Introduction
Gefitinib, an inhibitor of epidermal growth factor
receptor (EGFR) tyrosine kinase, is an effective and well-tolerated
drug used for the treatment of advanced non-small cell lung cancer
(NSCLC) (1,2). However, gefitinib treatment may result
in a number of severe adverse effects, including the development of
interstitial lung disease (ILD) (3–7). Although
certain studies have been conducted on the safety of
re-administering gefitinib to patients who were suspected of
suffering from gefitinib-induced ILD, no precise management
strategy has been established for such cases (8–11). The
present study reports the case of a patient with lung
adenocarcinoma, initially responding to gefitinib treatment.
However, the patient developed gefitinib-induced ILD, which was
treated with low-dose corticosteroids at the early stages of ILD,
and then gefitinib was re-administered along with
N-acetylcysteine.
Case report
A 64 year-old female nonsmoker was diagnosed with
lung adenocarcinoma (T4N2M1b) with
multiple pulmonary and bone metastases in August 2011 at the
Beijing Chao-Yang Hospital (Beijing, China). The patient received
four cycles of chemotherapy with gemcitabine (1400 mg, d1; 1600 mg,
d8) plus cisplatin (40 mg, d2-d3; 30 mg, d4) as the first-line
therapy (21 day cycles, 4 cycles). A brain MRI scan in November
2011 revealed multiple metastases in the patient, indicating
disease progression.
In February 2012, after 2 months of whole-brain
radiotherapy (dosage, 40Gy/20F) yielding a partial response,
gefitinib was administered at a dose of 250 mg/day as the
second-line therapy. However, an EGFR mutation test was not
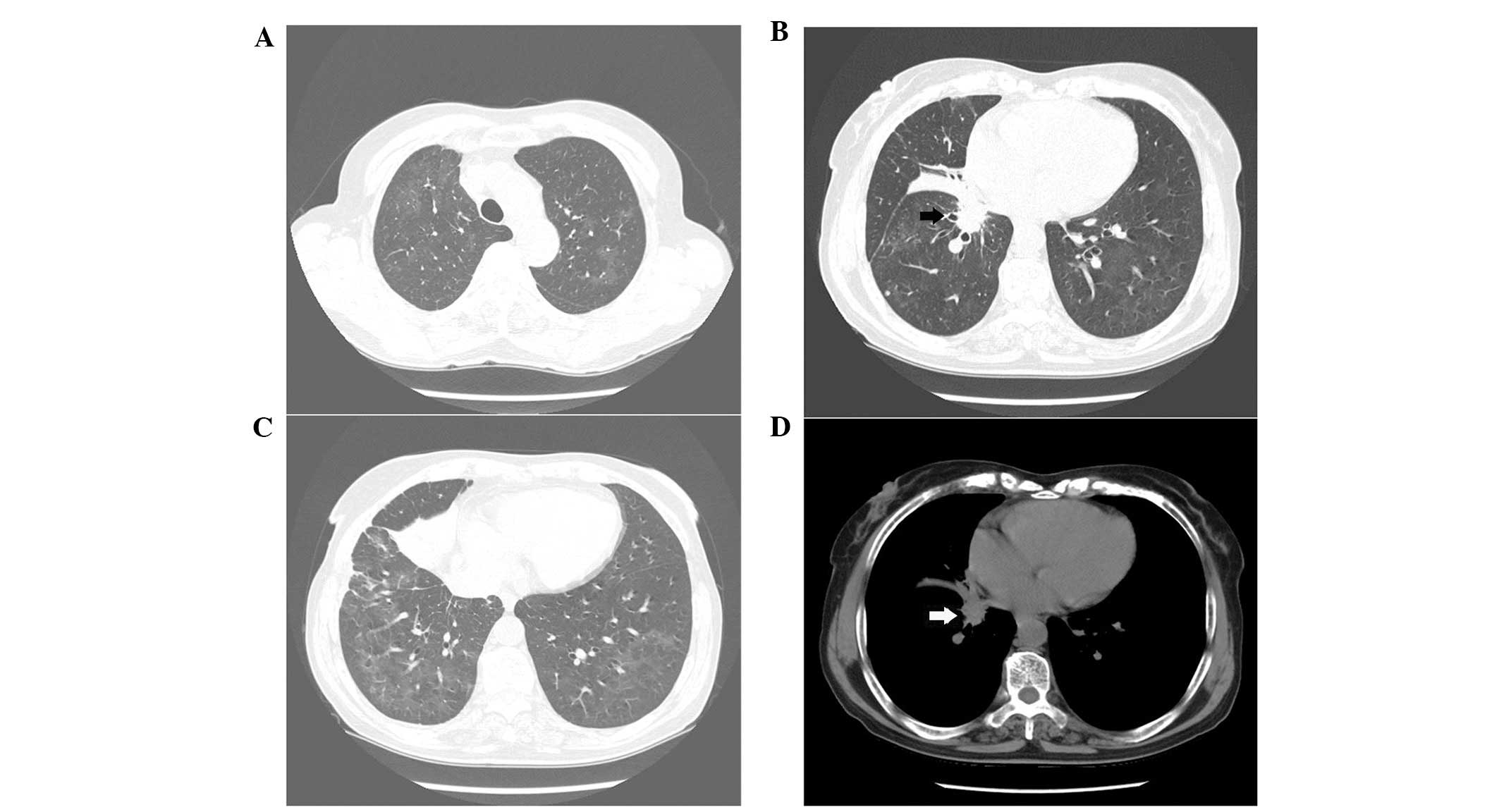
performed as not enough lung cancer tissue was obtained. After 5
months (July 4, 2012), the tumor exhibited partial response;
