Introduction
The most common benign odontogenic tumor of the jaw
is ameloblastoma, whereas ameloblastic carcinoma (AC) is rare. For
a long time, malignancy in ameloblastoma has been the subject of
controversy (1,2). In the 2005 World Health Organization
(WHO) classification (3),
odontogenic carcinomas included malignant ameloblastoma, AC and
primary intraosseous, ghost cell odontogenic and clear cell
odontogenic carcinomas. Malignant ameloblastoma is described as a
metastasizing ameloblastoma that presents with benign histological
characteristics in primary and metastatic lesions. By contrast, AC
is considered to be a rare malignant odontogenic tumor that has
combined histopathological features of ameloblastoma and carcinoma,
regardless of the presence or absence of metastasis. Furthermore,
AC has been classified into two types, primary and secondary. The
former develops de novo and the latter develops by malignant
transformation of a pre-existing benign ameloblastoma (3).
The mean age of AC occurrence is 30.1 years, but a
wide range of ages can be affected. There is no proven gender bias,
but certain studies have reported a male predominance (4,5).
Similar to ameloblastoma, AC is commonly located in the posterior
portion of the mandible and is extremely rare in the maxillary
region. The most usual clinical complaint is swelling, but other
symptoms, including dysphonia, associated pain, trismus and rapid
growth have been reported (2,4).
Radiography of AC can reveal poorly-defined radiolucency,
occasionally with focal radiopacities. These findings, which are
extremely unusual for ameloblastoma, could be due to necrosis with
dystrophic calcification in AC (4,6). With
regard to clinical behavior, AC tends to be aggressive and extends
with local destruction. Lymph node involvement and distant
metastasis to various regions have also been reported (4,7).
Therefore, diagnostic imaging prior to treatment is extremely
important. In comparison to AC of the mandible, AC of the maxilla
has not yet been well documented due to the lack of information
about this rare carcinoma.
The present study reports the clinical,
histological, immunohistochemical and therapeutic details of a case
of maxillary AC with a 22-month follow-up period. In addition, the
present study reviews a 60-year period of the literature with
regard to the clinical details, treatment results and
histopathological and phenotypic information available for AC of
the maxilla. Written informed consent was obtained from the
patient.
Case report
Patient characteristics and case
presentation
A 22-year-old male was referred to the Department of
Oral and Maxillofacial Surgery (Graduate School, Tokyo Medical and
Dental University Hospital, Tokyo, Japan). The patient complained
of painless swelling in the right maxilla that had been present for
one month. The facial configuration appeared symmetrical upon
clinical examination, but an intraoral examination revealed
