Introduction
Mammary ductal ectasia (MDE) (1) is an inflammatory breast disease with the
pathological characteristics of dilation of the major ducts
associated with intraluminal plugs of histiocytes and periductal
inflammation (2). The frequency of
MDE may range from 1.1% to 75%, according to the diagnostic method
used, which might be clinical, histopathological or necropsy-based
(3). MDE typically occurs in females
undergoing menopause, but can also occur in younger females, males
and infants. The disease usually affects mammary ducts that are
large or medium in size, and is one of the most prevalent causes of
bloody nipple discharge and sub-areolar masses, radiologically and
clinically mimicking invasive carcinoma (1,4,5). The treatment of MDE is usually
conservative. Biopsy is often required if the signs and symptoms of
ectasia do not disappear or indicate a tumor. When severe, duct
ectasia may require repeated surgical treatments and occasionally,
mastectomy (3). The etiology and
pathogenesis of MDE have not been defined. One previous study
described an association between the abnormal secretion of
prolactin and MDE (6). The present
study reports a case of bilateral MDE induced by
sulpiride-associated hyperprolactinemia in a young female with
long-term schizophrenia.
Case report
A 32-year-old female presented to Yantai Yuhuangding
Hospital Affiliated to Medical College of Qingdao University
(Yantai, Shandong, China) in 2012 with a 4-year history of a
non-palpable mass in the bilateral breast initially detected by
ultrasound, with mastalgia. The patient described a history of a
small amount of intermittent creamy nipple discharge. The patient's
menarche occurred at a normal age, but with irregular menstrual
periods. The patient married at 26-year-old and had one child,
which had not been breast-fed. The patient had never smoked and did
not have a family history of cancer. A diagnosis of schizophrenia
was made at the age of 26 years, followed by treatment with 0.5 g
sulpiride once a day, 2 mg trihexyphenidyl twice a day and 0.8 mg
alprazolam every night, for six years. A dysembryoma of the ovary
had also previously been removed in Yantai Yuhuangding Hospital
Affiliated to Medical College of Qingdao University.
A physical examination revealed bilateral nipple
retraction and a 1.5×1.0-cm non-tender mass in the upper internal
quadrant of the left breast, with a small amount of nipple
discharge. There was no evidence of axillary lymphadenopathy.
