Introduction
Extramedullary plasmacytoma (EMP) of the larynx is
an uncommon neoplasm of plasma cells, which is extremely rarely
observed in the cricoid cartilage. A previous study reported that
80–90% EMP cases occur in the head and neck (1), but only three case reports have
described EMP occurring in the cricoid cartilage (2–4). The
typical treatments for this disease are irradiation, surgery, or
irradiation combined with surgery in certain locations such as the
head and neck, with a 50–80% survival rate after 10 years (5). However, the most important factor that
influences the prognosis of the disease is the development to
myeloma (6). The current study
reports one case of EMP, subsequently progressing to multiple
myeloma. The treatment and collection of information for this study
was approved by the ethics committee of West China Hospital,
Sichuan University (Chengdu, China). Written informed consent was
obtained from the patient.
Case report
A 43-year-old male was admitted to the Department of
Otorhinolaryngology of West China Hospital on June 2, 2009,
complaining of hoarseness lasting for over two years and dyspnea
for over one year, which had intensified for a week. An emergency
tracheostomy was performed under local anesthesia. Electronic
laryngoscopy revealed swelling of the arytenoid, vocal cord,
laryngeal ventricle and ventricular band, and also indicated
limited movement of the right vocal cord and subglottic stenosis.
However, no neoplasm was observed in the laryngeal cavity or main
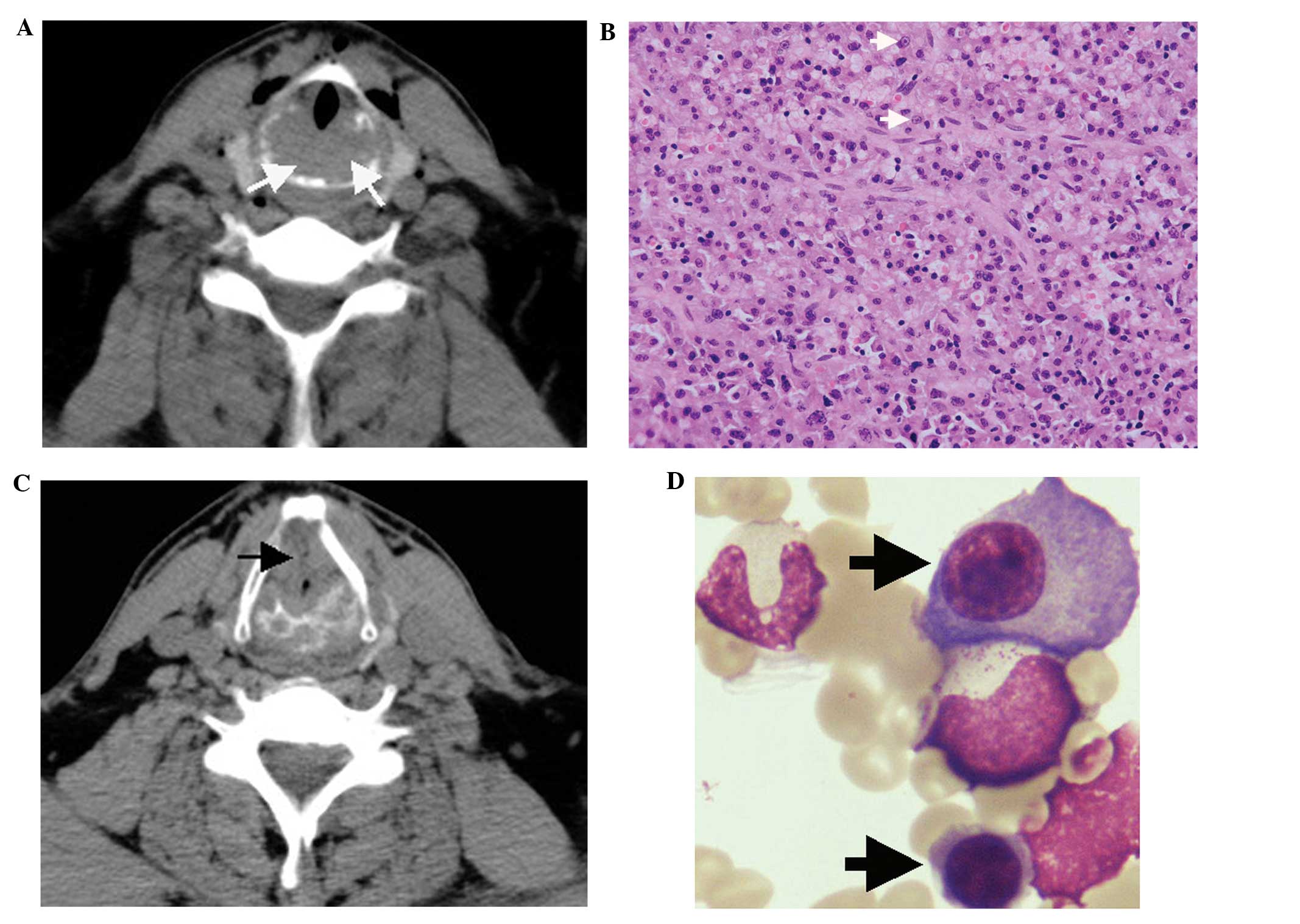
bronchus. Computed tomography (CT) imaging of the neck revealed a
space-occupying lesion of the cricoid cartilage (Fig. 1A), with enlargement of the left
lymph nodes. Three days after hospitalization, the patient
underwent partial laryngectomy, reconstruction of laryngeal
function, and left cervical lymphadenectomy.
Surgery revealed erosion of the posterior and
lateral cricoid cartilage (fish meat-like tissue was observed), and
two swollen lymph nodes in the second left cervical area. The
invaded tissue was completely excised, and the laryngeal cavity was
reconstructed. Histopathological analysis revealed laryngeal
plasmacytoma (Fig. 1B) without
lymph node metastasis. The patient was diagnosed with solitary EMP
of the larynx following positron emission tomography (PET)-CT and
immunofixation electrophoresis. PET-CT revealed no tumors, cancer
or lytic bone metastases and immunofixation electrophoresis did not
reveal monoclonal immunoglobulin. Against medical advice, the