elastic, hard, well-defined swelling with a smooth surface in the
right maxillary molar region. The lesion measured 31×25×15 mm in
size (Fig. 1).
Panoramic radiography revealed a cystic radiolucent
lesion in the right maxilla elevating the floor of the right
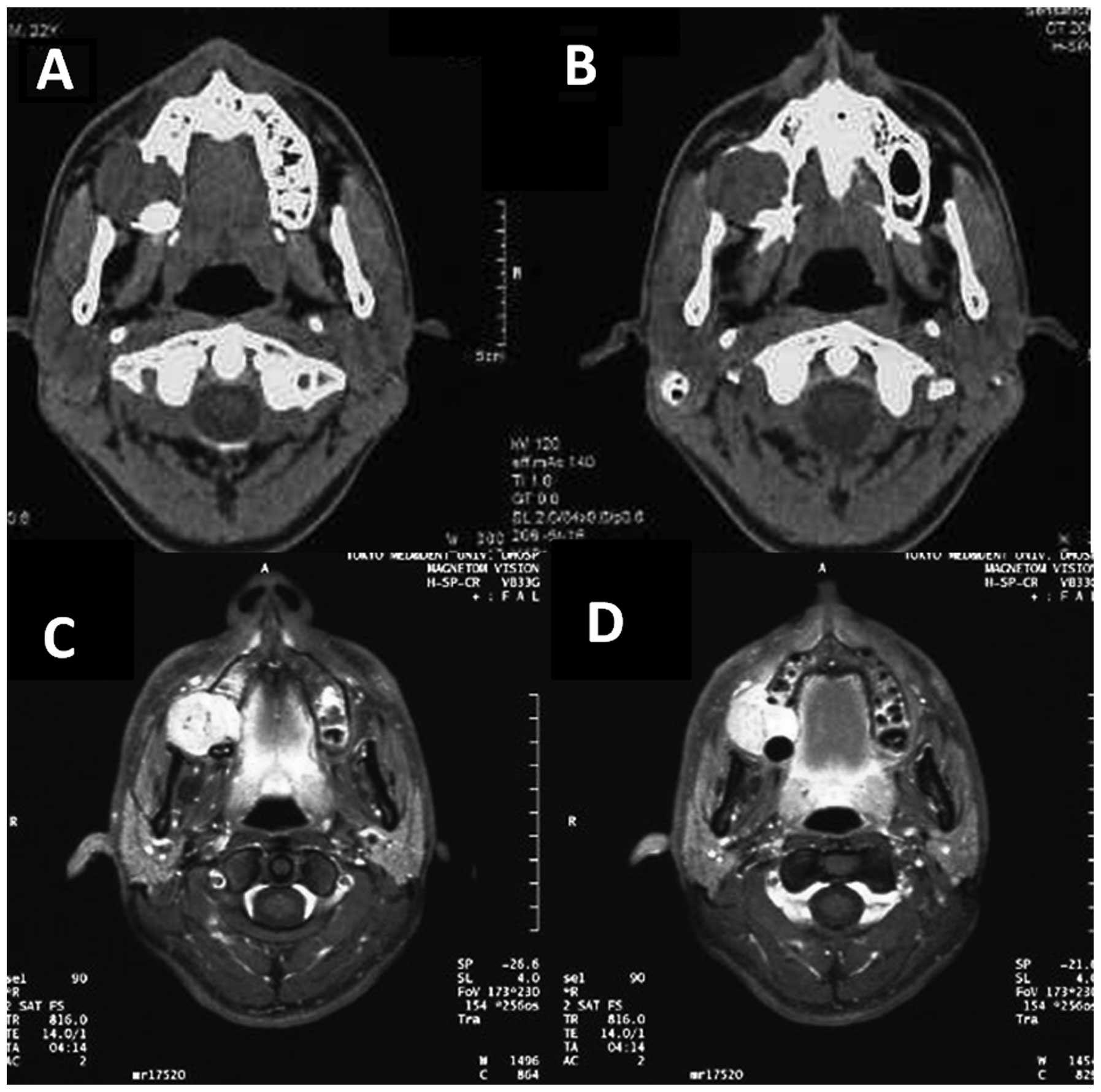
maxillary sinus (Fig. 2). Computed
tomography (CT) examination was subsequently performed. The axial
CT image revealed a globular-shaped lesion arising from the inside
of the maxillary bone, with destruction of the posterior wall and
alveolar bone. The diameter of this lesion reached 30 mm in size.
The right maxillary tuberosity and pterygoid plates appeared to be
intact, but coronal CT imaging revealed destruction of the elevated
sinus floor in the right posterior maxilla. The margin of the
lesion was almost well defined. These findings indicated that this
lesion was a benign tumor, such as an ameloblastoma (Fig. 3A and B). An incision biopsy was
performed and the lesion was revealed not to be cystic, but to be a
solid mass. Although the biopsy revealed that the lesion was an
odontogenic carcinoma, its histopathological type was
unidentifiable. Next, 18F-fluorodeoxyglucose-positron
emission tomography (FDG-PET)/CT was performed to examine the
extent of the primary lesion and the presence of regional lymph
node and distant metastasis. Furthermore, contrast-enhanced
magnetic resonance imaging (CE-MRI) with gadodiamide, including a
dynamic study, was performed to evaluate soft-tissue invasion at
the maxillary sinus and pterygopalatine fossa.
On FDG-PET imaging, slightly elevated FDG uptake was
identified in the right maxilla and bilateral superior internal
jugular nodes. The maximum standardized uptake value
(SUVmax) was 5.6 in the right maxilla, 3.3 in the right
cervical lymph node and 2.6 in the left cervical lymph node. No
abnormal uptake indicating distant metastasis was observed on
FDG-PET images (Fig. 4). CE-MRI
revealed a distinctly-bordered lesion that was 31×30 mm in size and
extended from the right maxillary alveolar process to the right
palate and reached the retromaxillary fat space. This lesion
exhibited intermediate signal intensity on T1-weighted imaging and
heterogeneous high signal intensity on T2-weighted and short TI
inversion-recovery imaging (Fig. 3C and
D). In addition, ultrasonography was performed to evaluate the
bilateral superior internal jugular nodes, which exhibited slight
FDG uptake on the FDG/PET analysis. The findings did not indicate
that a metastatic lymph node lesion was present.
On the basis of these imaging findings, the patient
was diagnosed with an odontogenic carcinoma of the right maxilla
(T4N0M0, stage IV). The patient underwent a right partial
maxillectomy and full-thickness skin grafting from the left
inguinal region. Following the surgery, the diagnosis was
histopathologically confirmed using the whole surgical specimen.
These lesions were pathologically diagnosed as AC.
