Introduction
Retroperitoneal tumors arise from the tissues of the
retroperitoneal space, which includes the following structures: The
adrenal glands, kidneys, ureter, aorta, inferior vena cava,
pancreas (part), duodenum, colon (part), rectum, esophagus, lymph
nodes, and soft tissue. Although in other sites the incidence of a
benign tumor is higher than that of a malignant tumor, the
incidence of a malignant tumor in the peritoneum is ∼4 times higher
than that of a benign tumor (1). The
majority of retroperitoneal tumors are malignant soft tissue
tumors, lymphoproliferative disorders, and malignancies arising
from parenchymal tissues (1).
Approximately one-third of retroperitoneal tumors
are soft tissue sarcomas, with liposarcoma and leiomyosarcoma
accounting for ∼70% and 15% of reteroperitoneal sarcomas,
respectively (2). The retroperitoneum
is the second most common site of origin of soft tissue tumors
(2), with 10–15% of soft tissue
sarcomas arising from the retroperitoneum (3,4). More
rarely, Castleman's tumors (5), adult
neuroblastoma (6), gastrinoma
(7), solitary fibrous tumor of the
pancreas (8), teratoma (9) and neurogenic tumors (10) have been reported to occur in this
region. Due to the rarity of retroperitoneal large adenocarcinoma,
literature regarding the surgical treatment of large
retroperitoneal tumors is limited (11). Furthermore, no standard treatment
exists for patients with inoperable large retroperitoneal tumors
and thus, only palliative chemotherapy or radiotherapy or best
supportive care is administered for these patients.
Retroperitoneal tumors show few clinical symptoms in
the early phase, and are typically detected incidentally by
computed tomography (CT), or by palpation when they become larger.
The current study reports the case of a patient with a large
retroperitoneal tumor, which was treated with definitive
