Introduction
Gastric cancer is the fourth most common malignancy
and the second most common cause of cancer-related death worldwide
(1). As a result of early
detection, developments in surgical techniques and the development
of anticancer agents, the survival of patients with gastric cancer
has improved. However, the prognosis of advanced gastric cancer is
still poor. While a 5-year survival rate of patients with stage I
is more than 96%, that of patients with stage IV is less than 20%
(2). Central nervous system (CNS)
metastasis is a rare complication of gastric cancer, occurring in
0.16–0.69% of gastric cancer patients, and its clinical features,
treatment outcomes and prognostic factors remain unclear (3).
Numerous molecular events are involved in metastatic
progression, such as loss of cellular adhesion, detachment of tumor
cells from the original sites, degradation of the extracellular
matrix, migration of tumor cells, angiogenesis, and implantation of
tumor cells at distant sites (4).
The transmembrane glycoproteins E- and N-cadherin play a role in
calcium-dependent cell-to-cell adhesion, and reduced E-cadherin
expression is associated with gastric and colon cancer progression
and metastasis (5,6). MSS1 is a nuclear-encoded mitochondrial
GTPase, and silencing of MSS1 gene expression is associated with
neuroinflammation (7). Claudin-3
and -4 are major structural molecules of the tight junctions that
link epithelial cells (8). They are
associated with worse malignancy grades, not only in terms of size
and invasiveness, yet also in potential metastatic ability and
patient outcome. Malignant cells show increased glucose uptake
in vitro and in vivo, and this is facilitated by
glucose transporters (Gluts) (9).
The expression of Glut1 has been described in several malignancies,
including those of the esophagus, colon and brain, and Glut1
expression is associated with tumor aggressiveness and survival in
gastric cancer (10). Clusterin
expression is upregulated in many malignancies, including head and
neck, breast and prostate cancers (11). The function of clusterin in cell
reconstruction contributes to the occurrence and progression of
cancer (12). ITGB4 is an adhesion
receptor for lamins and plays a key role in the progression of
various carcinomas via its ability to orchestrate key signal
transduction events and promote cell motility (13). Vascular endothelial growth factor
(VEGF) is one of the most important factors promoting
vascularization, and it plays a role in both physiological and
malignant conditions (14). Several
studies have reported that VEGF is associated with lymph node
metastasis in gastric cancer. Epidermal growth factor receptor
(EGFR) is a transmembrane receptor that contributes to many
processes involved in cell survival and proliferation and also
inhibits apoptosis, which leads to cancer development (15). Preusser et al evaluated the
expression of EGFR immunohistochemically in tissue samples of
gastroesophageal cancer brain metastasis, which they proposed could
be treated by agents targeting EGFR (16). p53 is a nuclear phosphoprotein
involved in regulating cell proliferation by inhibiting the
G1 to S phase progression of the cell cycle, and it is
frequently mutated in a variety of human cancers (17). The present study evaluated the
expression of E- and N-cadherin, MSS1, claudin-3 and -4, Glut1,
clusterin, ITGB4, VEGF, EGFR and p53 in surgical specimens of
gastric cancer with and without brain metastasis and analyzed their
correlations with clinicopathological features and survival.
Metformin is an oral biguanide introduced in the
1950 for the treatment of type 2 diabetes (18). A recent epidemiologic survey found
that metformin had also significant effects on tumorigenesis
(19). It was also reported that
metformin inhibits human gastric cancer cell proliferation and
tumor growth, possibly by suppressing cell cycle-related molecules
(20). Candidate markers associated
with brain metastasis were investigated in tumor-bearing mouse
models treated with metformin to evaluate its use in preventing or
targeting brain metastasis therapeutically.
Materials and methods
Patients
Nine samples of gastric adenocarcinoma with brain
metastasis were acquired from St. Vincent's Hospital, The Catholic
University of Korea from June 1997 to September 2009. Two of the
nine patients underwent craniotomies to resect metastatic brain
lesions. Seven patients were diagnosed with brain metastasis using
brain magnetic resonance imaging (MRI), four of whom showed
positive cytology in the cerebrospinal fluid (CSF). Thirteen
samples of advanced gastric adenocarcinoma without brain metastasis
were also included.
The study protocol was approved by the Institutional
Review Board of St. Vincent's Hospital, The Catholic University of
Korea. The stages of all patients were evaluated in accordance with
the guidelines of the Japanese Classification of Gastric Carcinoma
(21). The surgical treatment
comprised gastric resection, bypass procedures or laparotomy alone.
All patients were followed for a median of 12.5 (range 3–80)
months. Patient data were obtained from our own and the Korea
Central Cancer Registry database. Survival time was measured from
the date of the initial surgery to that of death or last follow-up.
Patients who died as a result of surgery or from other causes were
excluded from the present study.
Construction of the tissue microarray
block
Formalin-fixed paraffin-embedded tissues were
obtained from the subjects. Using hematoxylin and eosin
(H&E)-stained slides, a representative tumor site was chosen,
and the site corresponding to the confirmed tumor site in the
paraffin block was marked. Areas with necrosis, hemorrhage or
artifacts were excluded. Single-core biopsy specimens 2 mm in
diameter were taken from the representative regions (Seongkohn
Trader's Co, Seoul, Korea), placed on a trimethylamine (TMA) mold
with 60-pores, and re-embedded with paraffin. The TMA blocks were
prepared as 4-µm-thick sections and stained with H&E.
The tissues were then examined to determine whether an appropriate
tumor site had been selected.
