Introduction
Human parvovirus B19 (B19) is a small DNA virus with
a single-stranded linear genome which encodes one non-structural
protein, NS-1, and two viral capsid proteins, VP1 (83 kDa) and VP2
(58 kDa) (1). B19 is the
aetiological agent of a number of diseases (2) and infection with B19 is a global
concern. In immunologically healthy hosts, B19 may cause a number
of acute, generally self-limiting diseases, notably, fifth disease
or erythema infectiosum in children, acute polyarthritis in adults,
and aplastic crisis in patients with chronic hemolytic anemia,
including sickle cell anemia or hereditary spherocytosis (3–6). In
pregnant women, B19 infection may result in the lysis of nucleated
fetal red blood cells, hydrops fetalis, and subsequent spontaneous
abortion and fetal mortality (7).
B19 has also been found to be associated with glomerulonephritis,
vasculitis, peripheral neuropathies, myocarditis and fulminant
hepatic failure (8). In
immunocompromised hosts, B19 infection may persist and lead to
chronic anemia, red cell aplasia, and less frequently,
thrombo-cytopenia, neutropenia and pancytopenia (9–11).
However, only a small amount of literature regarding the
involvement of B19 in malignant tumors is available. In this study,
we examined whether cancer patients have a higher risk of B19
infection, in order to further understand the effect of B19
infection on the pathogenesis of cancer patients.
Human bocavirus (HBoV) is a recently identified
parvovirus associated with respiratory and gastrointestinal
diseases in humans. It was first identified in children with lower
respiratory tract infections (LRTIs) in October 2005 (12). Since then, the detection of HBoV in
acute respiratory illness has been reported worldwide, with
prevalence rates between 1.5 and 19% (13–15).
It was subsequently detected in serum (16–17),
fecal (18–19) and urine samples (20). HBoV detection was significantly
higher in patients with symptoms of respiratory tract infections or
gastroenteritis than in asymptomatic individuals (14,16,21–23).
Findings of a recent study suggest that acute infection of HBoV
causes systemic infection, induces immune responses and is often
associated with coinfection (24).
At present, the biological features of HBoV and the significance of
human disease by this virus remain unknown. Since a second
parvovirus causes human disease following B19, the infection
incidence of this virus in cancer patients also evokes our
interest.
Materials and methods
Patients and specimens
Serum samples of 288 cancer patients, 156 of which
were from known clinicopathological cancer patients, were collected
from the Second Hospital of Wuhan Iron and Steel Company (WISCO).
To evaluate whether hepatitis B virus (HBV) infection is associated
with B19 infection, 113 blood samples from patients with hepatitis
were also obtained from the same hospital. A total of 800 serum
samples from normal blood donors, without known ages and genders,
were randomly selected at the Sixth Hospital of Wuhan and 941
aspirate samples from children with respiratory tract infections
were collected at the Hubei Maternal and Child Health Hospital in
Wuhan. Both served as controls. All the nucleic acid extracted from
the serum and sputum samples were stored at −80°C upon arrival in
the laboratory until it was tested for parvovirus DNA. The study
was approved by the academic committee of the Central China Normal
University and the analysis of patients’ blood samples was agreed
by the Second Hospital of Wuhan Iron and Steel Company (WISCO).
Primer design
The primers used to amplify the DNA of the B19,
HBoV, HBV and transfusion transmitted virus (TTV) were designed
(Table I) based on the most
conserved sequences encoding the non-structural protein (NS) of
parvovirus B19 (GenBank accession number, AY386330), the
non-structural protein (NP1) of parvovirus HBoV (GU139423), the S
gene region of HBV and the ORF1 region of TTV (AB008394), and were
synthesized by Genscript Genetech Co. Ltd, China. The virus DNA was
detected using nested-PCR with 2 pairs of primers, except for HBoV,
which was detected by only one pair of primers.
 | Table IPrimers used in viral genome
amplification. |
Table I
Primers used in viral genome
amplification.
