Introduction
Pheochromocytomas (also known as paragangliomas) are
functional or non-functional tumors of the sympathetic nervous
tissue (1). Catecholamine is
secreted by functional pheochromocytomas, resulting in paroxysmal
hypertension and palpitation. The majority of pheochromocytomas are
derived from the chromaffin tissue of the adrenal medulla (2). Extra-adrenal pheochromocytomas are
rare tumors that originate from the chromaffin tissue of the
sympathetic nervous system (3). In
adults, pheochromocytomas are often called the ‘10% tumor’, as ~10%
occur above the diaphragm, while 10% of intra-abdominal
pheochromocytomas are extra-adrenal, 10% are bilateral, 10% are
multiple, 10% are familial, 10% are malignant and 10% recur
post-operatively (3). Diagnosing
extra-adrenal pheochromocytomas is challenging due to their low
incidence, and as their clinical manifestations can be
inconsistent. The present study reports an extra-adrenal
pheochromocytoma that was localized to the ovary, presented as
gynecologically asymptomatic and was detected via computed
tomography angiography (CTA). Written informed consent was obtained
from the patient.
Case report
A 43-year-old female with abdominal pain was
referred to Xiangya Hospital (Changsha, Hunan, China) and underwent
abdominal CTA with a suspected diagnosis of an abdominal aortic
dissecting aneurysm. A right ovarian tumor was found, and no
dissecting abdominal aortic aneurysm was detected.
The patient’s history included three viable
pregnancies, regular menstrual cycles and no history of vaginal
bleeding. For the past seven years she had experienced sustained
hypertension, with the highest blood pressure recorded being
200/100 mmHg. The patient had not taken any medication to treat the
hypertension until one month prior to the present hospital visit
for abdominal pain. No headache, syncope or palpitations were
indicated.
Upon physical examination, the patient has a body
temperature of 36.4°C (normal range, 36.3–37.2°C), with a heart
rate of 106 beats/min (normal range, 60–100 beats/min), a
respiratory rate of 20 breaths/min (normal range, 12–20
breaths/min) and a blood pressure of 167/114 mmHg (normal range,
60–90/90–114 mmHg). The gynecological examination indicated a
normal uterus and cervix, and no significant mass was palpable.
Abdominal CTA showed a well-defined 5.2×5.7×4.0-cm tumor in close
proximity to the right ovary (Fig.
1A–D). The tumor was highly vascularized and obtained its blood