Immunohistochemistry
We performed immunohistochemical staining using
tissue microarray sections and a BenchMark XT autostainer (Ventana
Medical Systems, Tucson, AZ, USA), according to the manufacturer's
protocol. The respective antibodies used for immunohistochemistry
of E- and N-cadherin, MSS1, claudin-3 and -4, Glut1, clusterin,
ITGB4, VEGF, EGFR and p53 were 36/E-cadherin (1:50; BD Biosciences,
Rockville, MD, USA), N-cadherin rabbit monoclonal antibody (1:100;
Enzo Life Sciences, Plymouth Meeting, PA, USA), ab78161 (1:25),
ab15102 (1:50) (both from Abcam, Cambridge, MA, USA), mouse
monoclonal antibody to claudin-4 (1:100; Young in Frontier, Seoul,
Korea), ab14683 (1:200; Abcam), mouse monoclonal antibody to
clusterin (1:50; Young in Frontier), ITGB4 rabbit monoclonal
antibody (1:15; Abgent, San Diego, CA, USA), mouse monoclonal
antibodies to VEGF (1:100), EGFR (1:100) (both from Santa Cruz
Biotechnology, Santa Cruz, CA, USA) and ab61256 (1:100; Abcam).
Ki-67 p53, bcl-2 and Bax were detected using clone PP-67 (1:100;
Abcam). Clone images were acquired using an Olympus BX41 microscope
with a DP72 digital camera (both from Olympus, Tokyo, Japan).
The immunostained slides were examined under light
microscopy by one of the authors (S.H. Kim). The
immunohistochemical results were scored semi-quantitatively using a
four-point scale: 0, no immunoreaction; 1+, faint or equivocal
immunoreaction in <10% of cells; 2+, unequivocal, strong
immunoreaction in <30% of cells; and 3+, unequivocal, strong
immunoreaction in >30% of cells. Tumors with 1+, 2+ or 3+
expression were interpreted as positive, while tumors with no
expression were interpreted as negative.
Inoculation of intracranial cancer cells
and experimental design
The human gastric adenocarcinoma MK28 cell line was
provided by one of the authors (S.H. Kim) and maintained in
RPMI-1640 medium supplemented with 10% fetal bovine serum (FBS)
under routine tissue culture conditions. Four-weeks-old male
athymic nude mice (Central Laboratory Animals, Seoul, Republic of
Korea) were used. The nude mice were anesthetized using an
intraperitoneal (i.p.) injection of 12 mg/kg xylazine (Rompun;
Cutter Laboratories, Shawnee, KS, USA) and 30 mg/kg ketamine
(Ketalar; Parke-Davis, Morris Plains, NJ, USA). The mice were then
stereotactically inoculated with 1×106 MK28 cells into
the right frontal lobe (2 mm lateral and 1 mm anterior to the
bregma at a depth of 2.5 mm from the skull) using a sterile
Hamilton syringe fitted with a 26-gauge needle (Hamilton, Reno, NV,
USA) and a microinfusion pump (Harvard Apparatus, Holliston, MA,
USA).
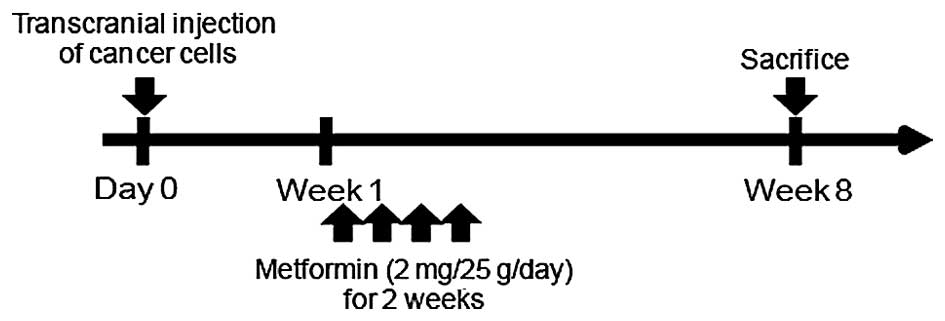
The experimental design is shown in Fig. 1. Each group contained five mice
initially. Mice in the treatment group were treated with metformin
(2 mg/25 g/day) via i.p. injection for 14 days, 1 week after being
inoculated intracranially with MK28 cells. Mice in the control and
treatment groups were euthanized 8 weeks after the intracranial
inoculation, and tumor specimens were obtained for reverse
transcription-polymerase chain reaction (RT-PCR) and western
blotting. All experiments were approved by the Ethics Committee of
the St. Vincent's Hospital, The Catholic University of Korea.
Reverse transcription-PCR
Total RNA from all specimens was extracted using an
RNeasy Mini kit (Qiagen), and 1 µg was reverse-transcribed
using RT-premix (M-Biotech, Seoul, Korea). RT-PCR was performed on
cDNA samples using a DNA Thermal Cycler (Bio-Rad) with Go
Taq Green Master Mix (Promega, Madison, WI, USA), RNase-free
water and the following primers: E-cadherin
5′-AAGTGACCGATGATGATGCC-3′ (forward), and
5′-CTTCTCTGTCCATCTCAGCG-3′ (reverse); and 18S rRNA
5′-CGCGGTTCTATTTTGTTGGT-3′ (forward), and
5′-AGTCGGCATCGTTTATGGTC-3′ (reverse). Expression of MMP9,
N-cadherin and VEGF was assessed by RT-PCR using the following
primers: MMP9 5′-AGTTTGGTGTCGCGGAGCAC-3′ (forward), and
5′-TACATGAGCGCTTCCGGCAC-3′ (reverse); N-cadherin
5′-GCCACCATATGACTCCCTCTTAGT-3′ (forward), and
5′-CAGAAAACTAATTCCAATCTGAAA-3′ (reverse); and VEGF
5′-CCAGCGAAGCTACTGCCGTCCA-3′ (forward), and
5′-ACAGCGCATCAGCGGCACAC-3′ (reverse). The RT-PCR products were
separated on 1.2% agarose gels containing ethidium bromide and were
visualized with ultraviolet light.