radiotherapy and surgery. Written informed consent was obtained
from the patient.
Case report
A 45-year-old female presented to the emergency
department of Yamagata University Hospital (Yamagata, Japan)
complaining of left abdominal pain and fever. The patient was
initially diagnosed with left hydronephrosis caused by
retroperitoneal abscess. Ureteral catheterization was performed to
treat the left hydronephrosis, and antibiotics (intravenous
meropenem, 1 g/day) were prescribed. However, the abdominal pain
and fever had not improved after 2 weeks, and the patient was
subsequently referred to the Department of Urology (Yamagata
University Hospital).
A CT-guided core-needle biopsy of the
retroperitoneal mass was performed. The mass, which was >10 cm
in maximum diameter, and was determined to be a
poorly-differentiated adenocarcinoma. An immunohistochemical
examination revealed the following characteristics of the tumor:
Cytokeratin (CK)7(+), CK20(-), CK5/6(-), carcinoembryonic antigen
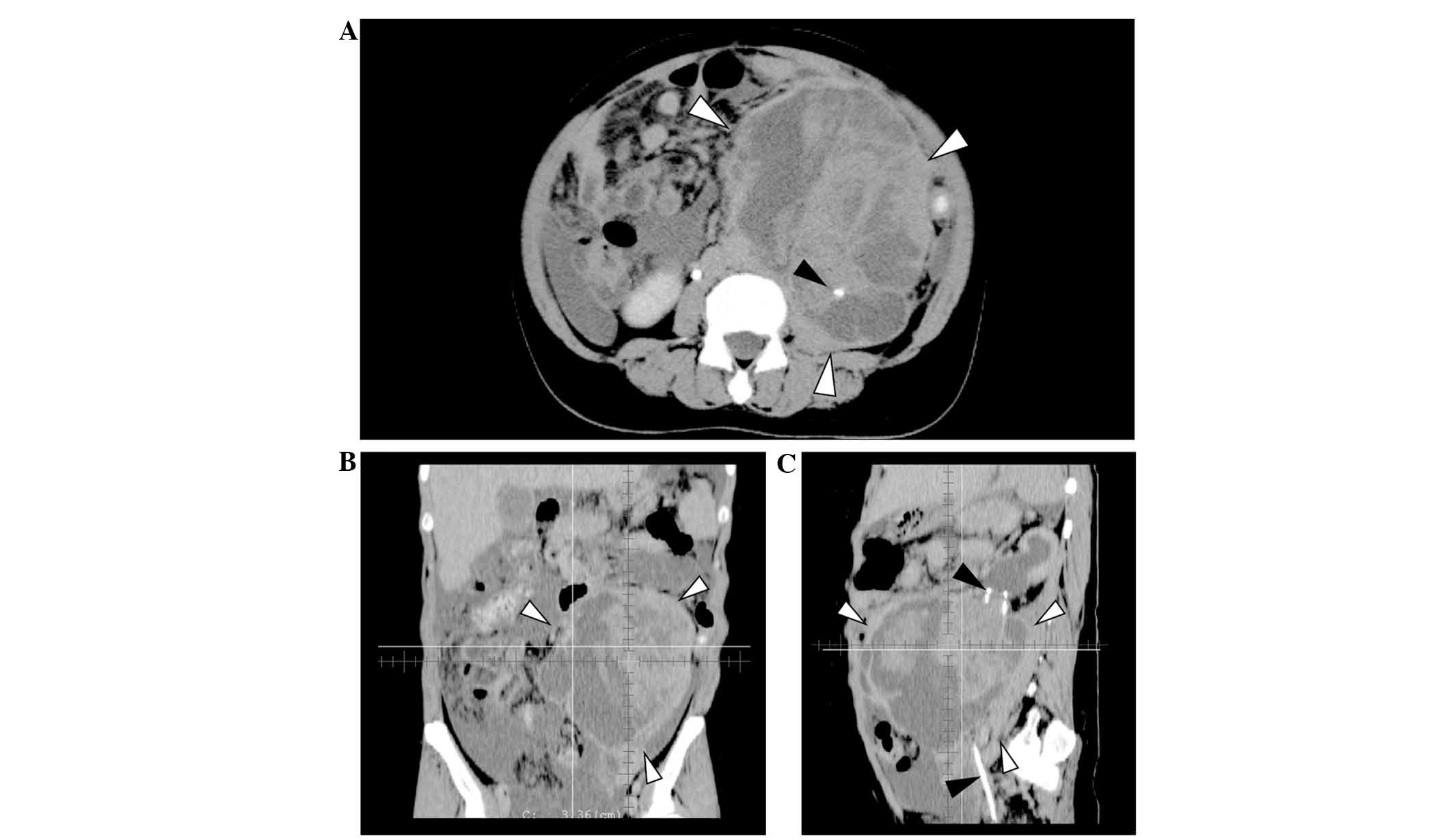
(CEA) (-), and carletinin(-). A CT scan showed a large tumor of
12×16×16 cm, with heterogeneous enhancement and irregular borders,
located in the left retroperitoneum (Fig.
1). Left ureteral involvement of the tumor (Fig. 1A and C, black arrowheads) and
secondary hydronephrosis were detected, however, there was no
continuity between the tumor and the pancreas, adrenal glands,
kidneys or stomach. The tumor was determined to be a
poorly-differentiated adenocarcinoma arising from the left ureter
(12). Although a small amount of
ascites was observed in the abdomen, no definite peritoneal
dissemination or distant metastasis was identified. The patient's
plasma levels of carbohydrate antigen (CA)-125, CA19-9, and CEA
were 201.3 U/ml (normal, <40 U/ml), 16.5 U/ml (normal, <37
U/ml), and 1.42 ng/ml (normal, <5 ng/ml), respectively; of
these, only CA-125 levels were abnormally elevated.