supply from the right ovarian artery. There was no evidence of
hydronephrosis or retroperitoneal lymph node enlargement.
Laboratory results indicated a significantly elevated total urinary
vanillylmandelic acid (VMA) of 111.8 μmol/24 h (normal VMA,
<68.6 μmol/24 h). The patient was thus diagnosed with ovarian
extra-adrenal pheochromocytoma.
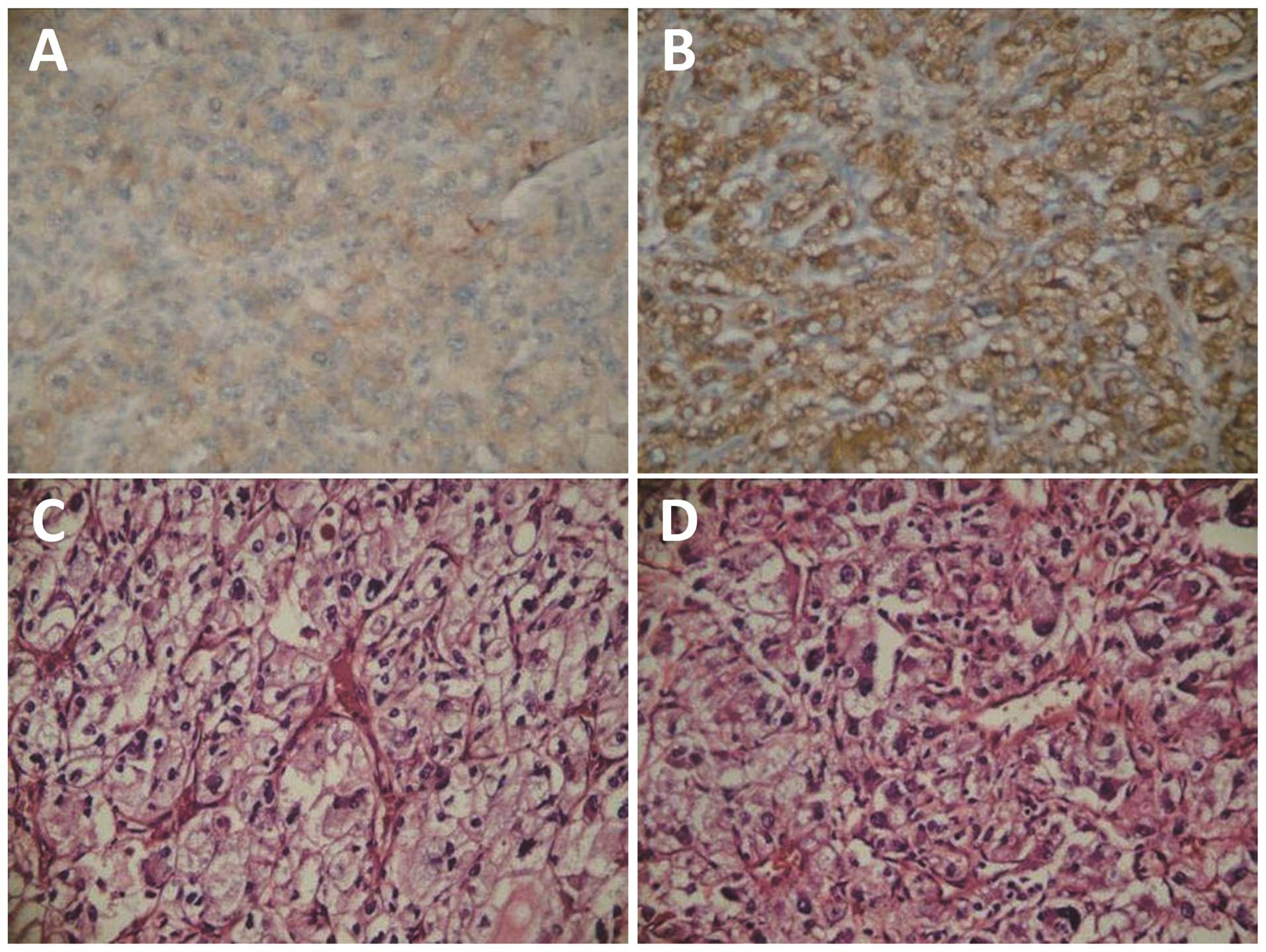
Surgical resection of a 5×5×6-cm mass located
superior to the right ovary was performed. Immunohistochemically,
the tumor cells were positive for chromogranin A, neuron-specific
enolase and synaptophysin (Fig. 2),
and the definitive diagnosis was made upon examination of this
staining. Following surgery, the patient’s blood pressure
stabilized to 115/95 mmHg, with no significant fluctuations, and
abdominal pain was no longer experienced.
Discussion
The majority of extra-adrenal pheochromocytomas are
located in the uterus, retroperitoneum, lumbar spine, bladder,
ocular orbit, heart and mediastinum (4–8). To
the best of our knowledge, the present study is only the second
reported case of an ovarian extra-adrenal pheochromocytoma in the
literature. Montemurro et al (3) reported a case of an ovarian
extra-adrenal pheochromocytoma removed via laparoscopic surgery,
but there have been no studies describing the CTA manifestations in
the ovary. Apart from the extremely rare location of the
pheochromocytoma, the present case is significant due to its
asymptomatic course and characteristic radiological features.
Extra-adrenal pheochromocytomas are divided into two
categories, namely, functional and non-functional tumors. The
clinical manifestations of the former are similar to those of
adrenomedullary pheochromocytomas. In functional tumors, increased
catecholamine secretion is responsible for symptoms such as
hypertension, sweating, headache, diaphoresis, anxiety, tachycardia
and/or palpitations (9). In
addition, the majority of patients with abdominal paragangliomas
exhibit abdominal pain or a palpable abdominal mass (10); however, atypical symptoms may also
be present. In the current study, the patient presented with
abdominal pain similar to that associated with aortic dissection
and persistent hypertension. The significantly increased secretion
of catecholamine causes the abdominal aorta to contract, leading to
abdominal pain. CTA was able to show the tumor site, borders, size
and blood supply, which assisted in guiding the surgical plan.
