Introduction
Breast cancer is the most prevalent and leading
cause of mortality among females worldwide. Through epidemiological
studies, it has been found that family history is one of the major
risk factors that increases susceptibility to breast cancer.
Approximately 5–10% of breast cancers have a hereditary component
(1), and inherited mutations in
high penetrance genes, such as BRCA1 and BRCA2 (2), closely correlate with an increased
risk of females of different ethnic and age groups developing
breast and/or ovarian cancer (1).
In addition, such mutations in the germline increase the
susceptibility to develop cancer of the colon, prostate, pancreas
and melanoma (2). It is evident
that these mutations are involved in a small fraction of all
cancers detected and the presence of sequence alterations in the
BRCA genes has significant clinical relevance.
Mutations in the BRCA1 and BRCA2 genes are
transmitted from one generation to the next by an autosomal
dominant (3). The germline
mutations are usually point mutations (4) and are commonly frameshift small
insertions or deletions, non-sense mutations, or mutations
affecting the splicing sites (2).
The majority of these mutations identified in familial breast
cancer result in the partial or complete deletion of exons or
intronic sequence inserts, which may ultimately yield
non-functional, truncated BRCA1 and BRCA2 proteins (2). Approximately 50% of these mutations
are located within exon 11 of BRCA1 and BRCA2 (5). Females who carry mutations in the
BRCA1 gene have an 80% chance of developing breast cancer during
their lifetime, and a 65% chance of developing a second breast
cancer prior to the age of 70 years. Similarly, females with BRCA2
mutations have an 85% chance of developing breast cancer (6).
BRCA1 and BRCA2 are structurally similar and of
similar size (100 and 70 Kb, respectively) (4). The two genes are considered to be
tumor suppressor genes. BRCA1 is located on chromosome 17 at the
q21 position and consists of 22 exons (60% of the gene
corresponding to exon 11) that encode a protein of 1,863 amino
acids (7,8). Due to its large size, exon 11 is the
main target for mutation detection. BRCA2 is located on chromosome
13 at the 12q position and consists of 27 exons that encode a
protein of 3,418 amino acids (9,10).
Functionally, BRCA1 and BRCA2 are involved in a
multitude of cellular processes, such as transcriptional regulation
in response to DNA damage, maintenance of chromosomal stability and
the regulation of genes involved in the cell cycle and apoptosis
(11).
In total, >600 mutations have been described in
BRCA1, while 450 mutations have been described in BRCA2 (6). Approximately 50% of the unique
variants detected in BRCA1 and BRCA2, regardless of the
polymorphisms, are variants with unknown pathogenic potential and
are thus termed unclassified variants (2). It is also possible to identify
variants of unknown significance. These are variations in the gene
sequence which have not been identified to affect the function of
the protein. It is possible that polymorphisms of the two genes may
result in loss of protein function and thereby increase the risk of
cancer; however, the polymorphisms may also exist without risk
(12).
The aim of this study was to differentiate between
harmless deleterious mutations and polymorphisms in the BRCA1 gene
of 154 females with breast cancer in the city of Bahía Blanca in
Argentina, as well as cities in close proximity to Bahía Blanca. To
the best of our knowledge, this is the first study in Argentina to
detect variations in the BRCA1 gene.
Materials and methods
Study approval
The study was approved by the research ethics
committees of the South Regional Italian Hospital (Bahía Blanca,
Argentina), FEMALE Medical Institute MEDIFEM (Bahía Blanca,
Argentina), Lavalle Institute of Diagnostics (Bahía Blanca,
Argentina), Dr Leonidas Lucero’s Hospital (Bahía Blanca,
Argentina), Viedma Clinic (Viedma, Argentina), Lucio Molas’s
Hospital (Santa Rosa, Argentina) and Pigue Municipal’s Hospital
(Pigue, Argentina), and written informed consent was provided by
all patients prior to voluntarily participating in this study.