An auxiliary examination revealed a carbohydrate
antigen-125 level of 73.52 U/ml (normal value, 0–35.0 U/ml), a
serum prolactin level of 100.6 ng/ml (normal value, 6.0–29.9 ng/ml)
and a testosterone level of 0.992 ng/ml (normal value, 0.06–0.82
ng/ml), as detected by a Roche Cobas E601 electrochemiluminescence
immunoassay analyzer (Roche Diagnostics GmbH, Mannheim,
Germany).
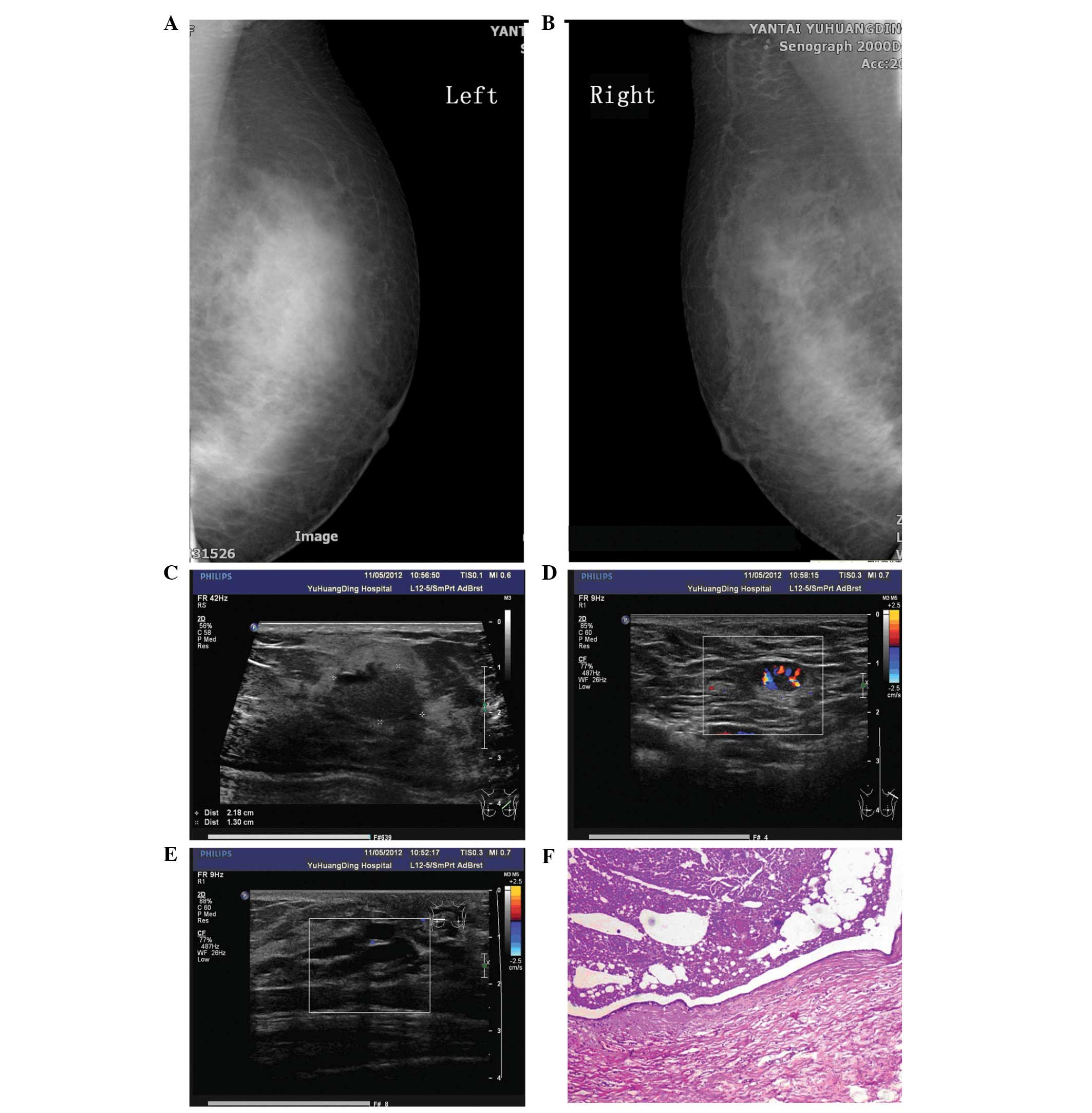
Ultrasound examination performed 4 years previously
revealed several well-defined cysts. A repeat ultrasound performed
following referral to Yantai Yuhuangding Hospital Affiliated to
Medical College of Qingdao University revealed several masses in
the bilateral breasts. The largest mass, measuring 2.2×1.3 cm, was
located in the upper inner quadrant of the left breast, with a
clear boundary and uneven echo. Color Doppler flow imaging revealed
a rich blood flow signal around the nodule. The ducts in the
bilateral breasts exhibited cystic ectasia and a maximum duct size
of 0.8×1.8 cm. Multiple enlarged lymph nodes were found in the
bilateral axillae. The largest node in the right axilla was 1.6×0.8
cm and the largest node in the left axilla was 1.4×0.8 cm. The
nodes exhibited clear boundaries with an uneven echo and had not
fused together (Fig. 1).
Mammography showed thickened breast tissue without
an observable mass, and sand-like calcification in the bilateral
breasts (Breast Imaging-Reporting and Data System classification,
0) (7). The patient refused to
undergo pituitary magnetic resonance imaging. A clinical diagnosis
of mammary duct ectasia and breast tumors in the bilateral breasts
was formed (Fig. 1).
A segmental mastectomy was preformed in November
2012 due to the palpable mass and nipple discharge in the left
breast. Macroscopic examination revealed that the duct exhibited
ectasia, with multiple galactoceles and sebaceous gland cysts
containing white/yellow-colored fluid. The gland was fibrous and
hard. Similar fluid was drained from the peri-areolar ducts once
the lesion had been excised. Histological examination revealed
multiple dilated ducts, the largest measuring 4.5×3.5 cm and
containing eosinophilic material. The duct epithelium was flattened
or lost in places. The breast lobule was atrophic. The interstitial
fibrous tissue and lymphoid exhibited hyperplasia with formation of
lymphoid follicles. A large amount of infiltrative foam cells was
also found. The subsequent pathological diagnosis was of breast
duct dilatation (Fig. 1).