Definitive surgery was initially scheduled. However,
due to the infiltration and rapid growth of the tumor, and the poor
general condition of the patient, the possibility of surgery was
excluded. The patient was referred to the Department of Radiation
Oncology for palliation. She was unable to consume meals due to the
large size of abdominal tumor, and her Eastern Cooperative Oncology
Group performance status was determined to be 3 (13).
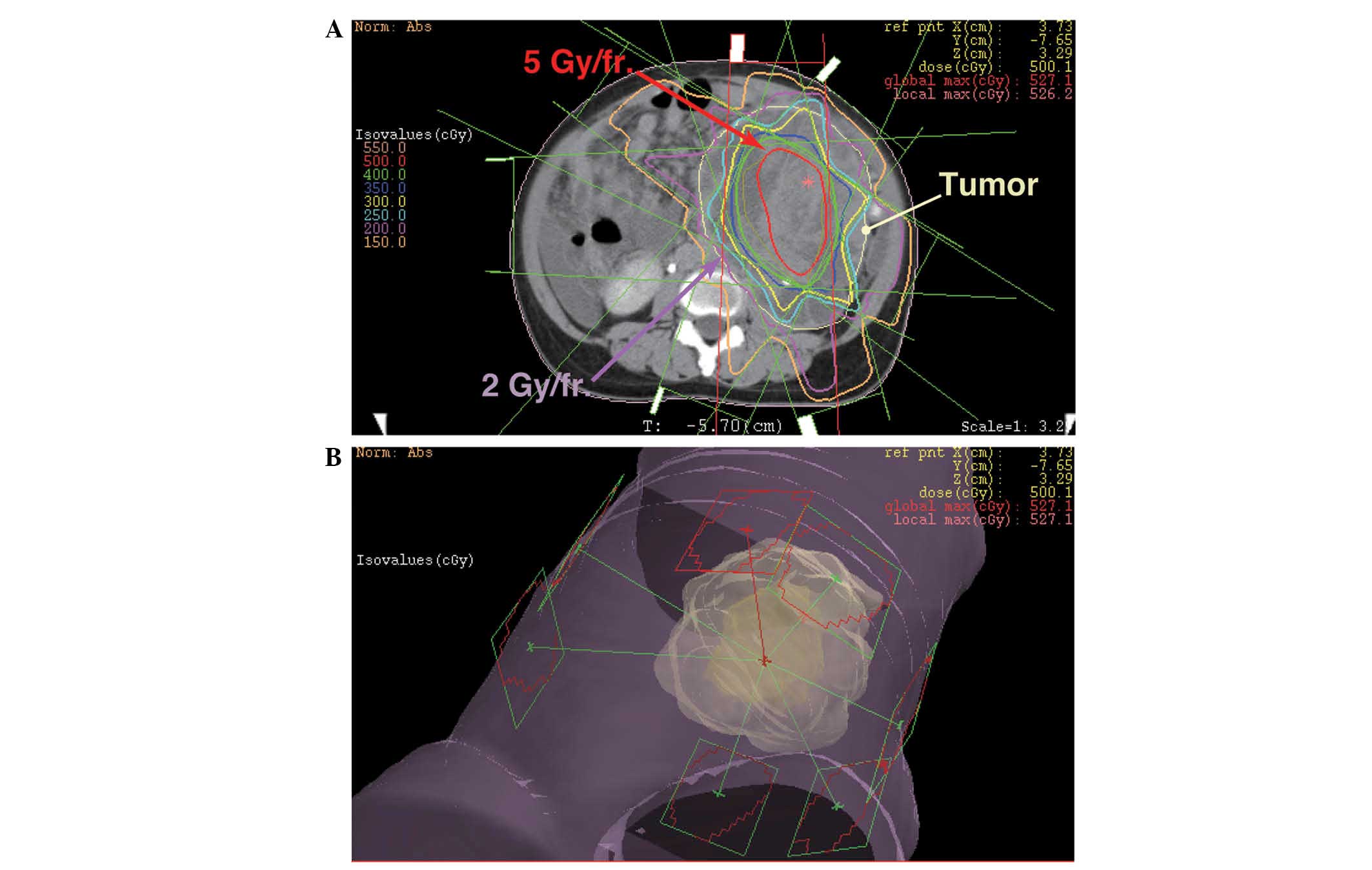
The initial radiation treatment consisted of
coplanar, eight static field three-dimensional-conformal
radiotherapy. The treatment was planned to irradiate the center of
the tumor with 5 Gy/fraction, and the border area of the tumor and
healthy tissue with <2 Gy/fraction (Fig. 2). In total, the center of the tumor
was irradiated with 25 Gy/5 fractions and the border area of the
tumor and healthy tissue was irradiated with 10 Gy/5 fractions.