however, a high-resolution computerized tomography (HRCT) scan
revealed the presence of diffuse ground glass opacities (GGOs) in
the lungs (Fig. 1). Since no
respiratory symptoms or evidence of infections or collagen vascular
diseases were observed, the patient was diagnosed with
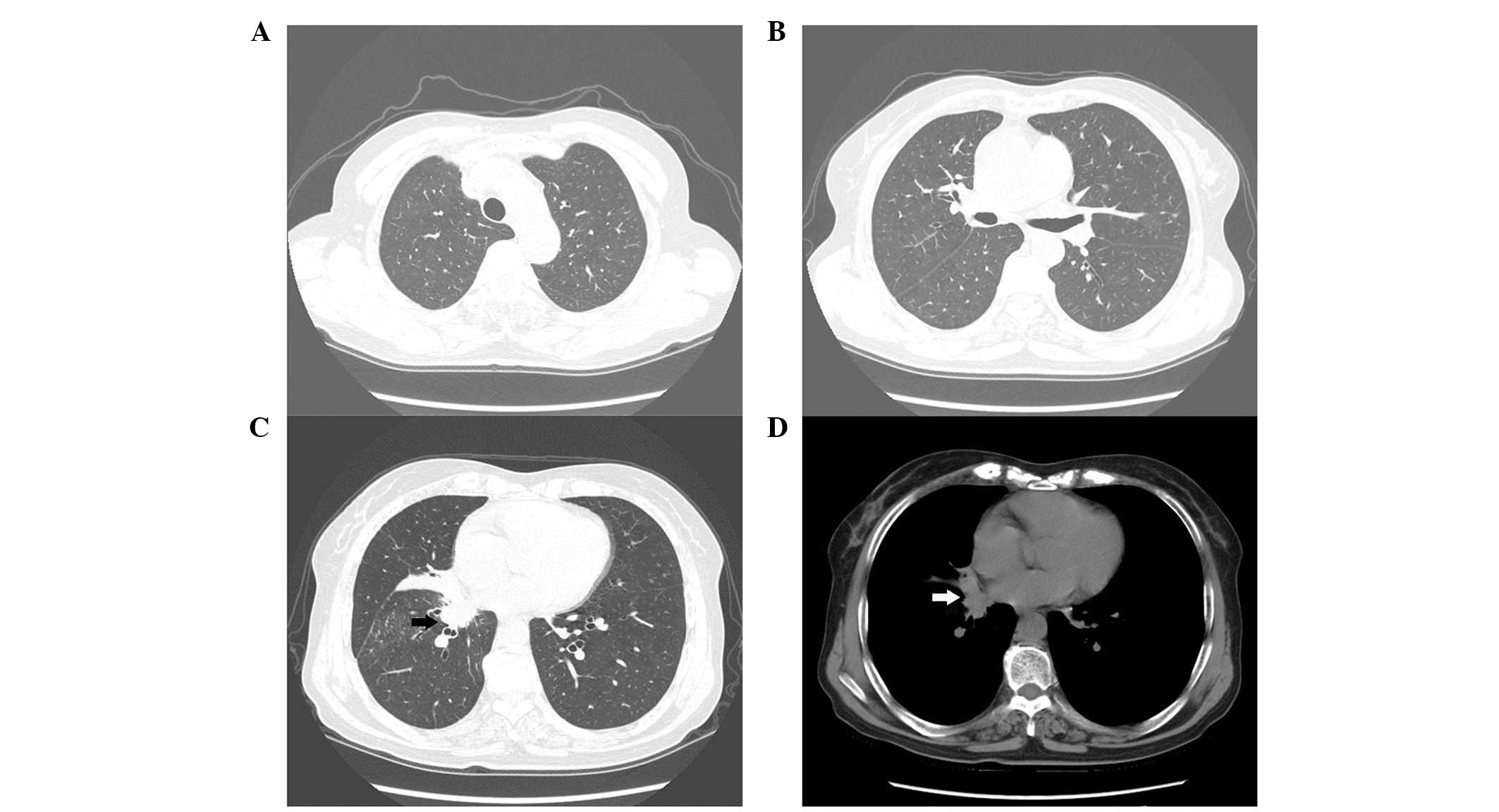
gefitinib-induced ILD. Gefitinib administration was immediately
discontinued, and prednisone was administered orally at a lower
dose of 20 mg/day, which was reduced by 5 mg/week. After a further
2 weeks later (July 20, 2012), an HRCT scan revealed that the size
of the GGOs reduced. After an additional 3.5 months (October 30,
2012), the GGOs disappeared; however, the primary cancer remained
unchanged (Fig. 2). Since the patient
refused further chemotherapy and a marked antitumor response to the
gefitinib treatment was previously observed, gefitinib was
re-administered at the same dose as before, along with
N-acetylcysteine (dosage, 600 mg PO tid for ∼11 months). The
patient achieved 20 months of progression-free survival (PFS) and
30.5 months of overall survival (OS), until April 15, 2014. No GGOs
were detected in HRCT images captured during the 16-month period
prior to the patient succumbing to lung cancer-induced respiratory
failure. The current study was approved by the ethics committees of
Beijing Chao-Yang Hospital, Capital Medical University and written
informed consent was provided by the patient's family.
Discussion
Gefitinib-induced ILD has been reported to occur in
∼4.0% of patients treated with gefitinib in a study on the Japanese
population (12). To date, no precise
management strategy exists for gefitinib-induced ILD. Immediate
withdrawal of gefitinib, administration of corticosteroids and
oxygen therapy are currently recommended (13). Previous reported cases of
gefitinib-induced ILD have typically been treated with a high-dose