| Virus | Amplification
region | Forward primer | Reverse primer | Size (bp) |
|---|
| B19 | NS | Outer
5′-TCACCATATTCTTGGGAACAAGA-3′ |
5′-CTGCTTTCACTGAGTTCTTC-3′ | 663 |
| | Inner
5′-AATACACTGTGGTTTTATGGGCCG-3′ |
5′-CCATTGCTGGTTATAACCACAGGT-3′ | 284 |
| HBoV | NP1 |
5′-TATCGTCTTGCACTGCTTCG-3′ |
5′-AGAGTAGGCGTGATCATGTAA-3′ | 602 |
| HBV | S | Outer
5′-TCACCATATTCTTGGGAACAAGA-3′ |
5′-CGAACCACTGAACAAATGGC-3′ | 1103 |
| | Inner
5′-CCCATATCGTCAATCTTCTCGAGGA-3′ |
5′-GTAGTTGATGTTCCTGGAAGTAGAGG-3′ | 392 |
| TTV | ORF1 | Outer
5′-GCAGCAGCATATGGATATGT-3′ |
5′-TGACTGTGCTAAAGCCTCTA-3′ | 270 |
| | Inner
5′-CATACACATGAATGCCAGGC-3′ |
5′-TGACTGTGCTAAAGCCTCTA-3′ | 217 |
DNA extraction, nested-PCR and
sequencing
Total nucleic acid was extracted from each specimen
by the Roche High Pure Viral Nucleic Acid kit (Roche Diagnostics,
Mannheim, Germany), according to the manufacturer’s instructions.
The DNA extracts were stored at −80°C prior to PCR analysis.
The extracted DNA (2.5 μl) was added to the PCR
mixture containing 2.5 μl of 10X reaction buffer (Tiangen Biotech,
Beijing Co. Ltd, China), 200 μM of each dATP, dCTP, dGTP and dTTP,
12.5 pmol of each primer and 1.25 units of Taq polymerase (Tiangen
Biotech). The nested-PCR of B19 was performed under the following
conditions: denaturation at 94°C for 4 min, 30 cycles of 94°C for
30 sec, annealing at 56°C for 30 sec and 72°C for 1 min and
elongation at 72°C for 10 min. Following the first amplification,
the second PCR was performed under the same conditions as described
above, except that the annealing temperature was reset at 58°C, and
0.5 μl of the first PCR product was added to the nested-PCR mixture
using the specific primers. The amplification of HBoV included a
step at 94°C for 3 min, followed by 35 cycles of 30 sec at 94°C, 30
sec at 55°C and 1 min at 72°C. The reactions were carried out using
a thermocycler 5332 (Eppendorf, Germany).
Samples (5 μl) of second-round PCR products were
analyzed by electrophoresis on a 2% agarose gel and then visualized
by UV light following ethidium bromide staining. The plasmids
pB19–4244 (kindly provided by Professor Tijjsen, Canada) and pWHL-1
(genomic clones of HBoV constructed previously in our lab) were
used as the positive controls for B19 and HBoV, respectively. A
number of precautions were taken to avoid contamination of the
samples with PCR products. The reaction reagents were prepared with
pipettes and containers which had never come into contact with
amplified products or with positive samples. Reactions containing
all the PCR reagents and sterile distilled water, instead of the
DNA samples from the specimens, were used as negative controls.
The amplified DNA fragments of the expected sizes
were gel purified, cloned into the vector
pCR®2.1-TOPO® (Invitrogen Life Technologies,
Carlsbad, CA, USA) and transformed into chemically competent E.
coli DH5α. A single colony was cultured and the corresponding
plasmid DNA was sequenced using standard techniques.
Statistical analysis
A pairwise comparison between cancerous serum and
control samples, and the correlation between parvovirus infection
and clinicopathological variables, including gender and cancer
type, was evaluated by the χ2 test, Fisher’s exact test or the
t-test. P<0.05 was considered to indicate a statistically
significant difference. Statistical analyses were performed using
SAS9.2 software (SAS institute Inc, Cary, NC, USA).
Results
High prevalence of B19 and HBoV infection
in tumor patients
To determine the prevalence of B19 infection in
cancer patients, a total of 288 cancer patients were enrolled in
this study between August and November 2010 and B19 DNA was
examined using nested-PCR (Fig.