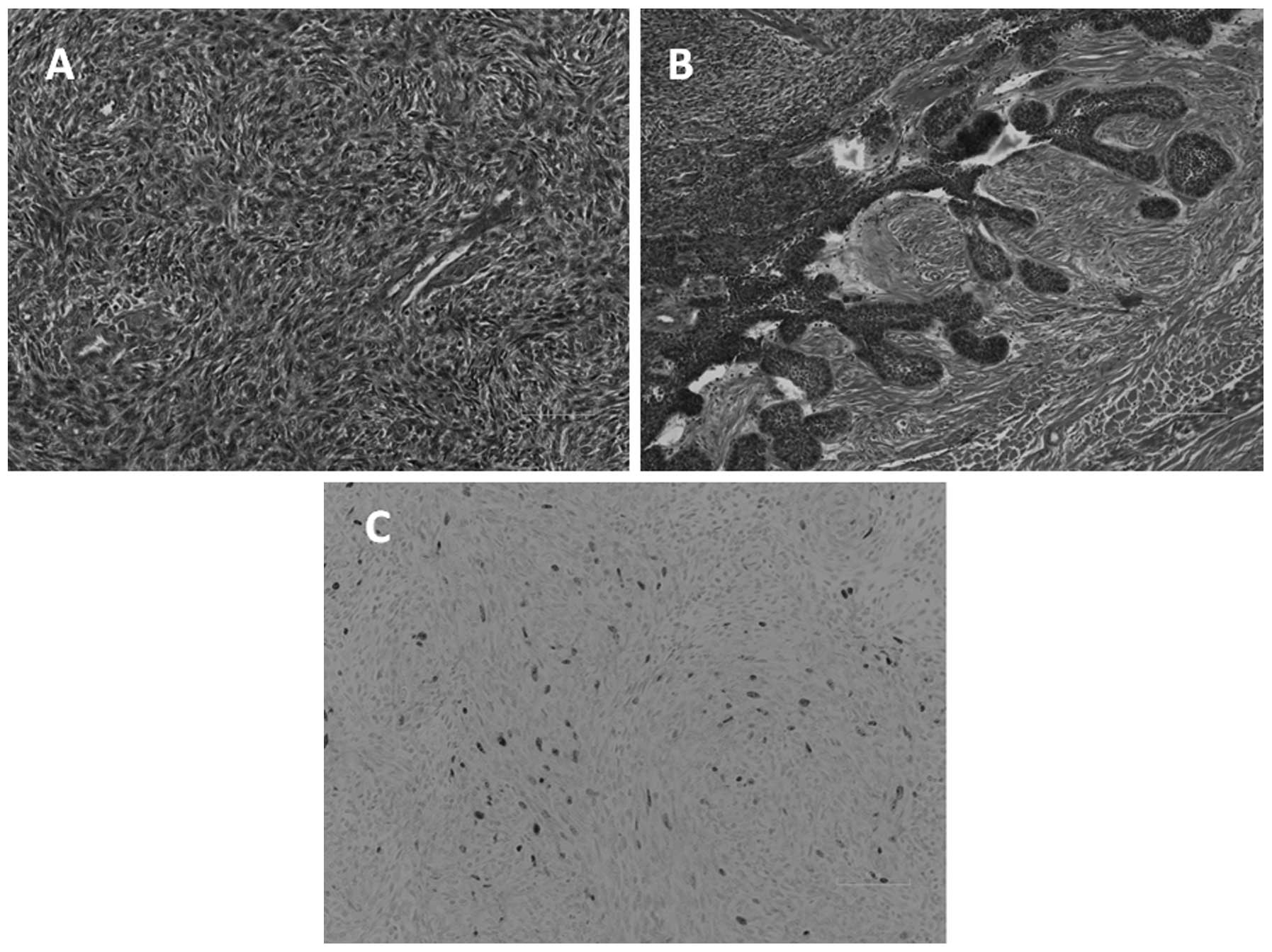
Microscopic examination revealed the presence of an
osteolytic mass with slit-like cystic formation. The majority of
the mass consisted of spindle tumor cells exhibiting a storiform,
pseudosarcomatous pattern. The epithelial component demonstrated
cytological malignancy, characterized by nuclear pleomorphism, an
increased nucleus to cytoplasm ratio, hyperchromatic nuclei and a
high mitotic rate (Fig. 5A). By
contrast, an alternative region of the tumor, the tumor cell nest,
revealed peripheral palisading of columnar cells, with a vacuolated
cytoplasm and reverse-polarized nuclei. These findings were similar
to those for ameloblastoma (Fig.
5B). In the immunohistological assessment, the specimen was
found to be positive for cytokeratin AE1/3 and vimentin expression.
The Ki-67 proliferation index was 5%, indicating that the tumor was
of low malignancy (Fig. 5C).
Therefore, it was concluded that the tumor was a primary AC, based
on the histopathological and immunohistochemical findings.
The post-operative progress of the patient was fair,
resulting in discharge from the hospital on the 22nd day. At the 22
months post-surgical follow-up examination, the patient was free of
symptoms and neither recurrence nor metastases were detected.
Analysis of the literature on AC,
including the present case
A review of the English literature published between
1948 and 2012 revealed 45 cases of maxillary AC, including the
present case (1,2,4–33).
These cases are summarized in Table
I. The 45 patients ranged in age between 5 and 90 years, with
an average age of 55.2 years. A breakdown of the age distribution
is presented in Fig. 6. The studies
reported the cases of 34 males and 11 females, with a male to
female ratio of 3:1. The predominant symptom of AC was swelling,
followed by ulceration, pain and bleeding. According to the
literature, AC occurs most often in the posterior maxilla.
 | Table IAxillary ameloblastic carcinomas:
Review of published reports. |
Table I
Axillary ameloblastic carcinomas:
Review of published reports.