Sampling
For this study, 154 female patients (age range,
38–67 years), with breast cancer at any stage of disease, with or
without familial breast cancer history, and with or without cancer
treatment, but had undergone breast surgery were included. From
each patient, buccal mucosa cells were obtained from the patients
via a cheek swab performed by the doctors responsible for the study
in their respective hospitals. Samples were collected in duplicate
for analysis. To avoid inadequate samples, the patients were
required to fast for 6–8 h, have good oral hygiene and to rinse the
mouth several times with water prior to sampling. In addition, the
administration of drugs prior to sampling was prohibited, to
prevent interference with the subsequent analysis. The doctor who
performed the sampling used two swabs simultaneously to achieve a
duplicate sample. The sterile swabs (Cole-Parmer, Vernon Hills, IL,
USA) were removed from their packaging and rubbed firmly and
several times on the bilateral buccal mucosa of the patient. The
swabs were then air-dried for 15 min, and sent to the laboratory
(Breast Cancer Research Laboratory, CERZOS-CONICET, Bahía Blanca,
Argentina)within 24 h. The buccal swab samples were kept dry and
protected from light at room temperature. The first swab was used
for the isolation of DNA, while the second swab was kept in the
aforementioned conditions for later use if required.
Extraction of the genomic DNA
DNA was extracted from the buccal mucosa cells using
a commercial kit for genomic DNA isolation (Nexttec™ 1-step DNA
Isolation; Nextec Applications, Inc., Greenwich, CT, USA). The
commercial kit included all the reagents required for the lysis of
the cells and purification of the DNA. The aim of the protocol was
to retain the proteins, detergents and components of low molecular
weight on the resin column, allowing the passage of the DNA through
the column. The DNA extracted from the buccal swab samples was
preserved in a freezer at −20°C.
Quality control and semi-quantitation of
DNA
The concentration and quality of the DNA obtained
using the isolation kit purchased from Nextec Applications, Inc.
was analyzed by gel electrophoresis in 1.5% agarose at 80 V for 2
h. Subsequently, the gel was stained with ethidium bromide and the
bands were displayed on an ultraviolet transilluminator
(FOTO/UV® 21 FOTODYNE 312 nm DNA transilluminators;
Fotodyne Incorporated, Hartland, WI, USA). A molecular weight
marker was used in each run. The isolated DNA concentration was
determined by comparing the fluorescence intensity between the
weight marker of a known concentration and DNA bands of unknown
concentration. The integrity of the bands was the parameter used to
evaluate the quality of the isolated DNA.
Selection of primers and nucleotide
sequence
The single-strand conformational polymorphism (SSCP)
technique was employed to analyze exons 2, 3, 5, 20 and 11 of the
BRCA1 gene. Considering the large size of exon 11, and in order to
analyze it in its entirety, the exon was divided into 12
overlapping fragments. The primers were selected according to a
previous study in the Brazilian literature investigating the
frequency of mutations in these regions of the BRCA1 gene in
females of the Latino population (6).
Fragment amplification by polymerase
chain reaction (PCR)
Each PCR was performed using 50 ng of DNA, 1X PCR
Buffer with 1.5 mM MgCl2 (Amersham Biosciences,
Piscataway, NJ, USA), 200 μM dNTPs (Amersham Biosciences), 10 μM of
each primer (see Table I) and 1
unit of Taq DNA polymerase (Amersham Biosciences) in a final volume
of 12.5 μl. The PCR protocol used was the same for each amplified
gene region with the exception of the annealing temperature, which
was specified by each primer pair. The amplification conditions
were as follows: Initial denaturalization for 5 min at 96°C; 35
cycles of 30 sec at 96°C and 30 sec at the annealing temperature
(annealing) of each pair of primers; 1 min for elongation at 72°C;
and a final extension for 10 min at 72°C. The samples were
maintained at 4°C until removal from the thermocycler.
 | Table IBRCA1 gene primer nucleotide sequences
for single-strand conformational polymorphism analysis. |
Table I
BRCA1 gene primer nucleotide sequences
for single-strand conformational polymorphism analysis.