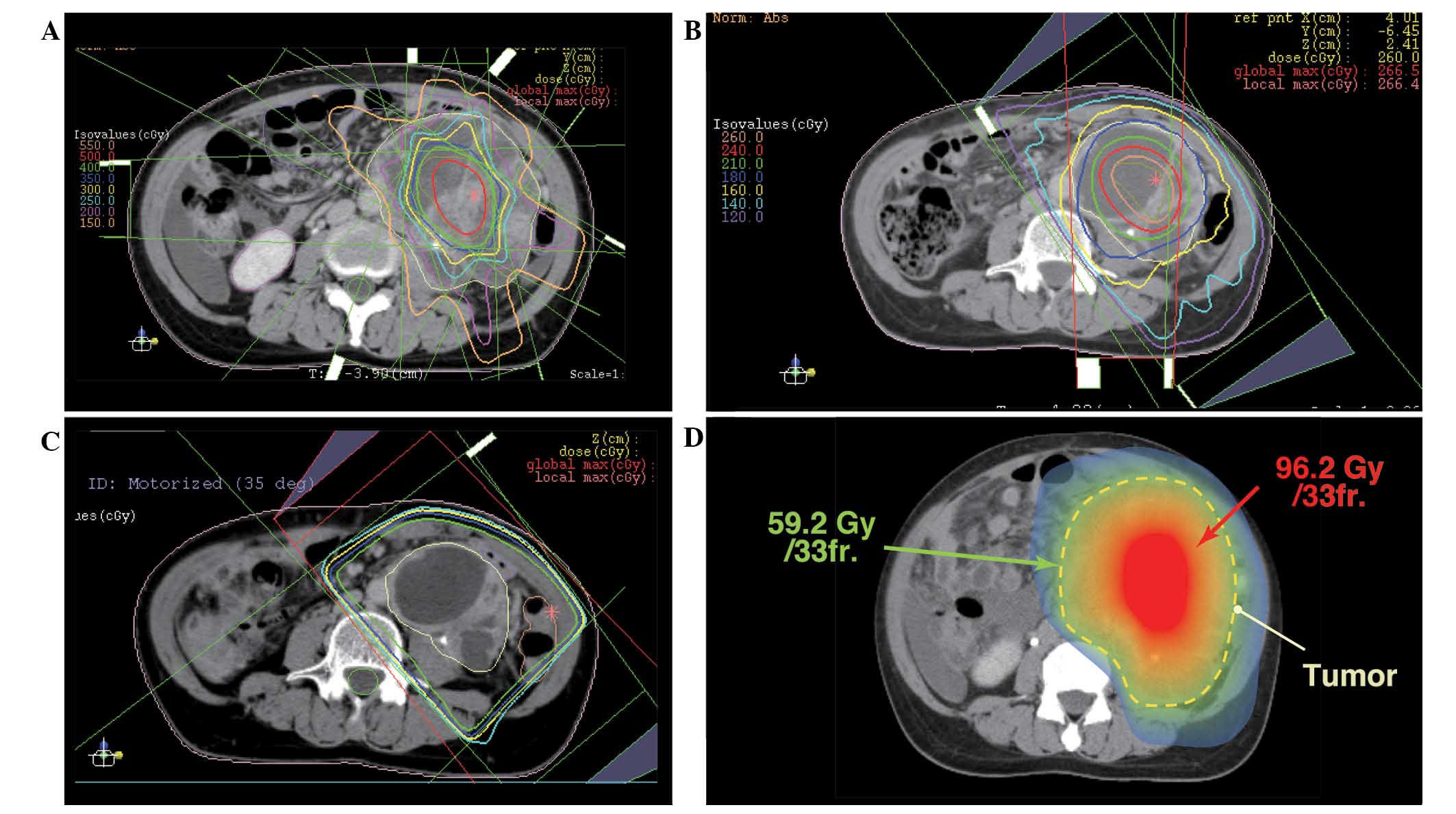
Subsequently, the center of the tumor was irradiated with an
additional 20 Gy/4 fractions (Fig.