| Case | First author, year
(ref.) | Gender | Age | Symptoms | Location | Tumor type | Primary
treatment | Time between
treatment and recurrence, months | Treatment for
recurrence | Time to metastasis,
months | Site of
metastasis | Follow-up,
months | Outcome |
|---|
| 1 | Grimes and Stephens,
1948 (8) | F | 56 | Unknown | Po | S | S/R | | | 120 | Lung | 120 | NM |
| 2 | Eda et al,
1972 (9) | F | 44 | Painless
swelling | Po | S | Sa | 1st, 43 | Sa | 120 | LN, lung,
vertebra | 121 | Dc |
| | | | | | | | 2nd, 32 | Sa | | | | |
| | | | | | | | 3rd, 8 | Sa | | | | |
| | | | | | | | 4th, 8 | Sa | | | | |
| | | | | | | | 5th, 5 | R | | | | |
| 3 | Krempien et
al, 1979 (10) | M | 5 | Unknown | NM | M | Sa | | | 72 | LN, lung | 144 | Ao |
| 4 | Daramola et
al, 1980 (11) | M | 22 | Swelling | Po | S | Sa | 1st, 24 | Sa | 60 | Lung | NM | NM |
| | | | | | | | 2nd, 36 | C/R | | | | |
| 5 | Madiedo et
al, 1981 (12) | M | 49 | Swelling | Po | S | Sa | 1st, 18 | S+ND/R | 36 | Lung | 60 | Dc |
| | | | | | | | 2nd, 42 | C | | | | |
| 6 | Andersen and Bang,
1986 (13) | M | 77 | Bleeding | S | S | Sa | 36 | Sa | | | NM | NM |
| 7 | Nadimin et
al, 1986 (14) | F | 15 | Swelling | APo | P | Sa | | | | | NM | NM |
| 8 | Corio et al,
1987 (4) | M | 15 | Swelling | NM | ND | Sa | | | | | NM | NM |
| 9 | Inoue et al,
1988 (15) | F | 51 | Swelling | Po | S | Sa | 137 | Sa | 145 | Lung | 186 | Dc |
| 10 | MacClatchey et
al, 1989 (16) | F | 77 | Concavity,
granulation | Po | P | Sa | | | | | 24 | Ao |
| 11 | Lee et al,
1990 (17) | M | 56 | Pain | Po | P | S/R | 3 | Untreated | 6 | Mandible | 7 | NM |
| 12 | Lolachi et
al, 1995 (18) | F | 82 | Trismus,
bleeding | S | P | Sa | | | | | NM | NM |
| 13 | Ingram et
al, 1996 (19) | M | 83 | Pain, erosion | Po | P | S/R | | | | | 24 | Ao |
| 14 | Infante-Cossio
et al, 1998 (20) | F | 69 | Painless swelling,
anaethesia | APoS | P | S/R | | | | | 60 | Ao |
| 15 | | M | 77 | Swelling, pain,
anaesthesia | APoS | P | S/R | | Untreated | | | 9 | Dc |
| 16 | | M | 64 | Swelling,
fistula | PoS | P | S/R | | | | | 36 | Ao |
| 17 | Sastre et
al, 2002 (21) | M | 40 | Painful
swelling | A | P | S/S | | | | | 24 | Ao |
| 18 | Dhir et al,
2003 (22) | M | 72 | Unknown | PoS | P | S/R | | | | | 20 | Ao |
| 19 | Avon et al,
2003 (23) | M | 68 | Fistula | PoMS | P | S/S | | | | | 24 | Ao |
| 20 | Oginni et
al, 2003 (24) | F | 61 | Bleeding | Po | P | Sa | 15 | Untreated | | | 15 | Ac |
| 21 | Zwahlen et
al, 2003 (25) | M | 44 | Ulcer | Po | M | S/R | 1st, 72 | Sa | 156 | Lung, mycardial,
skull base | 156 | Dc |
| | | | | | | | 2nd, 24 | Sa | | | | |
| | | | | | | | 3rd, 12 |
R/Sb | | | | |
| 22 | Goldenberg et
al, 2004 (7) | M | 72 | Unknown | NM | ND | S/R | | | | | 36 | Ao |
| 23 | Philip et
al, 2005 (26) | M | 70 | Unknown | NM | P | S/R | | | | | 40 | Ao |
| 24 | | M | 56 | Unknown | NM | P | S/R | | | | | 8 | Ao |
| 25 | Hall et al,
2007 (27) | M | 15 | Swelling | A | S | Sa | 1st, 10 | Sa | | | 196 | Ao |
| | | | | | | | 2nd, 28 | Sa | | | | |
| | | | | | | | 3rd, 2 | Sa | | | | |
| 26 | | M | 16 | Swelling | PoMS | S | Sa | | | | | 288 | Ao |
| 27 | | M | 75 | Numbness, loose
tooth, nasal obstruction | PoMS | S | Sa | 27 | Sa | | | 153 | Do |
| 28 | | F | 7 | Swelling | Po | S | Sa | 35 | Sa | | | 119 | Ao |
| 29 | | M | 63 | Swelling,
ulcer | PoMS | S | Sa | 1st, 151 | Sa | | | 228 | Dc |
| | | | | | | | 2nd, 13 | Sa | | | | |
| | | | | | | | 3rd, 50 | Sa | | | | |
| | | | | | | | 4th, 14 | Biopsy | | | | |
| 30 | | M | 52 | Nasal congestion,
pain | PoMS | S | Sa | 47 | C | 47 | Lung, liver | 51 | Ac |
| 31 | Ward et al,
2007 (28) | M | 64 | Swelling,
erythema | A | P | Sa | | | | | 42 | Ao |
| 32 | Benlyazid et
al, 2007 (5) | M | 90 | Exophytic,
ulcer | Po | P | Sa | | | | | 25 | Do |
| 33 | Naik and Kale, 2007
(6) | M | 70 | Swelling | APoMS | P | Sa | | | | | 12 | Ao |
| 34 | Yazici et
al, 2008 (29) | M | 10 | Swelling | S | P | S/R | | | | | 6 | Ao |
| 35 | Angiero et
al, 2008 (1) | M | 68 | Bleeding | PoMS | S | Sa | | | | | 6 | Ao |
| 36 | Yoon et al,
2009 (2) | M | 63 | Ulcer,
swelling | Po | P | S/R | 1st, Unknown | Sa | | | 13 | Ao |
| | | | | | | | 2nd, Unknown | Sa | | | | |
| 37 | | F | 73 | Pain, swelling | PoMS | P | Sa | | | | | 31 | Ao |
| 38 | | M | 61 | Pain, swelling,
trismus | PoMS | P | Biopsy | | | | | NM | NM |