| Exon no. | Nucleotide
sequence | Annealing
temperature, °C |
|---|
| 2 | F: GAA GTT GTC ATT
TTA TAA ACC TTT | 57 |
| R: TGT CTT TTC TTC
CCT AGT ATG T | 57 |
| 3 | F: TCC TGA CAG AGC
AGA CAT TTA | 53 |
| R: TTG GAT TTT CGT
TCT CAC TTA | 53 |
| 5 | F: CTC TTA AGG GCA
GTT GTC AG | 58 |
| R: TTC CTA CTG TGG
TTG CTT CC | 58 |
| 20 | F: ATA TGA CGT GTC
TGC TCC AC | 57 |
| R: GGG AAT CCA AAT
TAC ACA GC | 57 |
| 11.1 | F: CCA AGG TGT ATG
AAG TAT GT | 57 |
| R: GAT CAG CAT TCA
GAT CTA CC | 57 |
| 11.2 | F: CTC ACT AAA GAC
AGA ATG | 56 |
| R: CTT TCT GAA TGC
TGC TAT | 56 |
| 11.3 | F: CAG AAA CTG CCA
TGC TTC AGA | 56 |
| R: AGG CTT GCC TTC
TTC CGA TA | 56 |
| 11.4 | F: GTT CAC TCC AAA
TCA GTA GAG AG | 56 |
| R: CAG CTT TGC TTT
TGA AGG CAG | 56 |
| 11.5 | F: CCT AAC CCA ATA
GAA TCA CTC G | 56 |
| R: GAA CCA GGT GCA
TTT GTT AAC TTC | 56 |
| 11.6 | F: CAG CGA TAC TTT
CCC AGA GC | 56 |
| R: GTC CCT TGG GGT
TTT CAA A | 56 |
| 11.7 | F: CTG GAA GTT AGC
ACT CTA GG | 56 |
| R: GTT GCA CAT TCC
TCT TCT GC | 56 |
| 11.8 | F: CCG TTT TCA AAT
CCA GGA AA | 56 |
| R: TGA TGG GAA AAA
GTG GTG GT | 56 |
| 11.9 | F: GAG GCA ACG AAA
CTG GAC TCA | 56 |
| R: CTC AGG TTG CAA
AAC CCC TA | 56 |
| 11.10 | F: AAC AGA GGG CCA
AAA TTG AA | 56 |
| R: GGG TGA AAG GGC
TAG GAC TC | 56 |
| 11.11 | F: AAA GCG TCC AGA
AAG GAG AGC | 56 |
| R: GCC TTT GCC AAT
ATT ACC TGG | 56 |
| 11.12 | F: CAT TGA AGA ATA
GCT TAA ATG | 56 |
| R: CCT GGT TCC AAT
ACC TAA GTT | 56 |
SSCP fragment separation in denaturing
polyacrylamide gel
The PCR products were diluted 3:1 in 3X Loading
buffer (0.5 M EDTA, 95% formamide and 0.05% bromophenol blue;
Promega Corporation, Madison, WI, USA). The PCR products denatured
at 98°C for 10 min and immediately placed on ice to allow the
fragments of ssDNA to fold into three-dimensional structures as a
result of intrastrand base pairing. The gel running conditions were
as follows: 700 V and 17 Watt for 11 h at room temperature. To
visualize the resulting band pattern of the electrophoretic run,
the gel was stained with silver nitrate and revealed with sodium
carbonate.
Polymorphism confirmation
All polymorphisms detected in the acrylamide gel
were confirmed by repeating the PCR reaction, subsequently
employing the genetic material isolated from the preserved second
swab. Next, the reaction was repeated using DNA obtained from the
peripheral blood of each patient to sequence and determine the type
of mutation existing in the polymorphic region.