3A) and 26 Gy/10 fractions (Fig.
3B) using a modified simultaneous integrated boost (SIB)
technique, and with 25.2 Gy/14 fractions using a standard technique
(Fig. 3C). The cumulative dose to the
center of the tumor and border area of the tumor was 96.2 Gy/33
fractions and 59.2 Gy/33 fractions, respectively (Fig. 3D). The equivalent dose in 2
Gy/fraction (EQD2Gy) was calculated using the following equation:
EQD2Gy = (total dose) × (dose/fraction + α/β) / (2 + α/β) (14), and the α/β of the tumor was assumed to
be 10 (15). The EQD2Gy of the center
of the tumor was calculated to be ∼108 Gy, and the EQD2Gy of the
surrounding healthy tissue was calculated to be ∼58 Gy. This
radiotherapy with modified SIB technique was approved as a clinical
trial by the Institutional Review Board of Yamagata University
Hospital.
Almost no side effects were caused by radiation
therapy during the course of irradiation. Symptoms caused by the
tumor decreased with the progression of the treatment, and the
performance status at the completion of irradiation treatment was
0. The size of the tumor at the end of the irradiation was 7×6×15
cm (80% reduction in volume), and the cystic components and
fibrotic septum without enhancing solid components were dominant in
the tumor (Fig. 3C). After 47 days
from the final day of irradiation, the patient underwent a combined
resection of the tumor and adjacent organs (including part of the
peritoneum and small bowel). Although no tumor regrowth was
observed, the resection was performed for confirmation of tumor
response as the patient's physical condition had improved and was
considered suitable for surgery.
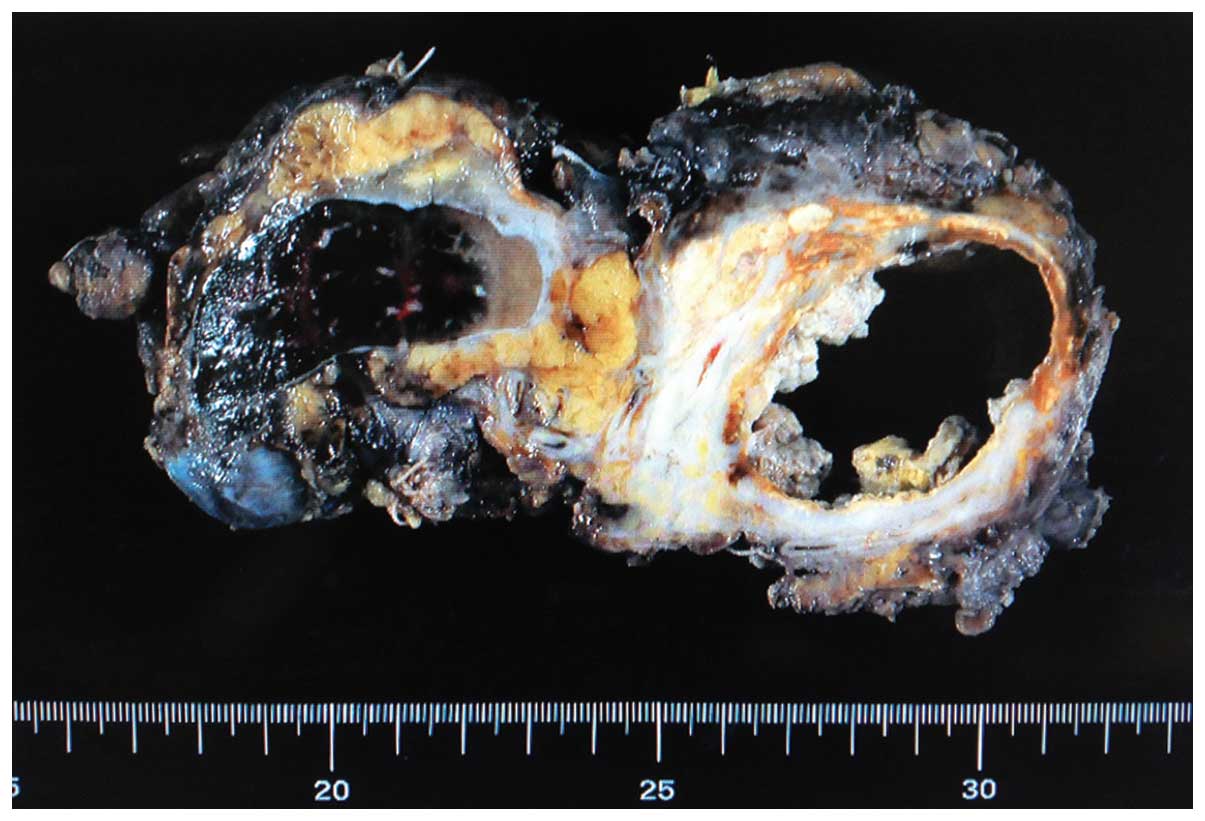
The resected tumor is shown in Fig. 4. Almost all of the cystic component