1A), as described in the Materials and methods. The results
indicated that the overall prevalence of B19 DNA in adult cancer
patients was 50.69% (146/288), which was significantly higher than
that of the healthy controls with 4.5% (36/800) (χ2 test,
P<0.0001). Among these 288 cancer patients, 156 patients with
pertinent clinicopathological features were subjected to further
examination of the seropositive rate of HBoV, HBV and TTV in their
serum (Fig. 1B-D). Our data
revealed that the prevalence percentage of HBoV infection in cancer
patients was 39.74% (62/156), ranked second as compared to the
total analysis, whereas the infection prevalence of HBoV from 941
children with respiratory tract infections was 3.51% (33/941),
which was significantly less (Table
III) than that in the cancer patients.
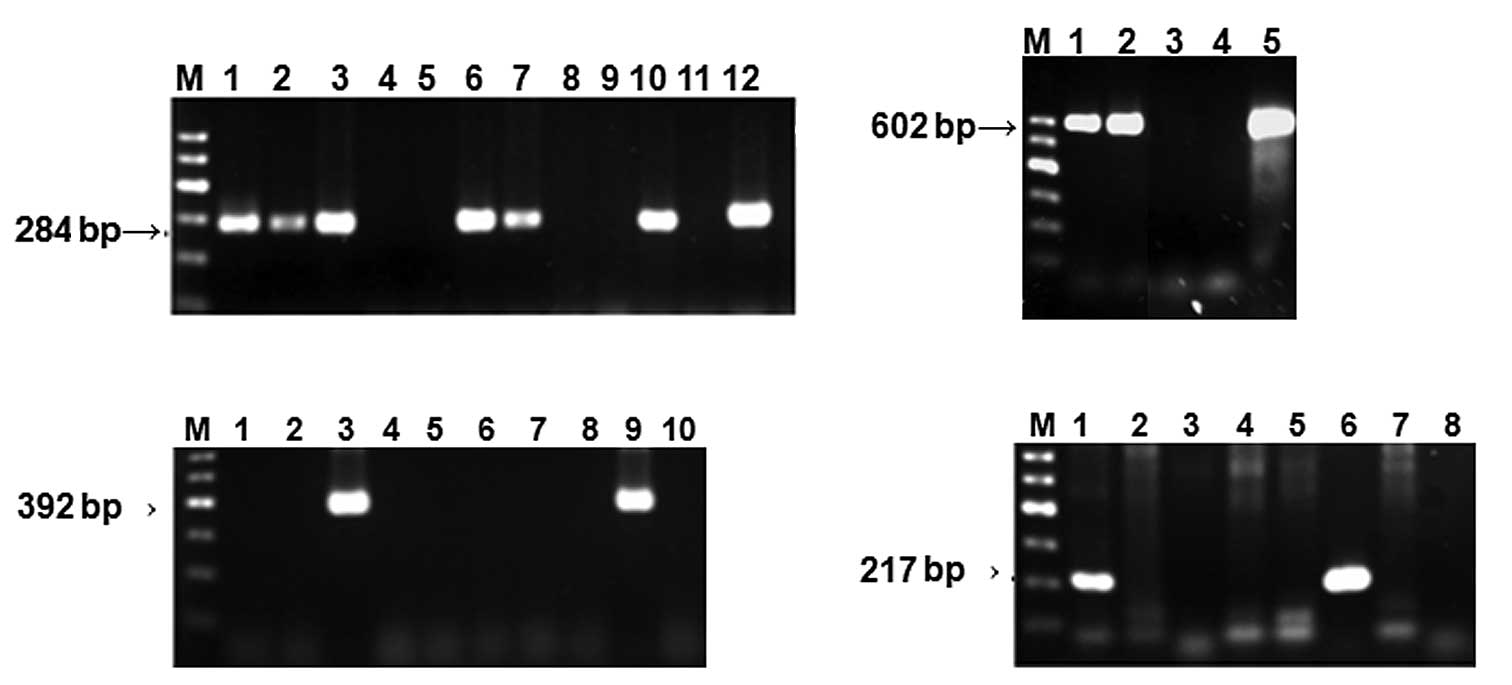 | Figure 1Analysis of PCR products by agarose
gel electrophoresis. M, Marker. (A) B19 DNA was amplified using
nested-PCR as described in Materials and methods. Lanes 1, 2, 3, 6,
7 and 10, six seropositive samples; lanes 4, 5, 8 and 9, four
seronegative samples; lane 11, negative control; lane 12, positive
control.(B) HBoV DNA amplified using PCR. Lanes 1 and 2,
seropositive samples; lane 3, seronegative sample; lane 4, negative
control; lane 5, positive control. (C) HBV DNA amplified using
nested-PCR. Lanes 3 and 9, seropositive samples; lane 10, negative
control. (D) TTV DNA was amplified using nested-PCR. Lanes 1 and 6,
seropositive samples; lane 8, negative control. B19, parvovirus 19;
HBoV, human bocavirus; HBV, hepatits B virus; TTV, transfusion
transmitted virus. |
| Table IIISeroprevalence of HBoV DNA detected by
nPCR in cancer patients and control groups. |
Table III
Seroprevalence of HBoV DNA detected by
nPCR in cancer patients and control groups.