Sequencing of the polymorphism SSCP
products
The PCR products with abnormal bands (polymorphisms)
in the electrophoretic pattern of the SSCP were sent to Ruralex
Fagos (Buenos Aires, Argentina) for sequencing. The sequencing was
performed using the dideoxy method using the terminal chain method
and Big Dye® technology (Applied Biosystems, Foster
City, CA, USA). The primers used for sequencing were the same as
those used for the PCR reaction. The cycling conditions were as
follows: 96°C for 5 min; 35 cycles of 30 sec at 94°C, 30 sec at
51°C and 4 min at 60°C; followed by a cycle of 10 min at 60°C. The
amplification products were purified using a protocol based on
MgCl2/ethanol and run on an ABI 310 genetic analyzer
(Applied Biosystems). The results were analyzed using ABI
PRISM® 3100-Avant and 3100 Data Collection v2.0 software
(Applied Biosystems).
Results
Analysis was performed on a total of 154 DNA samples
obtained from females with breast cancer, with or without a family
history. Exons 2, 3, 5, 20 and 11 (including the 11.1 to 11.12
regions) of the BRCA1 gene were analyzed. These exons were selected
as several studies have shown increased mutagenic frequency in
these regions (13–18). Following sampling of the buccal
mucosa and subsequent extraction of the DNA as previously
described, the SSCP technique was performed based on the separation
of the DNA fragments according to their three dimensional
conformation in non-denaturing polyacrylamide gels. The DNA of an
individual without breast or ovarian cancer was used to identify
the altered electrophoretic pattern in patients with cancer. In the
full analysis, 21 possible polymorphisms were detected; one in exon
2, four in exon 20, two in exon 11.1, four in exon 11.3, two in
exon 11.5, one in exon 11.7, two in exon 11.8, one in exon 11.10,
one in exon 11.11 and three in exon 11.12 (Fig. 1, Table
II). Overall, 76.20% of the altered electrophoretic activity
was identified within exon 11, as predicted given its large size.
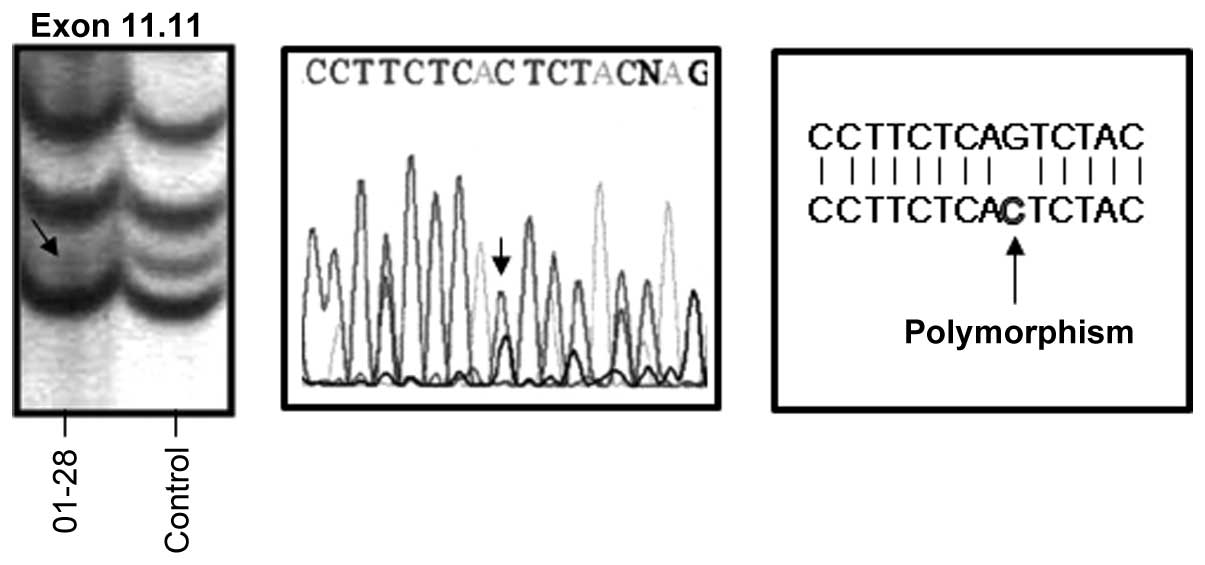
Of these possible polymorphisms, three were confirmed by performing
the full analysis process using the second preserved swab.