was necrotic tissue, and xanthogranulomatous changes and fibrosis
were observed in the peripheral region. No residual adenocarcinoma
cells were observed (pathologically complete response). The ureter
that was located in the center of the tumor was replaced by
fibrotic tissue due to tumor invasion and irradiation, and
pyelonephritis and hydronephrosis were observed in the left kidney.
The patient has been recurrence-free for 3 years and 3 months, with
no metastasis or complications.
Discussion
Soft tissue sarcoma or lymphoproliferative disorders
are dominant in retroperitoneal neoplasms (1,3,4). Various types of adenocarcinoma of the
retroperitoneum have been reported, including pancreatic cancer,
renal cell carcinoma, mucinous adenocarcinoma (16,17),
Müllerian adenocarcinoma (18),
cystadenocarcinoma (19) and
adenocarcinoma arising from retroperitoneal teratoma (20).
Surgical resection is typically used for the
treatment of retroperitoneal malignant tumors, including soft
tissue sarcoma, pancreatic cancer, adrenal cancer (3), whilst chemotherapy with/without
radiotherapy is used for the treatment of lymphoproliferative
disorders (21,22). Non-hematological tumors, including
sarcoma, adenocarcinoma and neurogenic tumors, are usually
insensitive to radiation. Furthermore, although microscopic lesions
may be controlled with intraoperative or postoperative radiotherapy
(23,24), radiotherapy is not used as the
definitive treatment of retroperitoneal tumors. The tolerance dose
of abdominal organs, such as the small intestine and duodenum, is
≤60 Gy in EQD2Gy; however, adenocarcinomas of >10 cm cannot be
controlled with a total dose of 60 Gy, thus the required dose for
control of large retroperitoneal tumors exceeds the tolerance dose
of healthy tissues.