Western blot analysis
Total proteins in the tumor specimens were extracted
using PRO-PREP Protein Extraction Solution (Intron Biotechnology,
Gyeonggi-Do, Korea) according to the manufacturer's instructions.
Western blot analysis was performed to confirm expression using
antibodies recognizing the specific epitopes. The proteins were
separated by sodium dodecyl sulfate-polyacrylamide gel
electrophoresis (SDS-PAGE), transferred to nitrocellulose membranes
and detected with antibodies to E-cadherin (BD Biosciences,
Franklin Lakes, NJ, USA), MMP9 (Abcam), VEGF (Santa Cruz
Biotechnology), N-cadherin (Abcam) and β-actin (Sigma-Aldrich, St.
Louis, MO, USA). After washing, the membrane was incubated with
anti-mouse IgG or anti-rabbit IgG, horseradish peroxidase
(HRP)-linked secondary antibody (Cell Signaling Technology,
Danvers, MA, USA) or anti-goat IgG HRP-antibody derived from rabbit
(Sigma-Aldrich). Immunoreactivity was detected using the ECL
chemiluminescence system (Thermo, Rockford, IL, USA) and quantified
using an imaging densitometer (Model LAS 4000 mini; GE Healthcare
Bio-Sciences AB Hercules, Japan). The density of each band was
quantified using Quantity One software (Bio-Rad Laboratory,
Hercules, CA, USA).
Statistical analysis
The distributions of patient characteristics were
compared between the study and control groups using the Wilcoxon
rank-sum and Fisher's exact tests for continuous and discrete
variables, respectively. Differences in the immunohistochemical
results between groups were analyzed using the Chi-square test.
Overall survival was analyzed using the Kaplan-Meier method, and
survival data were compared using a log-rank test. A p-value of
<0.05 was considered to indicate a statistically significant
result.
Results
Patient characteristics
The characteristics of the present study population
are listed in Table I. There were
no significant differences in age, gender, histology type, tumor
size, stage, vascular invasion or perineural invasion between the
case and control groups. Lymphatic invasion was significantly
higher in the control group than the case group (92.3 vs. 44.4%,
p=0.023). The median interval between the diagnosis of stomach
cancer and the detection of brain metastasis was 9 (range 1–77)
months.
 | Table ICharacteristics of the patients. |
Table I
Characteristics of the patients.
| Parameters | Case group | Control group | P-value |
|---|
| Gender | | | >0.05 |
| Men | 7 | 10 | |
| Women | 2 | 3 | |
| Age (years) | | | >0.05 |
| Median (range) | 74 (45–82) | 71 (43–81) | |
| Differentiation | | | >0.05 |
| Well | 0 | 1 | |
| Moderate | 4 | 4 | |
| Poor | 5 | 7 | |
| Mucinous | 0 | 1 | |
| Size | | | >0.05 |
| Mean ± SD | 5.0±1.8 | 6.7±2.5 | |
| Stage | | | >0.05 |
| I | 1 | 0 | |
| II | 0 | 2 | |
| III | 7 | 4 | |
| IV | 1 | 7 | |
| Lymphatic
invasion | 44.40% | 92.30% | 0.023 |
| Vascular
invasion | 44.40% | 38.50% | >0.05 |
| Neural
invasion | 33.30% | 69.20% | 0.192 |
| Follow-up
(months) | | | >0.05 |
| Median
(range) | 12 (4–80) | 18 (3–36) | |
Immunohistochemistry
The immunohistochemical staining results for each
protein are presented in Table II.
E-cadherin had the strongest expression in both groups (100 vs.
69.2%). EGFR expression was lowest in the case group (0%), while
the expression levels of ITGB4 and VEGF were lowest in the control
group (0%). No significant differences in biomarker expression were
detected between cases and controls. However, VEGF expression
tended to be higher in the case group (33.3 vs. 0%, p=0.055). The
immunoreactivity of N-cadherin and VEGF is shown in Fig. 2.
