemical staining demonstrated that the
monomorphous tumor cells demonstrated diffuse expression of CD3ε,
CD30, granzyme-B and CD43 (Fig.
3A–D). The tumor cells did not express CD56 (Fig. 3E), cytokeratin (Fig. 3F), CD2, CD4, CD5, CD7, CD8, anaplastic
lymphoma kinase, CD20 or paired box-5 transcription factor (PAX5)
(data not shown). All the antibody in the immunohistochemical
staining are bought from Fuzhou Maixin Biotech Co., Ltd., Fuzhou,
China). The Ki-67 (ZhongShanJinQiao Co., Ltd., Beijing, China)
labeling index was 80% (Fig. 3G).
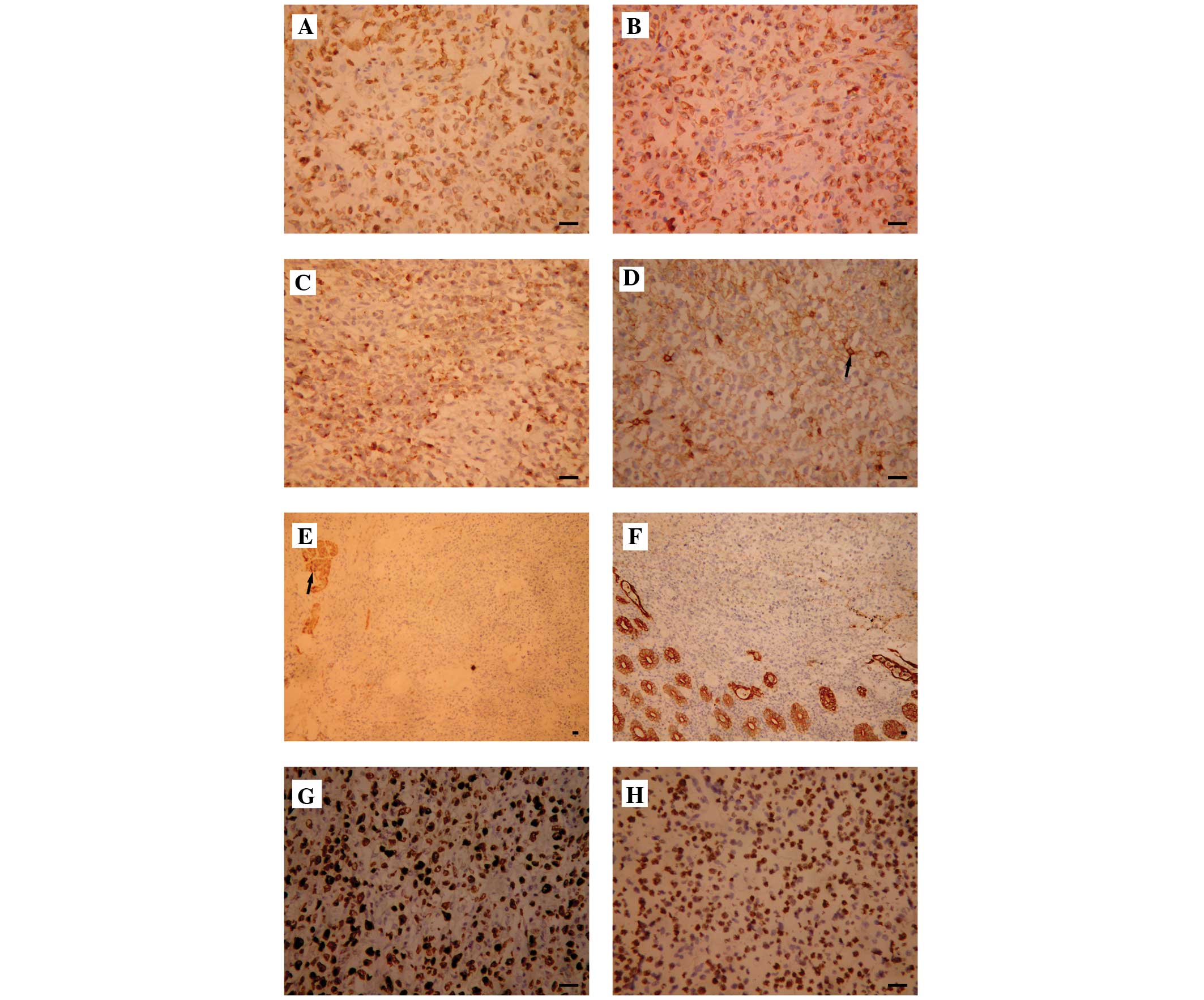 | Figure 3.Immunohistochemical staining and in
situ hybridization. The expression profiles of different
phenotypic markers in tumor cells were observed using
immunostaining, as follows: (A) CD3ε, diffusely expressed; (B)
CD30, diffusely expressed in the membrane and golgi; (C)
granzyme-B, expressed; (D) CD43, expressed, the black arrow
indicates marked expression of normal reactive T cells; (E) CD56,
not expressed, the black arrow indicates residual nerve fibers that
express CD56, which acts as an internal control to validate the
CD56 negative staining of tumor cells; (F) cytokeratin AE1/AE3,
expressed in the glandular epithelium; (G) Ki-67 index, ~80%; and
(H) EBV RNA, diffusely expressed, as detected by EBV-encoded RNA
in situ hybridization. Scale bar=20 µm. ×200, magnification.
CD, cluster of differentiation; EBV, Epstein-Barr virus. |
Based on the morphology and immunophenotype, the
diagnosis of the tumor was altered to ALCL. Following a
consultation with other pathologists, the detection of EBV was
advised to elimate the possibility that the tumor was a NK/T-cell
lymphoma. Consequently, the tumor cells were analyzed for EBER
status by in situ hybridization. As a result, the EBV RNA
signal was identified as diffuse positive (Fig. 3H). Therefore, the final diagnosis was
corrected to primary gastric NK/T-cell lymphoma. Additional