In the present case, modified SIB radiotherapy was
used. The standard SIB technique can create contrasts in the dose
distribution, and is used for head and neck or brain tumors
(25,26). However, the dose distribution in the
tumor is homogeneous in the standard SIB technique, and the dose
received by the tumor usually does not exceed the tolerance dose of
the surrounding healthy tissue. With the modified SIB technique, it
is possible to irradiate the center of tumor with higher doses than
the surrounding healthy tissue, by creating contrasts in the dose
distribution in the tumor (27,28). This
difference between the standard SIB technique and modified SIB
technique is demonstrated in the present study. For example, as a
single dose of 5 Gy is dangerous for the digestive tract, it is
typically not used in abdominal radiotherapy. However, in the
current patient, the modified SIB technique was used to safely
irradiate the tumor with 5 Gy/fraction by reducing the dose to the
surrounding tissue to <2 Gy/fraction (Fig. 2). The total irradiation dose received
by the center of the tumor was calculated to be ∼108 Gy in EQD2Gy.
Although this dose is not used in standard radiotherapy, the
modified SIB technique allowed the safe administration of the
scheduled radiotherapy. In addition, surgical resection was
successfully performed without complications.
In conclusion, recent advanced technologies in
radiotherapy have enabled the planning of precise and complex
radiotherapy in the present case. The modified SIB technique is a
new method that is considered to change the conventional concept
that the irradiation dose must not exceed the tolerance dose of
healthy tissues. This technique is particularly effective for large
tumors in which a dose higher than the tolerance dose of healthy
tissues is necessary. Furthermore, as demonstrated by the present
case, complete recovery can be achieved for patients who cannot
undergo surgery due to the advanced nature of the tumor. Modified
SIB radiotherapy may be used in abdominal tumors and also in tumors
arising at other sites (27). Future
challenges include the establishment of a technique for the use of
modified SIB radiotherapy and increasing the number of enrolled
patients.
References
|
1
|
Van Roggen JF and Hogendoorn PC: Soft
tissue tumours of the retroperitoneum. Sarcoma. 4:17–26. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Strauss DC, Hayes AJ and Thomas JM:
Retroperitoneal tumours: Review of management. Ann R Coll Surg
Engl. 93:275–280. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Strauss DC, Hayes AJ, Thway K, Moskovic
EC, Fisher C and Thomas JM: Surgical management of primary
retroperitoneal sarcoma. Br J Surg. 97:698–706. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Clark MA, Fisher C, Judson I and Thomas
JM: Soft-tissue sarcomas in adults. N Engl J Med. 353:701–711.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Menenakos C, Braumann C, Hartmann J and
Jacobi CA: Retroperitoneal Castleman's tumor and paraneoplastic
pemphigus: report of a case and review of the literature. World J
Surg Oncol. 5:452007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zerrweck-López C, Quijano-Orvañanos F,
Montañez-Ramírez H, Murillo-Zolezzi A, Toledo-Valdovinos S and
Padilla-Longoria R: Neuroblastoma in the adult. Case report. Cir
Cir. 77:397–401. 2009.PubMed/NCBI
|
|
7
|
Kattepura S, Das K, Correa MM and
Devarabhavi H: Giant gastrinoma in a child: Case report and review.
Pediatr Surg Int. 24:1083–1085. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tasdemir A, Soyuer I, Yurci A, Karahanli I
and Akyildiz H: A huge solitary fibrous tumor localized in the
pancreas: A young women. JOP. 13:304–307. 2012.PubMed/NCBI
|
|
9
|
Gatcombe HG, Assikis V, Kooby D and
Johnstone PA: Primary retroperitoneal teratomas: A review of the
literature. J Surg Oncol. 86:107–113. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li Z, Xiang J, Yan S, Gao F and Zheng S:
Malignant triton tumor of the retroperitoneum: A case report and
review of the literature. World J Surg Oncol. 10:962012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Buse S, Gilfrich C, Wagener N,
Pfitzenmaier J, Haferkamp A and Hohenfellner M: Thoraco-abdominal
approach to large retroperitoneal tumours. BJU Int. 98:969–972.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
National Comprehensive Cancer Network, .