| Cancer serum | Throat swab | Hepatitis serum | P-valuea |
|---|
|
|
|
|
|
|---|
| Group | A
HBoV | B
HBV | C
TTV | D
HBoV | E
HBoV | A vs. B | A vs. C | A vs. D | A vs. E |
|---|
| Positive rate %
(n)b | 36.7 (62/156) | 5.13 (8/156) | 6.41 (10/156) | 3.51 (33/941) | 7.08 (8/113) | 0.0001 | 0.0001 | 0.0001 | 0.0001 |
Subsequently, 113 serum samples from hepatitis
patients without cancer were examined for B19 and HBoV DNA using
PCR assay as the control. The prevalence percentages of B19 and
HBoV infection in hepatitis B patients were 15.9 (18/113) and 7.08%
(8/113), respectively; both are significantly less than that of the
cancer patients with 42.3 (66/156) and 39.7% (62/156) (Tables II and III). These results suggest that a high
prevalence of parvovirus infection commonly occurred in cancer
patients, and a possible novel link may exist between parvovirus
infection and malignant tumors.
| Table IISeroprevalence of B19 DNA detected by
nPCR in cancer patients and control groups. |
Table II
Seroprevalence of B19 DNA detected by
nPCR in cancer patients and control groups.
| Cancer serum | Normal serum | Hepatitis serum | P-valuea |
|---|
|
|
|
|
|
|---|
| Group | A
B19 | B
HBV | C
TTV | D
B19 | E
B19 | A vs. B | A vs. C | A vs. D | A vs. E |
|---|
| Positive rate %
(n)b | 42.3 (66/156) | 5.13 (8/156) | 6.41 (10/156) | 4.5 (36/800) | 15.9 (18/113) | 0.0001 | 0.0001 | 0.0001 | 0.0001 |
We then evaluated whether or not the cancer patients
are also the targets of other viruses, by using HBV and TTV as
controls. Our results revealed that the infection prevalence for
HBV and TTV were 5.13 (8/156) and 6.41% (10/156), respectively
(Tables II and III), demonstrating that the decreased
immunity of the patients with malignant tumors is not the only
reason for high parvovirus infection incidence.
Clinical parameters of the cancer
patients
Analysis of the detection results for B19, HBoV, HBV
and TTV from the 156 cancer patients, ranging from 26 to 85 years
old (mean, 63.38±10.56; 110 male and 46 female), indicated that the
infection rate in all age groups of patients was higher for B19 and
HBoV (Table II and III). The infection prevalence of B19
increased slightly in the older age groups, but no such trend was
observed for HBoV infection.