laboratory examinations, including a hematological examination, of
the patient were normal. Levels of tumor markers were within normal
limits, as follows: Carcinoembryonic antigen (CEA), 0.432 ng/ml
(normal, <5.000 ng/ml); carbohydrate antigen (CA) 19-9, 12.26
U/ml (normal, <27.00 U/ml) and CA125, 21.0 U/ml (normal,
<35.0 U/ml). The patient did not possessed nasal cavity lesions,
and no superficial lymphadenopathy or hepatosplenomegaly was
observed. Following chemotherapy, the patient was alive without
tumor recurrence subsequent to a 14-month follow-up period.
The present study was approved by the Ethics
Committee of The First Affiliated Hospital of Dalian Medical
University. Written informed consent was obtained from the patient
for the publication of the present study and the use of the
accompanying images.
Discussion
NK/T-cell lymphoma may overlap in morphology,
results of endoscopic imaging and immunophenotype with numerous
other tumors of the stomach. Therefore, careful consideration is
required to distinguish NK/T-cell lymphoma from other tumors of the
stomach, and this may be based on pathological and phenotypic
features.
Poorly-differentiated adenocarcinoma, which is the
most common tumor of the stomach, is the primary choice for a
differential diagnosis of a stomach tumor (4). The results of endoscopic imaging and the
morphological features of a poorly-differentiated adenocarcinoma
occasionally resemble NK/T-cell lymphoma (5). In the present study, the tumor was
removed using an endoscopic biopsy and was diagnosed as
poorly-differentiated adenocarcinoma, based on the tumor
morphology. However, the adenocarcinoma did not express leukocyte
common antigen (LCA), a T cell and B cell marker, and did express
cytokeratin. Therefore, the present study recommends that when a
tumor diagnosis of poorly differentiated adenocarcinoma is
considered, immunostaining for cytokeratin and LCA should be
performed to exclude a diagnosis of lymphoma.