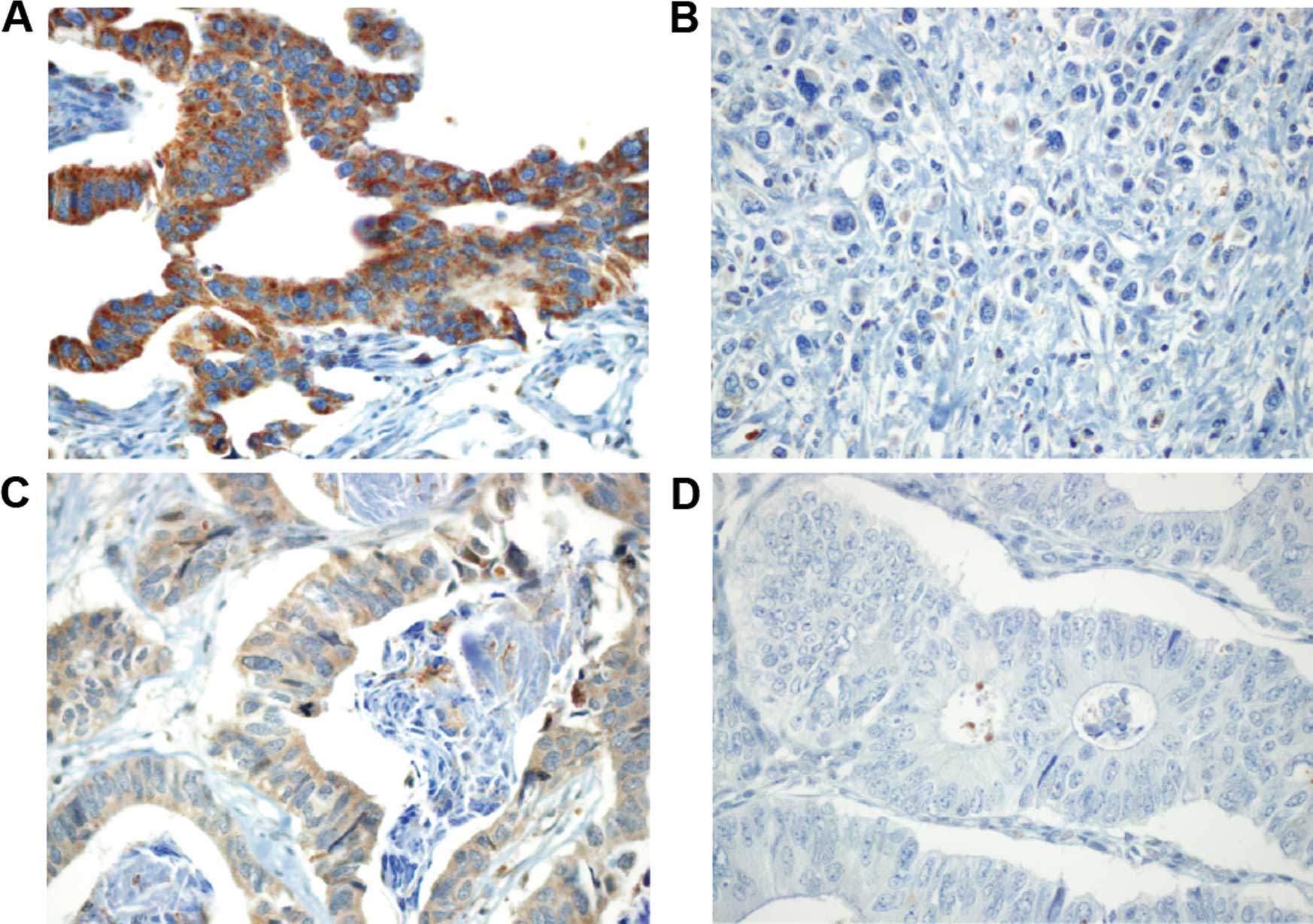 | Figure 2Immunohistochemical staining for
N-cadherin and VEGF. A tissue core of gastric adenocarcinoma showed
strong N-cadherin expression (A, 3+, ×400), whereas
another tissue core showed negative N-cadherin expression (B,
negative, ×400). Weak (C, 1+, ×400) and negative (D,
negative, ×400) VEGF expression are also shown. VEGF, vascular
endothelial growth factor. |
| Table IIImmunostaining. |
Table II
Immunostaining.
| Biomarker | Positive
| P-value |
|---|
| Case (%) | Control (%) |
|---|
| E-cadherin | 100 | 69.2 | 0.115 |
| N-cadherin | 66.7 | 46.2 | >0.05 |
| MSS1 | 66.7 | 38.5 | >0.05 |
| Claudin 3 | 44.4 | 23.1 | >0.05 |
| Claudin 4 | 55.6 | 23.1 | >0.05 |
| Glut 1 | 33.3 | 30.8 | >0.05 |
| Clusterin | 44.4 | 38.5 | >0.05 |
| ITGB4 | 22.2 | 0 | >0.05 |
| VEGF | 33.3 | 0 | 0.055 |
| EGFR | 0 | 7.7 | >0.05 |
| p53 | 66.7 | 53.9 | >0.05 |
Survival analysis
Survival analyses with respect to the
clinicopathological variables and biomarker expression profiles
using the Kaplan-Meier method are summarized in Table III and IV. N-cadherin expression (36 vs. 12
months, p=0.027) and vascular invasion (12 vs. 33 months, p=0.008)
were significantly correlated with the median survival.
| Table IIIAnalysis of immunostaining for
overall survival. |
Table III
Analysis of immunostaining for
overall survival.
| Median survival
(months) Positivity vs. negativity | P-value |
|---|
| E-cadherin | 20 vs. 8 | >0.05 |
| N-cadherin | 36 vs. 12 | 0.027 |
| MSS1 | 20 vs. 16 | >0.05 |
| Claudin 3 | 32 vs. 16 | >0.05 |
| Claudin 4 | 32 vs. 16 | >0.05 |
| Glut 1 | 20 vs. 33 | >0.05 |
| Clusterin | 16 vs. 32 | >0.05 |
| VEGF | 16 vs. 20 | >0.05 |
| EGFR | 20 vs. 32 | >0.05 |
| p53 | 16 vs. 36 | >0.05 |
| Table IVAnalysis of clinical factors for
overall survival. |
Table IV
Analysis of clinical factors for
overall survival.
| Median survival
(months) | P-value |
|---|
| Age (<70 vs.