| 39 | Yoon et al,
2009 (2) | M | 58 | Pain, ulcer | P | P | S+ND | | | | | 12 | Ao |
| 40 | Lucca et al,
2010 (30) | M | 73 | Swelling | APoMS | P | Biopsy | | | | | 4 | Dc |
| 41 | | M | 69 | Ulcer | P | P | Sa | | | | | 11 | Ao |
| 42 | Matsuzaki et
al, 2011 (31) | F | 73 | Swelling | PoMS | P | Sa | | | | | 12 | Ao |
| 43 | Nicolotti et
al, 2011 (32) | M | 77 | Swelling,
ulcer | AP | P | Sb | | | 0 | Lung, liver,
cerebal | 5 | Dc |
| 44 | França et
al, 2012 (33) | M | 59 | Swelling, pain | APoMS | ND | S/R | | | | | 24 | Ao |
| 45 | Present case | M | 22 | Swelling | Po | P | Sa | | | | | 13 | Ao |
The type of AC was classified according to the
clinical, follow-up, histopathological and phenotypic information
available for these cases. As a result, 27 cases (60%), including
the present case, developed de novo, primary AC, and 13
cases (29%) arose from a pre-existing ameloblastoma as secondary
AC. The remaining three cases could not be determined using the
information provided and two cases presented with a benign
histological appearance in the primary and metastatic regions,
indicating malignant ameloblastoma. Of the 27 primary and 13
secondary AC cases, follow-up data were available for 23 primary
cases and 10 cases of carcinoma ex ameloblastoma. Of the 23 cases
with both primary AC and follow-up data, only three patients
(13.0%) succumbed to the disease. By contrast, four of the 10 cases
of secondary AC with follow-up data (40%) succumbed to the
tumor.
With regard to the first treatment modality for the
primary lesions, 28 of the 45 cases (62.2%) only underwent surgical
resection and 14 (31.1%) underwent surgical resection and adjuvant
radiotherapy. In the remaining three cases, biopsy only was
performed in two cases and palliative tumor reduction was performed
in one case. When these six cases were excluded, primary recurrence
occurred in 15 of the 39 cases (38.5%). Although eight out of the
15 patients (53.3%) experienced recurrence only once, the remaining
seven patients experienced recurrence several times. The mean
duration between the primary treatment and the initial recurrence
was 47.5 months, with a wide range of 3–151 months. In addition, in
seven of the 15 primary recurrence cases (46.7%), distant
metastasis was observed in several regions. In total, 10 of the 39
patients (25.6%) experienced metastatic lesions. Regional
metastasis occurred in three cases and distant metastasis occurred
in nine cases. In the cases with regional metastasis, two involved
lymph node metastasis and the remaining case involved maxillary AC
that had metastasized to the mandible. The most common region of
distant metastasis was the lung, occurring in nine cases (8–12,15,25,27,33).
Distant metastasis was also reported in the liver in two cases
(27,32), in the bone in two cases (9,25), in
the brain in one case (32) and in
the myocardium in one case (25).
Survival analyses were performed on the 35 cases
with follow-up data. Three cases not undergoing curative treatment
and seven cases without a description of the treatment outcome were
excluded from the survival analyses. Overall, 12 of the 35 patients
(34.3%) had experienced a recurrence of the disease and eight
patients (22.9%) succumbed to AC. Kaplan-Meier survival curves for
disease-free survival (DFS) and overall survival (OS) are presented
in Fig. 7A and B, respectively. The
five- and 10-year DFS rates were 53.7 and 32.2%, respectively. The
five-year OS rate was 83.2% and the 10-year OS rate was 32.2%, the
same as that for DFS. Although approximately half of the cases
experienced recurrence of the disease in less than five years,
salvage treatment appeared to be successful in several cases.
Discussion
There has been controversy regarding the definition
and classification of AC in the past. The 1972 WHO classification
of odontogenic carcinoma included malignant ameloblastoma, but the
term AC was not used in that classification. The term malignant
ameloblastoma refers to tumors that metastasize to several regions
while the histological appearance of the primary and metastatic
lesions remains benign (34). The
term AC was introduced by Elazy in 1982 (35). In addition, in 1984, Slootweg and
Müller provided definitions and nomenclature used to distinguish AC
from malignant ameloblastoma (36).