Next, a bacterial culture and drug sensitivity
analysis was performed. The secretions were inoculated into a blood
plate and a Jimmy Kang Kai plate, and then cultured in an incubator
for 24 h at 37°C. If bacterial growth was detected, the colonies
were selected out and tested by a VITEK 2 Compact system
(bioMérieux, Ltd., Marcy l'Etoile, France) for drug sensitivity.
Bacterial culture and drug sensitivity analysis of the secretions
from the cystic cavity revealed no bacterial growth after being
cultured for two days, and an acid-fast bacillus smear test was
negative. The surgical incision was beginning to heal, however,
extravasation of the wound occurred one month later.
Saphylococcus epidermidis was observed using a bacterial
culture. The bacteria were sensitive to moxifloxacin, which was
used for one week for wound healing.
We suggested that the patient should switch to a
prolactin-sparing antipsychotic in view of the hyperprolactinemia.
However, the patient rejected the suggestion. After a clinical
follow-up of 16 months, the wound had healed well and no palpable
mass was found in the breast.
The study protocol was approved by the Human Ethical
Committee of the Yantai Yuhuangding Hospital Affiliated to Medical
College of Qingdao University. Informed consent was obtained from
the patient prior to the surgery and the examination of the
specimens.
Discussion
MDE is an inflammatory breast disease associated
with inflammation and periductal fibrosis of varying degrees
(8). The disease has also been known
as comedomastitis, plasma cell mastitis and cholesterol granuloma.
Duct dilatation is usually asymptomatic in the initial phases
(9). When symptomatic, the most
common clinical presentation is mammary secretion (10). In the majority of cases, no palpable
abnormalities are present, however, in later stages, painful
sub-areolar masses with associated skin retraction occur, which can
be misdiagnosed as infiltrative carcinoma. The diagnosis of MDE is
usually clinical. Mammography usually identifies irregular
thickening of the sub-areolar breast tissue and
microcalcifications, which can mimic a carcinoma (11). Ultrasonography allows the diagnosis
and measurement of duct diameters of >5 mm (12). Ductography usually identifies ductal
dilatation with multifocal luminal obstruction in a beaded pattern,
but is limited as a diagnostic method for MDE (13). Histopathologically, the diagnosis
requires the identification of peri-ductal inflammation.
Circumferential deposits of lymphocytes, plasma cells or foamy
histiocytes are usually found. The initial phase of MDE is
characterized by the presence of dilatation of the duct terminals
(14). Following this, the
inflammatory process is replaced by fibrosis. The approach towards
MDE is usually conservative. Duct ectasia occasionally improves
without treatment or with the use of warm compresses and
antibiotics. Biopsy is usually required if the signs and symptoms
of ectasia do not disappear, and the abnormal duct can be removed
surgically. Surgery is also reserved for cases associated with
suspected malignant abnormalities. Duct excision usually provides
good results for symptomatic duct ectasia. In its most severe form,
duct ectasia may require repeated surgical treatments and
occasionally, mastectomy (9).
Two theories exist with regard to the pathogenesis
of MDE (15). First, the primary
pathological process is believed to be involutional, with atrophy
of the ducts and glands, followed by dilation of the ducts, leading
to the inactivity of secretion, duct rupture and inflammation.
Second, the causative event is proposed to be an inflammatory
process; periductal inflammation being the underlying abnormality,
followed by duct sclerosis, obliteration and ectasia. However, the
etiology of duct ectasia is unknown. Predisposing factors include
squamous metaplasia of the terminal duct epithelium, phenothiazine
treatment, cigarette smoking, bacterial growth and
hyperprolactinemia. Rahal et al (16) suggested that tobacco smoking is a risk
factor for ductal ectasia, while a history of breast-feeding,
hormonal contraceptive use, abortions and breast abscesses has no
association. A study by Dixon et al (17) indicated that smoking is a significant
risk factor for periductal mastitis, but not for duct ectasia. One
previous study hypothesized that duct ectasia may be due to
bacterial contamination by aerobic and anaerobic agents (16). Certain reports have recorded the
presence of bacterial growth in infants (18) and adults (10) with duct ectasia. In the present case,
Staphylococcus epidermidis was observed using a bacterial
culture. However, this was not enough to be believed to be
etiological, and bacterial infection is more likely to be secondary
rather than a primary cause. Another previous study (6) described an association between abnormal
prolactin secretion and MDE. Shousha et al (19) also concluded that an association
existed between certain hypothalamic/pituitary disorders, possibly
associated with prolactin secretion and mammary duct ectasia
development in postmenopausal patients.