≥70) | 18 vs. 32 | >0.05 |
| Tumor size
(mm)(<50 vs. ≥50) | 16 vs. 33 | >0.05 |
| M stage (0 vs.
1) | 32 vs. 12 | >0.05 |
| Lymphatic invasion
(yes vs. no) | 20 vs. NR | >0.05 |
| Vascular invasion
(yes vs. no) | 12 vs. 33 | 0.008 |
| Neural invasion
(yes vs. no) | 16 vs. 33 | 0.061 |
| Brain metastasis
(yes vs. no) | 16 vs. 20 | >0.05 |
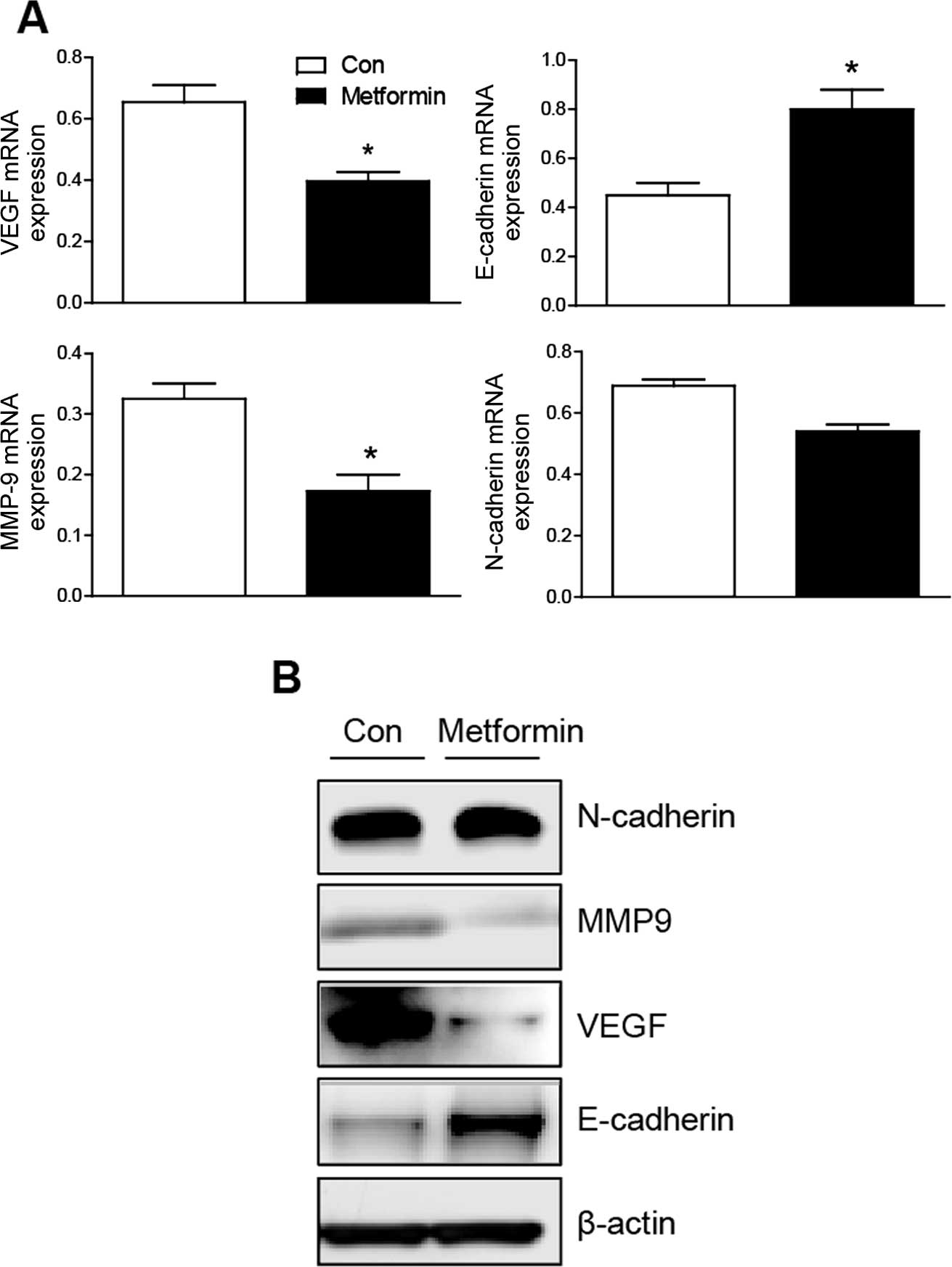
Modulation of VEGF and N-cadherin by
metformin in tumor-bearing mice
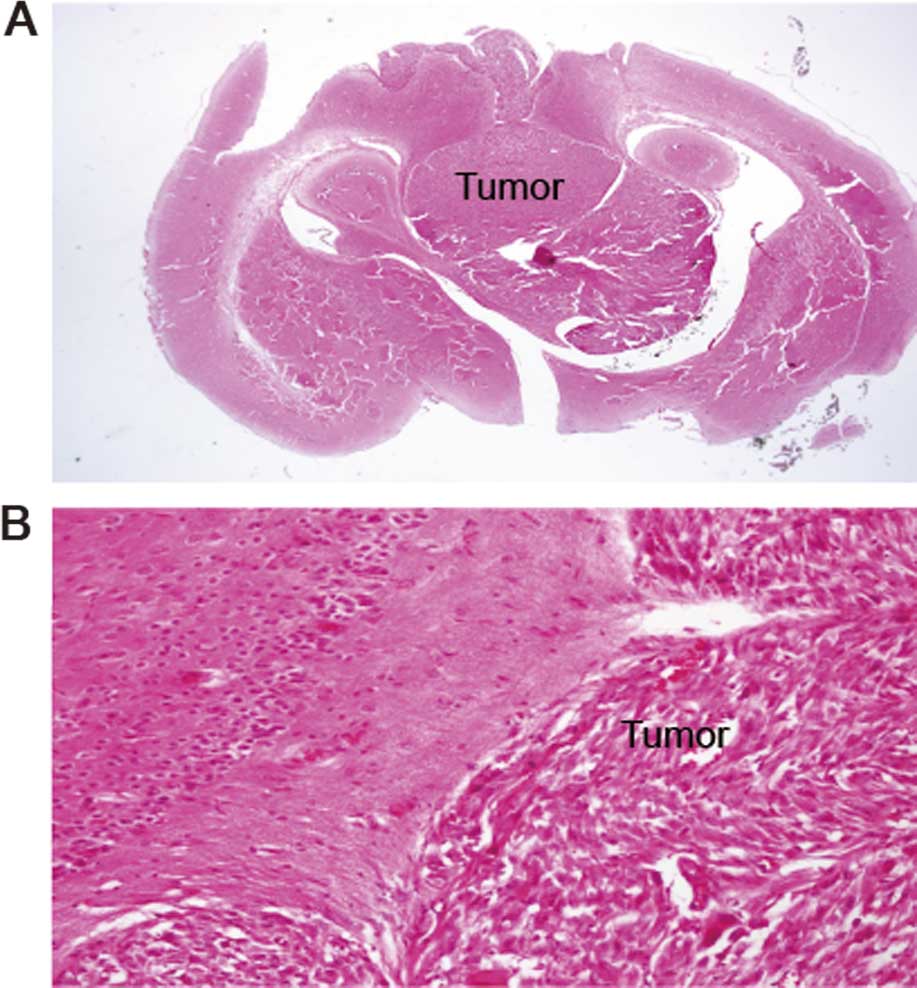
As shown in Fig. 3,
the inoculation of MK28 cells was found in the mouse brain. The
level of VEGF mRNA was decreased in the treatment group compared
with the controls. E-cadherin was increased in the treatment group,
while N-cadherin did not alter after administration of metformin.
To investigate changes in epithelial-to-mesenchymal transition
(EMT), expression of the mesenchymal marker MMP9 was assessed. The
MMP9 expression was decreased in the metformin-treated group
compared with the controls. These findings are compatible with the
western blotting results (Fig.
4).
Discussion
The present study evaluated the correlations between
clinicopathological findings and survival in brain metastasis of
advanced gastric cancers. The overall survival of all 22 patients
with advanced gastric cancer was influenced by vascular invasion
and expression of N-cadherin. Our results suggested a role for VEGF
expression in gastric cancer brain metastasis. It has been reported
that elevated VEGF expression contributes to the ability of breast
and prostate cancer cells to metastasize to the brain in nude mice
(22,23). Angiogenic factors expressed by
metastatic cancers are potent mediators of angiogenesis and
vascular permeability in brain metastasis. High VEGF levels in CSF
have a very high specificity for leptomeningeal metastasis
(24). The role of angiogenesis in
brain metastasis is not clear. Bevacizumab monoclonal antibody to
VEGF and sunitinib, a multi-kinase inhibitor that affects the VEGF
receptor are in clinical trials for treating brain metastasis of
breast and lung cancer (25).
Generally, the loss of E-cadherin and the gain of
N-cadherin indicate the conversion of tumor cells into a metastatic