of corticosteroids (intravenous injection of 1 g/day
methylprednisolone for three consecutive days, followed by 50 or 60
mg/day oral prednisone, which is reduced by 10 mg/week) or with the
cessation of gefitinib administration, which result in ILD recovery
or mortality (9,11). Intravenous cyclophosphamide has also
been reported as a valid treatment (10). In the present study, gefitinib was
discontinued immediately following the onset of ILD, and a low-dose
of corticosteroids were administered at an early stage.
Takamochi et al (9) reported the re-administration of
gefitinib in a patient who developed gefitinib-induced ILD. A chest
CT scan revealed a significant response following gefitinib
re-administration at a 50% dose (125 mg/day) for a month. However,
Suzuki et al (8) reported a
case of recurrent gefitinib-induced ILD following re-administration
of gefitinib at a dose of 250 mg/day in a patient with severe
ILD.
In the present study, the initial gefitinib
treatment was associated with a remarkable antitumor response, and
no evidence of other adverse events induced by gefitinib was
detected, with the exception of ILD. Thus, gefitinib was
re-administered along with N-acetylcysteine and the patient was
under close observation. N-acetylcysteine is a thiol-containing
compound that contains sulfhydryl groups, which function as a
glutathione precursor or as reduced glutathione, serving as direct
scavengers of reactive oxygen species (14). N-acetylcysteine is commonly used to
treat patients with idiopathic pulmonary fibrosis (15–17). The
patient of the present study exhibited an encouraging response to
gefitinib treatment and achieved long PFS and OS periods. The
clinical benefits observed in the present case suggest that the
management of gefitinib-induced ILD requires further investigation.
