Introduction
Spinal schwannomas are usually intradural
extramedullary tumors. As Schwann cells are not typically found in
the parenchyma of the central nervous system (CNS), these tumors
are rarely observed within the spinal cord (1). Intramedullary schwannomas account for
0.3% of intraspinal tumors and 1.1% of intraspinal schwannomas
(2,3). Definitive preoperative differentiation
from other intramedullary tumors based solely on imaging is
impossible, unless there is a predominant extramedullary component
or when the tumor is continuous with a thickened spinal nerve root
(4,5). Since intramedullary schwannomas are
slow growing and benign tumors, gross total resection (GTR) of the
tumors is the primary treatment choice with good outcome (3). Ependymal cysts are ependymal-lined
fluid collections within the CNS, the majority of which are
generally located in the paraventricular white matter of the
frontal and parietal lobes (6).
Intramedullary ependymal cysts are particularly rare, with few
pathologically determined cases to date (7). Although these cysts are completely
independent from the central canal, only 28% of intramedullary
ependymal cysts could be totally resected (7). Thus, complete decompression and
cyst-subarachnoid shunt placement is the optimal treatment, and the
outcome may be favorable (8). In
the literature, only one case has been reported in association with
a filar lipoma in an infant (9).
The present study reports a case of intramedullary schwannoma
coexisting with an ependymal cyst in an adult patient. Written
informed consent for the publication of this study was obtained
from the patient.
Case report
On March 4, 2013, a 35-year-old male was admitted to
Beijing Tiantan Hospital (Beijing, China) with a two-year history
of lower back pain and weakness in the left leg. In addition, the
patient had experienced sphincter dysfunction for two months. The
patient had no history of spinal cord injury or previous back
surgery. Neurological examination revealed the power in the left
leg to be 3/5, as classified by the Medical Research Council
grading system (10). Superficial
sensation in the perineum and left leg was reduced.
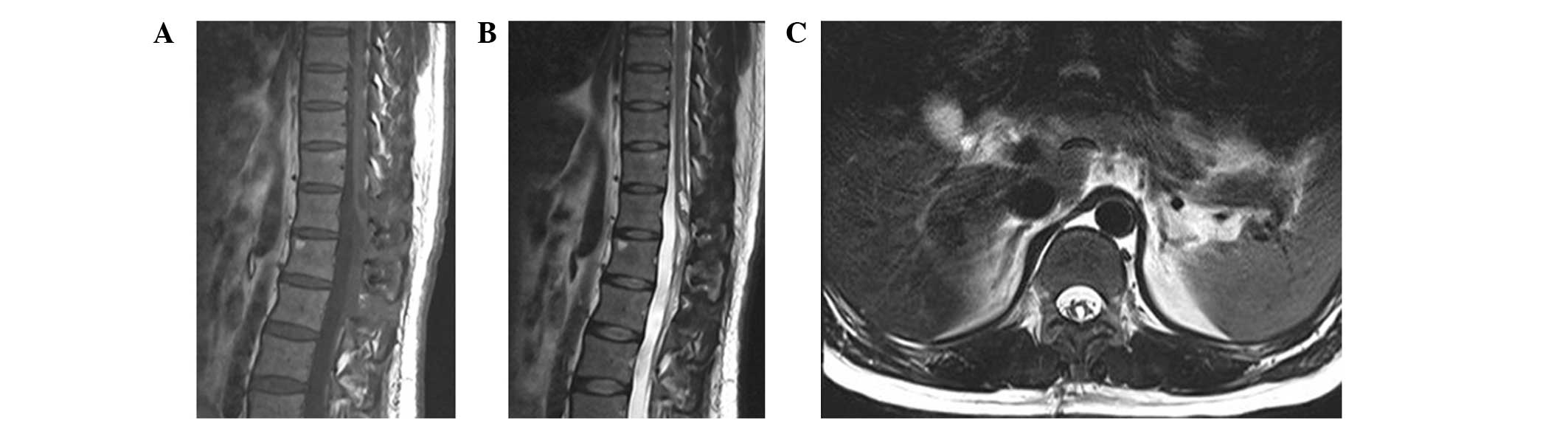
The patient initially underwent pre-operative
magnetic resonance imaging (MRI; Fig.
1). Sagittal T1-weighted images demonstrated an intramedullary
cystic-solid lesion in the conus medullaris; following gadolinium
injection, the solid mass demonstrated inhomogeneous enhancement.