patient refused radiotherapy suggested by the Department of
Oncology, for financial reasons.
One year later, the patient was readmitted after
complaining of dysphonia, and electronic laryngoscopy revealed the
presence of extensive adhesion and stenosis in the subglottic
tissue. CT imaging of the neck showed thickening of the left wall
of the subglottic area, and the cricoid cartilage was broken
(Fig. 1C). Tumor recurrence was
suspected, and therefore a second surgery was performed.
During surgery, an irregular callus was identified
in the middle of the cricoid cartilage, which was causing airway
stenosis. The left side of the cricoid cartilage had been destroyed
by the tumor. Complete resection of the tumor tissue and the left
cricoid cartilage was performed in order to expand the airway. On
histopathological evaluation, the postoperative diagnosis was
determined to be recurrence of solitary plasmacytoma of the larynx.
As previously, against medical advice, the patient refused to
undergo radiotherapy following surgery. Two years and four months
after the second surgery, the patient presented with osseous masses
in the bilateral clavicle, right cheekbone, and ribs, and was
subsequently diagnosed with multiple myeloma based on whole body
radiography, a bone marrow smear showing that plasmocytes accounted
for 15% of the total cells(Fig.
1D), significantly active proliferation shown by the bone
marrow biopsy and immunofixation electrophoresis confirming the
type of λ light chain. The patient received five systematic
chemotherapy, each cycle lasting one month, in the hematology
department, which consisted of the MPT regimen: Melphalan (4 mg,
three times a day, days 1–4), prednisone (45 mg, three times a day,
days 1–4) and thalidomide (100 mg, once a day, days 1–28). The
patient’s general condition stabilized, and no further anemia, bone
pain, infection or other discomfort was experienced. The patient
remains alive after 4 years of follow-up, and follow-up will
continue to screen for recurrence.
Discussion
Solitary plasmacytoma is a rare malignant plasma
cell tumor that is caused by the monoclonal proliferation of plasma
cells, and may be classified as EMP or solitary plasmacytoma of the
bone. According to the National Comprehensive Cancer Network
Guidelines for multiple myeloma (version 1.2013), the patient in
the current case was diagnosed with EMP. EMP is typically observed
in males aged from 40–70 years (7)
and accounts for approximately 3% of plasma cell neoplasms, and
<1% of head and neck tumors (8).