Subsequently, peripheral blood was extracted from the patients
whose results had shown an altered electrophoretic pattern. The DNA
was extracted and the samples were sent for sequencing. The samples
were sequenced and two indeterminate results were obtained; one a
missense mutation of a G to C change at position 3,674
corresponding to exon 11.11 of the BRCA1 gene (Fig. 2).
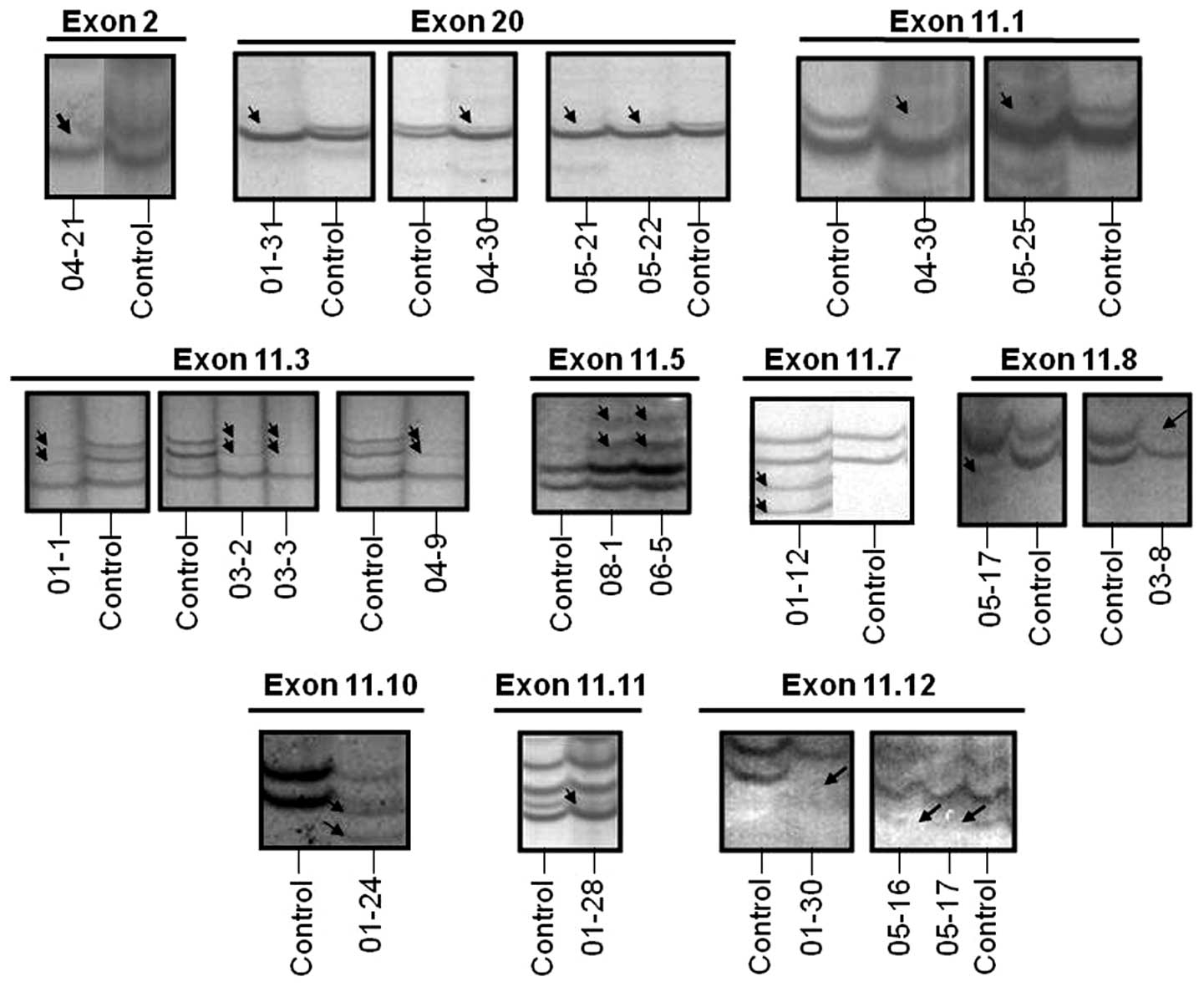 | Figure 1BRCA1 gene polymorphisms detected in
21 out of 154 breast cancer patients using the SSCP method. Images
of the SSCP products run in the polyacrylamide non-denaturing gel
and developed with silver nitrate. BRCA1 polymorphisms were
identified in the following exons of the breast cancer patients
(identification number indicated in the figure): 2, 20, 11.1, 11.3,
11.5, 11.7, 11.8, 11.10, 11.11 and 11.12. In each gel, the control
column was run in parallel with the sample, corresponding to a
normal healthy patient without breast cancer. SSCP, single-strand
conformational polymorphism. |
| Table IIPrevalence of BRCA1 gene polymorphisms
detected in 154 breast cancer patients from the south region of
Argentina. |
Table II
Prevalence of BRCA1 gene polymorphisms
detected in 154 breast cancer patients from the south region of
Argentina.
| Polymorphisms
detected |
|---|
|
|
|---|
| Exon no. | Patients with
alterations, n | General prevalence,
% |
|---|
| 2 | 1 | 0.69 |
| 20 | 4 | 2.76 |
| 11.1 | 2 | 1.38 |
| 11.3 | 4 | 2.76 |
| 11.5 | 2 | 1.38 |
| 11.7 | 1 | 0.69 |
| 11.8 | 2 | 1.38 |
| 11.10 | 1 | 0.69 |
| 11.11 | 1 | 0.69 |
| 11.12 | 3 | 2.07 |
| Total | 21 | 14.49 |
Discussion
It has been reported that ~0.1% of the population
possess a total of 5,000 different BRCA gene mutations (19). Collaboration among medical
professionals and researchers is required to gain increased
knowledge concerning the mutational spectrum and ethnic
distribution of the different mutations (1). It is also important to establish the
pattern of breast cancer risk in the population associated with a
given mutation. This may clarify the mechanism responsible and
allow the proper precautions to be taken (14).