phenotype; nevertheless, we could not find any correlation between
brain metastasis and E- or N-cadherin expression. In 146 gastric
cancer patients, including 84 patients with stage I, the 5-year
survival rate of the N-cadherin-positive group was significantly
worse than that of the N-cadherin-negative group (58 vs. 78%)
(26). By contrast, in our series
of advanced gastric cancers, the survival of patients with positive
N-cadherin immunoreactivity was longer than that of those with
negative immunoreactivity, while E-cadherin expression did not
correlate with survival. This discrepancy could have arisen since
the number of patients we enrolled was very small, and early-stage
gastric cancers were excluded from our series.
Of the nine patients with brain metastasis,
resection and radiation therapy were performed in two, radiation
only in two, intrathecal methotrexate chemotherapy in one and four
were conservatively treated. In 19 cases of cytologically confirmed
leptomeningeal carcinomatosis, the median survival was 4–8 weeks
(27,28). Other authors have described a longer
median survival of ~13 months for patients who underwent surgical
resection of brain metastasis followed by radiotherapy (29,30).
Since the systemic disease was already advanced and multiple
lesions were not accessible surgically, it is not difficult to
choose aggressive multidisciplinary treatment. The overall survival
of patients with and without brain metastasis did not differ in our
series of advanced gastric cancers. However, since no standard
therapy for gastric cancer brain metastasis has been established,
it is important to investigate the predictors of brain metastasis
and develop a preventive strategy for gastric cancer brain
metastasis. We investigated modulation of the expression of VEGF,
N- and E-cadherin, and MMP9 in mouse models of brain metastasis
that had been inoculated with gastric cancer cells
transcranially.
The invasion and metastasis of solid tumors require
EMT for tumor cells to invade and metastasize (31). During EMT, non-motile, polarized
epithelial cells embedded via cell-cell junctions in a cell
collective dissolve their cell-cell junctions and transform into
individual, non-polarized, motile and invasive mesenchymal cells.