It is three times more common in males than in females (9).
The diagnosis of solitary plasmacytoma of the
cricoid cartilage is predominantly determined using histopathology,
following the exclusion of multiple myeloma (10). The preferred treatment for EMP is
radiotherapy at 45 Gy and/or surgical intervention for the involved
region (9). EMP is highly
radiosensitive, with an 80–100% local control rate following
radical radiotherapy. However, chemotherapy is preferred for cases
involving whole-body dissemination (10). EMP prognosis is associated with the
extent of differentiation; tumors with lower differentiation are
more likely to develop into multiple myeloma (11). Hematoxylin and eosin staining
revealed a low differentiation of tumor cells acquired from our
patient, which was consistent with previous studies (11,12).
Although radiotherapy and surgery are both viable
treatment options for solitary plasmacytoma, complete surgical
resection of the tumors may not be possible in cases involving the
primary cricoid cartilage due to the necessity to preserve larynx
function. In such cases, patients should receive radiotherapy
following surgery (13). Clinicians
must also be alert to signs of progression to multiple myeloma,
such as anemia, bone pain and renal insufficiency, particularly in
cases of relapse.
References
|
1
|
Korolkowa O, Osuch-Wójcikiewicz E, Deptała
A and Suleiman W: Extramedullary plasmacytoma of the head and neck.
Otolaryngol Pol. 58:1009–1012. 2004.(In Polish).
|
|
2
|
Rodriguez-de-Velasquez A, Weber A and
Montgomery W: Extramedullary laryngeal plasmacytoma. Ann Otol
Rhinol Laryngol. 105:483–486. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hall FT, Perez-Ordonez B and Irish J:
Pathology quiz case 1. Multiple myeloma with an extramedullary
plasmacytoma involving the subglottis. Arch Otolaryngol Head Neck
Surg. 130:366–368. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pichi B, Terenzi V, Covello R and Spriano
G: Cricoid-based extramedullary plasmocytoma. J Craniofac Surg.
22:2361–2363. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Straetmans J and Stokroos R:
Extramedullary plasmacytomas in the head and neck region. Eur Arch
Otorhinolaryngol. 265:1417–1423. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ben Salah H, Hdiji S, Makni S, et al:
Extramedullary plasmocytomas. Cancer Radiother. 16:282–287. 2011.
View Article : Google Scholar
|
|
7
|
Kim KS, Yang HS, Park ES and Bae TH:
Solitary Extramedullary Plasmacytoma of the Apex of Arytenoid:
Endoscopic, CT, and Pathologic Findings. Clin Exp Otorhinolaryngol.
5:107–111. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Miller FR, Lavertu P, Wanamaker JR,
Bonafede J and Wood BG: Plasmacytomas of the head and neck.
Otolaryngol Head Neck Surg. 119:614–618. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Anderson KC, Alsina M, Bensinger W, et al:
Multiple myeloma, version 1.2013. J Natl Compr Canc Netw. 11:11–17.
2013.PubMed/NCBI
|
|
10
|
Soutar R, Lucraft H, Jackson G, et al;
Guidelines Working Group of the UK Myeloma Forum; British Committee
for Standards in Haematology; British Society for Haematology.
Guidelines on the diagnosis and management of solitary plasmacytoma
of bone and solitary extramedullary plasmacytoma. Br J Haematol.
124. pp. 717–726. 2004, View Article : Google Scholar
|
|
11
|
Susnerwala SS, Shanks JH, Banerjee SS,
Scarffe JH, Farrington WT and Slevin NJ: Extramedullary
plasmacytoma of the head and the neck region: clinicopathological
correlation in 25 cases. Br J Cancer. 75:921–927. 1997. View Article : Google Scholar
|
|
12
|
Gerry D and Lentsch EJ: Epidemiologic
evidence of superior outcomes for extramedullary plasmacytoma of
the head and neck. Otolaryngol Head Neck Surg. 148:974–981. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tsang RW, Gospodarowicz MK, Pintilie M, et
al: Solitary plasmacytoma treated with radiotherapy: impact of
tumor size on outcome. Int J Radiat Oncol Biol Phys. 50:113–120.
2001. View Article : Google Scholar : PubMed/NCBI
|