In the 2005 WHO classification, AC is defined as a rare odontogenic
malignant tumor in which the histopathological features of
ameloblastoma and malignancy coexist. In addition, AC can develop
de novo, as the primary type, or by malignant transformation
of an ameloblastoma, as the secondary type, with a distinction
between carcinoma ex intraosseous ameloblastoma and carcinoma ex
peripheral ameloblastoma (3). In
the present study, no pre-existing ameloblastoma in the right side
of the maxilla was identified and the presence of the combined
histopathological features of ameloblastoma and malignancy were
confirmed. Therefore, the tumor in the present case was diagnosed
as a primary AC.
Recently, Casaroto et al reported a case of
AC that arose in the mandible and also presented a literature
review of AC classified into primary or secondary types using the
recent WHO classification (40). In
total, 31 studies published between 2005 and 2011 were reviewed,
with 15 cases arising from the maxilla and 16 from the mandible. It
was indicated that the primary type occurs more frequently in the
maxilla, unlike the secondary type, which was reported more often
in the mandible. In addition, it was found that the secondary type
appears to correlate with recurrence and mortality, suggesting that
it is more aggressive compared with the primary type. The present
study also reviewed 45 AC cases that had occurred in the maxilla
from a 60-year period. The results of the present study were
compatible with those of the aforementioned study and confirmed
that primary AC is dominant in the maxilla and is not as aggressive
as secondary AC.
Due to the rarity of large clinical series and
long-term follow-up, there is no consensus on the treatment of AC.
Based on follow-up data from the present review, radical surgical
resection appears to be the most reliable treatment of choice. In
the present review, wide surgical resection was performed in 42 of
the 45 cases (93.3%). With regard to the surgical margin, Avon
et al advocated 2- or 3-cm bony margins for an en bloc
removal (23). In addition, Zwahlen
and Grätz also recommended partial maxillectomy with a 10–15-mm
safety margin of healthy bone, including the lateral nasal wall,
alveolar ridge, mucosa of the maxillary sinus and hard palate
(41). However, even if various ACs
occurred in the same patient, it was revealed that aggressiveness
varied according to whether the AC was primary or secondary
(40). Thus, surgical margins
should be determined with consideration of tumor types. In the
cases of secondary AC, the surgical margin should be set to at
least 10–15 mm. By contrast, in the case of primary AC, it may be
possible to decrease the surgical margins. Neck dissection should
also be considered when there is evident lymphadenopathy. By
contrast, controversy remains regarding the treatment of AC, with
certain studies suggesting radiotherapy (26) and others doubting its effectiveness
(27). Although primary
radiotherapy is not a reliable treatment modality, it is expected
to be useful in cases with perineural or massive soft-tissue
invasion and in cases with positive surgical margins (26). In the present review, radiotherapy
was used as either a primary or secondary treatment in the 20 cases
(44.4%) with metastatic or recurrent disease out of the 45 total
cases. Experience with chemotherapy as a treatment of AC is
minimal. In the present study, only three patients with a
progressive AC were treated with chemotherapy. One of these
patients succumbed to AC and the response to this treatment was not
described in the remaining cases. Several studies have also
reported that this modality appears to have limited value in the
treatment of AC (37,38).
In the present study, the local recurrence of AC
occurred in 15 out of 39 cases (38.4%). In addition, half of these
cases experienced recurrence several times and distant metastases
occurred in several regions. The presence of recurrence appears to
correlate with mortality, since the majority of the cases that
resulted in mortality had a previous history of tumor recurrence.
These findings strongly indicate that an early, aggressive and
complete removal of the tumor is the best treatment for survival.
Additionally, a more radical and aggressive treatment modality is
required in cases with primary recurrence. The other significant
problem in treating AC is that the period of recurrence and distant
metastasis is long compared with other malignancies that occur in
the head and neck regions, such as squamous cell carcinomas. In the
present review, the average period between primary treatment and
recurrence was 47.5 months, with a wide range of 3 to 151 months.
In addition, the mean interval between the initial treatment and
the manifestation of distant metastasis was 84.7 months, although
the development of metastasis reached up to 156 months after
primary treatment. Since there is no definitive modality or
strategy for a follow-up of this tumor, long-term periodic
follow-up following surgical resection is indispensable for the
early detection of recurrence and metastatic lesions.
The nuclear protein Ki-67 antigen has been used to
determine the proliferation rate of numerous types of tumors and
cystic lesions. This is a reliable marker of cellular
proliferation. The results on immunohistochemistry for the Ki-67
labeling index (LI) in seven maxillary ACs, including the present
case, are as follows: Yoon et al reported six cases of AC,
with five cases occurring in the maxilla and one case occurring in
the mandible, and the mean Ki-67 LI of these six cases was
determined to be 13.91% (standard deviation, 6.96; range,
9.30–22.9%) (2). Yazici et
al also examined a case of maxillary AC that occurred in a
10-year-old male, and the Ki-67 LI was determined to be 10%
(29). In the present case,
immunohistochemical examination of Ki-67 was performed on the only
biopsy specimen, but the LI was only 5%. This result suggests that
the tumor in the present case possessed low malignancy compared
with those in the previous studies.