Antipsychotic drugs are the foundation of treatment
for schizophrenia, a chronic and debilitating psychotic mental
disorder. All conventional antipsychotic drugs block D2 receptors
on lactotroph cells, thereby removing the main inhibitory effect on
prolactin secretion. With an occurrence rate of 40–50%,
hyperprolactinemia is one of the most common side-effects
associated with antipsychotics. Higher prolactin levels are a
consequence of longer exposure to high-dose antipsychotics, and are
particularly evident during treatment with older antipsychotics or
with risperidone, sulpiride or amisulpride. Hyperprolactinemia may
result in galactorrhea, enlargement of the breasts, ovarian
dysfunction, reduced libido, reduced vaginal lubrication,
dyspareunia, infertility, and atrophic changes in the urethra and
vaginal mucosa. Serum prolactin levels are usually measured in
patients on antipsychotic drugs when the clinical indicators of
galactorrhea, amenorrhea and loss of libido or impotence are
present. By analogy with prolactinoma-induced symptoms, increased
levels of >1,500 mU/l and particularly >3,000 mU/l are likely
to cause symptoms. Decreasing the dose of antipsychotic should be
considered if it is unnecessarily high. Hyperprolactinemia is
rapidly reversed following the discontinuation of amisulpride
treatment (20) or once the patient
has been switched to a prolactin-sparing antipsychotic, such as
quetiapine (21), olanzapine,
ziprasidone or aripiprazole. The addition of the partial agonist
aripiprazole (22), including the use
of dopamine agonists, to the treatment was an alternative approach.
However, thi is associated with a risk of worsening or inducing
psychosis, which would require specialist services. Carmoxirole is
also able to reduce the hyperprolactinemia induced by amisulpride
without altering its main effect (23). However, bromocriptine appears to
destroy the main effect of amisulpride at a dose that reduces
amisulpride-induced hyperprolactinemia, and is therefore not a
suitable treatment (21,24).
In the present case, we hypothesize that there was
an association between sulpiride-induced prolactin secretion and
the development of mammary duct ectasia. First, the patient was
treated with sulpiride in high doses for 6 years, during which,
bilateral creamy nipple discharge was observed. Second, the serum
prolactin level in the patient was extremely high (2,132.72 mU/l).
There have been no reports on the use of trihexyphenidyl or
alprazolam to induce hyperprolactinemia. Third, ultrasonography
revealed multiple ducts that exhibited cystic ectasia in the
bilateral breasts rather than a localized lesion. We believe that
this was the result of the changes in the serum hormone levels.
Fourth, one previous study (6)
described an association between the abnormal secretion of
prolactin and MDE. The possible mechanism behind this is through
the inspissated secretion leading to chronic inflammation, fibrosis
and the persistence of ductal dilatation. Bilateral nipple
retraction is also one of the causes of MDE. The delay in the
development of ectasia can be explained by the fact that the
disease process probably does not start until atrophic changes have
occurred in the breast.
In summary, the present study reports the case of a
long-term schizophrenia patient with a high level of prolactin and
bilateral MDE. We hypothesize that there is an association between
the two conditions, although the specific mechanisms involved
remain unclear. In view of this, certain antipysychotics that have
a lower potential for increasing prolactin levels should be
considered when prescribing an antipsychotic. In the future, larger
studies are required to elucidate the association between these
disorders, so that the risk factors can be identified for
assessment in clinical practice, thereby enabling disease
prevention.
References
|
1
|
McHoney M, Munro F and Mackinlay G:
Mammary duct ectasia in children: report of a shortseries and
review of the literature. Early Hum Dev. 87:527–530. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Haagensen CD: Mammary-duct ectasia; a
disease that may simulate carcinoma. Cancer. 4:749–761. 1951.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Thomas WG, Williamson RC, Davies JD and
Webb AJ: The clinical syndrome of mammary duct ectasia. Br J Surg.