ALCL is the secondary choice for a differential
diagnosis in tumors of the stomach that express CD30 (6). In the present study, the tumor cells
possessed irregular kidney-shaped nuclei, which expressed CD3ε and
diffusely expressed CD30, but did not express CD56, therefore
leading to an initial diagnosis of ALCL. However, there have been
studies reporting NK/T-cell lymphoma in the nasal cavity, prostate,
spleen and adrenal glands, where the tumor expresses CD30, with or
without CD56 expression (7–10). To the best of our knowledge, no
studies have reported this type of lymphoma in the stomach. The
previous studies concluded that the absence of a CD56 signal is not
sufficient to exclude NK/T-cell lymphoma, and therefore, EBV
detection is required (5,6,11,12). The present study observed that the
tumor cells did not have clear nucleoli and demonstrated clear
coagulative necrosis, which does not support a diagnosis of ALCL.
However, the diagnosis of the patient was only altered when the EBV
status of the patient was assessed. The patient expressed EBV RNA,
leading to a final diagnosis of NK/T-cell lymphoma.
NK-cell lymphoproliferative lymphomatoid gastropathy
should also be considered since this type of tumor expresses CD3
and CD56, therefore resembling NK/T-cell lymphoma. However, NK-cell
lymphoproliferative lymphomatoid gastropathy has a low
proliferative index (Ki-67) and an indolent clinical course with an
improved prognosis. Notably, this disease is not associated with an
EBV infection (13,14).
EATL type I is often observed in conjunction with
refractory celiac disease and mainly occurs in the jejunum and
ileum, but rarely occurs in the stomach. This lymphoma should also
be distinguished from gastric NK/T-cell lymphoma. EATL type I
possesses large or pleomorphic cells that are express CD3,
partially express CD30, but usually do not express CD8 and CD56.
EATL also lacks EBV RNA expression in an EBER in situ
hybridization (15).
Mucosa-associated lymphoid tissue lymphoma and
diffuse large B-cell lymphoma are other common types of lymphomas
that occur in the stomach, where atypical lymphoid cells diffusely
infiltrate the gastric mucosa. Furthermore, the B cell phenotype is
characterized by the expression of CD20 and PAX5 (16,17).
Consequently, these lymphomas may be easily distinguished from
NK/T-cell lymphoma.
NK/T-cell lymphomas that express CD30, with or
without CD56 expression, have been reported in previous studies in
the nasal cavity, spleen, prostate and adrenal glands (7–10,18–20).
However, to the best of our knowledge, no studies have reported
this NK/T-cell lymphoma phenotype occurring in the stomach. The
present study reports a unique case of primary gastric NK/T-cell
lymphoma without CD56 expression and with diffuse CD30 expression
in a 41-year-old woman. Due to the occurrence of this rare
phenotype of NK/T-cell lymphoma, the present study recommends that
the EBV status of a patient should be investigated to avoid a
misdiagnosis.
References
|
1
|
Kobold S, Merz H, Tiemann M, Mahuad C,
Bokemeyer C, Koop I and Fiedler W: Primary NK/T cell lymphoma nasal
type of the stomach with skin involvement, A case report. Rare
Tumors. 1:e582009.PubMed/NCBI
|
|
2
|
Chan JKC, Quintanilla-Martinez L, Ferry JA
and Peh SC: Extranodal NK/T-cell lymphoma, nasal type. World Health
Organization Classification of Tumours of Haematopoietic and
Lymphoid Tissues. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri
SA, Stein H, Thiele J and Vardiman JW: 2:(4th). (Lyon). IARC Press.
285–288. 2008.
|
|
3
|
de Leval L and Gaulard P: Pathology and
biology of peripheral T-cell lymphomas. Histopathology. 58:49–68.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Romero Espejo H and Navarrete Siancas J:
Classification of stomach adenocarcinomas. Rev Gastroenterol Peru.
23(3): 199–212. 2003.PubMed/NCBI
|
|
5
|
Kim H, Lee D, Kim JW, Huh J, Park SH, Ha
HK, Suh C, Yoon SM, Kim KJ, Choi KD, et al: Endoscopic and clinical
analysis of primary T-cell lymphoma of the gastrointestinal tract
according to pathological subtype. J Gastroenterol Hepatol.