Furthermore, T2-weighted images revealed that the solid mass was
accompanied by a cranial cystic lesion. According to the
pre-operative MRI, a diagnosis of ependymoma with cranial
syringomyelia or cystic degeneration was determined.
The patient underwent a T11-12 laminectomy via the
posterior approach with intraoperative monitoring of somatosensory
and motor-evoked potentials. Intradural exploration revealed a
bulging conus medullaris. Subsequently, classic median myelotomy
was performed in the conus medullaris for intramedullary
exploration. The solid mass was nodular in shape, with a poor blood
supply. The mass was well demarcated from the spinal cord
parenchyma and not attached by any nerve root, which facilitated
its exposure and dissection. Following GTR of the solid mass, the
cranial syringomyelia was examined. A cyst filled with clear fluid
was identified; the cyst was in close proximity to the solid mass,
however, it was separated by neural tissue. The cyst appeared
yellow in color, was filled with clear fluid and did not adhere to
the spinal cord, therefore, a GTR of the cyst was performed.
Pathological examination of the solid mass
identified spindle-shaped cells with features of a schwannoma
(Fig. 2A). Surgical specimens
obtained from the cyst wall were examined and thin ependymal cells
were identified to line the cavity (Fig. 2B). An immunohistochemical
examination revealed that the cells lining the cyst wall were
positive for cytokeratin, glial fibrillary acidic protein and S-100
protein expression (Fig. 2C–E).
In the immediate post-operative period, although the
weakness in the left leg and the sphincter dysfunction did not
improve, the lower back pain disappeared. The patient was
discharged two weeks later; the weakness in the left leg had
improved to grade 5/5 and sphincter dysfunction gradually improved
after three months. No recurrence of the schwannoma or the cyst
were observed on the follow-up MRI (Fig. 3). The present retrospective study
was approved by the Institutional Review Board of Beijing Tiantan
Hospital.
Discussion
Schwannomas and ependymal cysts represent two
distinct disease entities. To the best of our knowledge,
intramedullary ependymal cysts have not previously been reported in
association with schwannomas. Intramedullary schwannomas are
predominantly located in the cervical region, followed by the
thoracic region and the lumbar cord (11,12);
the conus medullaris is rarely involved. According to the location
in the cross-section of the spinal cord, intramedullary schwannomas
can be divided into three types: Central, surfacing and exophytic
(13). In the present case, the
tumor was located exclusively within the spinal cord and, thus, was
classified as a central-type intramedullary schwannoma. A
central-type tumor with no association to the posterior nerve root
is considered to be a congenital neoplasm, which consists of
ectopic Schwann cells originating from the embryonic neural ridge
during closure of the neural tube at the fourth week (13,14).
Pain is always the initial symptom (12), and sensory and motor dysfunction
appear in the late stages of the disease.
Intramedullary schwannomas have no specific imaging
features, and are hypointense or isointense on T1-weighted images
and generally hyperintense on T2-weighted images. Furthermore,
heterogeneous enhancement and well-defined margins of the tumor on
T1-weighted images are regarded as characteristic, but not specific
for schwannomas (15,16). Therefore, unless a predominantly
extramedullary component or nerve root thickening is observed, a
definitive pre-operative diagnosis of intramedullary schwannoma is
difficult to determine based solely on MRI data (4,5).
However, only 50% of intramedullary schwannomas are directly
connected with nerve roots (17).
Hence, performing GTR without sacrificing the nerve roots is
feasible in the majority of intramedullary schwannoma cases.
Subtotal removal is advisable to avoid unacceptable surgical
complications if the tumor exhibits dense adhesion to the neural
tissue. For example, Hida et al (18) described two cases of adherent
intramedullary schwannoma treated with two-stage surgery; the
residual tumor was removed completely, decreasing the morbidity of
the two patients.
Ependymal cysts originate from isolated ependymal
cells of the neuroectoderm, which are cut off from the neural tube
in the developing embryo (9). The
nature of ependymal cysts may cause them to occur anywhere along
the craniospinal axis (19),
however, they are predominantly located in the conus medullaris
(20,21). The etiology of the conus medullaris
predominance remains unclear, although one explanation may be that
the ependymal structure is more often present in the conus
medullaris in the process of embryogenesis (22). Upon pathological examination of the
cyst wall, a continuous lining with a single layer of epithelial
cells and no a basement membrane is observed (23–25).