69:423–425. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dogan BE, Ceyhan K, Tukel S, Saylisoy S
and Whitman GJ: Ductal dilatation as the manifesting sign of
invasive ductal carcinoma. J Ultrasound Med. 24:1413–1417.
2005.PubMed/NCBI
|
|
5
|
Duchesne N, Skolnik S and Bilmer S:
Ultrasound appearance of chronic mammary duct ectasia. Can Assoc
Radiol J. 56:297–300. 2005.PubMed/NCBI
|
|
6
|
Peters F and Schuth W: Hyperprolactinemia
and nonpuerperal mastitis (duct ectasia). JAMA. 261:1618–1620.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
D'Orsi C, Mendelson EB, Ikeda D, et al:
Breast Imaging Reporting Data SystemACR BI-RADS - breast imaging
atlas. American College of Radiology; Reston, VA: 2003
|
|
8
|
Leung AK and Kao CP: Mammary duct ectasia:
a cause of bloody nipple discharge. J Natl Med Assoc. 96:543–545.
2004.PubMed/NCBI
|
|
9
|
Browning J, Bigrigg A and Taylor I:
Symptomatic and incidental mammary duct ectasia. J R Soc Med.
79:715–716. 1986.PubMed/NCBI
|
|
10
|
Rahal RM, Junior RF, Reis C, Pimenta FC,
Netto JC and Paulinelli RR: Prevalence of bacteria in the nipple
discharge of patients with duct ectasia. Int J Clin Pract.
59:1045–1050. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sweeney DJ and Wylie EJ: Mammographic
appearances of mammary duct ectasia that mimic carcinoma in a
screening programme. Australas Radiol. 39:18–23. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rizzatto G and Chersevani R:
Breastultrasound and new technologies. Eur J Radiol. 27(Suppl 2):
S242–249. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sakorafas GH: Nipple discharge:
currentdiagnostic and therapeutic approaches. Cancer Treat Rev.
27:275–282. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ying T, Li Q, Xu L, Liu F and Hu B:
Three-dimensional ultrasound appearance of pelvic floor in
nulliparouswomen and pelvic organ prolapse women. Int J Med Sci.
9:894–900. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang Z, Leonard MH Jr..Khamapirad T and
Castro CY: Bilateral extensive ductitis obliterans manifested by
bloody nipple discharge in a patient with long-term diabetes
mellitus. Breast J. 13:599–602. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rahal RM, de Freitas-Júnior R and
Paulinelli RR: Risk factors for duct ectasia. Breast J. 11:262–265.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dixon JM, Ravisekar O, Chetty U and
Anderson TJ: Periductal mastitis and duct ectasia: different
conditions with different aetiologies. Br J Surg. 83:820–822. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kitahara S, Wakabayashi M, Shiba T, Nonaka
K, Nonaka H and Kobayashi I: Mammary duct ectasia in children
presenting bloody nipple discharge: a case in a pubertal girl. J
Pediatr Surg. 36:E22001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shousha S, Backhouse CM, Dawson PM,
Alaghband-Zadeh J and Burn I: Mammary ductectasia and pituitary
adenomas. Am J Surg Pathol. 12:130–133. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Paparrigopoulos T, Liappas J, Tzavellas E,
Mourikis I and Soldatos C: Amisulpride-induced hyperprolactinemia
is reversible following discontinuation. Prog Neuropsychopharmacol
Biol Psychiatry. 31:92–96. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kovács L and Kovács G: Endocrine side
effects among psychiatric patients treated with antipsychotics.
Neuropsychopharmacol Hung. 8:61–66. 2006.[In Hungarian]. PubMed/NCBI
|
|
22
|
Mir A, Shivakumar K, Williamson RJ,
McAllister V, O'Keane V and Aitchison KJ: Change in sexual
dysfunction with aripiprazole: a switching or add-on study. J
Psychopharmacol. 22:244–253. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Marchese G, Ruiu S, Casti P, et al:
Carmoxirole is able to reduce amisulpride-induced
hyperprolactinemia without affecting its central effect. Eur J
Pharmacol. 447:109–114. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bliesener N, Yokusoglu H, Quednow BB,
Klingmüller D and Kühn KU: Usefulness of bromocriptine in the
treatment of amisulpride-induced hyperprolactinemia: a case report.
Pharmacopsychiatry. 37:189–191. 2004. View Article : Google Scholar : PubMed/NCBI
|