Occult Primary. Version 3. 2014.http://www.nccn.org/professionals/physician_gls/pdf/occult.pdfJuly
9–2014
|
|
13
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Joiner MC: A simple alpha/beta-independent
method to derive fully isoeffective schedules following changes in
dose per fraction. Int J Radiat Oncol Biol Phys. 58:871–875. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stuschke M, Budach V, Budach W, Feldmann
HJ and Sack H: Radioresponsiveness, sublethal damage repair and
stem cell rate in spheroids from three human tumor lines:
Comparison with xenograft data. Int J Radiat Oncol Biol Phys.
24:119–126. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jiang H, Jin K, You Q, Fang W and Xu N:
Retroperitoneal primary mucinous adenocarcinoma: A case report.
Oncol Lett. 2:633–636. 2011.PubMed/NCBI
|
|
17
|
Cupp JS, Illeck J, Rahbar N, Rettenmaier
MA and Goldstein BH: A rare case of primary retroperitoneal
mucinous adenocarcinoma: A case report. J Reprod Med. 58:85–88.
2013.PubMed/NCBI
|
|
18
|
Spinelli C, Strambi S, Tartaglia D, Di
Franco G, Pucci V, Faviana P and Lencioni M: Primary
retroperitoneal müllerian adenocarcinoma: A case report and
literature review. Case Rep Oncol. 6:616–621. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yadav R, Kataria K, Balasundaram P and
Karak AK: Mucinous cystadenocarcinoma arising in an ectopic kidney
simulating a retroperitoneal dermoid cyst: A rare tumour presenting
as a diagnostic dilemma. Malays J Pathol. 35:95–98. 2013.PubMed/NCBI
|
|
20
|
Ghosal SR, Das S, Maji A, Dey KK and
Bagchi D: Adenocarcinoma in retroperitoneal teratoma. Indian J
Surg. 75:33–35. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tambo M, Fujimoto K, Miyake M, et al:
Clinicopathological review of 46 primary retroperitoneal tumors.
Int J Urol. 14:785–788. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
National Comprehensive Cancer Network, .
Non-Hodgkin's Lymphomas. Version 2. 2014.http://www.nccn.org/professionals/physician_gls/pdf/nhl.pdfMay
29–2014
|
|
23
|
Clark JA and Tepper JE: Role of radiation
therapy in retroperitoneal sarcomas. Oncology (Williston Park).
10:1867–1872. 1996.PubMed/NCBI
|
|
24
|
Thomas DM, O'Sullivan B and Gronchi A:
Current concepts and future perspectives in retroperitoneal
soft-tissue sarcoma management. Expert Rev Anticancer Ther.
9:1145–1157. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Peponi E, Glanzmann C, Kunz G, Renner C,
Tomuschat K and Studer G: Simultaneous integrated boost
intensity-modulated radiotherapy (SIB IMRT) in nasopharyngeal
cancer. Strahlenther Onkol. 186:135–142. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cho KH, Kim JY, Lee SH, et al:
Simultaneous integrated boost intensity-modulated radiotherapy in
patients with high-grade gliomas. Int J Radiat Oncol Biol Phys.
78:390–397. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nomiya T, Akamatsu H, Harada M, et al:
Modified simultaneous integrated boost radiotherapy for an
unresectable huge refractory pelvic tumor diagnosed as a rectal
adenocarcinoma. World J Gastroenterol. 20:18480–18486. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Nomiya T, Akamatsu H, Harada M, Ota I,
Hagiwara Y, Ichikawa M, Miwa M, Suzuki A and Nemoto K: Modified
simultaneous integrated boost radiotherapy for unresectable locally
advanced breast cancer: Preliminary results of a prospective
clinical trial. Clin Breast Cancer. Nov 15–2014.(Epub ahead of
print). PubMed/NCBI
|