Intramedullary ependymal cyst is a well-circumscribed, homogeneous
lesion with a smooth margin, the contents of which are isointense
with cerebrospinal fluid on T1- and T2-weighted images and no
enhancement on contrast-enhanced T1-weighted images (8,23–25).
In the present case, the ependymal cyst did not exhibit typical
imaging features, instead demonstrating features similar to
syringomyelia. We hypothesize that the intramedullary schwannoma
altered the configuration of the ependymal cyst. Surgery is the
optimal treatment strategy for symptomatic patients; a range of
surgical treatments have been utilized for ependymal cysts,
including GTR, biopsy, partial resection, marsupialization of the
cyst and cyst-subarachnoid shunts (19–21,23–25).
In the present case, the cyst was totally resected
with a discernible plane between the spinal cord and the cyst wall.
However, this is not always feasible, as the majority of cysts
appear densely adherent to the neural tissue. A review by Park
et al (7) demonstrated that
only 28% of intramedullary ependymal cysts can be totally resected.
Therefore, adequate decompression and communication between the
cyst and subarachnoid space may be necessary (8). Recurrence of ependymal cysts is rare
and neurological function is usually improved by surgical
decompression.
Definitive differentiation from other intramedullary
tumors (such as ependymoma, astrocytoma and hemangioblastoma) based
solely on MRI is not viable pre-operatively. In the present study,
the solid mass did not demonstrate the significant enhancement
observed in hemangioblastoma and it presented with cranial
syringomyelia or cystic degeneration, therefore, a pre-operative
diagnosis of ependymoma was considered. Certain studies have
diagnosed cranial or caudal cystic degeneration as simply
non-neoplastic peritumoral syringomyelia (26,27).
Entering or draining the syringomyelia during the course of
resection should be avoided, as it would collapse following tumor
removal (28). In addition, it has
been reported that syringomyelia resolution is not affected by
whether the syringomyelia cavity is entered (29). However, the present surgery explored
the syringomyelia and identified an independent cyst, which was
subsequently demonstrated to be an ependymal cyst.
In conclusion, the present study reports a rare
condition in which the association between the two different
congenital neoplasms may indicate the presence of dysembryogenesis
as the causative mechanism. Owing to the rarity of concurrent
intramedullary schwannoma and ependymal cysts, as well as a lack of
clinical and imaging characteristics, intramedullary schwannoma is
easily misdiagnosed as ependymoma. Therefore, tumor excision with
exploration of the syringomyelia adjacent to the tumor is the
recommended surgical strategy.
Acknowledgements
The authors would like to thank the patient, and all
of the physicians and staff who participated in the study.
References
|
1
|
Kim SD, Nakagawa H, Mizuno J and Inoue T:
Thoracic subpial intramedullary schwannoma involving a ventral
nerve root: a case report and review of the literature. Surg
Neurol. 63:389–393. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Riffaud L, Morandi X, Massengo S,
Carsin-Nicol B, Heresbach N and Guegan Y: MRI of intramedullary
spinal schwannomas: case report and review of the literature.
Neuroradiology. 42:275–279. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kodama Y, Terae S, Hida K, Chu BC, Kaneko
K and Miyasaka K: Intramedullary schwannoma of the spinal cord:
report of two cases. Neuroradiology. 43:567–571. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Parmar HA, Ibrahim M, Castillo M and
Mukherji SK: Pictorial essay: diverse imaging features of spinal
schwannomas. J Comput Assist Tomogr. 31:329–334. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kono K, Inoue Y, Nakamura H, Shakudo M and
Nakayama K: MR imaging of a case of a dumbbell-shaped spinal
schwannoma with intramedullary and intradural-extramedullary
components. Neuroradiology. 43:864–867. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kumar R, Nayak SR, Krishnani N and Chhabra
DK: Spinal intramedullary ependymal cyst. Report of two cases and
review of the literature. Pediatr Neurosurg. 35:29–34. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Park CH, Hyun SJ, Kim KJ and Kim HJ:
Spinal intramedullary ependymal cysts: a case report and review of
the literature. J Korean Neurosurg Soc. 52:67–70. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yang T, Wu L, Deng X, Yang C, Fang J, Zhao
L, Wang G, Yang J and Xu Y: Clinical characteristics and surgical
outcomes of spinal intramedullary ependymal cysts. Acta Neurochir
(Wien). 156:269–275. 2014. View Article : Google Scholar
|
|
9
|
Balasubramaniam C, Balasubramaniam V and
Santosh V: Intramedullary glioependymal cyst and tethered cord in
an infant. Childs Nerv Syst. 20:496–498. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Compston A: Aids to the investigation of
peripheral nerve injuries. Medical Research Council: Nerve Injuries
Research Committee His Majesty’s Stationery Office: 1942; pp 48
(iii) and 74 figures and 7 diagrams; with aids to the examination
of the peripheral nervous system By Michael O’Brien for the
Guarantors of Brain Saunders Elsevier: 2010; pp[8] 64 and 94
Figures. Brain. 133:2838–2844. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kahilogullari G, Aydin Z, Ayten M, Attar A
and Erdem A: Schwannoma of the conus medullaris. J Clin Neurosci.