Comparison of parvovirus infection in
different cancer categories
A further comparison of the seropositive rate of
parvovirus B19 DNA in different cancer categories revealed a
markedly higher seroprevalence in the lung and stomach cancer
groups (Table IV). No significant
difference in B19 seroprevalence was observed among breast, liver
and prostate cancer patients. The consequence of high levels of
infection in lung and stomach cancer patients is unknown and more
samples may be required to confirm the results.
| Table IVParvovirus B19 infection and
clinicopathological variables. |
Table IV
Parvovirus B19 infection and
clinicopathological variables.
| B19 DNAa | |
|---|
|
| |
|---|
| Variables | Positive (%) | Negative (%) | P-valueb |
|---|
| Total patient
sample | 66 (42.3) | 90 (57.7) | |
| Male | 47 (42.7) | 63 (57.3) | 0.8697 |
| Female | 19 (41.3) | 27 (58.7) | |
| Cancer
category |
| Lung | 30 (56.6) | 23 (43.4) | 0.0095 |
| Breast | 6 (31.6) | 13 (68.4) | 0.3125 |
| Stomach | 9 (56.2) | 7 (43.8) | 0.2334 |
| Liver | 5 (31.3) | 11 (68.7) | 0.4978 |
| Prostate | 6 (46.2) | 7 (53.8) | 0.7694 |
| Intestinal | 5 (29.4) | 12 (70.6) | 0.2542 |
| Renal | 1 (20.0) | 4 (80.0) | 0.3969 |
| Other
malignanciesc | 4 (23.5) | 13 (76.5) | 0.1217 |
The highest level of HBoV seroprevalence was
detected in prostate cancer patients with 61.54%, although there is
no statistical significance due to the small sample size (Table V). The HBoV occurrence was ranked
second highest in the stomach cancer patients with a 50% (8 of 16)
seropositivity rate, followed by colon cancer with 47.1, breast
cancer with 42.11 and lung cancer with 35.85%. The liver cancer and
other malignancies, including lymphoma, nasopharyngeal cancer,
hepatocellular carcinoma, germ cell tumor, uterus carcinoma, cancer
of the larynx, brain metastases, bladder carcinoma, mediastinal
mass, endometrial, esophageal and pancreatic cancers, had a
relatively lower HBoV seroprevalence of 18.75 and 29.41%,
respectively.
| Table VParvovirus HBoV infection and
clinicopathological variables. |
Table V
Parvovirus HBoV infection and
clinicopathological variables.
| HBoV DNAa | |
|---|
|
| |
|---|
| Variables | Positive (%) | Negative (%) | P-valueb |
|---|
| Total patient
sample | 62 (39.7) | 94 (60.3) | |
| Male | 42 (38.2) | 68 (61.8) | 0.5376 |
| Female | 20 (43.5) | 26 (56.5) | |
| Cancer
category |
| Lung | 19 (35.8) | 34 (64.2) | 0.4756 |
| Breast | 8 (42.1) | 11 (57.9) | 0.8224 |
| Stomach | 8 (50.0) | 8 (50.0) | 0.3762 |
| Liver | 3 (18.8) | 13 (81.2) | 0.1042 |
| Prostate | 8 (61.5) | 5 (38.5) | 0.7694 |
| Intestinal | 8 (47.1) | 9 (52.9) | 0.5138 |
| Renal | 0 (00.0) | 5 (100.0) | 0.1577 |
| Other
malignanciesc | 5 (29.4) | 12 (70.6) | 0.5138 |
Discussion
The initial objective of this study was to determine
the correlation between parvovirus 4 occurrence and coinfection
with other parvoviruses. Therefore, sera randomly selected from 132
cancer and 83 hepatitis B patients, without known clinical
features, were screened for several viruses, including parvovirus 4
(PARV4), human bocavirus (HBoV), parvovirus B19 and hepatitis B
virus (HBV) using PCR. We found that the seroprevalence of B19 and
HBoV in cancer patients was extremely high compared to the normal
population and HBV patients (data not shown).
We further collected sera from 156 cancer and 30
hepatitis patients with pertinent clinicopathological parameters,
and examined the DNA of B19, HBoV, HBV and TTV in the sera of these
cancer and hepatitis patients, and obtained the same results. As
TTV and HBV are widely distributed throughout the world, with
characteristics of latent infection and positivity rates for the
two viruses at below 20% in healthy populations, similar to B19
occurrence, we selected these two viruses as the controls. Overall
prevalence of B19 DNA in adult cancer patients and healthy blood
donors was found to be 46.0 and 4.5%, respectively (P<0.0001),
whereas the infection rates of HBoV in cancer patients and children
with respiratory tract infections were 39.7 and 3.51%, respectively
(P<0.0001). The parvovirus B19 and HBoV viral load levels in the
diagnostic serum samples revealed a correlation between malignant
tumors and parvovirus DNA, suggesting that cancer patients are at
high risk of parvovirus B19 and HBoV infection. This is the first
study describing the high prevalence of parvovirus B19 and HBoV
infection in cancer patients, especially the high prevalence of B19
infection in lung cancer patients. Since B19 and HBoV infections
usually present with non-specific symptoms and are easily
overlooked, a high degree of suspicion and a careful search for
clinical evidence of infection are required.