It is important to identify females at high risk of
developing breast cancer. Inheriting a deleterious BRCA mutation is
one of the most important predictors of individual risk (15). Only 10% of all breast cancers are
hereditary and, as previously described, <1% of the population
carry BRCA gene mutations. BRCA mutations are associated with a
relative increase of 2.7–6.4 times the risk of breast cancer, as
well as an increased risk of ovarian cancer of 9.3–35.3 times the
average risk. Females who carry a deleterious mutation in the BRCA
genes may be offered chemoprevention, such as early surveillance
and prophylactic surgery. Health professionals should increase
patient understanding of the risk of mutations in the BRCA genes.
It is also important to promote public policies through adherence
of the female population to preventive strategies, thus reducing
the morbidity and mortality associated with hereditary cancers
(20).
As previously described, being a carrier of a BRCA
gene mutation is associated with an increased risk of certain types
of cancer, particularly breast and ovarian cancer. However,
individuals with a family history of BRCA mutations may not carry
the mutation and a negative result may be misleading. Therefore, in
this study, patients suffering from cancer were employed as the
priority group, as these patients have an increased chance of
having a BRCA1 gene alteration than healthy females without breast
cancer. Although the results of genetic analysis may be normal or
without alterations, the patient may have mutations in other
regions of the gene which were not analyzed or in other genes
associated with the BRCA genes. Notably, the presence of mutations
in the BRCA genes in females with primary breast cancer indicates a
higher chance of developing a second cancer in another organ,
bilateral breast cancer or recurrence of the cancer in the same
breast. In addition, healthy relatives may also carry the same
genetic alteration in the BRCA1 gene and, therefore, have a
significantly higher risk of developing the disease than the
general population.