Early discontinuation and gefitinib re-administration along with
N-acetylcysteine may be a potential new treatment strategy for
patients suffering from lung tumors and gefitinib-induced ILD.
Acknowledgements
This study was supported by a grant from the Wu
Jieping Medical Foundation (grant no. 320.6750.12623) and by an
educational grant from the Ministry of Education of China (grant
no. 201347; 2014).
References
|
1
|
Fukuoka M, Yano S, Giaccone G, et al:
Multi-institutional randomized phase II trial of gefitinib for
previously treated patients with advanced non-small-cell lung
cancer (The IDEAL 1 Trial) [corrected]. J Clin Oncol. 21:2237–2246.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kris MG, Natale RB, Herbst RS, et al:
Efficacy ofgefitinib, an inhibitor of the epidermal growth factor
receptor tyrosinekinase, in symptomatic patients with non-small
cell lung cancer: a randomized trial. JAMA. 290:2149–2158. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Inoue A, Saijo Y, Maemondo M, et al:
Severe acute interstitialpneumonia and gefitinib. Lancet.
361:137–139. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Okamoto I, Fujii K, Matsumoto M, et al:
Diffuse alveolar damage after ZD1839 therapy in a patient with
non-small cell lung cancer. Lung Cancer. 40:339–342. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ricciardi S, Tomao S and de Marinis F:
Toxicity of targeted therapy in non-small-cell lung cancer
management. Clin Lung Cancer. 10:28–35. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ando M, Okamoto I, Yamamoto N, et al:
Predictive factors for interstitial lungdisease, antitumorresponse
and survival in non-small-cell lung cancer patients treated with
gefitinib. J Clin Oncol. 24:2549–2556. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Luo C, Lv M, Li Y, et al:
Gefitinib-induced interstitial pneumonia: A casereport and review
of the literature. Exp Ther Med. 7:855–859. 2014.PubMed/NCBI
|
|
8
|
Suzuki M, Asahina H, Konishi J, Yamazaki K
and Nishimura M: Recurrent gefitinib-induced interstitial lung
disease. Intern Med. 47:533–536. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Takamochi K, Suzuki K, Bashar AH, et al:
Readministration of gefitinib in a responder after treatment
discontinuation due to gefinitib-related interstitial lung disease:
a case report. J Med Case Rep. 1:1382007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Goto Y, Hojo M, Takeda Y, Kobayashi N and
Kudo K: Gefitinib-induced interstitial lung disease-addition of
intravenous cyclophosphamide to corticosteroids is a valuable
treatment option: A case report. Med Oncol. 27:753–755. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Seto T, Seki N, Uematsu K, et al:
Gefitinib-induced lung injury successfully treated with high-dose
corticosteroids. Respirology. 11:113–116. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kudoh S, Kato H, Nishiwaki Y, et al: Japan
Thoracic Radiology Group: Interstitial lung disease in Japanese
patients with lung cancer: acohort and nested case-control study.
Am J Respir Crit Care Med. 177:1348–1357. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kitajima H, Takahashi H, Harada K, et al:
Gefitinib-induced interstitial lung disease showing improvement
after cessation: disassociation of serummarkers. Respirology.
11:217–220. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gillissen A: Anti-inflammatory efficacy of
N-acetylcysteine and therapeutic usefulness. Pneumologie.
65:549–557. 2011.[In German]. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Albera C, Ferrero C, Rindone E, Zanotto S
and Rizza E: Where do we stand with IPF treatment? Respir Res.
14(Suppl 1): S72013.PubMed/NCBI
|
|
16
|
Behr J and Richeldi L: Recommendations on
treatment for IPF. Respir Res. 14(Suppl 1): S62013.PubMed/NCBI
|
|
17
|
Idiopathic Pulmonary Fibrosis Clinical
Research Network, ; Raghu G, Anstrom KJ, King TE Jr..Lasky JA and
Martinez FJ: Prednisone, azathioprine and N-acetylcysteine for
pulmonary fibrosis. N Engl J Med. 366:1968–1977. 2012. View Article : Google Scholar : PubMed/NCBI
|