A host with a compromised immune system is
particularly at risk of B19 infection, including individuals with
AIDS, cancer patients who are receiving chemotherapy and transplant
patients on immunosuppressive drugs (25). These individuals are usually unable
to produce neutralizing antibodies to clear the virus and this can
lead to persistent infection, resulting in anemia (25–26).
Therefore, it is comprehensible that the B19 infection rate in
cancer groups is higher than that in the normal population in this
study. However, the low infection prevalence of HBV and TTV in the
same cancer sera suggested that the damaged immunity of the
patients with malignant tumors is not the sole reason for
explaining the high parvovirus infection incidence.
Wang et al (24) reported that acute infection of HBoV
causes systemic infection and induces immune responses. In the
present study, we found that although HBoV commonly exists in the
serum of cancer patients, 50% (31/62) of the incidence is
coinfection with other viruses (28 of which are with B19). Thus,
whether HBoV is a major cause of malignant tumors remains to be
determined. However, it is advisable for cancer patients to avoid
contact with individuals who are infected with B19 and HBoV.
Additionally, the reasons for only lung cancer
patients being more susceptible to B19 infection remain to be
defined. We suspect that nosocomial infection by B19 may be
significant in this scenario (27).
Lung cancer is one of the most common malignant tumors in China,
and its incidence ranks first compared to all types of tumors.
Therefore, lung cancer patients are more often hospitalized to
receive chemotherapy and may have an increased risk of nosocomial
infection with B19 due to blood transmission and person-to-person
contact. In this study, sera were collected from cancer patients in
the Second Hospital of Wuhan Iron and Steel Company (WISCO). The
patients mostly work in or reside in the area near the factory.
Long-term air pollution may be the main cause of the large numbers
of lung cancers. Another possible factor is that we obtained the
majority of the serum samples from the lung cancer patients and an
insufficient sample size is the main reason for the seroprevalence
of B19 infection being of statistical significance in the
analysis.
In conclusion, human parvovirus B19 and HBoV DNA
commonly occur in the serum of cancer patients, and a
possible novel link may exist between parvovirus infection and
malignant tumors. Early diagnosis of this easily over-looked
infection is crucial and can only be achieved by a high degree of
clinical suspicion. Further studies are required to delineate an
epidemiological investigation of the correlation between malignant
tumors and human parvovirus infection.
Acknowledgements
We are grateful to all the patients who participated
in this study. This study was supported by the National Natural
Science Foundation of P.R. China (30670081).
References
|
1
|
Ozawa K and Young NS: Characterization of
capsid and noncapsid proteins of B19 parvovirus propagated in human
erythroid bone marrow culture. J Virol. 61:2627–2630.
1987.PubMed/NCBI
|
|
2
|
Bultmann BD, Klingel K, Sotlar K, et al:
Parvovirus B19: a pathogen responsible for more than hematologic
disorders. Virchows Arch. 442:8–17. 2003.PubMed/NCBI
|
|
3
|
Anderson MJ, Higgins PG, Davis LR, et al:
Experimental parvoviral infection in humans. J Infect Dis.
152:257–265. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kelleher JF, Luban NL, Mortimer PP and
Kamimura T: Human serum parvovirus: a specific cause of aplastic
crisis in children with hereditary spherocytosis. J Pediatr.
102:720–722. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pattison JR, Jones SE, Hodgson J, et al:
Parvovirus infections and hypoplastic crisis in sickle-cell anemia.