A recent study has yielded encouraging results on
the development of a test gene expression profile from the
peripheral blood for the early detection of breast cancer with a
prediction accuracy of 79.5%, sensitivity of 80.6% and specificity
of 78.3% (21).
It is extremely important to perform genetic
analysis for BRCA mutations in patients at a high risk of
developing breast cancer in Argentina to aid health professionals
in addressing the prevention, treatment and prognosis of the
disease (1,4). However, such studies have been limited
to a small sample size in BRCA1 mutation analysis and, therefore,
the current study performed this screening with a large sample size
of 154 patients.
The social impact of this study could be important
as, to the best of our knowledge, similar studies have not be
performed in Argentina. The majority of the studies conducted in
different countries differ in their results for the pathological
features of patients with breast cancer associated with the type of
BRCA1 gene mutation. However, these tumors tend to be of high
grade, and less frequently express the estrogen receptor (ER) or
progesterone receptor (PR), which have been associated with a poor
prognosis in sporadic tumors. The aim of the present study was to
determine whether there is a correlation between the type of
alteration found in BRCA1 and the histological subtype, which may
also be useful for determining the association between the
expression of hormone receptors, such as ER, PR and HER2, that were
analyzed in all patients included in this study. In addition, this
study is important to report the genetic variations in Argentinian
females and to examine similarities with the world population.
The social impact of this project may also be
important for the prevention and early diagnosis of breast cancer,
which are essential to patients carrying mutations in the BRCA 1/2
gene, to select the best and most appropriate method of prevention
for the development of breast cancer, including prophylactic breast
surgery or risk reduction strategies. It is also important to note
that a healthy person possessing a mutation may not develop the
disease, but is at a higher risk of developing breast cancer. At
present, the use of prophylactic surgery in Argentina is unlikely
as the family history of alterations in the BRCA 1 and 2 genes
remain unknown. We consider it essential that proper and adequate
explanations are provided to BRCA gene mutation carriers with
regard to the risk of cancer to facilitate the testing of relatives
for genetic alterations and identification of BRCA1 mutation
carriers, and subsequently, with the aid of professionals, to
select the most appropriate preventive option.
In conclusion, the current study identified 21
polymorphisms in the 154 patients analyzed (14.49%). One patient
was identified with a polymorphism in exon 2 (0.69%), four in exon
20 (2.76%), two in exon 11.1 (1.38%), four in exon 11.3 (2.76%),
two in exon 11.5 (1.38%), one in exon 11.7 (0.69%), two in exon
11.8 (1.38%), one in exon 11.10 (0.69%), one in exon 11.11 (0.69%)
and three in exon 11.12 (2.07%). Polymorphisms are verified by
sequencing to determine the type of mutation that characterizes
them. The most prevalent polymorphisms of the BRAC1 gene in
Argentinian patients were located in exon 11 (16 out of the 21
patients; 76.20%; Table II). The
objective of our next study is to evaluate the genetic
susceptibility of healthy patients, as well as relatives of
BRCA1-positive patients in Argentina, and to analyze 20 regions of
the BRCA2 gene.
References
|
1
|
Farooq A, Naveed AK, Azeem Z and Ahmad T:
Breast and ovarian cancer risk due to prevalence of BRCA1 and BRCA2
variants in Pakistani population: A Pakistani database report. J
Oncol. 2011:6328702011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
van der Groep P, van der Wall E and van
Diest PJ: Pathology of hereditary breast cancer. Cell Oncol
(Dordr). 34:71–88. 2011. View Article : Google Scholar
|
|
3
|
Pruthi S, Gostout BS and Lindor NM:
Identification and management of women with BRCA mutations or
hereditary predisposition for breast and ovarian cancer. Mayo Clin
Proc. 85:1111–1120. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ewald IP, Izetti P, Vargas FR, et al:
Prevalence of the BRCA1 founder mutation c.5266dupin Brazilian
individuals at-risk for the hereditary breast and ovarian cancer
syndrome. Hered Cancer Clin Pract. 9:122011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lim MJ, Foster GJ, Gite S, Ostendorff HP,
Narod S and Rothschild KJ: An ELISA-based high throughput protein
truncation test for inherited breast cancer. Breast Cancer Res.