Previously, we reported that the reduced expression of molecules
involved in EMT, such as E-cadherin, could be used to identify
patients at high risk for developing brain metastasis of non-small
cell lung cancer (32). In the
present study, we suggest that VEGF expression is associated with
brain metastasis of advanced gastric cancer. Metformin inhibited
VEGF expression in MCF-7 breast cancer cells via the AMP-activated
protein kinase pathway (33).
Metformin inhibits both angiogenesis and the metastatic spread of
various cancer cells by preventing EMT (34,35).
In tumor-bearing mouse models, metformin administration decreased
the expression of VEGF and MMP9. In addition, the expression of
E-cadherin was increased, although that of N-cadherin did not
significantly change. In mouse models, the dose of metformin
administered to the mice (2 mg/25 g/day) is in the same range as
that administered to diabetic patients (3 g/75 kg/day) (36). These findings suggest that metformin
may prevent or attenuate the EMT process and cell invasiveness.
In conclusion, brain metastasis in advanced gastric
cancer was associated with the expression of VEGF. Metformin
treatment affects the metastatic capacity of gastric cancers by
reducing VEGF expression and blocking EMT.
Acknowledgments
The authors wish to acknowledge the financial
support of the St. Vincent's Hospital, Research Institute of
Medical Science Foundation (SVHR-2012-06).
References
|
1
|
Mathers CD, Shibuya K, Boschi-Pinto C,
Lopez AD and Murray CJ: Global and regional estimates of cancer
mortality and incidence by site: I. Application of regional cancer
survival model to estimate cancer mortality distribution by site.
BMC Cancer. 2:36–63. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Park CH, Song KY and Kim SN: Treatment
results for gastric cancer surgery: 12 years' experience at a
single institute in Korea. Eur J Surg Oncol. 34:36–41. 2008.
View Article : Google Scholar
|
|
3
|
Kim M: Intracranial involvement by
metastatic advanced gastric carcinoma. J Neurooncol. 43:59–62.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Gupta GP, Nguyen DX, Chiang AC, Bos PD,
Kim JY, Nadal C, Gomis RR, Manova-Todorova K and Massagué J:
Mediators of vascular remodelling co-opted for sequential steps in
lung metastasis. Nature. 446:765–770. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shiozaki H, Oka H, Inoue M, Tamura S and
Monden M: E-cadherin mediated adhesion system in cancer cells.
Cancer. 77(Suppl 8): S1605–S1613. 1996. View Article : Google Scholar
|
|
6
|
Ishimine H, Yamakawa N, Sasao M, Tadokoro
M, Kami D, Komazaki S, Tokuhara M, Takada H, Ito Y, Kuno S, et al:
N-Cadherin is a prospective cell surface marker of human
mesenchymal stem cells that have high ability for cardiomyocyte
differentiation. Biochem Biophys Res Commun. 438:753–759. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Decoster E, Vassal A and Faye G: MSS1, a
nuclear-encoded mitochondrial GTPase involved in the expression of
COX1 subunit of cytochrome c oxidase. J Mol Biol. 232:79–88. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Satake S, Semba S, Matsuda Y, Usami Y,
Chiba H, Sawada N, Kasuga M and Yokozaki H: Cdx2 transcription
factor regulates claudin-3 and claudin-4 expression during
intestinal differentiation of gastric carcinoma. Pathol Int.
58:156–163. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kawamura T, Kusakabe T, Sugino T, Watanabe
K, Fukuda T, Nashimoto A, Honma K and Suzuki T: Expression of
glucose transporter-1 in human gastric carcinoma: Association with
tumor aggressiveness, metastasis, and patient survival. Cancer.
92:634–641. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Maher F, Davies-Hill TM, Lysko PG,
Henneberry RC and Simpson IA: Expression of two glucose
transporters, GLUT1 and GLUT3, in cultured cerebellar neurons:
Evidence for neuron-specific expression of GLUT3. Mol Cell
Neurosci. 2:351–360. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tang M, Li J, Liu B, Song N, Wang Z and
Yin C: Clusterin expression and human testicular seminoma. Med
Hypotheses. 81:635–637. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Trougakos IP and Gonos ES:
Clusterin/apolipoprotein J in human aging and cancer. Int J Biochem
Cell Biol. 34:1430–1448. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gerson KD, Maddula VS, Seligmann BE,
Shearstone JR, Khan A and Mercurio AM: Effects of β4 integrin
expression on microRNA patterns in breast cancer. Biol Open.
1:658–666. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wu J, Liu X and Wang Y: Predictive value
of preoperative serum CCL2, CCL18, and VEGF for the patients with
gastric cancer. BMC Clin Pathol. 13:15–20. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen C, Yang JM, Hu TT, Xu TJ, Yan G, Hu
SL, Wei W and Xu WP: Prognostic role of human epidermal growth
factor receptor in gastric cancer: A systematic review and
meta-analysis. Arch Med Res. 44:380–389. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Preusser M, Berghoff AS, Ilhan-Mutlu A,
Dinhof C, Magerle M, Marosi C, Hejna M, Capper D, Von Deimling A,
Schoppmann SF, et al: Brain metastases of gastro-oesophageal
cancer: Evaluation of molecules with relevance for targeted
therapies. Anticancer Res. 33:1065–1071. 2013.PubMed/NCBI
|
|
17
|
Yamada Y, Yoshida T, Hayashi K, Sekiya T,
Yokota J, Hirohashi S, Nakatani K, Nakano H, Sugimura T and Terada
M: p53 gene mutations in gastric cancer metastases and in gastric
cancer cell lines derived from metastases. Cancer Res.