Lancet. 317:664–665. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Reid DM, Reid TM, Brown T, et al: Human
parvovirus associated arthritis: a clinical and laboratory
description. Lancet. 325:422–425. 1985. View Article : Google Scholar
|
|
7
|
Kinney JS, Anderson LJ, Farrar J, et al:
Risk of adverse outcomes of pregnancy after human parvovirus B
infection. J Infect Dis. 7:663–667. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Torok TJ: Unusual clinical manifestations
reported in patients with parvovirus B19 infection. Monogr.
20:61–92. 1997.
|
|
9
|
Ahsan N, Holman MJ, Gocke CD, et al: Pure
red cell aplasia due to parvovirus B19 infection in solid organ
transplantation. Clin Transpl. 11:265–270. 1997.PubMed/NCBI
|
|
10
|
Chernak E, Dubin G, Henry D, et al:
Infection due to parvovirus B19 in patients infected with human
immunodeficiency virus. Clin Infect Dis. 20:170–173. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kurtzman GJ, Ozawa K, Cohen B, et al:
Chronic bone marrow failure due to persistent B19 parvovirus
infection. N Engl J Med. 317:287–294. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Allander T, Tammi MT, Eriksson M, et al:
Cloning of a human parvovirus by molecular sereening of respiratory
tract samples. Proc Natl Acad Sci USA. 102:12891–12898. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Allander T: Human bocavirus. J Clin Virol.
41:29–33. 2008. View Article : Google Scholar
|
|
14
|
Lindner J, Karalar L, Schimanski S, et al:
Clinical and epidemiological aspects of human bocavirus infection.
J Clin Virol. 43:391–395. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tozer SJ, Lambert SB, Whiley DM, et al:
Detection of human bocavirus in respiratory, fecal, and blood
samples by real-time PCR. J Med Virol. 81:488–493. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fry AM, Lu X, Chittaganpitch M, et al:
Human bocavirus: a novel parvovirus epidemiologically associated
with pneumonia requiring hospitalization in Thailand. J Infect Dis.
195:1038–1045. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Allander T, Jartti T, Gupta S, et al:
Human bocavirus and acute wheezing in children. Clin Infect Dis.
44:904–910. 2007. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Neske F, Blessing K, Tollmann F, et al:
Real-time PCR for diagnosis of human bocavirus infections and
phylogenetic analysis. J Clin Microbiol. 45:2116–2122. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Vicente D, Cilla G, Montes M, et al: Human
bocavirus, a respiratory and enteric virus. Emerg Infect Dis.
13:636–637. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pozo F, García-García ML, Calvo C, et al:
High incidence of human bocavirus infection in children in Spain. J
Clin Virol. 40:224–228. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kesebir D, Vazquez M, Weibel C, et al:
Human bocavirus infection in young children in the United States:
molecular epidemiological profile and clinical characteristics of a
newly emerging respiratory virus. J Infect Dis. 194:1276–1282.
2006. View
Article : Google Scholar
|
|
22
|
Maggi F, Andreoli E, Pifferi M, et al:
Human bocavirus in Italian patients with respiratory diseases. J
Clin Virol. 38:321–325. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
García-García ML, Calvo C, Pozo F, et al:
Human bocavirus detection in nasopharyngeal aspirates of children
without clinical symptoms of respiratory infection. Pediatr Infect
Dis J. 27:358–360. 2008.PubMed/NCBI
|
|
24
|
Wang K, Wang W, Yan H, et al: Correlation
between bocavirus infection and humoral response, and co-infection
with other respiratory viruses in children with acute respiratory
infection. J Clin Virol. 47:148–155. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Young NS: Parvoviruses. Fields Virology.
Knipe DM and Howley PM: 3rd edition. Lippincott, Williams and
Wilkins; Philadelphia, USA: pp. 2199–2220. 1996
|
|
26
|
Kurtzman GJ, Cohen BJ, Field AM, et al:
Immune response to B19 parvovirus and an antibody defect in
persistent viral infection. J Clin Invest. 84:1114–1123. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sung HK, Lin LI, Chang CJ, et al:
Increased risk of parvovirus B19 infection in young adult cancer
patients receiving multiple courses of chemotherapy. J Clin
Microbiol. 40:3909–3912. 2002. View Article : Google Scholar : PubMed/NCBI
|