AC is known to have not only locally invasive
features, but to also result in regional and distant metastases. AC
metastasizes to the lung and other regions, including the cervical
lymph nodes, brain, bones, soft tissue and liver. Thus, the
extension of the lesion must be closely assessed and the patient
must be carefully examined to exclude the existence of metastases
and lesions elsewhere in the body. FDG-PET is a useful modality for
the evaluation of malignant tumors in the primary site and the
detection of regional lymph node and distant metastasis. However,
there have been a few studies investigating FDG-PET of AC.
Matsuzaki et al previously reported a case of maxillary AC
where strong FDG uptake (SUVmax, 28.3) was observed in
the primary tumor. However, there were no abnormal FDG
accumulations that suggested metastasis in that case (31). In the present case, slightly
elevated FDG uptake was observed in the primary lesion
(SUVmax, 5.6) and bilateral superior internal jugular
nodes (right side SUVmax, 3.3; left side
SUVmax, 2.6). No abnormal uptake that would suggest
distant metastasis was observed on the FDG-PET images in the
present case. Since AC has the potential for distant metastasis,
with or without cervical lymph node metastasis, it is essential to
use PET for the initial whole-body examination prior to
surgery.
In summary, the present study reports the case of a
22-year-old male patient with AC of the maxilla. AC is rare
disorder and its treatment remains controversial. The prognosis of
AC is dominated by the risk of local recurrence and distant
metastases, but the present patient has not yet experienced
recurrence or metastasis during the 22-month post-surgical
follow-up. Continued and long-term follow-up is mandatory to detect
late recurrence and metastasis. In addition, continued research,
case studies and treatment experience are necessary to establish
more useful treatment and management strategies for this rare
tumor.
References
|
1
|
Angiero F, Borloni R, Macchi M and Stefani
M: Ameloblastic carcinoma of the maxillary sinus. Anticancer Res.
28:3847–3854. 2008.
|
|
2
|
Yoon HJ, Hong SP, Lee JI, et al:
Ameloblastic carcinoma: an analysis of 6 cases with review of the
literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
108:904–913. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Barnes L, Eveson JW, Reichart P and
Sidransky D: Odontogenic carcinomas. World Health Organization
Classification of Tumours. Pathology and Genetics of Head and Neck
Tumours. IARC Press; Lyon: pp. 287–293. 2005
|
|
4
|
Corio RL, Goldblatt LI, Edwards PA and
Hartman KS: Ameloblastic carcinoma: a clinicopathologic study and
assessment of eight cases. Oral Surg Oral Med Oral Pathol.
64:570–576. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Benlyazid A, Lacroix-Triki M, Aziza R, et
al: Ameloblastic carcinoma of the maxilla: case report and review
of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 104:e17–e24. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Naik V and Kale AD: Ameloblastic
carcinoma: a case report. Quintessence Int. 38:873–879. 2007.
|
|
7
|
Goldenberg D, Sciubba J, Koch W and Tufano
RP: Malignant odontogenic tumors: a 22-year experience.
Laryngoscope. 114:1770–1774. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Grimes OF and Stephens HB: Adamantinoma of
the maxilla metastatic to the lung: case report. Ann Surg.
128:999–1005. 1948. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Eda S, Koike H, Tachikawa T, et al: An
autopsy case of the malignant ameloblastoma with metastases to the
submaxillary lymph nodes, lungs and thoracic vertebrae. Bull Tokyo
Dent Coll. 13:91–101. 1972.PubMed/NCBI
|
|
10
|
Krempien B, Brandeies WE and Singer R:
Ameloblastoma with metastases in a child. Light- and electron
microscopic findings. Virchows Arch A Path Anat Histol.
381:211–222. 1979.(In German). View Article : Google Scholar
|
|
11
|
Daramola JO, Abioye AA, Ajagbe HA and
Aghadiuno PU: Maxillary malignant ameloblastoma with intraorbital
extension: report of case. J Oral Surg. 38:203–206. 1980.PubMed/NCBI
|
|
12
|
Madiedo G, Choi H and Kleinman JG:
Ameloblastoma of the maxilla with distant metastases and
hypercalcemia. Am J Clin Pathol. 75:585–591. 1981.PubMed/NCBI
|
|
13
|
Andersen E and Bang G: Ameloblastic
carcinoma of the maxilla. A case report. J Maxillofac Surg.
14:338–340. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Nadimi H, Toto PD, Jaffe E and McReynolds
HD: Basement membrane defect in ameloblastic carcinoma: a case
study. J Oral Med. 41:79–81. 1986.PubMed/NCBI
|
|
15
|
Inoue N, Shimojyo M, Iwai H, et al:
Malignant ameloblastoma with pulmonary metastasis and
hypercalcemia: report of an autopsy case and review of the
literature. Am J Clin Pathol. 90:474–481. 1988.PubMed/NCBI
|
|
16
|
McClatchey KD, Sullivan MJ and Paugh DR:
Peripheral ameloblastic carcinoma: a case report of a rare
neoplasm. J Otolaryngol. 18:109–111. 1989.PubMed/NCBI
|
|
17
|
Lee L, Maxymiw WG and Wood RE:
Ameloblastic carcinoma of the maxilla metastatic to the mandible.