12:80–81. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wu L, Yao N, Chen D, Deng X and Xu Y:
Preoperative diagnosis of intramedullary spinal schwannomas. Neurol
Med Chir (Tokyo). 51:630–634. 2011. View Article : Google Scholar
|
|
13
|
Kyoshima K, Horiuchi T, Zenisaka H and
Nakazato F: Thoracic dumbbell intra- and extramedullary schwannoma.
J Clin Neurosci. 12:481–484. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Herregodts P, Vloeberghs M, Schmedding E,
Goossens A, Stadnik T and D’Haens J: Solitary dorsal intramedullary
schwannoma. Case report. J Neurosurg. 74:816–820. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Borges G, Bonilha L, Proa M Jr, Fernandes
YB, Ramina R, Zanardi V and Menezes JR: Imaging features and
treatment of an intradural lumbar cystic schwannoma. Arq
Neuropsiquiatr. 63:681–684. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim NR, Suh YL and Shin HJ: Thoracic
pediatric intramedullary schwannoma: report of a case. Pediatr
Neurosurg. 45:396–401. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Canbay S, Hasturk AE, Markoc F and Caglar
S: Schwannoma of the conus medullaris: a rare case. Chin J Cancer.
30:867–870. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hida K, Yano S and Iwasaki Y: Staged
operation for huge cervical intramedullary schwannoma: report of
two cases. Neurosurgery. 62(Suppl 2): ONS456–ONS460. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Iwahashi H, Kawai S, Watabe Y, Chitoku S,
Akita N, Fuji T and Oda T: Spinal intramedullary ependymal cyst: a
case report. Surg Neurol. 52:357–361. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nagano S, Ijiri K, Kawabata R, Zenmyo M,
Yone K, Kitajima S and Komiya S: Ependymal cyst in the conus
medullaris. J Clin Neurosci. 17:272–273. 2010. View Article : Google Scholar
|
|
21
|
Saito K, Morita A, Shibahara J and Kirino
T: Spinal intramedullary ependymal cyst: a case report and review
of the literature. Acta Neurochir (Wien). 147:443–446. 2005.
View Article : Google Scholar
|
|
22
|
Patankar AP and Sheth JH: Dermoid cyst: A
rare intramedullary inclusion cyst. Asian J Neurosurg. 7:81–83.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chhabra R, Bansal S, Radotra BD and
Mathuriya SN: Recurrent intramedullary cervical ependymal cyst.
Neurol India. 51:111–113. 2003.PubMed/NCBI
|
|
24
|
Kato M, Nakamura H, Suzuki E, Terai H,
Wakasa K, Wakasa T and Takaoka K: Ependymal cyst in the lumbar
spine associated with cauda equina compression. J Clin Neurosci.
15:827–830. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Takci E, Sengul G and Keles M: Spinal
intramedullary ependymal cyst and tethered cord in an adult. Case
report. J Neurosurg Spine. 4:506–508. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fine MJ, Kricheff II, Freed D and Epstein
FJ: Spinal cord ependymomas: MR imaging features. Radiology.
197:655–658. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Goy AM, Pinto RS, Raghavendra BN, Epstein
FJ and Kricheff II: Intramedullary spinal cord tumors: MR imaging,
with emphasis on associated cysts. Radiology. 161:381–386. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Maira G, Amante P, Denaro L, Mangiola A
and Colosimo C: Surgical treatment of cervical intramedullary
spinal cord tumors. Neurol Res. 23:835–842. 2001. View Article : Google Scholar
|
|
29
|
Lonser RR, Weil RJ, Wanebo JE, DeVroom HL
and Oldfield EH: Surgical management of spinal cord
hemangioblastomas in patients with von Hippel-Lindau disease. J
Neurosurg. 98:106–116. 2003. View Article : Google Scholar : PubMed/NCBI
|