29:934–943. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang FH, Li YH, Zeng J, Rao HL, Xia ZJ,
Sun XF, Huang HQ, Lin TY, Jiang WQ and Guan ZZ: Clinical analysis
of primary systemic anaplastic large cell lymphoma, A report of 57
cases. Ai Zheng. 28:49–53. 2009.PubMed/NCBI
|
|
7
|
Tsukahara T, Takasawa A, Murata M, Okumura
K, Nakayama M, Sato N and Hasegawa T: NK/T-cell lymphoma of
bilateral adrenal glands in a patient with pyothorax. Diagn Pathol.
7:1142012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cao Q, Huang Y, Ye Z, Liu N, Li S and Peng
T: Primary spleen extranodal NK/T cell lymphoma, nasal type, with
bone marrow involvement and CD30 positive expression, A case report
and literature review. Diagn Pathol. 9:1692014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ferenczi K, Summers P, Aubert P, Cooper B,
Meyerson H, Cooper KD and Honda K: A case of CD30+ nasal natural
killer/T-cell lymphoma. Am J Dermatopathol. 30:567–571. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jiang Q, Liu S, Peng J, Xiong H, Xiong Z,
Yang Y, Tan X and Gao X: An extraordinary T/NK lymphoma, nasal
type, occurring primarily in the prostate gland with unusual CD30
positivity, Case report and review of the literature. Diagn Pathol.
8:942013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bautista-Quach MA, Ake CD, Chen M and Wang
J: Gastrointestinal lymphomas, Morphology, immunophenotype and
molecular features. J Gastrointest Oncol. 3:209–225.
2012.PubMed/NCBI
|
|
12
|
Kawamoto K, Nakamura S, Iwashita A,
Watanabe J, Oshiro Y, Nakayama Y, Nimura S, Kimura N, Aoyagi K, Yao
T, et al: Clinicopathological characteristics of primary gastric
T-cell lymphoma. Histopathology. 55:641–653. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mansoor A, Pittaluga S, Beck PL, Wilson
WH, Ferry JA and Jaffe ES: NK-cell enteropathy: a benign NK-cell
lymphoproliferative disease mimicking intestinal lymphoma,
clinicopathologic features and follow-up in a unique case series.
Blood. 117:1447–1452. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tanaka T, Megahed N, Takata K, Asano N,
Niwa Y, Hirooka Y and Goto H: A case of lymphomatoid gastropathy,
An indolent CD56-positive atypical gastric lymphoid proliferation,
mimicking aggressive NK/T cell lymphomas. Pathol Res Pract.
207:786–789. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang L, Liu Y, Lin XY, Yu JH, Miao Y, Qiu
XS and Wang EH: A case of enteropathy-associated T-cell lymphoma
(type I) arising in stomach without refractory celiac disease.
Diagn Pathol. 7:1722012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ferreri AJ and Montalbán C: Primary
diffuse large B-cell lymphoma of the stomach. Crit Rev Oncol
Hematol. 63:65–71. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Psyrri A, Papageorgiou S and Economopoulos
T: Primary extranodal lymphomas of stomach, Clinical presentation,
diagnostic pitfalls and management. Ann Oncol. 19:1992–1999. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chang BH, Stork L and Fan G: A unique case
of adolescent CD56-negative extranodal NK/T-cell lymphoma, nasal
type. Pediatr Dev Pathol. 11:50–54. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pongpruttipan T, Kummalue T, Bedavanija A,
Khuhapinant A, Ohshima K, Arakawa F, Niino D and Sukpanichnant S:
Aberrant antigenic expression in extranodal NK/T-cell lymphoma, A
multi-parameter study from Thailand. Diagn Pathol. 6:792011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schwartz EJ, Molina-Kirsch H, Zhao S,
Marinelli RJ, Warnke RA and Natkunam Y: Immunohistochemical
characterization of nasal-type extranodal NK/T-cell lymphoma using
a tissue microarray, An analysis of 84 cases. Am J Clin Pathol.
130:343–351. 2008. View Article : Google Scholar : PubMed/NCBI
|