Case report. J Craniomaxillofac Surg. 18:247–250. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lolachi CM, Madan SK and Jacobs JR:
Ameloblastic carcinoima of the maxilla. J Laryngol Otol.
109:1019–1022. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ingram EA, Evans ML and Zitsch RP III:
Fine-needle aspiration cytology of ameloblastic carcinoma of the
maxilla: a rare tumor. Diagn Cytopathol. 14:249–252. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Infante-Cossio P, Hernandes-Guisado JM,
Fernandez-Machin P, et al: Ameloblastic carcinoma of the maxilla: a
report of 3 cases. J Craniomaxillofac Surg. 26:159–162. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sastre J, Muñoz M, Naval L and Adrados M:
Ameloblastic carcinoma of the maxilla: report of a case. J Oral
Maxillofac Surg. 60:102–104. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Dhir K, Sciubba J and Tufano RP:
Ameloblastic carcinoma of the maxilla. Oral Oncol. 39:736–741.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Avon SL, McComb J and Clokie C:
Ameloblastic carcinoma: case report and literature review. J Can
Dent Assoc. 69:573–576. 2003.PubMed/NCBI
|
|
24
|
Oginni FO, Ugboko VI, Owotade JF and
Adebiyi KE: Ameloblastic carcinoma of the jaws. A report of three
Nigerian cases. Odontostomatol Trop. 104:19–22. 2003.
|
|
25
|
Zwablen RA, Vogt P, Fiscber FS and Grätz
KW: Case report: myocardical metastasis of a maxillary
ameloblastoma. J Oral Maxillofac Surg. 61:731–734. 2003. View Article : Google Scholar
|
|
26
|
Philip M, Morris CG, Werning JW and
Mendenhall WM: Radiotherapy in the treatment of ameloblastoma and
ameloblastic carcinoma. J HK Coll Radiol. 8:157–161. 2005.
|
|
27
|
Hall JM, Weathers DR and Unni KK:
Ameloblastic carcinoma: an analysis of 14 cases. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod. 103:799–807. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ward BB, Edlund S, Sciubba J and Helman
JI: Ameloblastic carcinoma (primary type) isolated to the anterior
maxilla: case report with review of the literature. J Oral
Maxillafac Surg. 65:1800–1803. 2007. View Article : Google Scholar
|
|
29
|
Yazici N, Karagöz B, Varan A, et al:
Maxillary ameloblastic carcinoma in a child. Pediatr Blood Cancer.
50:175–176. 2008. View Article : Google Scholar
|
|
30
|
Lucca M, D’Innocenzo R, Kraus JA, et al:
Ameloblastic carcinoma of the maxilla: a report of 2 cases. J Oral
Maxillofac Surg. 68:2564–2569. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Matsuzaki H, Katase N, Hara M, et al:
Ameloblastic carcinoma: a case report with radiological features of
computed tomography and magnetic resonance imaging and positron
emission tomography. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 112:e40–e47. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Nicolotti M, Brucoli M, Arcuri F and
Benech A: Ameloblastic carcinoma: rare localization of a rare
neoplasm. J Craniofac Surg. 22:2353–2355. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
França DC, Moreira JM Jr, De Aguiar SM, et
al: Ameloblastic carcinoma of the maxilla: A case report. Oncol
Lett. 4:1297–1300. 2012.PubMed/NCBI
|
|
34
|
Kramer IRH, Pindborg JJ and Torloni H:
International Histological Classification of Tumours. Histological
Typing of Odontogenic Tumors, Jaw, Cyst and Allied Lesions. World
Health Organization; Geneva: 1971
|
|
35
|
Elzay RP: Primary intraosseous carcinoma
of the jaws. Review and update of odontogenic carcinomas. Oral Surg
Oral Med Oral Pathol. 54:299–303. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Slootweg PJ and Müller H: Malignant
ameloblastoma or ameloblastic carcinoma. Oral Surg Oral Med Oral
Pathol. 57:168–176. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lanham RJ: Chemotherapy of metastatic
ameloblastoma. A case report and review of the literature.
Oncology. 44:133–134. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Duffey DC, Bailet JW and Newman A:
Ameloblastoma of the mandible with cervical lymph node metastasis.
Am J Otolaryngol. 16:66–73. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ramadas K, Jose CC, Subhashini J, et al:
Pulmonary metastases from ameloblastoma of the mandible treated
with cisplatin, adriamycin, and cyclophosphamide. Cancer.
66:1475–1479. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Casaroto AR, Toledo GL, Filho JL, et al:
Ameloblastic carcinoma, primary type: case report,
immunohistochemical analysis and literature review. Anticancer Res.
32:1515–1525. 2012.PubMed/NCBI
|
|
41
|
Zwahlen RA and Grätz KW: Maxillary
ameloblastomas: a review of the literature and of a 15-year
database. J Craniomaxillofac Surgery. 30:273–279. 2002. View Article : Google Scholar
|