Although rare, the possibility of pheochromocytoma
should be included in the differential diagnosis of ovarian tumors,
particularly in females with hypertension. Further examinations,
such as tests for hematuria VMA, are necessary. Surgical resection
is the only treatment option for extra-adrenal pheochromocytomas
(11,12). Gynecologists should consider the
possibility of an extra-adrenal pheochromocytoma prior to preparing
to surgically remove a pelvic mass.
It can be difficult to observe any histological
distinction between benign and malignant cases, and therefore
predict malignant potential, due to the variable and non-specific
clinical presentation and imaging data of these patients. Local
recurrence or distant metastases are common. The establishment of
an effective diagnosis, management strategy and follow-up regime is
vital and requires a multidisciplinary approach involving
collaboration between geneticists, endocrinologists,
anesthesiologists, surgeons, laboratory specialists, oncologists,
radiologists and pathologists.
In conclusion, although ovarian paragangliomas occur
infrequently, it is important that they are recognized as a
potential cause of an abdominal mass. Clinical and imaging data of
patients with extra-adrenal, intra-abdominal paragangliomas are
inconsistent. These tumors can even be asymptomatic, as shown in
the present case. Therefore, it is essential that a comprehensive
histological and immunohistochemical evaluation is performed as the
only safe modality for diagnosis. Since these tumors can localize
to the ovary and are difficult to definitively diagnose
pre-operatively, gynecologists and radiologists should consider the
possibility of an extra-adrenal pheochromocytoma prior to preparing
to surgically remove a pelvic mass.
References
|
1
|
Sheps SG, Jiang NS, Klee GG and van
Heerden JA: Recent developments in the diagnosis and treatment of
pheochromocytoma. Mayo Clin Proc. 65:88–95. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Elder EE, Elder G and Larsson C:
Pheochromocytoma and functional paraganglioma syndrome: no longer
the 10% tumor. J Surg Oncol. 89:193–201. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Montemurro S, Ruggieri E, Maselli E, Zito
AF, Chiumarulo F and Gargano G: A rare case of extra-adrenal
pheochromocytoma masquerading as an ovarian mass treated by
laparoscopic surgery. Eur J Gynaecol Oncol. 28:491–496. 2007.
|
|
4
|
Tavassoli FA: Melanotic paraganglioma of
the uterus. Cancer. 58:942–948. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Miraldi F, Taffon C, Toscano M and
Barretta A: Black cardiac paraganglioma in a multiple paraganglioma
syndrome. Eur J Cardiothorac Surg. 32:940–942. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tsai CC, Wu WJ, Chueh KS, et al:
Paraganglioma of the urinary bladder first presented by bladder
bloody tamponade: two case reports and review of the literatures.
Kaohsiung J Med Sci. 27:108–113. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Paulus W, Jellinger K and Brenner H:
Melanotic paraganglioma of the orbit: a case report. Acta
Neuropathol. 79:340–346. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hofmann WJ, Wöckel W, Thetter O and Otto
HF: Melanotic paraganglioma of the posterior mediastinum. Virchows
Arch. 425:641–646. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hayes WS, Davidson AJ, Grimley PM and
Hartman DS: Extraadrenal retroperitoneal paraganglioma: clinical,
pathologic, and CT findings. AJR Am J Roentgenol. 155:1247–1250.
1990. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sclafani LM, Woodruff JM and Brennan MF:
Extraadrenal retroperitoneal paragangliomas: natural history and
response to treatment. Surgery. 108:1124–1130. 1990.PubMed/NCBI
|
|
11
|
Nozaki T, Iida H, Morii A, Fujiuchi Y,
Okumura A and Fuse H: Laparoscopic resection of adrenal and
extra-adrenal pheochromocytoma. J Endourol. 27:862–868. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bruynzeel H, Feelders RA, Groenland TH, et
al: Risk factors for hemodynamic instability during surgery for
pheochromocytoma. J Clin Endocrinol Metab. 95:678–685. 2010.
View Article : Google Scholar
|