51:5800–5805. 1991.PubMed/NCBI
|
|
18
|
de Vries AC and Kuipers EJ: Commentary:
Metformin use is associated with reduced gastric cancer risk.
Aliment Pharmacol Ther. 39:12392014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ruiter R, Visser LE, van Herk-Sukel MP,
Coebergh JW, Haak HR, Geelhoed-Duijvestijn PH, Straus SM, Herings
RM and Stricker BH: Lower risk of cancer in patients on metformin
in comparison with those on sulfonylurea derivatives: Results from
a large population-based follow-up study. Diabetes Care.
35:119–124. 2012. View Article : Google Scholar :
|
|
20
|
Kato K, Gong J, Iwama H, Kitanaka A, Tani
J, Miyoshi H, Nomura K, Mimura S, Kobayashi M, Aritomo Y, et al:
The anti-diabetic drug metformin inhibits gastric cancer cell
proliferation in vitro and in vivo. Mol Cancer Ther. 11:549–560.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Japanese Gastric Cancer Association:
Japanese classification of gastric carcinoma: 3rd English edition.
Gastric Cancer. 14:101–112. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim LS, Huang S, Lu W, Lev DC and Price
JE: Vascular endothelial growth factor expression promotes the
growth of breast cancer brain metastases in nude mice. Clin Exp
Metastasis. 21:107–118. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
JuanYin J, Tracy K, Zhang L, Munasinghe J,
Shapiro E, Koretsky A and Kelly K: Noninvasive imaging of the
functional effects of anti-VEGF therapy on tumor cell extravasation
and regional blood volume in an experimental brain metastasis
model. Clin Exp Metastasis. 26:403–414. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Herrlinger U, Wiendl H, Renninger M,
Förschler H, Dichgans J and Weller M: Vascular endothelial growth
factor (VEGF) in leptomeningeal metastasis: Diagnostic and
prognostic value. Br J Cancer. 91:219–224. 2004.PubMed/NCBI
|
|
25
|
Gril B, Evans L, Palmieri D and Steeg PS:
Translational research in brain metastasis is identifying molecular
pathways that may lead to the development of new therapeutic
strategies. Eur J Cancer. 46:1204–1210. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kamikihara T, Ishigami S, Arigami T,
Matsumoto M, Okumura H, Uchikado Y, Kita Y, Kurahara H, Kijima Y,
Ueno S, et al: Clinical implications of N-cadherin expression in
gastric cancer. Pathol Int. 62:161–166. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lee JL, Kang YK, Kim TW, Chang HM, Lee GW,
Ryu MH, Kim E, Oh SJ, Lee JH, Kim SB, et al: Leptomeningeal
carcinomatosis in gastric cancer. J Neurooncol. 66:167–174. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Tomita H, Yasui H, Boku N, Nakasu Y,
Mitsuya K, Onozawa Y, Fukutomi A, Yamazaki K, Machida N, Taku K, et
al: Leptomeningeal carcinomatosis associated with gastric cancer.
Int J Clin Oncol. 17:361–366. 2012. View Article : Google Scholar
|
|
29
|
York JE, Stringer J, Ajani JA, Wildrick DM
and Gokaslan ZL: Gastric cancer and metastasis to the brain. Ann
Surg Oncol. 6:771–776. 1999. View Article : Google Scholar
|
|
30
|
Kasakura Y, Fujii M, Mochizuki F, Suzuki T
and Takahashi T: Clinicopathological study of brain metastasis in
gastric cancer patients. Surg Today. 30:485–490. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Prudkin L, Liu DD, Ozburn NC, Sun M,
Behrens C, Tang X, Brown KC, Bekele BN, Moran C and Wistuba II:
Epithelial-to-mesenchymal transition in the development and
progression of adenocarcinoma and squamous cell carcinoma of the
lung. Mod Pathol. 22:668–678. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yoo JY, Yang SH, Lee JE, Cho DG, Kim HK,
Kim SH, Kim IS, Hong JT, Sung JH, Son BC, et al: E-cadherin as a
predictive marker of brain metastasis in non-small-cell lung
cancer, and its regulation by pioglitazone in a preclinical model.
J Neurooncol. 109:219–227. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ishibashi Y, Matsui T, Takeuchi M and
Yamagishi S: Metformin inhibits advanced glycation end products
(AGEs)-induced growth and VEGF expression in MCF-7 breast cancer
cells by suppressing AGEs receptor expression via AMP-activated
protein kinase. Horm Metab Res. 45:387–390. 2013.
|
|
34
|
Cufí S, Vazquez-Martin A,
Oliveras-Ferraros C, Martin-Castillo B, Joven J and Menendez JA:
Metformin against TGFβ-induced epithelial-to-mesenchymal transition
(EMT): From cancer stem cells to aging-associated fibrosis. Cell
Cycle. 9:4461–4468. 2010. View Article : Google Scholar
|
|
35
|
Rattan R, Graham RP, Maguire JL, Giri S
and Shridhar V: Metformin suppresses ovarian cancer growth and
metastasis with enhancement of cisplatin cytotoxicity in vivo.
Neoplasia. 13:483–491. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Cerezo M, Tichet M, Abbe P, Ohanna M,
Lehraiki A, Rouaud F, Allegra M, Giacchero D, Bahadoran P,
Bertolotto C, et al: Metformin blocks melanoma invasion and
metastasis development in AMPK/p53-dependent manner. Mol Cancer
Ther. 12:1605–1615. 2013. View Article : Google Scholar : PubMed/NCBI
|