12:R782010. View
Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dufloth RM, Carvalho S, Heinrich JK,
Shinzato JY, dos Santos CC, Zeferino LC and Schmitt F: Analysis of
BRCA1 and BRCA2 mutations in Brazilian breast cancer patients with
positive family history. Sao Paulo Med J. 123:192–197. 2005.
View Article : Google Scholar
|
|
7
|
Hall JM, Lee MK, Newman B, et al: Linkage
of early-onset familial breast cancer to chromosome 17q21. Science.
250:1684–1689. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Miki Y, Swensen J, Shattuck-Eidens D, et
al: A strong candidate for the breast and ovarian cancer
susceptibility gene BRCA1. Science. 266:66–71. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wooster R, Neuhausen SL, Mangion J, et al:
Localization of a breast cancer susceptibility gene, BRCA2, to
chromosome 13q12–13. Science. 265:2088–2090. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wooster R, Bignell G, Lancaster J, et al:
Identification of the breast cancer susceptibility gene BRCA2.
Nature. 378:789–792. 1995. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yoshida K and Miki Y: Role of BRCA1 and
BRCA2 as regulators of DNA repair, transcription, and cell cycle in
response to DNA damage. Cancer Sci. 95:866–871. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Domchek SM and Greenberg RA: Breast cancer
gene variants: separating the harmful from the harmless. J Clin
Invest. 119:2895–2897. 2009. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hedau S, Jain N, Husain SA, et al: Novel
germline mutations in breast cancer susceptibility genes BRCA1,
BRCA2 and p53 gene in breast cancer patients from India. Breast
Cancer Res Treat. 88:177–186. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yassaee VR, Zeinali S, Harirchi I,
Jarvandi S, Mohagheghi MA, Hornby DP and Dalton A: Novel mutations
in the BRCA1 and BRCA2 genes in Iranian women with early-onset
breast cancer. Breast Cancer Res. 4:R62002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Koumpis C, Dimitrakakis C, Antsaklis A,
Royer R, Zhang S, Narod SA and Kotsopoulos J: Prevalence of BRCA1
and BRCA2 mutations in unselected breast cancer patients from
Greece. Hered Cancer Clin Pract. 9:102011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cierniková S, Tomka M, Sedláková O, et al:
The novel exon 11 mutation of BRCA1 gene in a high-risk family.
Neoplasma. 50:403–407. 2003.PubMed/NCBI
|
|
17
|
Risch HA, McLaughlin JR, Cole DE, et al:
Population BRCA1 and BRCA2 mutation frequencies and cancer
penetrances: a kin-cohort study in Ontario, Canada. J Natl Cancer
Inst. 98:1694–1706. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vorkas PA, Christopoulos K, Kroupis C, et
al: Mutation scanning of exon 20 of the BRCA1 gene by
high-resolution melting curve analysis. Clin Biochem. 43:178–185.
2010. View Article : Google Scholar
|
|
19
|
Paradiso A and Formenti S: Hereditary
breast cancer: clinical features and risk reduction strategies. Ann
Oncol. 22(Suppl 1): i31–i36. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Surbone A: Social and ethical implications
of BRCA testing. Ann Oncol. 22(Suppl 1): i60–i66. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Aarøe J, Lindahl T, Dumeaux V, et al: Gene
expression profiling of peripheral blood cells for early detection
of breast cancer. Breast Cancer Res. 12:R72010. View Article : Google Scholar : PubMed/NCBI
|